Lateral Sinus Floor Elevation Performed with Trapezoidal and Modified Triangular Flap Designs: A Randomized Pilot Study of Post-Operative Pain Using Thermal Infrared Imaging

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
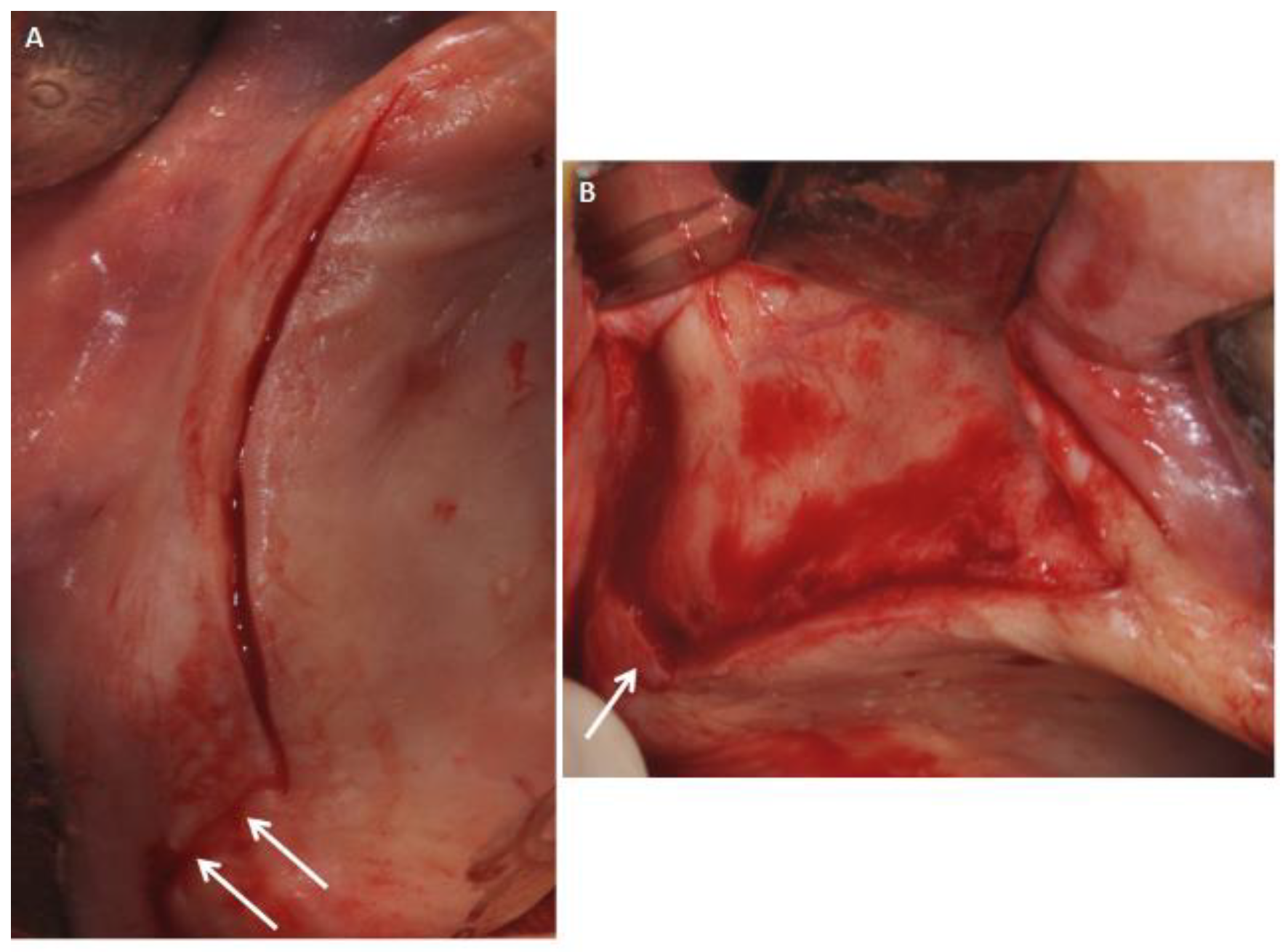
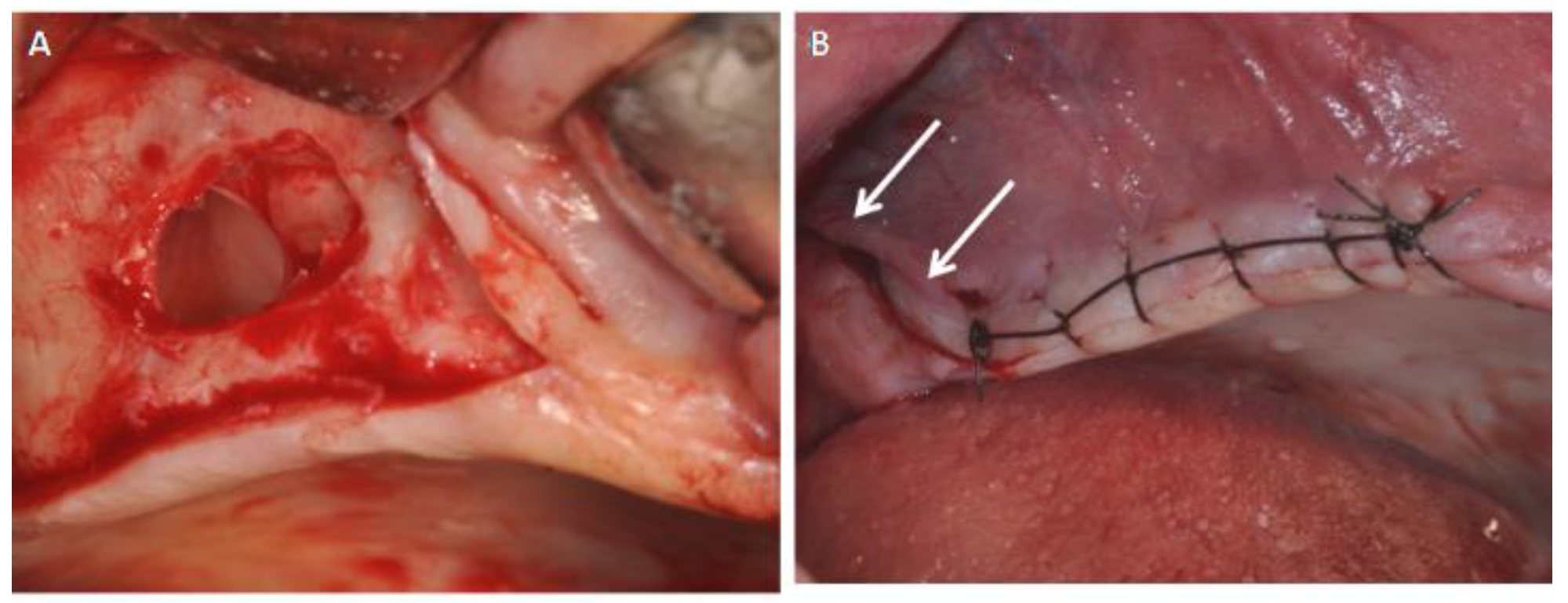
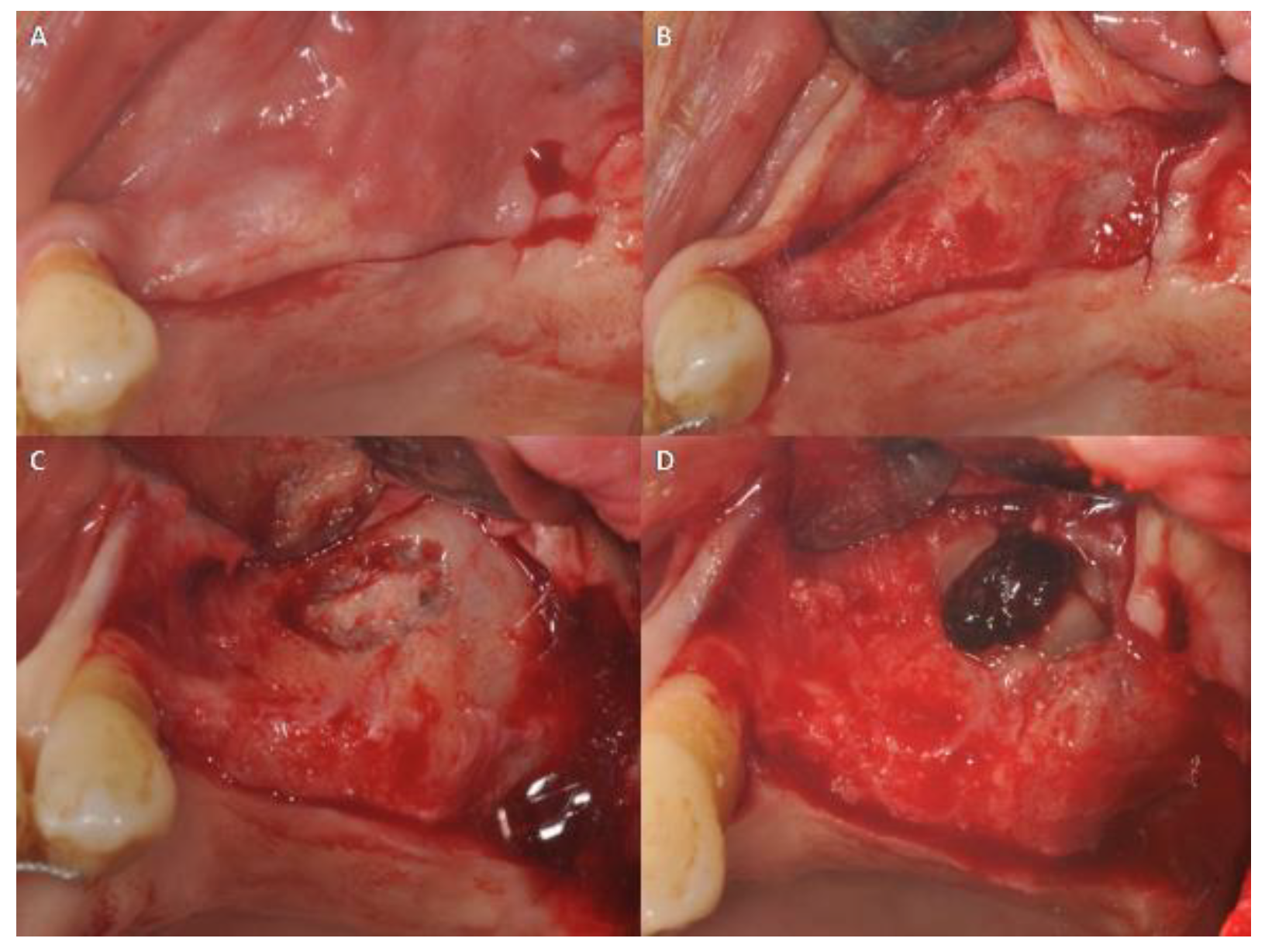
2.2. Surgical Procedures and Flap Design
2.3. Temperature Measurements
2.4. Statistical Evaluation
2.5. Trial Registration
3. Results
3.1. Group I: TZ Flap
3.2. Group II: MT Flap
3.3. Statistical Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Zucoloto, M.L.; Maroco, J.; Campos, J.A.D.B. Impact of oral health on health-related quality of life: A cross-sectional study. BMC Oral Health 2016, 16, 55. [Google Scholar] [CrossRef] [PubMed]
- Wallace, S.S.; Froum, S.J. Effect of maxillary sinus augmentation on the survival of endosseous dental implants. A systematic review. Ann. Periodontol. 2003, 8, 328–343. [Google Scholar] [CrossRef] [PubMed]
- Ersanli, S.; Arısan, V.; Bedeloğlu, E. Evaluation of the autogenous bone block transfer for dental implant placement: Symphysal or ramus harvesting? BMC Oral Health 2016, 16, 4. [Google Scholar] [CrossRef] [PubMed]
- Piattelli, M.; Favero, G.A.; Scarano, A.; Orsini, G.; Piattelli, A. Bone reactions to anorganic bovine bone (Bio-Oss) used in sinus augmentation procedures: A histologic long-term report of 20 cases in humans. Int. J. Oral Maxillofac. Implants 1999, 14, 835–840. [Google Scholar] [PubMed]
- Landi, L.; Pretel, R.W.; Hakimi, N.M.; Setayesh, R. Maxillary sinus floor elevation using a combination of DFDBA and bovine-derived porous hydroxyapatite: A preliminary histologic and histomorphometric report. Int. J. Periodontics Restor. Dent. 2000, 20, 574–583. [Google Scholar]
- Mangano, C.; Scarano, A.; Perrotti, V.; Iezzi, G.; Piattelli, A. Maxillary sinus augmentation with a porous synthetic hydroxyapatite and bovine-derived hydroxyapatite: A comparative clinical and histologic study. Int. J. Oral Maxillofac. Implants 2007, 22, 980–986. [Google Scholar] [PubMed]
