Experiences and Opinions of Adults with Type 2 Diabetes Regarding a Self-Regulation-Based eHealth Intervention Targeting Physical Activity and Sedentary Behaviour

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
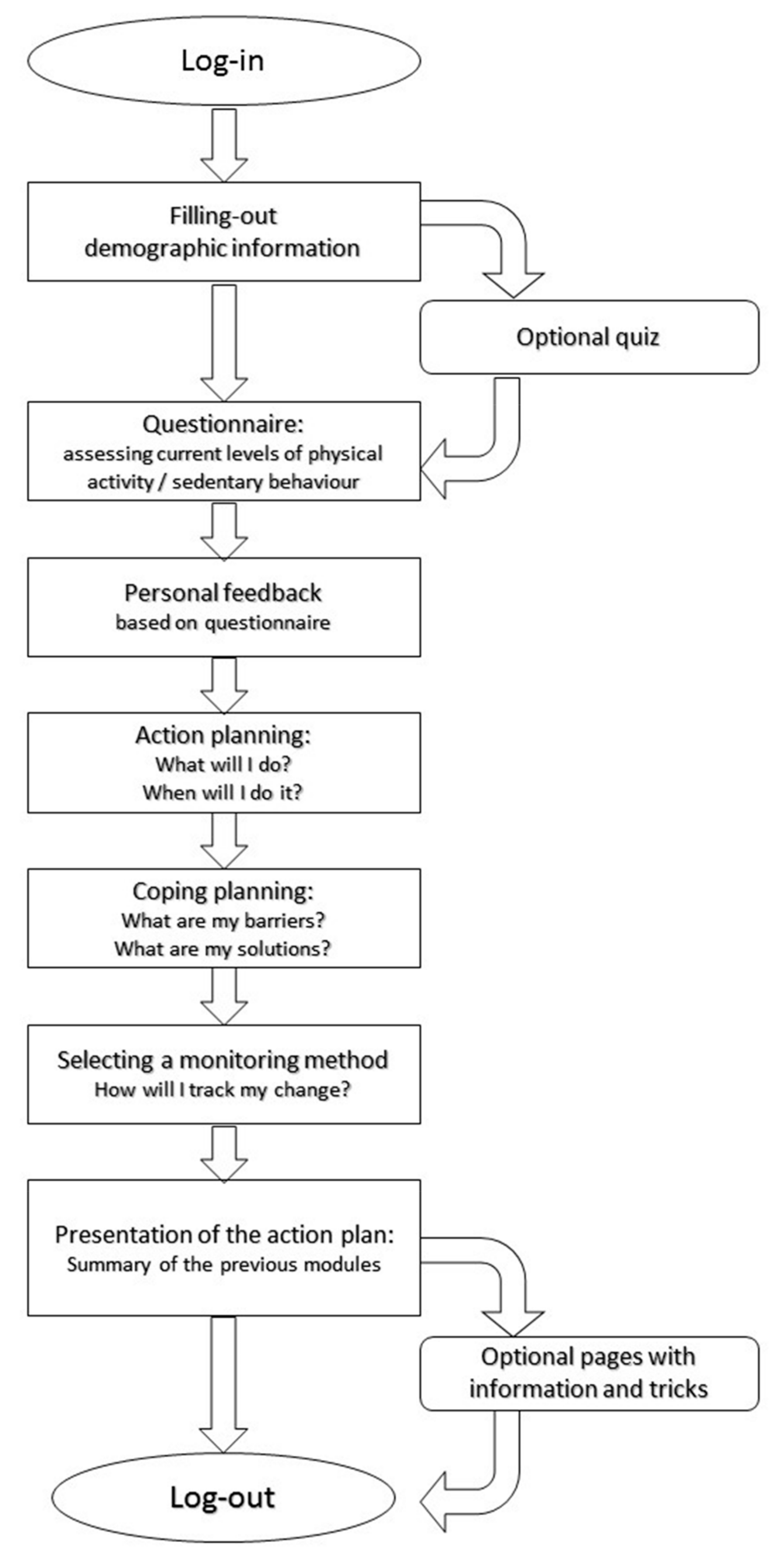
2.2. MyPlan 2.0
2.3. Procedures
2.4. Interview Guide
2.5. Data-Analysis
3. Results
3.1. Participants
3.2. Website Usage
3.3. Interviews
3.3.1. Usefulness of the Website
“No, I knew the advantages for your heart, veins and sugar levels.”(Female, 66 years old)
“I already knew it. Move more often, eat less sweets, those are the basics of diabetes management.”(Male, 66 years old)
“Sometimes I do not think about the fact that I am diabetic but then you receive an e-mail that you need to fill out the website. It awakes the subconscious idea that you need to move more. I feel like they are reminders that keep you awake.”(Male, 61 years old)
“On each occasion I think about the fact that I should get up and walk a little. I am more aware of this than I used to be.”(Male, 73 years old)
“I was surprised, I said “ow, I am still sitting a lot”. I often work standing, I iron standing, I prepare meals standing … but still …”(Female, 67 years old)
“You get confronted with the fact that you do not move very often. And we know it is one of the things you should do as a diabetic. Drink water and move more often. Those are two things that are hard for me and currently lacking.”(Male, 67 years old)
“Yes, yes, absolutely, because being physically active is very important for us!”(Male, 70)
“I think it fits for every age, even for younger people it would be good.”(Female, 57)
“I must say that we already move a lot, so we already did as much as possible.”(Female, 66)
“Yes, that is good! Also because it is not much, well, you do not ask a lot from people. They are small steps that you should take. So each week there are one or two steps and that is achievable. It is not a list of ten things making you say “I need to do all of this!”. No, you do it by yourself, you make your own choices and you get tips and that helps. But you, you do not overwhelm people with it and make it achievable.”(Male, 61)
“Otherwise I put everything near me: water, the remote, a piece of fruit, it is near me. How many times do I get up then? Not once. Now I leave it here and get it when I need it.”(Female, 67)
“It was good and I felt a bit obliged, in a friendly way, to get off the couch or off my bed and to do groceries by foot.”(Male, 69)
“I knew that it (the website) would contact me again, so I had to do something about it!”(Female, 62)
“Well, I think it was good that I had to ask myself what is wrong, why are you not coming out of the couch, why are you not walking around, why am I not doing groceries… So, I think that was good.”(Male, 70)
“Well, there are always barriers, but the solutions are not logic or easy to find.”(Male, 58)
“I printed it and put it next to my computer. If I forgot it, I could review it.”(Female, 67)
