Risk Factors and Spatial Clusters of Cryptosporidium Infection among School-Age Children in a Rural Region of Eastern China

Abstract
:1. Introduction
2. Materials and Methods
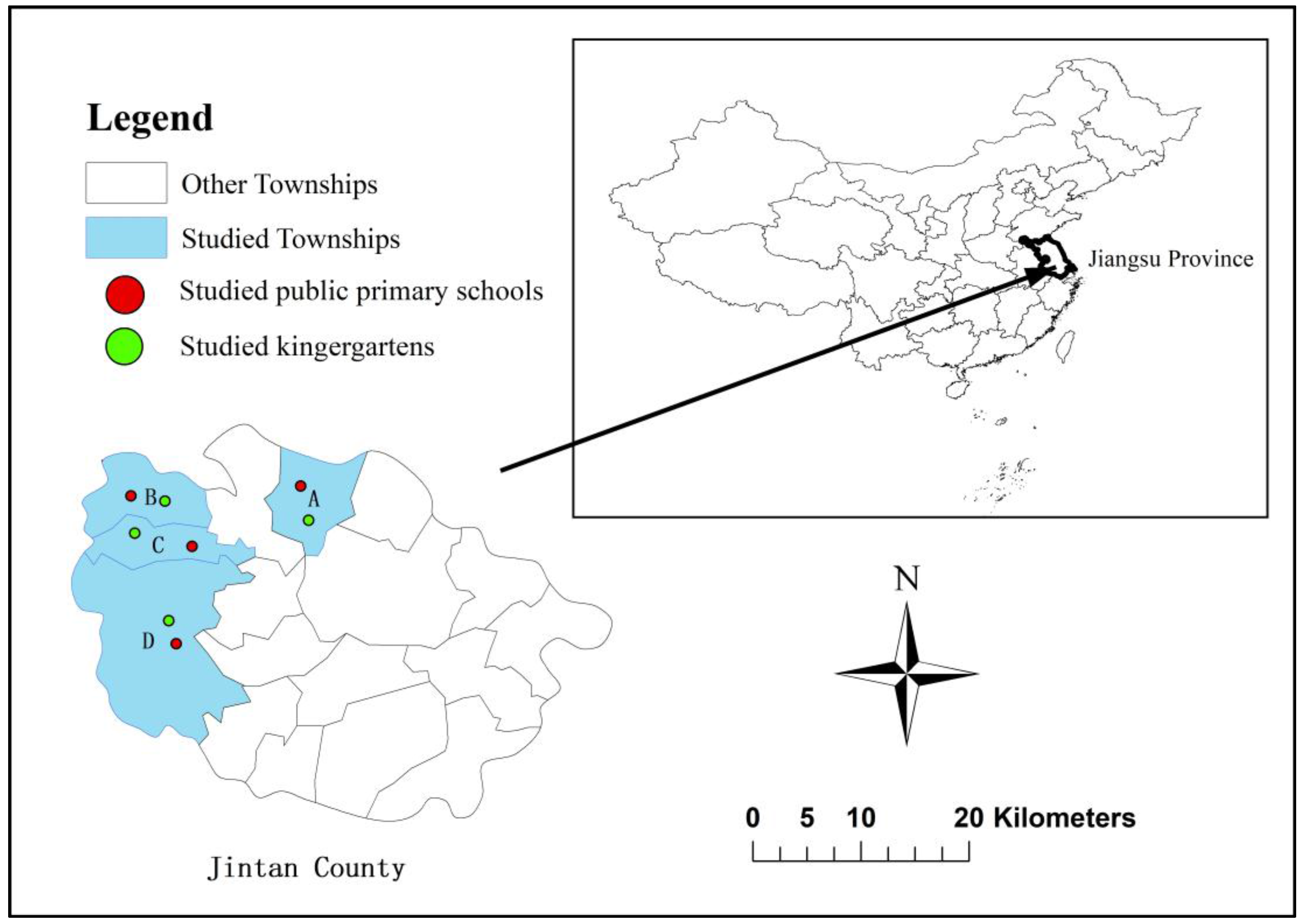
2.1. Study Area
2.2. Data Collection
2.3. Descriptive and Risk Factors Analysis
2.4. Cluster Analysis and Spatial Visualization
3. Results
3.1. Characteristics of the Participants
3.2. Prevalence and Risk Factors Associated with Cryptosporidium Infection
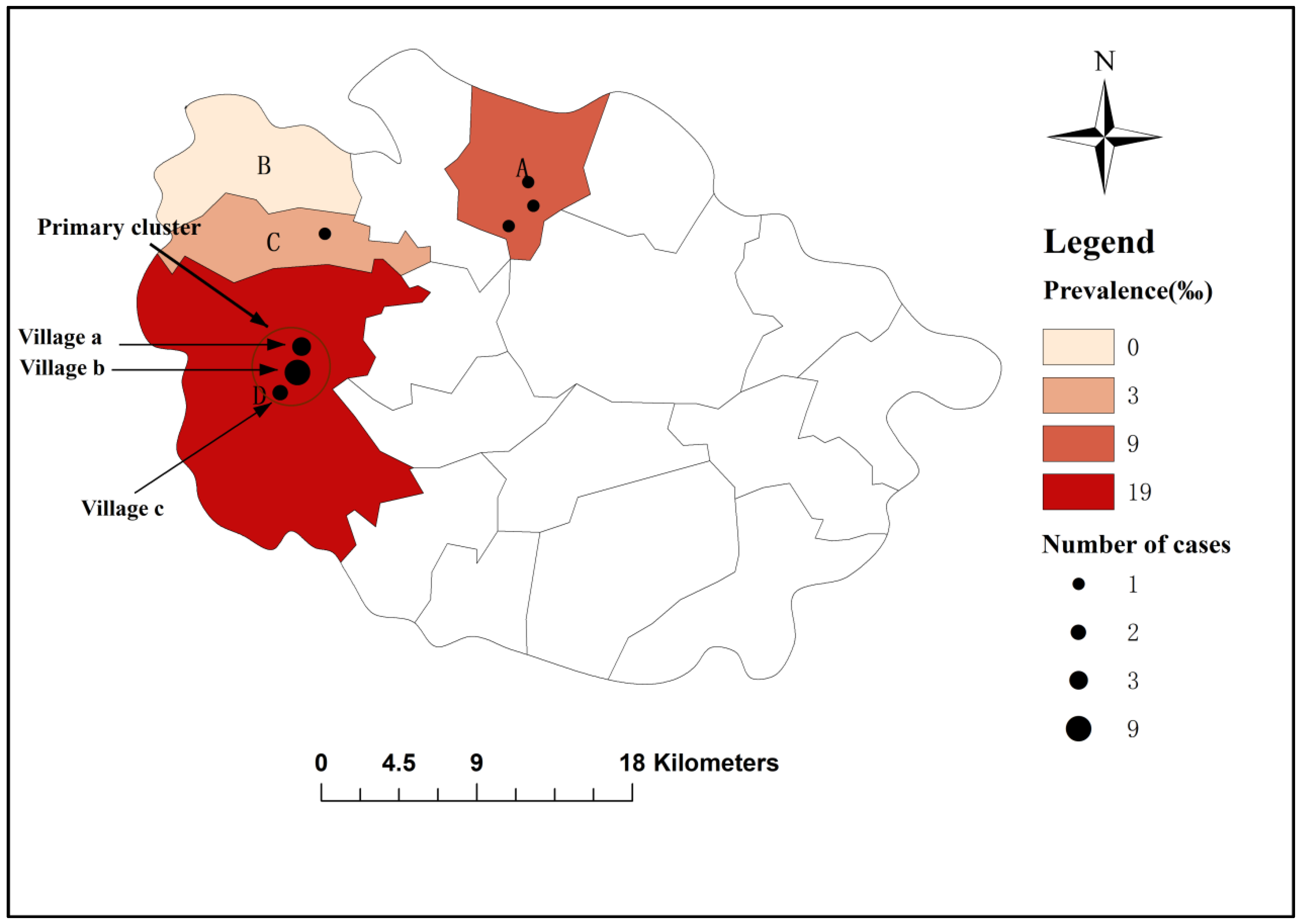
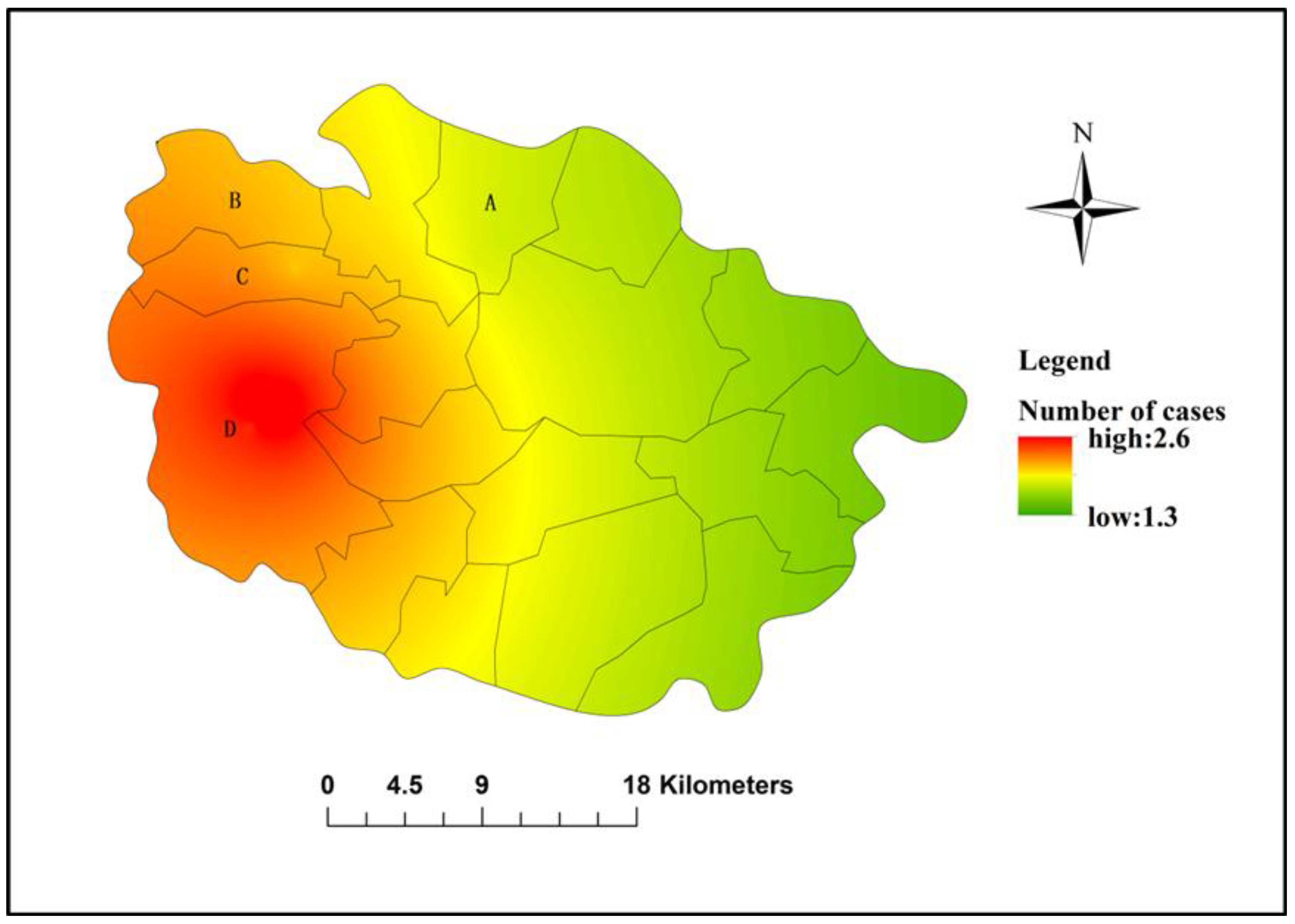
3.3. Cluster Analysis and Spatial Visualization
3.4. Association of Cryptosporidium Infection with Gastrointestinal Symptoms
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
Abbreviations
| OR | Odds Ratios |
| CI | Confidence Intervals |
| CDC | Center for Disease Control and Prevention |
| cOR | crude Odds Ratios |
| aOR | adjusted Odds Ratios |
| EBK | Empirical Bayesian Kriging |
| RR | Relative Risk |
References
- White, A.C., Jr. Cryptosporidiosis and the ears of the hippopotamus. Clin. Infect. Dis. 2010, 50, 1373–1374. [Google Scholar] [PubMed]
- Mahmoudi, M.R.; Ongerth, J.E.; Karanis, P. Cryptosporidium and cryptosporidiosis: The Asian perspective. Int. J. Hyg. Environ. Health 2017, 220, 1098–1109. [Google Scholar] [CrossRef] [PubMed]
- Laupland, K.B.; Church, D.L. Population-based laboratory surveillance for Giardia sp. and Cryptosporidium sp. Infections in a large canadian health region. BMC Infect. Dis. 2005, 5, 72. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.M.; Keithly, J.S.; Paya, C.V.; LaRusso, N.F. Cryptosporidiosis. N. Engl. J. Med. 2002, 346, 1723–1731. [Google Scholar] [CrossRef] [PubMed]
- Mor, S.M.; Tzipori, S. Cryptosporidiosis in children in sub-saharan africa: A lingering challenge. Clin. Infect. Dis. 2008, 47, 915–921. [Google Scholar] [CrossRef] [PubMed]
