Glucose Gel as a Potential Alternative Treatment to Infant Formula for Neonatal Hypoglycaemia in Australia


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
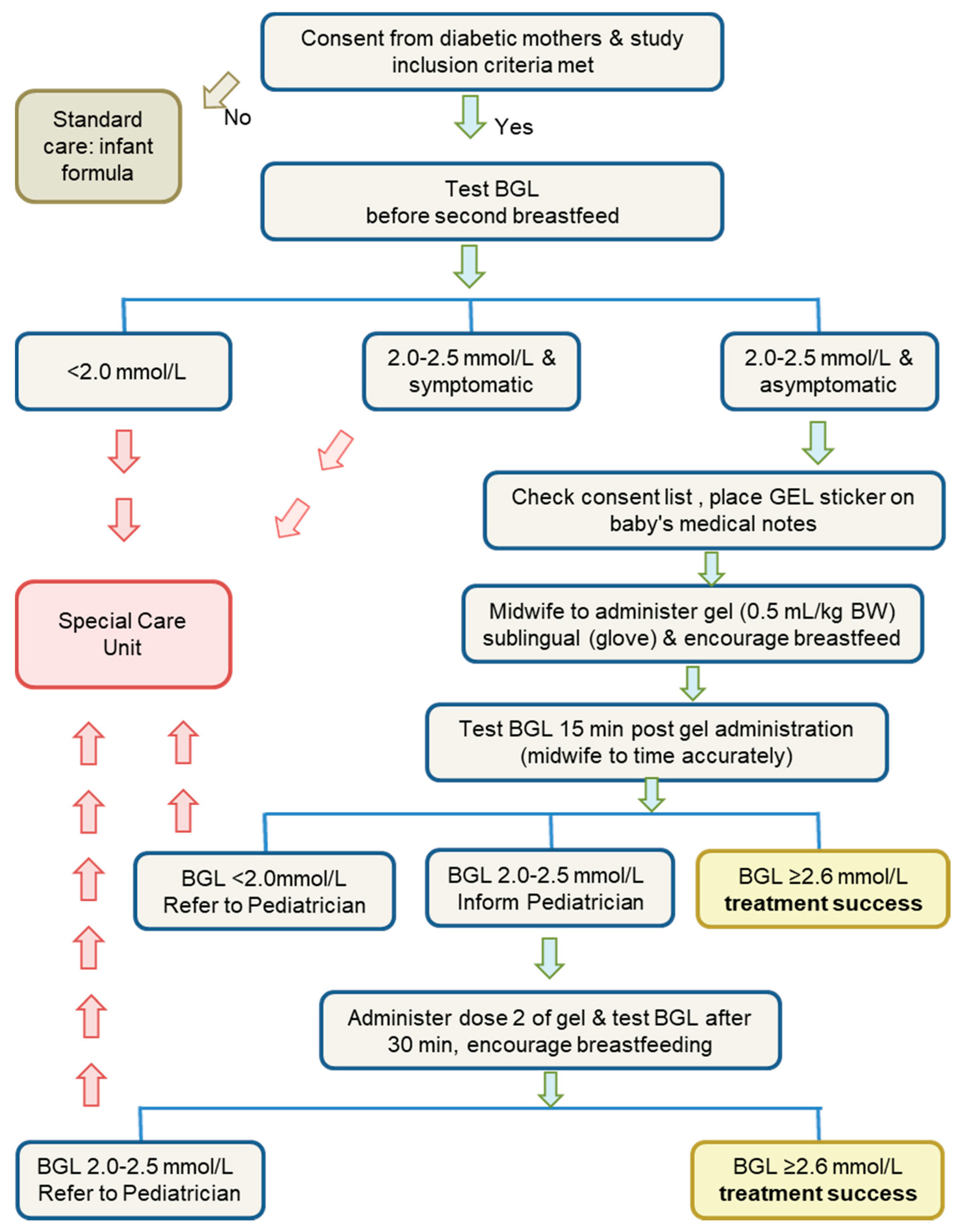
2.2. Protocol
2.3. Approval
2.4. Statistical Analysis
3. Results
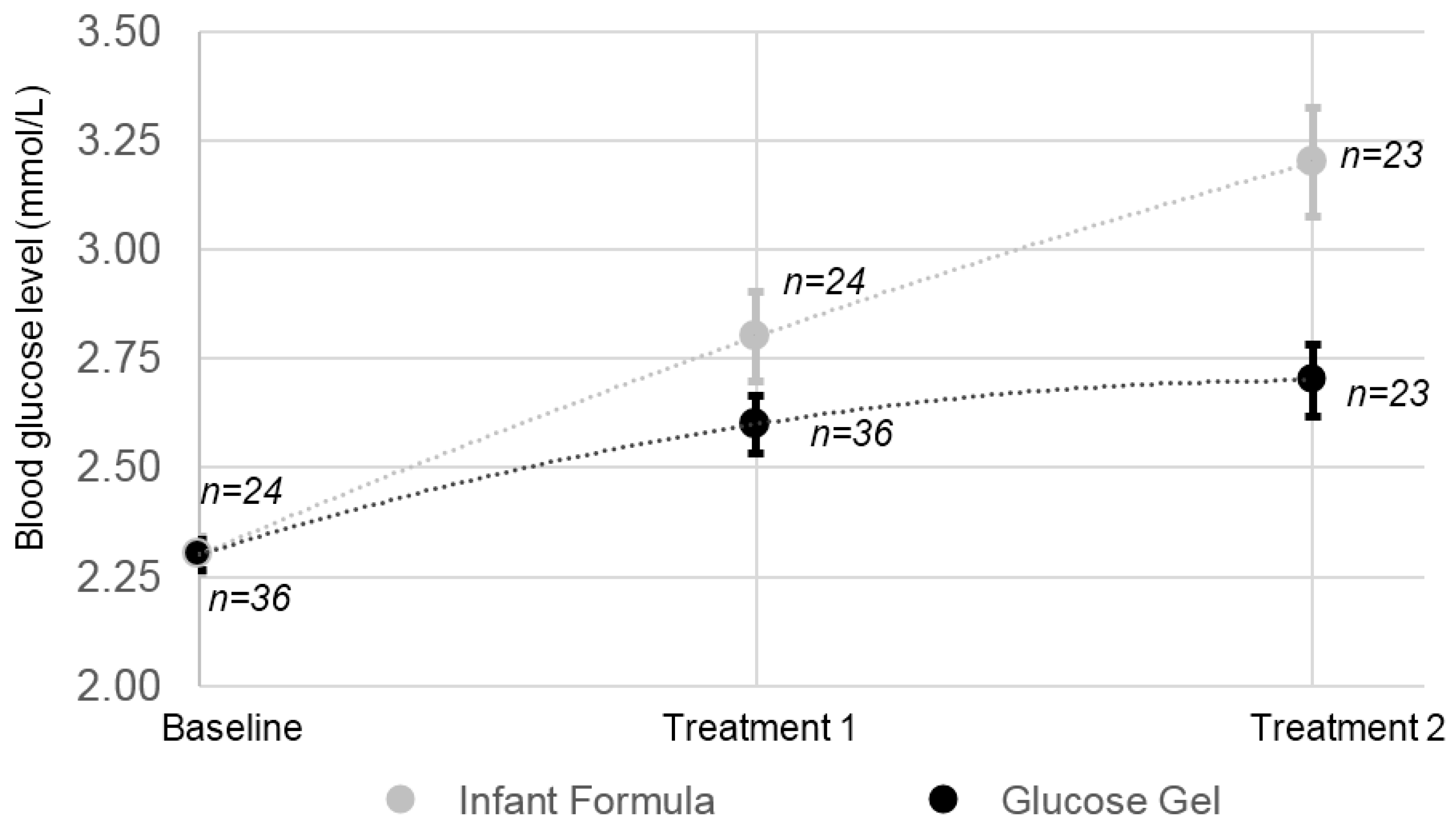
3.1. BGL Response to Treatments
3.2. Time to Normoglycemia
3.3. Special Care Nursery Admission
3.4. Adverse Reactions
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Hay, W.; Cornblath, M. Historical perspectives: Transient symptomatic neonatal hypoglycemia. NeoReviews 2003, 4, e1–e5. [Google Scholar] [CrossRef]
- Rozance, P.J.; Hay, W.W. Neonatal Hypoglycemia—Answers, but More Questions. J. Pediatr. 2012, 161, 775–776. [Google Scholar] [CrossRef] [PubMed]
- Hay, W.W.; Raju, T.N.K.; Higgins, R.D.; Kalhan, S.C.; Devaskar, S.U. Knowledge Gaps and Research Needs for Understanding and Treating Neonatal Hypoglycemia: Workshop Report from Eunice Kennedy Shriver National Institute of Child Health and Human Development. J. Pediatr. 2009, 155, 612–617. [Google Scholar] [CrossRef] [PubMed]
- Stenninger, E.; Flink, R.; Eriksson, B.; Sahlen, C. Long term neurological dysfunction and neonatal hypoglycaemia after diabetic pregnancy. Arch. Dis. Child. Fetal Neonatal Ed. 1998, 79, F174–F179. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.F. Hypoglycaemia of the newborn: A review. Bull. World Health Organ. 1997, 75, 216–290. [Google Scholar]
- Harris, D.L.; Battin, M.R.; Weston, P.J.; Harding, J.E. Continuous glucose monitoring in newborn babies at risk of hypoglycemia. J. Pediatr. 2010, 157, 198–202.e191. [Google Scholar] [CrossRef] [PubMed]
- Rozance, P.J.; Hay, W.W. Describing hypoglycemia—Definition or operational threshold? Early Hum. Dev. 2010, 86, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Harris, D.L.; Weston, P.J.; Battin, M.R.; Harding, J.E. A survey of the management of neonatal hypoglycaemia within the Australian and New Zealand Neonatal Network. J. Paediatr. Child Health 2014, 50, E55–E62. [Google Scholar] [CrossRef] [PubMed]