- Scarano, A.; Degidi, M.; Iezzi, G.; Pecora, G.; Piattelli, M.; Orsini, G.; Caputi, S.; Perrotti, V.; Mangano, C.; Piattelli, A. Maxillary sinus augmentation with different biomaterials: A comparative histologic and histomorphometric study in man. Implant Dent. 2006, 15, 197–207. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, R.; Salmon, B.; Codari, M.; Hassan, B.; Bornstein, M.M. Cone beam computed tomography in implant dentistry: Recommendations for clinical use. BMC Oral Health 2018, 18, 88. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.-H.; Kim, H.-M.; Byun, J.-H.; Kim, U.-K.; Sung, I.-Y.; Cho, Y.-C.; Park, B.-W. Stability of simultaneously placed dental implants with autologous bone grafts harvested from the iliac crest or intraoral jaw bone. BMC Oral Health 2015, 15, 172. [Google Scholar] [CrossRef] [PubMed]
- Stacchi, C.; Lombardi, T.; Ottonelli, R.; Berton, F.; Perinetti, G.; Traini, T. New bone formation after transcrestal sinus floor elevation was influenced by sinus cavity dimensions: A prospective histologic and histomorphometric study. Clin. Oral Implants Res. 2018, 29, 465–479. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, T.; Stacchi, C.; Berton, F.; Traini, T.; Torelli, L.; Di Lenarda, R. Influence of Maxillary Sinus Width on New Bone Formation After Transcrestal Sinus Floor Elevation: A Proof-of-Concept Prospective Cohort Study. Implant Dent. 2017, 26, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Scala, A.; Botticelli, D.; Rangel, I.G.; De Oliveira, J.A.; Okamoto, R.; Lang, N.P. Early healing after elevation of the maxillary sinus floor applying a lateral access: A histological study in monkeys. Clin. Oral Implants Res. 2010, 21, 1320–1326. [Google Scholar] [CrossRef] [PubMed]
- Avila-Ortiz, G.; Wang, H.-L.; Galindo-Moreno, P.; Misch, C.E.; Rudek, I.; Neiva, R. Influence of lateral window dimensions on vital bone formation following maxillary sinus augmentation. Int. J. Oral Maxillofac. Implants 2012, 27, 1230–1238. [Google Scholar] [PubMed]
