Mercury Levels in Women and Children from Interior Villages in Suriname, South America

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Description of Surinamese Study Population
2.2. Mercury (Hg) Analysis in Hair
2.3. Hair/Blood Hg Concentrations and Hazard Quotient Estimation
2.4. Statistical Analyses
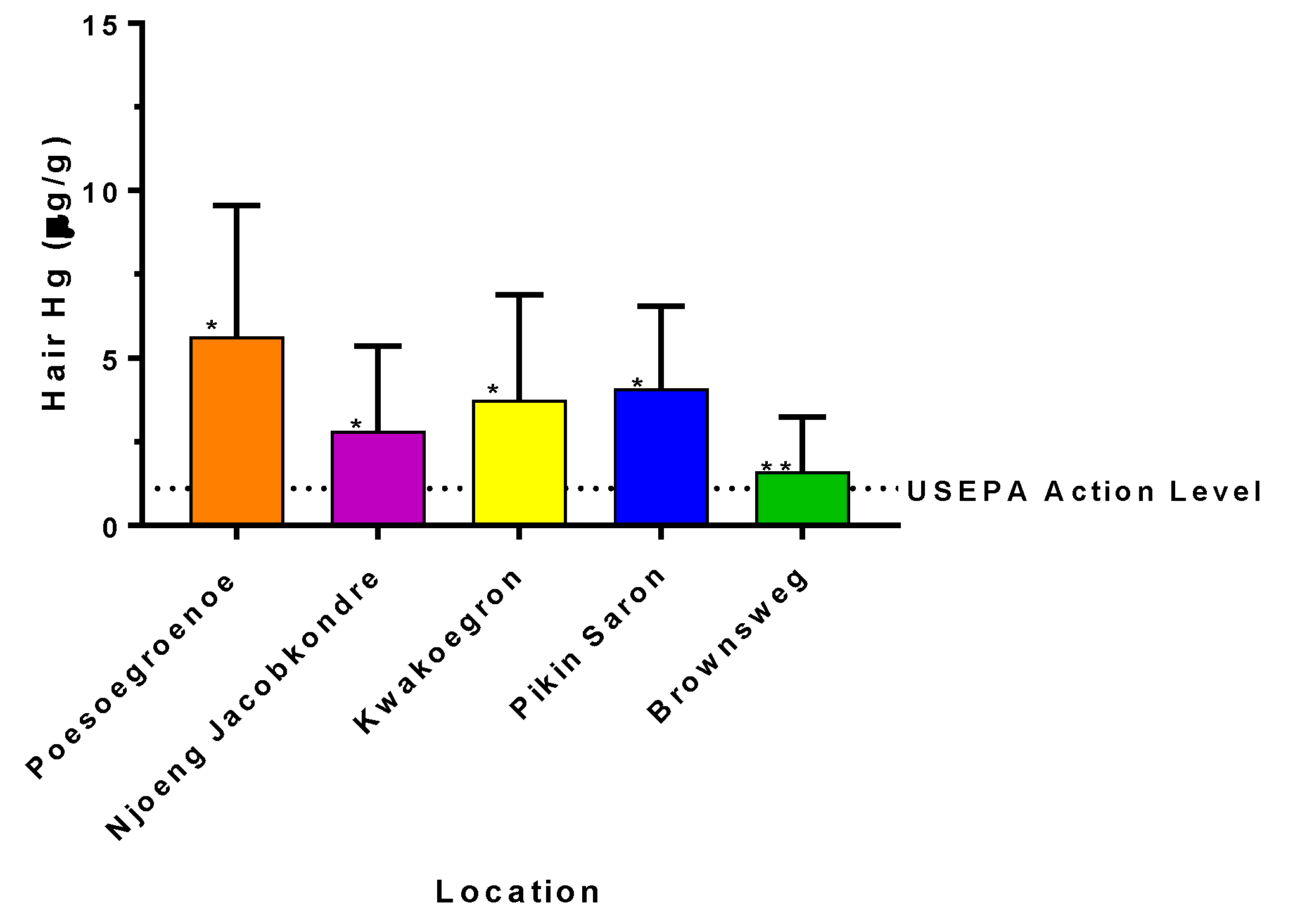
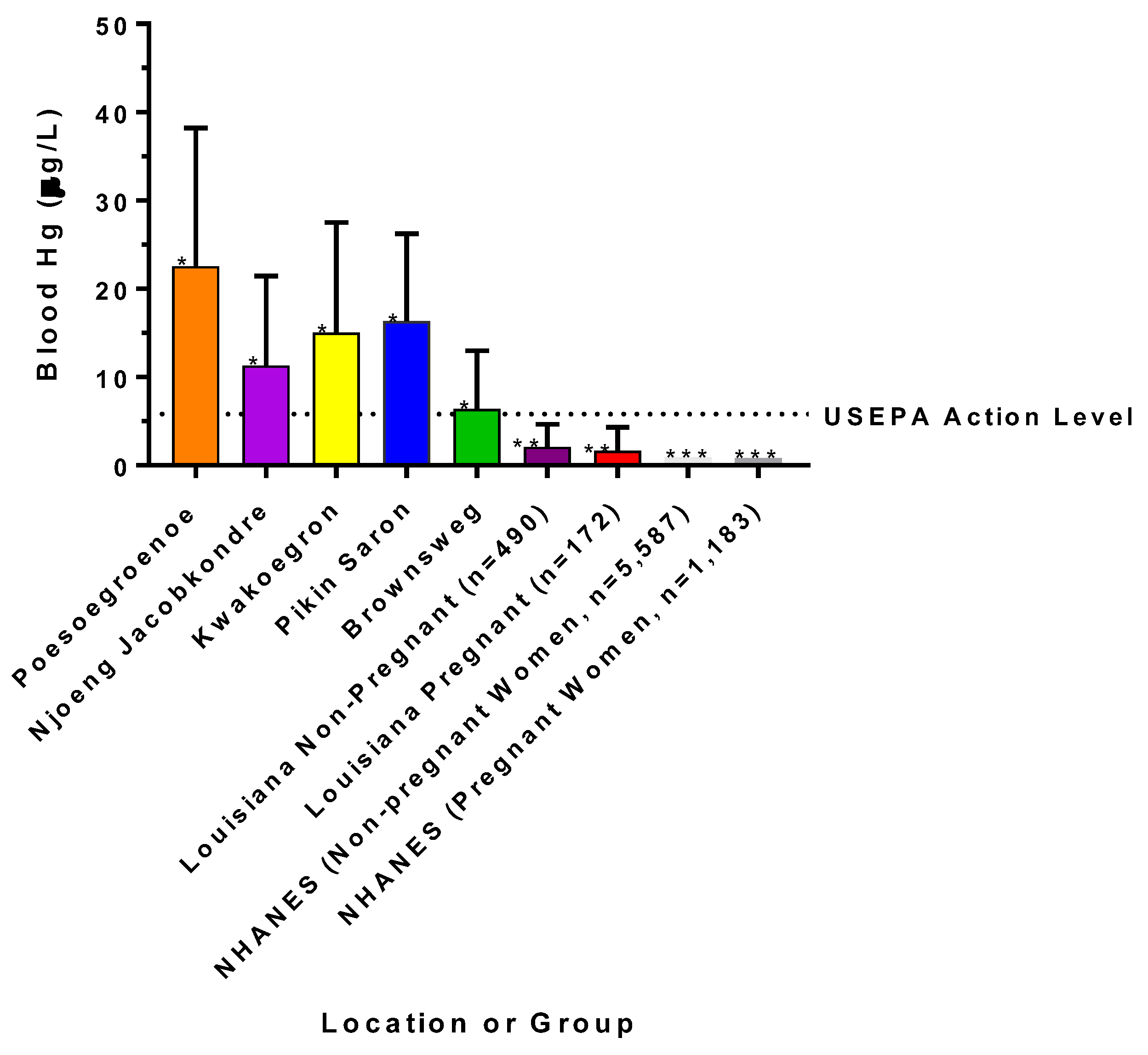
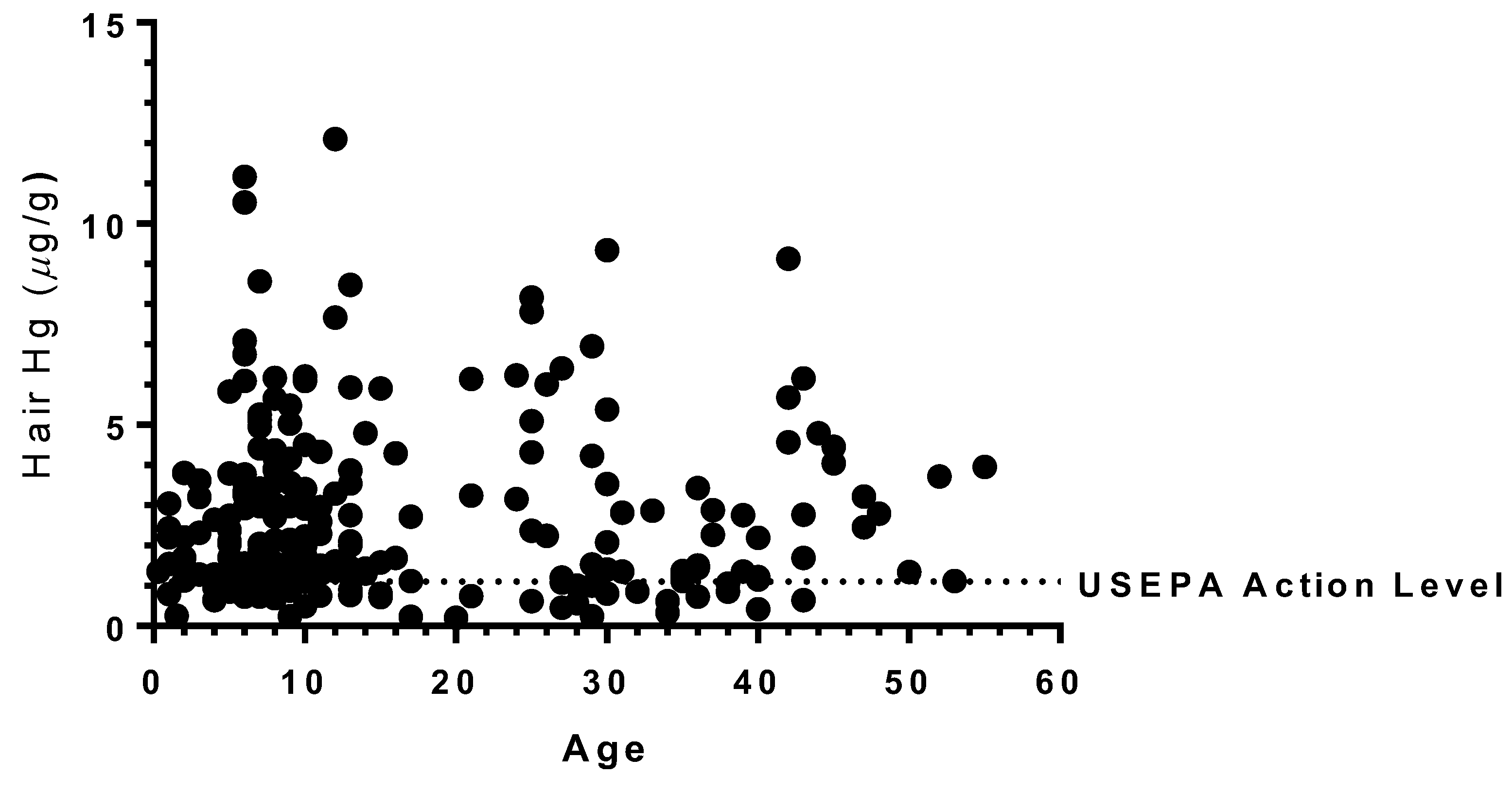
3. Results
4. Discussion
4.1. Possible Sources of Exposure to Hg in Suriname
4.2. Possible Health Implications Based on Previous Research
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Clarkson, T.W. The three modern faces of mercury. Environ. Health Perspect. 2002, 110, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Clarkson, T.W.; Magos, L. The toxicology of mercury and its chemical compounds. Crit. Rev. Toxicol. 2006, 36, 609–662. [Google Scholar] [CrossRef] [PubMed]
- Bakir, F.; Damluji, S.F.; Amin-Zaki, L.; Murtadha, M.; Khalidi, A.; Al-Rawi, N.Y.; Tikriti, S.; Dhahir, H.I.; Clarkson, T.W.; Smith, J.C.; et al. Methylmercury poisoning in Iraq. Science 1973, 181, 230–241. [Google Scholar] [CrossRef] [PubMed]
- Harada, M. Minamata disease: Methylmercury poisoning in Japan caused by environmental pollution. Crit. Rev. Toxicol. 1995, 25, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Crump, K.S.; Kjellström, T.; Shipp, A.M.; Silvers, A.; Stewart, A. Influence of prenatal mercury exposure upon scholastic and psychological test performance: Benchmark analysis of a New Zealand cohort. Risk Anal. 1998, 18, 701–713. [Google Scholar] [CrossRef] [PubMed]
- Grandjean, P.; Weihe, P.; Nielsen, F.; Heinzow, B.; Debes, F.; Budtz-Jorgensen, E. Neurobehavioral deficits at age 7 years associated with prenatal exposure to toxicants from maternal seafood diet. Neurotoxicol. Teratol. 2012, 34, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Grandjean, P.; Weihe, P.; White, R.F.; Debes, F. Cognitive performance of children prenatally exposed to “safe” levels of methylmercury. Environ. Res. 1998, 77, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Grandjean, P.; Weihe, P.; White, R.F.; Debes, F.; Araki, S.; Yokoyama, K.; Murata, K.; Sorensen, N.; Dahl, R.; Jorgensen, P.J. Cognitive deficit in 7-year-old children with prenatal exposure to methylmercury. Neurotoxicol. Teratol. 1997, 19, 417–428. [Google Scholar] [CrossRef]