“I liked the fact that I could evaluate my plans on a weekly basis. I liked this goal-oriented way of working with moments of evaluation.”(Female, 66)
“I did not keep track of it, but I kept it in my mind.”(Male, 70)
3.3.2. Design of the Website
“You get the feeling that someone else is taking care of you, individually, you get this feeling.”(Male, 70)
“I cannot say it is fun, because filling out a questionnaire is not fun.”(Male, 68)
“Yes, it is easy to use and that is nice. You only need to read one thing, not a whole text that you need to go through. These are short things, short questions and it goes well.”(Male, 73)
“Well yes, I thought it was easy because I told you I do not do anything else (with the computer) and this was very easy that I had to fill out something and go to the next page.”(Female, 66)
“It is simple and in fact I do not think that is bad, because we are constantly overwhelmed with websites with colours and commercials and other things, I liked it, it was simple but good.”(Male, 70)
“I really liked this! Yes, yes, very good, simple and it has a positive and playful character … It was not presented as a purely scientific thing … something of which you think “what are they sending me?” No, it is nicely made and remains attractive.”(Male, 61)
“I think the length was good. It should not be too long, because then you will be less interested of course. Succinctly like they say and that is how it was.”(Male, 69)
“The time? Oh, that is very doable! You don’t need to spend much time going through the website and then you are finished and you print your plan then it is done. No, no, initially you need to spend a little time on it, but is not worth to talk about that.”(Male, 73)
3.3.3. Knowledge
“Healthy body, healthy mind, it goes together. Because if you feel well, then you will not worry about things that are not good. So if you feel good, by letting your blood circulate by standing up and those things, for example taking the stairs, than you will also feel better on the mental level. That is absolutely true.”(Male, 61)
“On a mental level it absolutely does (have an effect). On the physical level I have not… I have not really experienced it yet.”(Male, 73)
3.3.4. Social Support
“I showed it to my husband and told him that I need to move more, because he is of course more physically active than me.”(Female, 66)
“Yes, sometimes he watched along … I found it interesting. I got a lot of support from that. Yes, by filling it out together. And well … when I had to do something he stimulated me. “It is evening, you need to cycle now” he said. Sometimes I did not feel like doing it, but he said “Come on, you made a promise, you made a deal, you need to do it.””(Female, 57)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- IDF. IDF Diabetes Atlas, 8th ed.; International Diabetes Federation: Brussels, Belgium, 2017; Available online: http://www.diabetesatlas.org/ (accessed on 22 April 2018).