- Rozance, P.; Hay, W. New approaches to management of neonatal hypoglycemia. Matern. Health Neonatol. Perinatol. 2016, 2, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Newnam, K.M.; Bunch, M. Glucose Gel as a Treatment Strategy for Transient Neonatal Hypoglycemia. Adv. Neonatal. Care 2017, 17, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Hewitt, V.; Watts, R.; Robertson, J.; Haddow, G. Nursing and midwifery management of hypoglycaemia in healthy term neonates. Int. J. Evid. Based Healthc. 2005, 3, 169–205. [Google Scholar] [PubMed]
- Women and Newborn Health Service. Metabolic Management: Neonatology Clinical Guidelines; King Edward Memorial Hospital: Perth, Australia, 2010.
- Haninger, N.C.; Farley, C.L. Screening for hypoglycemia in healthy term neonates: Effects on breastfeeding. J. Midwifery Womens Health 2001, 46, 292–301. [Google Scholar] [CrossRef]
- Bourchier, D.; Burke, T. Protocol: Hypoglycaemia in Neonates (Delivery Suite and Postnatal Wards); Waikato District Health Board: Hamilton, New Zealand, 2010. [Google Scholar]
- Barennes, H.; Pussard, E. Improving the management of dysglycemia in children in the developing world. Am. J. Trop. Med. Hyg. 2015, 92, 6–8. [Google Scholar] [CrossRef] [PubMed]
- Harris, D.L.; Gamble, G.D.; Weston, P.J.; Harding, J.E. What Happens to Blood Glucose Concentrations After Oral Treatment for Neonatal Hypoglycemia? J. Pediatr. 2017, 190, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Bourchier, D.; Weston, P.; Heron, P. Hypostop for neonatal hypoglycaemia. N. Z. Med. J. 1992, 105, 22. [Google Scholar] [PubMed]
- Ang, I.; Koh, T.; O’Halloran, M.; Berry, A. Oromucosal treatment of neonatal hypoglycaemia. J. Paediatr. Child Health 1991, 27, 128–129. [Google Scholar]
- Harris, D.L.; Weston, P.J.; Harding, J.E. Dextrose gel and infant formula are more effective than breast milk for reversing neonal hypoglycaemia. Pediatr. Res. 2011, 70, 651. [Google Scholar] [CrossRef]
- Harris, D.L.; Weston, P.J.; Signal, M.; Chase, J.G.; Harding, J.E. Dextrose gel for neonatal hypoglycaemia (the Sugar Babies Study): A randomised, double-blind, placebo-controlled trial. Lancet 2013, 382, 2077–2083. [Google Scholar] [CrossRef]