- Grandjean, P.; Weihe, P.; Debes, F.; Choi, A.L.; Budtz-Jørgensen, E. Neurotoxicity from prenatal and postnatal exposure to methylmercury. Neurotoxicol. Teratol. 2014, 43, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Marsh, D.O.; Clarkson, T.W.; Cox, C.; Myers, G.J.; Amin-Zaki, L.; Al-Tikriti, S. Fetal methylmercury poisoning: Relationship between concentration in single strands of maternal hair and child effects. Arch. Neurol. 1987, 44, 1017–1022. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.T.; Bellinger, D.C.; Shaywitz, B.A. A quantitative analysis of prenatal methyl mercury exposure and cognitive development. Am. J. Prev. Med. 2005, 29, 353–365. [Google Scholar] [CrossRef] [PubMed]
- Ratcliffe, H.E.; Swanson, G.M.; Fischer, L.J. Human exposure to nercury: A critical assessment of the evidence of adverse health effects. J. Toxicol. Environ. Health 1996, 49, 221–270. [Google Scholar] [CrossRef] [PubMed]
- Airey, D. Mercury in human hair due to environment and diet: A review. Environ. Health Perspect. 1983, 52, 303–316. [Google Scholar] [CrossRef] [PubMed]
- Castaño, A.; Cutanda, F.; Esteban, M.; Pärt, P.; Navarro, C.; Gómez, S.; Rosado, M.; López, A.; López, E.; Exley, K.; et al. Fish consumption patterns and hair mercury levels in children and their mothers in 17 EU countries. Environ. Res. 2015, 141, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.T.; Bellinger, D.C.; Connor, W.E.; Kris-Etherton, P.M.; Lawrence, R.S.; Savitz, D.A.; Shaywitz, B.A.; Teutsch, S.M.; Gray, G.M. A quantitative risk-benefit analysis of changes in population fish consumption. Am. J. Prev. Med. 2005, 29, 325–334. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.T.; Bellinger, D.C.; Connor, W.E.; Shaywitz, B.A. A quantitative analysis of prenatal intake of n-3 polyunsaturated fatty acids and cognitive development. Am. J. Prev. Med. 2005, 29, 366–374. [Google Scholar] [CrossRef] [PubMed]
- Dellinger, M.J.; Ripley, M.P. Mercury risks versus nutritional benefits of tribal commercial fish harvests in the upper laurentian great lakes. Hum. Ecol. Risk Assess. Int. J. 2016, 22, 1036–1049. [Google Scholar] [CrossRef]