- Balducci, S.; Zanuso, S.; Cardelli, P.; Salvi, L.; Mazzitelli, G.; Bazuro, A.; Iacobini, C.; Nicolucci, A.; Pugliese, G.; the Italian Diabetes Exercise Study (IDES) Investigators. Changes in Physical Fitness Predict improvements in Modifiable Cardiovascular Risk Factors Independently of Body Weight Loss in Subjects with Type 2 Diabetes Participating in the Italian Diabetes and Exercise Study (IDES). Diabetes Care 2012, 35, 1347–1354. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, P.C.; Owen, N.; Yates, T.E.; Kingwell, B.A.; Dunstan, D.W. Sitting Less and Moving More: Improved Glycaemic Control for Type 2 Diabetes Prevention and Management. Curr. Diabetes Rep. 2016, 16, 114. [Google Scholar] [CrossRef] [PubMed]
- Colberg, S.R.; Sigal, R.J.; Fernhall, B.; Regensteiner, J.G.; Blissmer, B.J.; Rubin, R.R.; Chasan-Taber, L.; Albright, A.L.; Braun, B.; FACSM. Exercise and Type 2 Diabetes. The American College of Sports Medicine and the American Diabetes Association: Joint position statement executive summary. Diabetes Care 2010, 33, 2692–2696. [Google Scholar] [CrossRef] [PubMed]
- Gary, T.L.; Genkinger, J.M.; Guallar, E.; Peyrot, M.; Brancati, F.L. Meta-Analysis of Randomized Educational and Behavioral Interventions in Type 2 Diabetes. Diabetes Educ. 2003, 29, 488–501. [Google Scholar] [CrossRef] [PubMed]
- El-Gayar, O.; Timsina, P.; Nawar, N.; Eid, W. A systematic review of IT for diabetes self-management: Are we there yet? Int. J. Med Inf. 2013, 82, 637–652. [Google Scholar] [CrossRef] [PubMed]
- Vandelanotte, C.; Müller, A.M.; Short, C.E.; Hingle, M.; Nathan, N.; Williams, S.L.; Lopez, M.L.; Parekh, S.; Maher, C.A. Past, Present, and Future of eHealth and mHealth Research to Improve Physical Activity and Dietary Behaviors. J. Nutr. Educ. Behav. 2016, 48, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Pal, K.; Eastwood, S.V.; Michie, S.; Farmer, A.J.; Barnard, M.L.; Peacock, R.; Wood, B.; Inniss, J.D.; Murray, E. Computer-based diabetes self-management interventions for adults with type 2 diabetes mellitus. Cochrane Database Syst. Rev. 2013, 6, 119–120. [Google Scholar]
- Cui, M.; Wu, X.; Mao, J.; Wang, X.; Nie, M. T2DM Self-Management via Smartphone Applications: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0166718. [Google Scholar] [CrossRef] [PubMed]
- Eysenbach, G. The Law of Attrition. J. Med. Internet Res. 2005, 7, e11. [Google Scholar] [CrossRef] [PubMed]
- Van der Mispel, C.; Poppe, L.; Crombez, G.; Verloigne, M.; De Bourdeaudhuij, I. A Self-Regulation-Based eHealth Intervention to Promote a Healthy Lifestyle: Investigating User and Website Characteristics Related to Attrition. J. Med. Internet Res. 2017, 19, e241. [Google Scholar] [CrossRef] [PubMed]
- Yardley, L.; Morrison, L.G.; Andreou, P.; Joseph, J.; Little, P. Understanding reactions to an internet-delivered health-care intervention: Accommodating user preferences for information provision. BMC Med. Inf. Decis. Mak. 2010, 10, 10. [Google Scholar] [CrossRef] [PubMed]
- Maes, S.; Karoly, P. Self-Regulation Assessment and Intervention in Physical Health and Illness: A Review. Appl. Psychol. Health Well Being 2005, 54, 267–299. [Google Scholar] [CrossRef]
- Plaete, J.; De Bourdeaudhuij, I.; Verloigne, M.; Crombez, G. Acceptability, feasibility and effectiveness of an eHealth behaviour intervention using self-regulation: ‘MyPlan’. Patient Educ. Couns. 2015, 98, 1617–1624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsieh, H.-F.; Shannon, S.E. Three Approaches to Qualitative Content Analysis. Qualitative Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- International Diabetes Federation. IDF Diabetes Atlas 2013 n.d. Available online: www.idf.org/diabetesatlas (accessed on 22 April 2018).