- Tumwine, J.K.; Kekitiinwa, A.; Nabukeera, N.; Akiyoshi, D.E.; Rich, S.M.; Widmer, G.; Feng, X.; Tzipori, S. Cryptosporidium parvum in children with diarrhea in Mulago hospital, Kampala, Uganda. Am. J. Trop. Med. Hyg. 2003, 68, 710–715. [Google Scholar] [PubMed]
- Kotloff, K.L.; Nataro, J.P.; Blackwelder, W.C.; Nasrin, D.; Farag, T.H.; Panchalingam, S.; Wu, Y.; Sow, S.O.; Sur, D.; Breiman, R.F.; et al. Burden and aetiology of diarrhoeal disease in infants and young children in developing countries (the global enteric multicenter study, gems): A prospective, case-control study. Lancet 2013, 382, 209–222. [Google Scholar] [CrossRef]
- Checkley, W.; Epstein, L.D.; Gilman, R.H.; Black, R.E.; Cabrera, L.; Sterling, C.R. Effects of cryptosporidium parvum infection in Peruvian children: Growth faltering and subsequent catch-up growth. Am. J. Epidemiol. 1998, 148, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Agnew, D.G.; Lima, A.A.; Newman, R.D.; Wuhib, T.; Moore, R.D.; Guerrant, R.L.; Sears, C.L. Cryptosporidiosis in northeastern Brazilian children: Association with increased diarrhea morbidity. J. Infect. Dis. 1998, 177, 754–760. [Google Scholar] [CrossRef] [PubMed]
- Checkley, W.; White, A.C., Jr.; Jaganath, D.; Arrowood, M.J.; Chalmers, R.M.; Chen, X.M.; Fayer, R.; Griffiths, J.K.; Guerrant, R.L.; Hedstrom, L.; et al. A review of the global burden, novel diagnostics, therapeutics, and vaccine targets for Cryptosporidium. Lancet Infect. Dis. 2015, 15, 85–94. [Google Scholar] [CrossRef]
- Han, F.; Tan, W.X.; Zhou, X.L. Two case reports of cryptosporidiosis in Nanjing. Jiangsu Med. J. 1987, 13, 692. [Google Scholar]