- Grandjean, P.; Weihe, P.; Jorgensen, P.J.; Clarkson, T.; Cernichiari, E.; Videro, T. Impact of maternal seafood diet on fetal exposure to mercury, selenium, and lead. Arch. Environ. Health 1992, 47, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Davidson, P.W.; Strain, J.J.; Myers, G.J.; Thurston, S.W.; Bonham, M.P.; Shamlaye, C.F.; Stokes-Riner, A.; Wallace, J.M.W.; Robson, P.J.; Duffy, E.M.; et al. Neurodevelopmental effects of maternal nutritional status and exposure to methylmercury from eating fish during pregnancy. Neurotoxicology 2008, 29, 767–775. [Google Scholar] [CrossRef] [PubMed]
- Katner, A.; Ogunyinka, E.; Sun, M.-H.; Soileau, S.; Lavergne, D.; Dugas, D.; Suffet, M. Fishing, fish consumption and advisory awareness among louisiana’s recreational fishers. Environ. Res. 2011, 111, 1037–1045. [Google Scholar] [CrossRef] [PubMed]
- Katner, A.; Sun, M.-H.; Suffet, M. An evaluation of mercury levels in louisiana fish: Trends and public health issues. Sci. Total Environ. 2010, 408, 5707–5714. [Google Scholar] [CrossRef] [PubMed]
- Lincoln, R.A.; Shine, J.P.; Chesney, E.J.; Vorhees, D.J.; Grandjean, P.; Senn, D.B. Fish consumption and mercury exposure among louisiana recreational anglers. Environ. Health Perspect. 2011, 119, 245–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahaffey, K.R.; Clickner, R.P.; Jeffries, R.A. Adult women’s blood mercury concentrations vary regionally in the united states: Association with patterns of fish consumption (NHANES 1999–2004). Environ. Health Perspect. 2008, 117, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Zilversmit, L.; Wickliffe, J.; Shankar, A.; Taylor, R.; Harville, E. Correlations of biomarkers and self-reported seafood consumption among pregnant and non-pregnant women in Southeastern Louisiana after the gulf oil spill: The growh study. Int. J. Environ. Res. Public Health 2017, 14, 784. [Google Scholar] [CrossRef] [PubMed]
- Dong, Z.; Jim, R.C.; Hatley, E.L.; Backus, A.S.N.; Shine, J.P.; Spengler, J.D.; Schaider, L.A. A longitudinal study of mercury exposure associated with consumption of freshwater fish from a reservoir in rural South Central USA. Environ. Res. 2015, 136, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Horrocks, L.A.; Yeo, Y.K. Health benefits of docosahexaenoic acid (DHA). Pharmacol. Res. 1999, 40, 211–225. [Google Scholar] [CrossRef] [PubMed]