- Zaphiris, P.; Kurniawan, S.; Ghiawadwala, M. A systematic approach to the development of research-based web design guidelines for older people. Univers. Access Inf. Soc. 2007, 6, 59. [Google Scholar] [CrossRef]
- Sniehotta, F.F.; Scholz, U.; Schwarzer, R. Action plans and coping plans for physical exercise: A longitudinal intervention study in cardiac rehabilitation. Br. J. Health Psychol. 2006, 11, 23–37. [Google Scholar] [CrossRef] [PubMed]
- Haug, S.; Meyer, C.; Dymalski, A.; Lippke, S.; John, U. Efficacy of a text messaging (SMS) based smoking cessation intervention for adolescents and young adults: Study protocol of a cluster randomised controlled trial. BMC Public Health 2012, 12, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aittasalo, M.; Rinne, M.; Pasanen, M.; Kukkonen-Harjula, K.; Vasankari, T. Promoting walking among office employees—Evaluation of a randomized controlled intervention with pedometers and e-mail messages. BMC Public Health 2012, 12, 403. [Google Scholar] [CrossRef] [PubMed]
- Kadirvelu, A.; Sadasivan, S.; Ng, S.H. Social support in type II diabetes care: A case of too little, too late. Diabetes Metab. Syndr. Obes. Target Ther. 2012, 5, 407–417. [Google Scholar] [CrossRef] [PubMed]
- Van Dyck, D.; De Greef, K.; Deforche, B.; Ruige, J.; Tudor-Locke, C.E.; Kaufman, J.-M.; Owen, N.; De Bourdeaudhuij, I. Mediators of physical activity change in a behavioral modification program for type 2 diabetes patients. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nordfeldt, S.; Hanberger, L.; Berterö, C. Patient and Parent Views on a Web 2.0 Diabetes Portal—The Management Tool, the Generator, and the Gatekeeper: Qualitative Study. J. Med. Internet Res. 2010, 12, e17. [Google Scholar] [CrossRef] [PubMed]
- Van der Vaart, R.; Drossaert, C.H.C.; de Heus, M.; Taal, E.; van de Laar, M.A.F.J. Measuring Actual eHealth Literacy Among Patients With Rheumatic Diseases: A Qualitative Analysis of Problems Encountered Using Health 1.0 and Health 2.0 Applications. J. Med. Internet Res. 2013, 15, e27. [Google Scholar] [CrossRef] [PubMed]
- Vandelanotte, C.; Spathonis, K.M.; Eakin, E.G.; Owen, N. Website-delivered physical activity interventions: A review of the literature. Am. J. Prev. Med. 2007, 33, 54–64. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Demographics | N (%) | Mean | SD | Range |
|---|---|---|---|---|
| Age in years | 65.86 | 5.6 | 57–81 | |
| Women | 8 (38.1) | |||
Level of education
| 2 (9.5) 9 (42.9) 10 (47.6) | |||
Marital status
| 15 (71.4) 2 (9.5) 2 (9.5) 2 (9.5) | |||
| Time since diagnosis in months | 183.3 | 155.1 | 4–480 | |
| BMI * in kg/m2 | 30.8 | 6.1 | 22.1–42.5 |
| Session Number | Mean Time Spent (SD; Range) | Number of Participants Visiting Optional Pages (%) |
|---|---|---|
| Session 1 | 22.2 (10.8; 9–46) | 15 (71.4) |
| Session 2 | 7.1 (4.4; 2–19) | 13 (61.9) |
| Session 3 | 6.8 (4.3; 2–21) | 18 (85.7) |
| Session 4 | 6.0 (3.8; 1–15) | 13 (61.9) |
| Session 5 | 6.5 (6.3; 1–30) | 17 (81.0) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poppe, L.; Crombez, G.; De Bourdeaudhuij, I.; Van der Mispel, C.; Shadid, S.; Verloigne, M. Experiences and Opinions of Adults with Type 2 Diabetes Regarding a Self-Regulation-Based eHealth Intervention Targeting Physical Activity and Sedentary Behaviour. Int. J. Environ. Res. Public Health 2018, 15, 954. https://doi.org/10.3390/ijerph15050954
Poppe L, Crombez G, De Bourdeaudhuij I, Van der Mispel C, Shadid S, Verloigne M. Experiences and Opinions of Adults with Type 2 Diabetes Regarding a Self-Regulation-Based eHealth Intervention Targeting Physical Activity and Sedentary Behaviour. International Journal of Environmental Research and Public Health. 2018; 15(5):954. https://doi.org/10.3390/ijerph15050954
Chicago/Turabian StylePoppe, Louise, Geert Crombez, Ilse De Bourdeaudhuij, Celien Van der Mispel, Samyah Shadid, and Maïté Verloigne. 2018. "Experiences and Opinions of Adults with Type 2 Diabetes Regarding a Self-Regulation-Based eHealth Intervention Targeting Physical Activity and Sedentary Behaviour" International Journal of Environmental Research and Public Health 15, no. 5: 954. https://doi.org/10.3390/ijerph15050954