- Lv, S.; Tian, L.G.; Liu, Q.; Qian, M.B.; Fu, Q.; Steinmann, P.; Chen, J.X.; Yang, G.J.; Yang, K.; Zhou, X.N. Water-related parasitic diseases in China. Int. J. Environ. Res. Public Health 2013, 10, 1977–2016. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Ren, J.; Yuan, Z.; Liu, A.; Zhao, H.; Liu, H.; Chu, L.; Pan, W.; Cao, J.; Lin, Y.; et al. Cryptosporidium andersoni as a novel predominant Cryptosporidium species in outpatients with diarrhea in jiangsu province, China. BMC Infect. Dis. 2014, 14, 555. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Shen, Y.; Yin, J.; Yuan, Z.; Jiang, Y.; Xu, Y.; Pan, W.; Hu, Y.; Cao, J. Prevalence and genetic characterization of Cryptosporidium, enterocytozoon, giardia and cyclospora in diarrheal outpatients in China. BMC Infect. Dis. 2014, 14, 25. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.; Li, F.; Zeng, Z.; Huang, Z.; Fan, Z.; Jin, Y.; Luo, W.; Xiang, X.; Deng, Q. Prevalence and clinical significance of Cryptosporidium infection in patients with hepatitis b virus-associated acute-on-chronic liver failure. Int. J. Infect. Dis. 2011, 15, e845–848. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.X.; Li, C.P.; Wang, J.; Pan, B.R. Epidemiological survey of cryptosporidiosis in Anhui province China. World J. Gastroenterol. 2002, 8, 371–374. [Google Scholar] [CrossRef] [PubMed]
- Muchiri, J.M.; Ascolillo, L.; Mugambi, M.; Mutwiri, T.; Ward, H.D.; Naumova, E.N.; Egorov, A.I.; Cohen, S.; Else, J.G.; Griffiths, J.K. Seasonality of Cryptosporidium oocyst detection in surface waters of meru, kenya as determined by two isolation methods followed by pcr. J. Water Health 2009, 7, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Jagai, J.S.; Castronovo, D.A.; Monchak, J.; Naumova, E.N. Seasonality of cryptosporidiosis: A meta-analysis approach. Environ. Res. 2009, 109, 465–478. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Li, C.P. The survey of cryptosporidium infection among young children in kindergartens in Anhui province. Zhongguo Ji Sheng Chong Xue Yu Ji Sheng Chong Bing Za Zhi 2004, 22, 331–333. [Google Scholar] [CrossRef]