- Innis, S.M. Dietary omega 3 fatty acids and the developing brain. Brain Res. 2008, 1237, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Kris-Etherton, P.M.; Hill, A.M. N-3 fatty acids: Food or supplements? J. Am. Diet. Assoc. 2008, 108, 1125–1130. [Google Scholar] [CrossRef] [PubMed]
- Strain, J.; Yeates, A.J.; van Wijngaarden, E.; Thurston, S.W.; Mulhern, M.S.; McSorley, E.M.; Watson, G.E.; Love, T.M.; Smith, T.H.; Yost, K.; et al. Prenatal exposure to methyl mercury from fish consumption and polyunsaturated fatty acids: Associations with child development at 20 MO of age in an observational study in the republic of seychelles. Am. J. Clin. Nutr. 2015, 101, 530–537. [Google Scholar] [CrossRef] [PubMed]
- Basu, N.; Clarke, E.; Green, A.; Calys-Tagoe, B.; Chan, L.; Dzodzomenyo, M.; Fobil, J.; Long, R.N.; Neitzel, R.L.; Obiri, S.; et al. Integrated assessment of artisanal and small-scale gold mining in ghana—Part 1: Human health review. Int. J. Environ. Res. Public Health 2015, 12, 5143–5176. [Google Scholar] [CrossRef] [PubMed]
- Gibb, H.; O’Leary, K.G. Mercury exposure and health impacts among individuals in the artisanal and small-scale gold mining community: A comprehensive review. Environ. Health Perspect. 2014, 122, 667–672. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, W.B. Global Environmental Public Health Issues Related to Gold Mining and Mercury Contamination in Indigenous Communities in Suriname, South America. Ph.D. Thesis, Tulane University, School of Public Health and Tropical Medicine, New Orleans, LA, USA, 2012. [Google Scholar]
- Legg, E.D.; Ouboter, P.E.; Wright, M.A.P. Small-Scale Gold Mining Related Mercury Contamination in the Guianas: A Review; World Wildlife Fund: Paramaribo, Suriname, 2015; p. 61. [Google Scholar]
- Manceau, A.; Enescu, M.; Simionovici, A.; Lanson, M.; Gonzalez-Rey, M.; Rovezzi, M.; Tucoulou, R.; Glatzel, P.; Nagy, K.L.; Bourdineaud, J.-P. Chemical forms of mercury in human hair reveal dources of exposure. Environ. Sci. Technol. 2016, 50, 10721–10729. [Google Scholar] [CrossRef] [PubMed]