- Ter, M.; Halibullah, I.; Leung, L.; Jacobs, S. Implementation of dextrose gel in the management of neonatal hypoglycaemia. J. Paediatr. Child Health 2017, 53, 408–411. [Google Scholar] [CrossRef] [PubMed]
- Narang, N.; Sharma, J. Sublingual mucosa as a route for systemic drug delivery. Int. J. Pharm. Pharm. Sci. 2011, 3, 18–22. [Google Scholar]
- Barennes, H.; Willcox, M.L.; Graz, B.; Pussard, E. Sublingual sugar for infant hypoglycaemia. Lancet 2014, 383, 1208. [Google Scholar] [CrossRef]
- International Diabetes Federation. Diabetes Atlas; International Diabetes Federation: Brussels, Belgium, 2015. [Google Scholar]
- DSS Research Statistical Power Calculators. Available online: https://www.dssresearch.com/KnowledgeCenter/toolkitcalculators/statisticalpowercalculators.aspx (accessed on 28 March 2018).
- Hegarty, J.E.; Harding, J.E.; Gamble, G.D.; Crowther, C.A.; Edlin, R.; Alsweiler, J.M. Prophylactic Oral Dextrose Gel for Newborn Babies at Risk of Neonatal Hypoglycaemia: A Randomised Controlled Dose-Finding Trial (the Pre-hPOD Study). PLoS Med. 2016, 13, e1002155. [Google Scholar] [CrossRef] [PubMed]
- Bennett, C.; Fagan, E.; Chaharbakhshi, E.; Zamfirova, I.; Flicker, J. Implementing a Protocol Using Glucose Gel to Treat Neonatal Hypoglycemia. Nurs. Womens Health 2016, 20, 64–74. [Google Scholar] [CrossRef] [PubMed]
- Crenshaw, J. Care Practice #6: No Separation of Mother and Baby, With Unlimited Opportunities for Breastfeeding. J. Perinat. Educ. 2007, 16, 39–43. [Google Scholar] [PubMed]
- Harris, D.L.; Alsweiler, J.M.; Ansell, J.M.; Gamble, G.D.; Thompson, B.; Wouldes, T.A.; Yu, T.Y.; Harding, J.E. Outcome at 2 Years after Dextrose Gel Treatment for Neonatal Hypoglycemia: Follow-Up of a Randomized Trial. J. Pediatr. 2016, 170, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Rawat, M.; Chandrasekharan, P.; Turkovich, S.; Barclay, N.; Perry, K.; Schroeder, E.; Testa, L.; Lakshminrusimha, S. Oral Dextrose Gel Reduces the Need for Intravenous Dextrose Therapy in Neonatal Hypoglycemia. Biomed. Hub 2016, 1. [Google Scholar] [CrossRef] [PubMed]