- Chen, Y.G.; Yao, F.B.; Li, H.S.; Shi, W.S.; Dai, M.X.; Lu, M. Cryptosporidium infection and diarrhea in rural and urban areas of jiangsu, people's republic of china. J. Clin. Microbiol. 1992, 30, 492–494. [Google Scholar] [PubMed]
- Yang, Y.; Zhou, Y.B.; Xiao, P.L.; Shi, Y.; Chen, Y.; Liang, S.; Yihuo, W.L.; Song, X.X.; Jiang, Q.W. Prevalence of and risk factors associated with cryptosporidium infection in an underdeveloped rural community of southwest China. Infect. Dis. Poverty 2017, 6, 2. [Google Scholar] [CrossRef] [PubMed]
- Al-Delaimy, A.K.; Al-Mekhlafi, H.M.; Nasr, N.A.; Sady, H.; Atroosh, W.M.; Nashiry, M.; Anuar, T.S.; Moktar, N.; Lim, Y.A.; Mahmud, R. Epidemiology of intestinal polyparasitism among orang asli school children in rural Malaysia. PLoS Negl. Trop. Dis. 2014, 8, e3074. [Google Scholar] [CrossRef] [PubMed]
- Wegayehu, T.; Adamu, H.; Petros, B. Prevalence of giardia duodenalis and cryptosporidium species infections among children and cattle in north Shewa zone, Ethiopia. BMC Infect. Dis. 2013, 13, 419. [Google Scholar] [CrossRef] [PubMed]
- de Lucio, A.; Amor-Aramendia, A.; Bailo, B.; Saugar, J.M.; Anegagrie, M.; Arroyo, A.; Lopez-Quintana, B.; Zewdie, D.; Ayehubizu, Z.; Yizengaw, E.; et al. Prevalence and genetic diversity of giardia duodenalis and Cryptosporidium spp. Among school children in a rural area of the Amhara region, north-west Ethiopia. PLoS ONE 2016, 11, e0159992. [Google Scholar] [CrossRef] [PubMed]
- Quihui-Cota, L.; Morales-Figueroa, G.G.; Javalera-Duarte, A.; Ponce-Martinez, J.A.; Valbuena-Gregorio, E.; Lopez-Mata, M.A. Prevalence and associated risk factors for giardia and cryptosporidium infections among children of northwest Mexico: A cross-sectional study. BMC Public Health 2017, 17, 852. [Google Scholar] [CrossRef] [PubMed]