- McKelvey, W.; Jeffery, N.; Clark, N.; Kass, D.; Parsons, P.J. Population-based inorganic mercury biomonitoring and the identification of skin care products as a source of exposure in new york city. Environ. Health Perspect. 2011, 119, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Ouboter, P.E.; Landburg, G.A. Mercury Poisoing: A Threat to Brownsweg Villagers; World Wildlife Fund: Paramaribo, Suriname, 2010; p. 16. [Google Scholar]
- Ouboter, P.E.; Landburg, G.A.; Quik, J.H.M.; Mol, J.H.A.; van der Lugt, F. Mercury levels in pristine and gold mining impacted aquatic ecosystems of suriname, south america. Ambio 2012, 41, 873–882. [Google Scholar] [CrossRef] [PubMed]
- Ouboter, P.E.; Landburg, G.A.; White, C.; Mol, J.; van der Lugt, F.; Quik, J.H.M. Final Technical Report Mercury Pollution in the Greenstone Belt; World Wildlife Fund: Paramaribo, Suriname, 2007; p. 51. [Google Scholar]
- Rajaee, M.; Long, R.; Renne, E.; Basu, N. Mercury exposure assessment and spatial distribution in a ghanaian small-scale gold mining community. Int. J. Environ. Res. Public Health 2015, 12, 10755–10782. [Google Scholar] [CrossRef] [PubMed]
- United States Environmental Protection Agency. Mercury Study Report to Congress Volume V: Health Effects of Mercury and Mercury Compounds; United States Environmental Protection Agency: Washington, DC, USA, 1997; Volume 5, pp. 1–348.
- World Health Organization. Evaluation of Certain Food Additives and Contaminants: Sixty-Seventh Report of the Joint Fao/Who Expert Committee on Food Additives; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Simon-Friedt, B.R.; Howard, J.L.; Wilson, M.J.; Gauthe, D.; Bogen, D.; Nguyen, D.; Frahm, E.; Wickliffe, J.K. Louisiana residents’ self-reported lack of information following the deepwater horizon oil spill: Effects on seafood consumption and risk perception. J. Environ. Manag. 2016, 180, 526–537. [Google Scholar] [CrossRef] [PubMed]
- Mohan, S.; Tiller, M.; Van der Voet, G.; Kanhai, H. Mercury exposure of mothers and newborns in Surinam: A pilot study. Clin. Toxicol. 2005, 43, 101–104. [Google Scholar] [CrossRef]
- McDowell, M.A.; Dillon, C.F.; Osterloh, J.; Bolger, P.M.; Pellizzari, E.; Fernando, R.; de Oca, R.M.; Schober, S.E.; Sinks, T.; Jones, R.L.; et al. Hair mercury levels in U.S. Children and women of childbearing age: Reference range data from nhanes 1999–2000. Environ. Health Perspect. 2004, 112, 1165–1171. [Google Scholar] [CrossRef] [PubMed]