- Maria Soardi, C.; Spinato, S.; Zaffe, D.; Wang, H.-L. Atrophic maxillary floor augmentation by mineralized human bone allograft in sinuses of different size: An histologic and histomorphometric analysis. Clin. Oral Implants Res. 2011, 22, 560–566. [Google Scholar] [CrossRef] [PubMed]
- Fenner, M.; Vairaktaris, E.; Stockmann, P.; Schlegel, K.A.; Neukam, F.W.; Nkenke, E. Influence of residual alveolar bone height on implant stability in the maxilla: An experimental animal study. Clin. Oral Implants Res. 2009, 20, 751–755. [Google Scholar] [CrossRef] [PubMed]
- Busenlechner, D.; Huber, C.D.; Vasak, C.; Dobsak, A.; Gruber, R.; Watzek, G. Sinus augmentation analysis revised: The gradient of graft consolidation. Clin. Oral Implants Res. 2009, 20, 1078–1083. [Google Scholar] [CrossRef] [PubMed]
- Valentini, P.; Abensur, D. Maxillary sinus floor elevation for implant placement with demineralized freeze-dried bone and bovine bone (Bio-Oss): A clinical study of 20 patients. Int. J. Periodontics Restor. Dent. 1997, 17, 232–241. [Google Scholar]
- Valentini, P.; Abensur, D.; Wenz, B.; Peetz, M.; Schenk, R. Sinus grafting with porous bone mineral (Bio-Oss) for implant placement: A 5-year study on 15 patients. Int. J. Periodontics Restor. Dent. 2000, 20, 245–253. [Google Scholar]
- Yildirim, M.; Spiekermann, H.; Biesterfeld, S.; Edelhoff, D. Maxillary sinus augmentation using xenogenic bone substitute material Bio-Oss in combination with venous blood. A histologic and histomorphometric study in humans. Clin. Oral Implants Res. 2000, 11, 217–229. [Google Scholar] [CrossRef] [PubMed]
- Hallman, M.; Sennerby, L.; Lundgren, S. A clinical and histologic evaluation of implant integration in the posterior maxilla after sinus floor augmentation with autogenous bone, bovine hydroxyapatite, or a 20:80 mixture. Int. J. Oral Maxillofac. Implants 2002, 17, 635–643. [Google Scholar] [PubMed]