- Weston, P.J.; Harris, D.L.; Battin, M.; Brown, J.; Hegarty, J.E.; Harding, J.E. Oral dextrose gel for the treatment of hypoglycaemia in newborn infants. In Cochrane Database of Systematic Reviews; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2016. [Google Scholar]
- McKinlay, C.J.; Alsweiler, J.M.; Ansell, J.M.; Anstice, N.S.; Chase, J.G.; Gamble, G.D.; Harris, D.L.; Jacobs, R.J.; Jiang, Y.; Paudel, N.; et al. Neonatal Glycemia and Neurodevelopmental Outcomes at 2 Years. N. Engl. J. Med. 2015, 373, 1507–1518. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Global Strategy on Infant and Young Child Feeding; WHO: Geneva, Switzerland, 2002. [Google Scholar]
- Wright, N. Hypoglycemia in breastfed neonates. Breastfeed. Med. 2006, 1, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Wight, N.; Marinelli, K.A. ABM clinical protocol #1: Guidelines for glucose monitoring and treatment of hypoglycemia in breastfed neonates. Breastfeed. Med. 2006, 1, 178–184. [Google Scholar] [PubMed]
- De Rooy, L.; Johns, A. Management of the vulnerable baby on the postnatal ward and transitional care unit. Early Hum. Dev. 2010, 86, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Stewart, C.E.; Sage, E.L.; Reynolds, P. Supporting ‘Baby Friendly’: A quality improvement initiative for the management of transitional neonatal hypoglycaemia. Arch. Dis. Child. Fetal Neonatal Ed. 2016, 101, F344–F347. [Google Scholar] [CrossRef] [PubMed]
- Barennes, H.; Valea, I.; Nagot, N.; Van de Perre, P.; Pussard, E. Sublingual sugar administration as an alternative to intravenous dextrose administration to correct hypoglycemia among children in the tropics. Pediatrics 2005, 116, e648–e653. [Google Scholar] [CrossRef] [PubMed]
- Women and Newborn Health Service. Oral Sucrose for Procedural Pain Relief. In Neonatology Clinical Guidelines; King Edward Memorial/Princess Margaret Hospitals: Perth, Australia, 2006. [Google Scholar]
- Stevens, B.; Yamada, J.; Ohlsson, A.; Haliburton, S.; Shorkey, A. Sucrose for analgesia in newborn infants undergoing painful procedures. Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef] [PubMed]