- Razzaghi, H.; Tinker, S.C.; Crider, K. Blood mercury concentrations in pregnant and non-pregnant women in the United States; national health and nutrition examination survey 1999–2006. Am. J. Obstet. Gynecol. 2013, 210, 357.e1–357.e9. [Google Scholar] [PubMed]
- Eaton, A.D.; Clesceri, L.S.; Greenberg, A.E.; Franson, M.A.H. Standard Methods for the Examination of Water and Wastewater, 20th ed.; American Public Health Assocation, American Water Works Association, Water Environment Federation: Washington, DC, USA, 1998. [Google Scholar]
- Phelps, R.W.; Clarkson, T.W.; Kershaw, T.G.; Wheatley, B. Interrelationships of blood and hair mercury concentrations in a north american population exposed to methylmercury. Arch. Environ. Health 1980, 35, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Van Wijngaarden, E.; Thurston, S.W.; Myers, G.J.; Harrington, D.; Cory-Slechta, D.A.; Strain, J.J.; Watson, G.E.; Zareba, G.; Love, T.; Henderson, J.; et al. Methyl mercury exposure and neurodevelopmental outcomes in the seychelles child development study main cohort at age 22 and 24 years. Neurotoxicol. Teratol. 2017, 59, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Myers, G.J.; Davidson, P.W.; Cox, C.; Shamlaye, C.F.; Palumbo, D.; Cernichiari, E.; Sloane-Reeves, J.; Wilding, G.E.; Kost, J.; Huang, L.-S.; et al. Prenatal methylmercury exposure from ocean fish consumption in the seychelles child development study. Lancet 2003, 361, 1686–1692. [Google Scholar] [CrossRef]
- George, G.N.; MacDonald, T.C.; Korbas, M.; Singh, S.P.; Myers, G.J.; Watson, G.E.; O’Donoghue, J.L.; Pickering, I.J. The chemical forms of mercury and selenium in whale skeletal muscle. Metallomics 2011, 3, 1232–1237. [Google Scholar] [CrossRef] [PubMed]
- Rideout, K.; Kosatsky, T. Fish for dinner? Balancing risks, benefits, and values in formulating food consumption advice. Risk Anal. 2017, 37, 2041–2052. [Google Scholar] [CrossRef] [PubMed]
- Ralston, N.V.C.; Ralston, C.R.; Blackwell, J.L.; Raymond, L.J. Dietary and tissue selenium in relation to methylmercury toxicity. Neurotoxicology 2008, 29, 802–811. [Google Scholar] [CrossRef] [PubMed]