- Ajjampur, S.S.; Liakath, F.B.; Kannan, A.; Rajendran, P.; Sarkar, R.; Moses, P.D.; Simon, A.; Agarwal, I.; Mathew, A.; O’Connor, R.; et al. Multisite study of cryptosporidiosis in children with diarrhea in India. J. Clin. Microbiol. 2010, 48, 2075–2081. [Google Scholar] [CrossRef] [PubMed]
- Al-Mohammed, H.I.; Amin, T.T.; Aboulmagd, E.; Hablus, H.R.; Zaza, B.O. Prevalence of intestinal parasitic infections and its relationship with socio–demographics and hygienic habits among male primary schoolchildren in Al–Ahsa, Saudi Arabia. Asian Pac. J. Trop. Med. 2010, 3, 906–912. [Google Scholar] [CrossRef]
- Speich, B.; Croll, D.; Furst, T.; Utzinger, J.; Keiser, J. Effect of sanitation and water treatment on intestinal protozoa infection: A systematic review and meta-analysis. Lancet Infect. Dis. 2016, 16, 87–99. [Google Scholar] [CrossRef]
- Wani, S.A.; Ahmad, F.; Zargar, S.A.; Ahmad, Z.; Ahmad, P.; Tak, H. Prevalence of intestinal parasites and associated risk factors among schoolchildren in Srinagar city, Kashmir, India. J. Parasitol. 2007, 93, 1541–1543. [Google Scholar] [CrossRef] [PubMed]
- Chin, Y.T.; Lim, Y.A.; Chong, C.W.; Teh, C.S.; Yap, I.K.; Lee, S.C.; Tee, M.Z.; Siow, V.W.; Chua, K.H. Prevalence and risk factors of intestinal parasitism among two indigenous sub-ethnic groups in Peninsular Malaysia. Infect. Dis. Poverty 2016, 5, 77. [Google Scholar] [CrossRef] [PubMed]
- Checkley, W.; Gilman, R.H.; Epstein, L.D.; Suarez, M.; Diaz, J.F.; Cabrera, L.; Black, R.E.; Sterling, C.R. Asymptomatic and symptomatic cryptosporidiosis: Their acute effect on weight gain in Peruvian children. Am. J. Epidemiol. 1997, 145, 156–163. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | No. of Participants | % |
|---|---|---|
| Total | 1637 | 100 |
| Gender | ||