- Karabuda, C.; Ozdemir, O.; Tosun, T.; Anil, A.; Olgaç, V. Histological and clinical evaluation of 3 different grafting materials for sinus lifting procedure based on 8 cases. J. Periodontol. 2001, 72, 1436–1442. [Google Scholar] [CrossRef] [PubMed]
- Miser, A.W.; Dothage, J.A.; Wesley, R.A.; Miser, J.S. The prevalence of pain in a pediatric and young adult cancer population. Pain 1987, 29, 73–83. [Google Scholar] [CrossRef]
- Danesh-Sani, S.A.; Engebretson, S.P.; Janal, M.N. Histomorphometric results of different grafting materials and effect of healing time on bone maturation after sinus floor augmentation: A systematic review and meta-analysis. J. Periodontal Res. 2017, 52, 301–312. [Google Scholar] [CrossRef] [PubMed]
- Aludden, H.C.; Mordenfeld, A.; Hallman, M.; Dahlin, C.; Jensen, T. Lateral ridge augmentation with Bio-Oss alone or Bio-Oss mixed with particulate autogenous bone graft: A systematic review. Int. J. Oral Maxillofac. Surg. 2017, 46, 1030–1038. [Google Scholar] [CrossRef] [PubMed]
- Stacchi, C.; Lombardi, T.; Oreglia, F.; Alberghini Maltoni, A.; Traini, T. Histologic and histomorphometric comparison between sintered nanohydroxyapatite and anorganic bovine xenograft in maxillary sinus grafting: A split-mouth randomized controlled Clinical Trial. BioMed Res. Int. 2017, 2017, 9489825. [Google Scholar] [CrossRef] [PubMed]
- Galindo-Moreno, P.; de Buitrago, J.G.; Padial-Molina, M.; Fernández-Barbero, J.E.; Ata-Ali, J.; O′ Valle, F. Histopathological comparison of healing after maxillary sinus augmentation using xenograft mixed with autogenous bone versus allograft mixed with autogenous bone. Clin. Oral Implants Res. 2018, 29, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Dursun, C.K.; Dursun, E.; Eratalay, K.; Orhan, K.; Tatar, I.; Baris, E.; Tözüm, T.F. Effect of porous titanium granules on bone regeneration and primary stability in maxillary sinus: A human clinical, histomorphometric, and microcomputed tomography analyses. J. Craniofacial Surg. 2016, 27, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Franceschetti, G.; Rizzi, A.; Minenna, L.; Pramstraller, M.; Trombelli, L.; Farina, R. Patient-reported outcomes of implant placement performed concomitantly with transcrestal sinus floor elevation or entirely in native bone. Clin. Oral Implants Res. 2017, 28, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Nickenig, H.