- Ralston, N.V.C.; Raymond, L.J. Dietary selenium’s protective effects against methylmercury toxicity. Toxicology 2010, 278, 112–123. [Google Scholar] [CrossRef] [PubMed]
- Skroder, H.; Kippler, M.; Tofail, F.; Vahter, M. Early-life selenium status and cognitive function at 5 and 10 years of age in bangladeshi children. Environ. Health Perspect. 2017, 125, 117003. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Village (or Subvillage) | Geometric Mean Hair Hg Level in µg/g (SD a) | Geometric Mean Blood Hg Level in µg/L (SD a) | Arithmetic Mean Age in Years (SD b) | Arithmetic Mean Body Mass in kg (SD b) |
|---|---|---|---|---|
| Kwakoegron (n = 26) | 3.75 (1.83) | 15.0 (1.83) | 24.5 (18.0) | 59.9 (30.4) |
| Pikin Saron (n = 16) | 4.09 (1.60) | 16.4 (1.60) | 21.6 (13.6) | 52.4 (24.0) |
| Poesoegroenoe (n = 13) | 5.64 (1.69) | 22.6 (1.69) | 9.9 (6.5) | N/A d |
| Njoeng Jacobkondre (n = 16) | 2.83 (1.89) | 11.3 (1.90) | 12.4 (9.6) | N/A d |
| Brownsweg (n = 161) | 1.60 (2.02) | 6.4 (2.03) | 15.8 (12.8) | 38.4 (22.8) |
| Kadyu c (n = 32) | 1.77 (1.94) | 7.1 (1.94) | 15.0 (12.5) | 38.4 (25.6) |
| Waki Basu I c (n = 21) | 1.53 (2.04) | 6.1 (2.04) | 17.9 (14.5) | 42.0 (21.4) |
| Waki Basu II c (n = 15) | 1.87 (2.09) | 7.5 (2.09) | 14.6 (11.9) | 34.8 (19.7) |
| Waki Basu III c (n = 7) | 1.76 (1.40) | 7.0 (1.40) | 19.9 (19.7) | 35.9 (20.9) |
| Makambi c (n = 33) | 1.09 (1.80) | 4.4 (1.82) | 17.0 (12.11) | 41.2 (22.3) |
| Nyun Gansee c (n = 34) | 1.50 (2.18) | 6.0 (2.18) | 14.0 (11.8) | 31.1 (21.9) |
| Biri Udu Mata c (n = 20) | 2.69 (1.72) | 10.7 (1.73) | 15.0 (13.2) | 42.6 (25.8) |
| Village (or Sub-Village) | Blood Hg > 5.8 µg/L | Blood Hg > 10 µg/L | HQ a > 1 (Individual Body Mass, USEPA RfD b) | HQ > 1 (60 kg Body Mass, USEPA RfD) | HQ > 1 (60 kg Body Mass, WHO PTWI c) |
|---|---|---|---|---|---|
| Kwakoegron | 88.5% | 80.8% | 95.8% | 100% | 80.8% |
| Pikin Saron | 100% | 81.3% | 100% | 100% | 81.3% |
| Poesoegroenoe | 100% | 92.3% | N/A e | 100% | 92.3% |
| Njoeng Jacobkondre | 81.3% | 62.5% | N/A e | 87.5% | 68.8% |
| Brownsweg | 56.1% | 27.4% | see sub-villages below | 76.2% | 29.9% |
| Kadyu d | 62.5% | 31.3% | 87.5% | 84.4% | 31.3% |
| Waki Basu I d | 57.1% | 23.8% | 81.0% | 81.0% | 23.8% |