- Taddio, A.; Shah, V.; Hancock, R.; Smith, R.W.; Stephens, D.; Atenafu, E.; Beyene, J.; Koren, G.; Stevens, B.; Katz, J. Effectiveness of sucrose analgesia in newborns undergoing painful medical procedures. CMAJ 2008, 179, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Harding, J.E.; Hegarty, J.E.; Crowther, C.A.; Edlin, R.; Gamble, G.; Alsweiler, J.M. Randomised trial of neonatal hypoglycaemia prevention with oral dextrose gel (hPOD): Study protocol. BMC Pediatr. 2015, 15, 120. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Mean ± Standard Deviation | |||
|---|---|---|---|
| Infant Formula (n = 24) | Glucose Gel (n = 36) | p Value | |
| Gender (male) | 12 (50%) | 20 (55%) | 0.68 |
| Weight (g) | 3330 ± 392 | 3496 ± 518 | 0.16 |
| Range | 2870–4440 | 2665–4160 | |
| Gestational age (weeks) | 38 ± 0.72 | 38 ± 1.12 | 0.27 |
| Range | 37–40 | 36–40 | |
| Maternal age (years) | 33 ± 6 | 38 ± 1 | 0.27 |
| Range | 22–45 | 21–45 | |
| Type of maternal diabetes | |||
| Gestational | 22 (92%) | 24 (67%) | 0.03 |
| Type 1 | 1 (4%) | 4 (11%) | |
| Type 2 | 1 (4%) | 8 (22%) | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barber, R.L.; Ekin, A.E.; Sivakumar, P.; Howard, K.; O’Sullivan, T.A. Glucose Gel as a Potential Alternative Treatment to Infant Formula for Neonatal Hypoglycaemia in Australia. Int. J. Environ. Res. Public Health 2018, 15, 876. https://doi.org/10.3390/ijerph15050876
Barber RL, Ekin AE, Sivakumar P, Howard K, O’Sullivan TA. Glucose Gel as a Potential Alternative Treatment to Infant Formula for Neonatal Hypoglycaemia in Australia. International Journal of Environmental Research and Public Health. 2018; 15(5):876. https://doi.org/10.3390/ijerph15050876
Chicago/Turabian StyleBarber, Raenee L., Amy E. Ekin, Pushparani Sivakumar, Kay Howard, and Therese A. O’Sullivan. 2018. "Glucose Gel as a Potential Alternative Treatment to Infant Formula for Neonatal Hypoglycaemia in Australia" International Journal of Environmental Research and Public Health 15, no. 5: 876. https://doi.org/10.3390/ijerph15050876