-J.; Wichmann, M.; Zöller, J.E.; Eitner, S. 3-D based minimally invasive one-stage lateral sinus elevation—A prospective randomized clinical pilot study with blinded assessment of postoperative visible facial soft tissue volume changes. J. Cranio-Maxillo-Facial Surg. 2014, 42, 890–895. [Google Scholar] [CrossRef] [PubMed]
- Trombelli, L.; Franceschetti, G.; Stacchi, C.; Minenna, L.; Riccardi, O.; Di Raimondo, R.; Rizzi, A.; Farina, R. Minimally invasive transcrestal sinus floor elevation with deproteinized bovine bone or β-tricalcium phosphate: A multicenter, double-blind, randomized, controlled clinical trial. J. Clin. Periodontol. 2014, 41, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Al-Samman, A.A.; Othman, H.A. Facial expression drawings and the full cup test: Valid tools for the measurement of swelling after dental surgery. Br. J. Oral Maxillofac. Surg. 2017, 55, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Inchingolo, F.; Murmura, G.; Traini, T.; Piattelli, A.; Lorusso, F. Three-Dimensional Architecture and Mechanical Properties of Bovine Bone Mixed with Autologous Platelet Liquid, Blood, or Physiological Water: An In Vitro Study. Int. J. Mol. Sci. 2018, 19, 1230. [Google Scholar] [CrossRef] [PubMed]
- Giuliani, A.; Manescu, A.; Larsson, E.; Tromba, G.; Luongo, G.; Piattelli, A.; Mangano, F.; Iezzi, G.; Mangano, C. In Vivo Regenerative Properties of Coralline-Derived (Biocoral) Scaffold Grafts in Human Maxillary Defects: Demonstrative and Comparative Study with Beta-Tricalcium Phosphate and Biphasic Calcium Phosphate by Synchrotron Radiation X-Ray Microtomography. Clin. Implant Dent. Relat. Res. 2014, 16, 736–750. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Lorusso, F.; Staiti, G.; Sinjari, B.; Tampieri, A.; Mortellaro, C. Sinus Augmentation with Biomimetic Nanostructured Matrix: Tomographic, Radiological, Histological and Histomorphometrical Results after 6 Months in Humans. Front. Physiol. 2017, 8, 565. [Google Scholar] [CrossRef] [PubMed]