| Male | 864 | 52.8 |
| Female | 773 | 47.2 |
| Age (years) | ||
| 3–6 | 863 | 52.7 |
| 7–9 | 774 | 47.3 |
| Location (Township) | ||
| A | 330 | 20.2 |
| B | 242 | 14.8 |
| C | 324 | 19.8 |
| D | 741 | 45.3 |
| Supplied with piped water | ||
| Yes | 1594 | 97.4 |
| No | 43 | 2.6 |
| Presence of toilets at household | ||
| Yes | 1580 | 96.5 |
| No | 57 | 3.5 |
| Raising livestock or poultry (e.g., cattle, sheep, chicken) | ||
| Yes | 756 | 46.2 |
| No | 881 | 53.8 |
| Contact with pets (e.g., dog, cat) | ||
| Yes | 416 | 25.4 |
| No | 1221 | 74.6 |
| Variables | Examined n | Infected n (‰) | cOR (95% Cl) | p | aOR (95% Cl) | p |
|---|---|---|---|---|---|---|
| Gender | ||||||
| Male | 864 | 8 (9) | 0.713 (0.280–1.815) | 0.476 | 0.713(0.278–1.828) | 0.481 |
| Female | 773 | 10 (13) | 1 | |||
| Age (years) | ||||||
| 3–6 | 863 | 14 (16) | 3.175 (1.041–9.709) | 0.032 | 3.072 (1.001–9.427) | 0.050 |
| 7–9 | 774 | 4 (5) | 1 | |||
| Location (Township) | ||||||
| A | 330 | 3 (9) | 1.00 | 0.031 | 1 | 0.244 |
| B | 242 | 0 (0) | 0.00 | 0.266 | 0.00 | 0.995 |
| C | 324 | 1 (3) | 0.337 (0.035–3.261) | 0.624 | 0.354 (0.036–3.438) | 0.371 |
| D | 741 | 14 (19) | 2.099 (0.599–7.354) | 0.236 | 2.196 (0.624–7.734) | 0.221 |
| Supplied with piped water | ||||||
| No | 43 | 0 (0.0) | 0.00 | 1.000 | ||
| Yes | 1594 | 18 (11) | 1 | |||
| Presence of toilets at household | ||||||
| Yes | 1580 | 17 (11) | 0.609 (0.080–4.651) | 0.473 | ||
| No | 57 | 1 (18) | 1 | |||
| Raising livestock or poultry | ||||||
| Yes | 756 | 7 (9) | 0.739 (0.285–1.915) | 0.533 | ||
| No | 881 | 11 (12) | 1 | |||
| Contact with pets (e.g., dog, cat) | ||||||
| Yes | 416 | 3 (7) | 0.584 (0.168–2.028) | 0.559 | ||
| No | 1221 | 15 (12) | 1 | |||
| Boiling water before drinking | ||||||
| Yes | 1361 | 15 (11) | 1.014 (0.292–3.521) | 1.000 | ||
| No | 276 | 3 (11) | 1 | |||