| Waki Basu II d | 66.7% | 46.7% | 93.3% | 73.3% | 53.3% |
| Waki Basu III d | 57.1% | 14.3% | 100.0% | 100.0% | 28.6% |
| Makambi d | 29.0% | 3.2% | 81.8% | 64.5% | 6.5% |
| Nyun Gansee d | 57.6% | 24.2% | 84.6% | 69.7% | 27.3% |
| Biri Udu Mata d | 85.0% | 65.0% | 87.5% | 95.0% | 65.0% |
| Southeast LA (Non-pregnant Women) | 11.3% | 3.7% | N/A | 14.8% | 2.5% |
| Southeast LA (Pregnant Women) | 11.4% | 4.0% | N/A | 13.6% | 2.3% |
| Poesoegroenoe | ||||
| IRs | Ounces/Svg | Grams/Svg | HQ | Predicted Hair Hg Level (µg/g) |
| 1 svg/week | 4 | 113.4 | 0.69 | 0.8 |
| 2 svgs/week | 8 | 226.8 | 1.39 | 1.6 |
| 3 svgs/week | 12 | 340.2 | 2.08 | 2.5 |
| 4 svgs/week | 16 | 453.6 | 2.78 | 3.3 |
| 7 svgs/week | 28 | 793.8 | 4.86 | 5.8 |
| Brownsweg | ||||
| IRs | Ounces/Svg | Grams/Svg | HQ | Predicted Hair Hg Level (µg/g) |
| 1 svg/week | 4 | 113.4 | 3.01 | 3.6 |
| 2 svgs/week | 8 | 226.8 | 6.02 | 7.1 |
| 3 svgs/week | 12 | 340.2 | 9.03 | 10.7 |
| 4 svgs/week | 16 | 453.6 | 12.03 | 14.3 |
| 7 svgs/week | 28 | 793.8 | 21.06 | 25.0 |
| ~0.5 svgs/week | 1.8 | 51.0 | 1.35 | 1.6 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ouboter, P.E.; Landburg, G.; Satnarain, G.U.; Starke, S.Y.; Nanden, I.; Simon-Friedt, B.; Hawkins, W.B.; Taylor, R.; Lichtveld, M.Y.; Harville, E.; et al. Mercury Levels in Women and Children from Interior Villages in Suriname, South America. Int. J. Environ. Res. Public Health 2018, 15, 1007. https://doi.org/10.3390/ijerph15051007
Ouboter PE, Landburg G, Satnarain GU, Starke SY, Nanden I, Simon-Friedt B, Hawkins WB, Taylor R, Lichtveld MY, Harville E, et al. Mercury Levels in Women and Children from Interior Villages in Suriname, South America. International Journal of Environmental Research and Public Health. 2018; 15(5):1007. https://doi.org/10.3390/ijerph15051007
Chicago/Turabian StyleOuboter, Paul E., Gwendolyn Landburg, Gaitrie U. Satnarain, Sheryl Y. Starke, Indra Nanden, Bridget Simon-Friedt, William B. Hawkins, Robert Taylor, Maureen Y. Lichtveld, Emily Harville, and et al. 2018. "Mercury Levels in Women and Children from Interior Villages in Suriname, South America" International Journal of Environmental Research and Public Health 15, no. 5: 1007. https://doi.org/10.3390/ijerph15051007