- Crellin, D.; Sullivan, T.P.; Babl, F.E.; O’Sullivan, R.; Hutchinson, A. Analysis of the validation of existing behavioral pain and distress scales for use in the procedural setting. Paediatr. Anaesth. 2007, 17, 720–733. [Google Scholar] [CrossRef] [PubMed]
- Mangano, F.; Macchi, A.; Shibli, J.A.; Luongo, G.; Iezzi, G.; Piattelli, A.; Caprioglio, A.; Mangano, C. Maxillary ridge augmentation with custom-made CAD/CAM scaffolds. A 1-year prospective study on 10 patients. J. Oral Implantol. 2014, 40, 561–569. [Google Scholar] [CrossRef] [PubMed]
- UStün, Y.; Erdogan, O.; Esen, E.; Karsli, E.D. Comparison of the effects of 2 doses of methylprednisolone on pain, swelling, and trismus after third molar surgery. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2003, 96, 535–539. [Google Scholar] [CrossRef]
- Amin, M.M.; Laskin, D.M. Prophylactic use of indomethacin for prevention of postsurgical complications after removal of impacted third molars. Oral Surg. Oral Med. Oral Pathol. 1983, 55, 448–451. [Google Scholar] [CrossRef]
- Scarano, A.; Piattelli, A.; Assenza, B.; Carinci, F.; Di Donato, L.; Romani, G.L.; Merla, A. Infrared thermographic evaluation of temperature modifications induced during implant site preparation with cylindrical versus conical drills. Clin. Implant Dent. Relat. Res. 2011, 13, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Graff-Radford, S.B.; Ketelaer, M.C.; Gratt, B.M.; Solberg, W.K. Thermographic assessment of neuropathic facial pain. J. Orofac. Pain 1995, 9, 138–146. [Google Scholar] [PubMed]