| Swimming in one month | ||||||
| Yes | 104 | 1 (10) | 0.866 (0.114–6.579) | 1.000 | ||
| No | 1533 | 17 (11) | 1 | |||
| Travelling in six months | ||||||
| Yes | 269 | 2 (7) | 0.632 (0.145–2.770) | 0.770 | ||
| No | 1368 | 16 (12) | 1 | |||
| Contact with water facilities in one month | ||||||
| Yes | 74 | 0 (0) | 0.00 | 1.000 | ||
| No | 1563 | 18 (12) | 1 | |||
| Contact with a person with diarrhea in three months | ||||||
| Yes | 264 | 4 (15) | 1.492 (0.488–4.566) | 0.700 | ||
| No | 1373 | 14 (10) | 1 | |||
| Washing hands before eating and after defecation | ||||||
| No | 753 | 13 (17) | 3.088 (1.096–8.703) | 0.025 | 3.003 (1.060–8.511) | 0.039 |
| Yes | 884 | 5 (6) | 1 | |||
| Cluster | Radius (km) | Number of Observed Cases | Number of Expected Cases | Population | RR | p |
|---|---|---|---|---|---|---|
| Primary | 2.86 | 14 | 8.16 | 15602 | 4.220 | 0.025 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zheng, H.; He, J.; Wang, L.; Zhang, R.; Ding, Z.; Hu, W. Risk Factors and Spatial Clusters of Cryptosporidium Infection among School-Age Children in a Rural Region of Eastern China. Int. J. Environ. Res. Public Health 2018, 15, 924. https://doi.org/10.3390/ijerph15050924
Zheng H, He J, Wang L, Zhang R, Ding Z, Hu W. Risk Factors and Spatial Clusters of Cryptosporidium Infection among School-Age Children in a Rural Region of Eastern China. International Journal of Environmental Research and Public Health. 2018; 15(5):924. https://doi.org/10.3390/ijerph15050924
Chicago/Turabian StyleZheng, Hao, Jianfeng He, Li Wang, Rong Zhang, Zhen Ding, and Wenbiao Hu. 2018. "Risk Factors and Spatial Clusters of Cryptosporidium Infection among School-Age Children in a Rural Region of Eastern China" International Journal of Environmental Research and Public Health 15, no. 5: 924. https://doi.org/10.3390/ijerph15050924