- Merla, A.; Mattei, P.A.; Di Donato, L.; Romani, G.L. Thermal imaging of cutaneous temperature modifications in runners during graded exercise. Ann. Biomed. Eng. 2010, 38, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Cardone, D.; Pinti, P.; Merla, A. Thermal Infrared Imaging-Based Computational Psychophysiology for Psychometrics. Comput. Math. Methods Med. 2015, 2015, 984353. [Google Scholar] [CrossRef] [PubMed]
- Weisensee, W.; Scheer, M.; Müller, L.; Rothamel, D.; Kistler, F.; Bayer, G.; Jöhren, P.; Neugebauer, J. Impact of anxiety parameters on prospective and experienced pain intensity in implant surgery. Implant Dent. 2012, 21, 502–506. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Sinjari, B.; Lorusso, F.; Mortellaro, C.; D’Ovidio, C.; Carinci, F. Intense, Instantaneous, and Shooting Pain during Local Anesthesia for Implant Surgery. J. Craniofac. Surg. 2018. [Google Scholar] [CrossRef] [PubMed]
- Rosano, G.; Taschieri, S.; Gaudy, J.-F.; Weinstein, T.; Del Fabbro, M. Maxillary sinus vascular anatomy and its relation to sinus lift surgery. Clin. Oral Implants Res. 2011, 22, 711–715. [Google Scholar] [CrossRef] [PubMed]
- Bergh, J.; Bruggenkate, C.M.; Disch, F.J.; Tuinzing, D.B. Anatomical aspects of sinus floor elevations. Clin. Oral Implants Res. 2000, 11, 256–265. [Google Scholar] [CrossRef] [PubMed]
- Venet, L.; Perriat, M.; Mangano, F.G.; Fortin, T. Horizontal ridge reconstruction of the anterior maxilla using customized allogeneic bone blocks with a minimally invasive technique—A case series. BMC Oral Health 2017, 17, 146. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
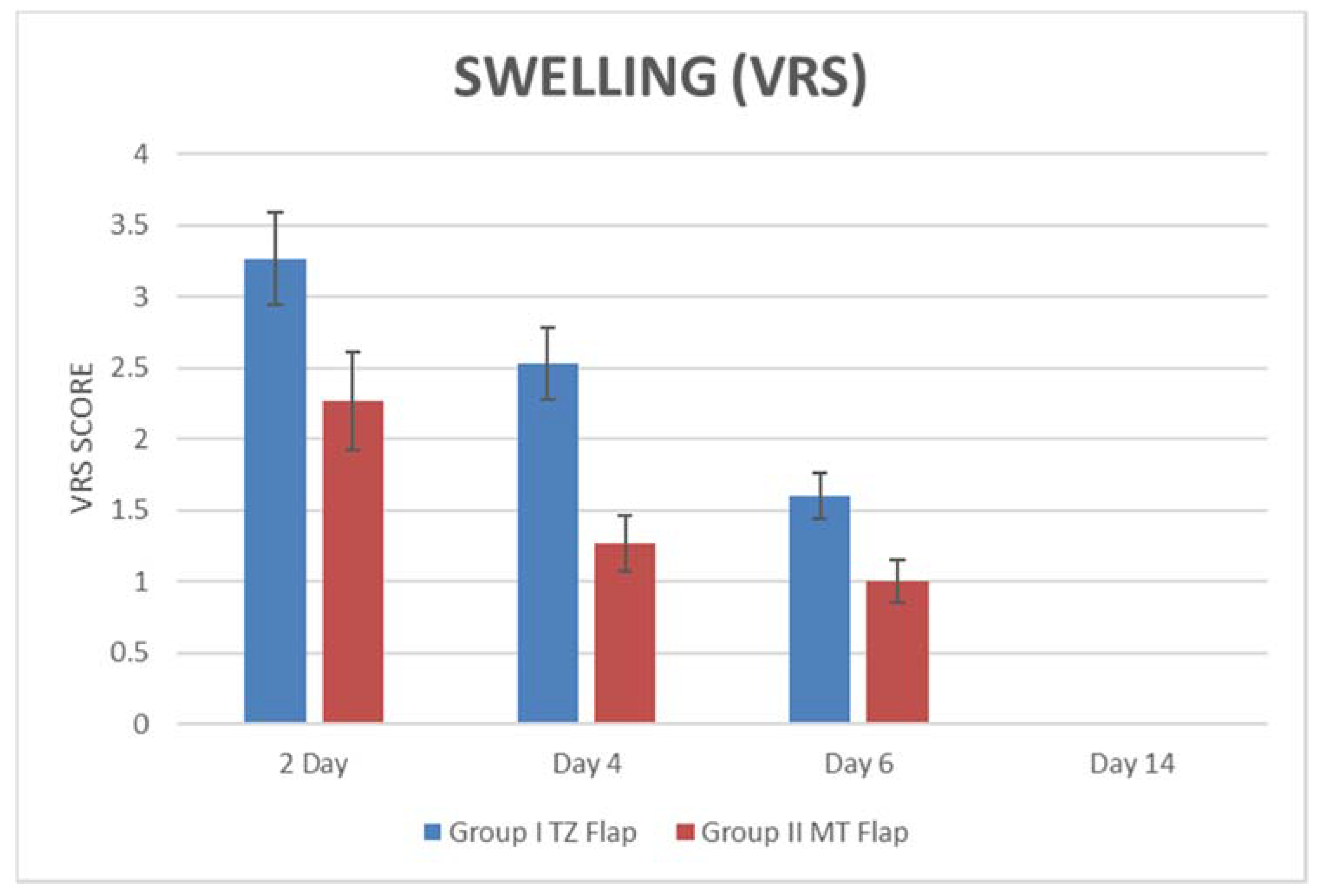
| PAIN (VAS) | SWELLING (VRS) | |||||||
|---|---|---|---|---|---|---|---|---|
| Group I TZ Flap | Day 2 | Day 4 | Day 6 | Day 14 | Day 2 | Day 4 | Day 6 | Day 14 |
| Min | 30 | 15 | 10 | 0 | 2 | 2 | 1 | 0 |
| Max | 50 | 50 | 30 | 0 | 4 | 4 | 3 | 0 |
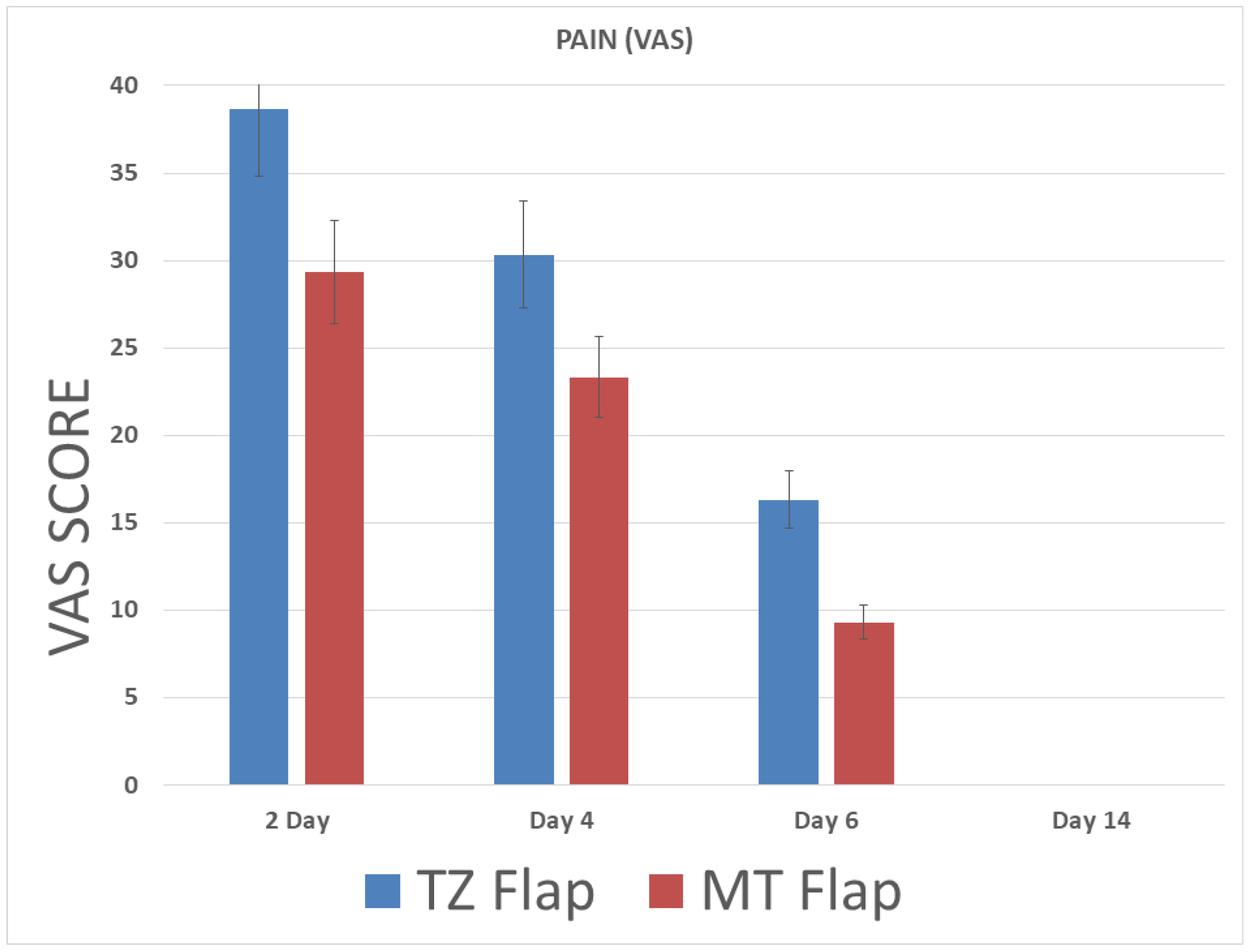
| Mean | 38.67 | 30.33 | 16.33 | 0 | 3.27 | 2.53 | 1.60 | 0 |
| SD | 6.40 | 9.34 | 6.11 | 0 | 0.59 | 0.74 | 0.82 | 0 |
| Group II MT Flap | Day 2 | Day 4 | Day 6 | Day 14 | Day 2 | Day 4 | Day 6 | Day 14 |
| Min | 20 | 10 | 0 | 0 | 2 | 1 | 0 | 0 |
| Max | 40 | 30 | 20 | 0 | 3 | 2 | 1 | 0 |
| Mean | 29.33 | 23.33 | 9.33 | 0 | 2.27 | 1.26 | 1 | 0 |
| SD | 7.03 | 6.17 | 7.98 | 0 | 0.45 | 0.45 | 0 | 0 |
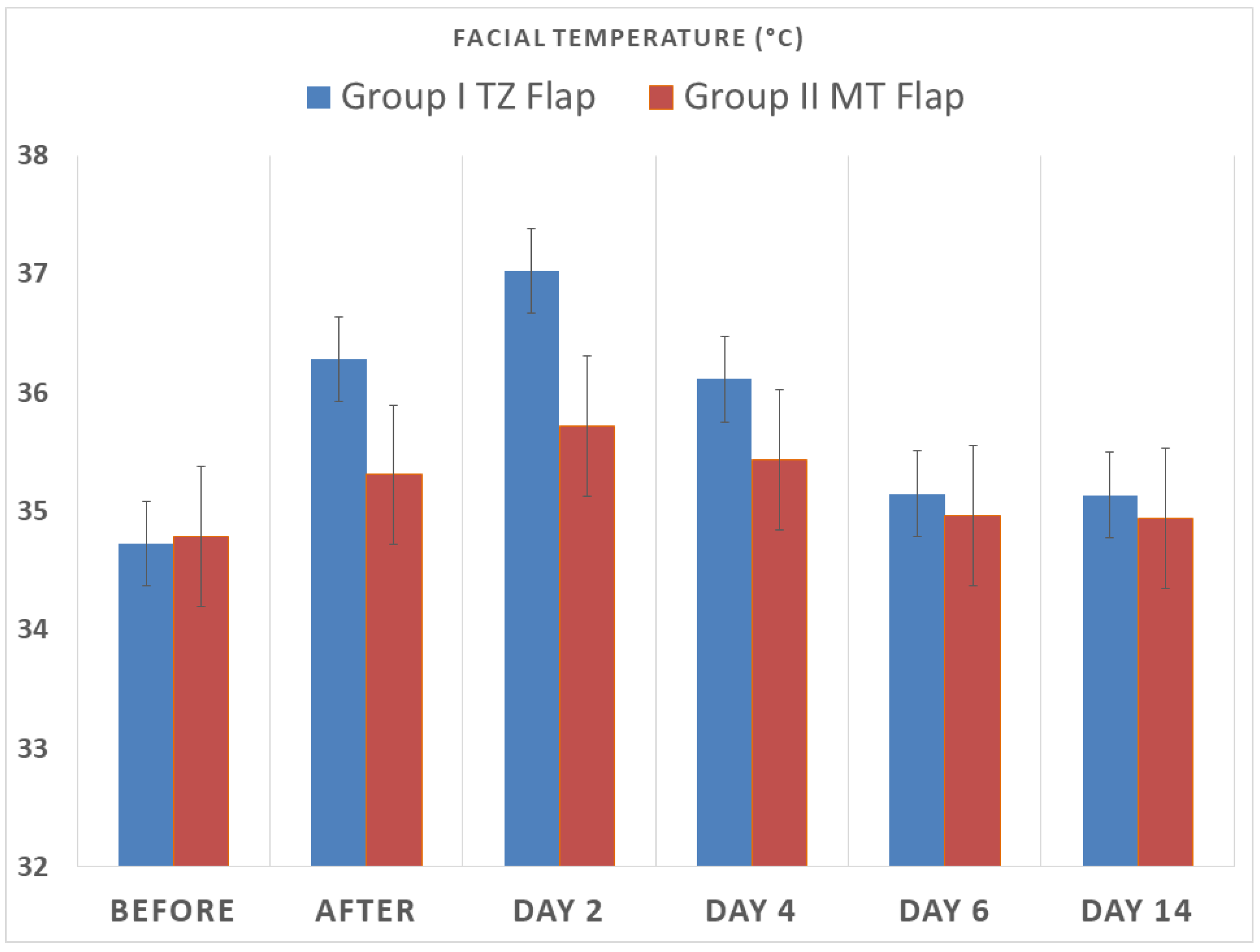
| Temperature (°C) | ||||||
|---|---|---|---|---|---|---|
| Group I TZ Flap | Before | After | Day 2 | Day 4 | Day 6 | Day 14 |
| Min | 34.20 | 35.2 | 35.60 | 34.9 | 34.50 | 34.3 |
| Max | 35.30 | 36.9 | 37.80 | 36.9 | 36.30 | 35.7 |
| Mean | 34.73 | 36.28 | 37.03 | 36.11 | 35.15 | 35.13 |
| SD | 0.37 | 0.44 | 0.53 | 0.55 | 0.55 | 0.52 |
| Group II MT Flap | Before | After | Day 2 | Day 4 | Day 6 | Day 14 |
| Min | 34.20 | 34.2 | 34.10 | 34 | 34.20 | 34.3 |
| Max | 35.60 | 36.8 | 38.10 | 36.8 | 36.30 | 35.7 |
| Mean | 34.79 | 35.30 | 35.72 | 35.43 | 34.96 | 34.94 |
| SD | 0.44 | 0.75 | 1.11 | 0.92 | 0.59 | 0.50 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scarano, A.; Lorusso, F.; Arcangelo, M.; D’Arcangelo, C.; Celletti, R.; De Oliveira, P.S. Lateral Sinus Floor Elevation Performed with Trapezoidal and Modified Triangular Flap Designs: A Randomized Pilot Study of Post-Operative Pain Using Thermal Infrared Imaging. Int. J. Environ. Res. Public Health 2018, 15, 1277. https://doi.org/10.3390/ijerph15061277
Scarano A, Lorusso F, Arcangelo M, D’Arcangelo C, Celletti R, De Oliveira PS. Lateral Sinus Floor Elevation Performed with Trapezoidal and Modified Triangular Flap Designs: A Randomized Pilot Study of Post-Operative Pain Using Thermal Infrared Imaging. International Journal of Environmental Research and Public Health. 2018; 15(6):1277. https://doi.org/10.3390/ijerph15061277
Chicago/Turabian StyleScarano, Antonio, Felice Lorusso, Merla Arcangelo, Camillo D’Arcangelo, Renato Celletti, and Pablo Santos De Oliveira. 2018. "Lateral Sinus Floor Elevation Performed with Trapezoidal and Modified Triangular Flap Designs: A Randomized Pilot Study of Post-Operative Pain Using Thermal Infrared Imaging" International Journal of Environmental Research and Public Health 15, no. 6: 1277. https://doi.org/10.3390/ijerph15061277