Development, Implementation and Evaluation of an Educational Intervention to Prevent Low Speed Vehicle Run-Over Events: Lessons Learned


Abstract
1. Background
1.1. Development of Intervention
1.2. Intervention
- Host: small children (those most at-risk) are unaware of vehicle/road safety, not able to increase awareness until out of the at-risk age group, therefore focus must shift to raising awareness among caregivers.
- Vehicle: all vehicle types must be considered, and visibility out of the car should be considered (including blind zones).
- Physical Environment: Driveway design should incorporate the separation of a barrier to the driveway similar to pool separation.
2. Method
2.1. Survey Instrument
- Demographic characteristics: Participants provided information on gender, age, post-code (later converted into a dichotomous measure of accessibility to major cities/services), education level, income, relationship status, main language spoken at home, ethnicity, and employment status. Participants were also asked about their caregiving responsibilities for children. Participants were asked whether they lived with children, whether they cared for children in their own (participants’) home, whether they cared for children in the children’s home, and the ages of these children.
- LSVRO environmental risk factors: Driveway features (whether driveway is separated from children’s access; whether driveway is used as a play area; and whether driveway is used for reversing vehicles) were assessed via a five-point Likert scale (1 = never; 5 = always), which were then dichotomised (never vs. any other response) for each item.
- LSVRO Knowledge/attitudes/behavior: Knowledge of frequency of LSVRO events and the age group most at risk were assessed via multiple choice questions, which were each categorised into correct or incorrect. Driveway behaviour was measured using a five-point Likert Scale (1 = never; 5 = always)—participants rated how frequently they performed a list of four safety behaviours (walk around car, look around car, lock car, and physically hold the child when someone else is reversing) before reversing their vehicle in the presence of children. Responses of 1–3 were allocated a score of 0, and other responses a score of 1; scores were then summed (≥3: adequate behaviour, <3: inadequate behaviour). Originally use of a reversing mirror was included in the list of behaviours but this was not used in the calculation of total score for driveway behaviour, because the majority of the sample did not have a reversing camera on their vehicles.
- Perceived behaviour of others: Participants rated how frequently they perceived that others perform the same list of four behaviours before reversing their vehicle in the presence of children; the same approach was used to calculate a total score. The item regarding use of a reversing camera was analysed as a separate variable (infrequent: never, sometimes, about half the time, frequently, usually, or always).
- Perceived Effectiveness: Participants rated the same five behaviours in terms of their perceived effectiveness in preventing an LSVRO incident (1—not at all effective; 5–100% effective). The mean scale score was calculated and categorised: <3.5: “low perceived effectiveness”; ≥3.5: high perceived effectiveness. Reliability analyses confirmed internal reliability of this measure (Chronbach’s alpha = 0.8). In addition, participants were asked two open-ended questions:
- ○
- Are there any strategies you use or think might be effective to prevent driveway run-overs?
- ○
- What reasons do you think people might give for not using safe strategies in the driveway?Responses to these questions were recorded verbatim and later grouped into eight themes.
- Intervention Awareness: Participants were asked to nominate from a list of sources whether they had seen or heard about driveway run-overs in children. To allow analyses of each of these potential sources of awareness regarding LSVROs, 10 separate variables were created (yes/no for each). In addition, one overall variable was created to describe whether participants had heard of LSVRO from any source (yes/no).
2.2. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. LSVRO Knowledge, Attitudes, and Behaviour
3.3. LSVRO Environmental Risk Factors
3.4. Reasons for Unsafe Driveway Behaviour
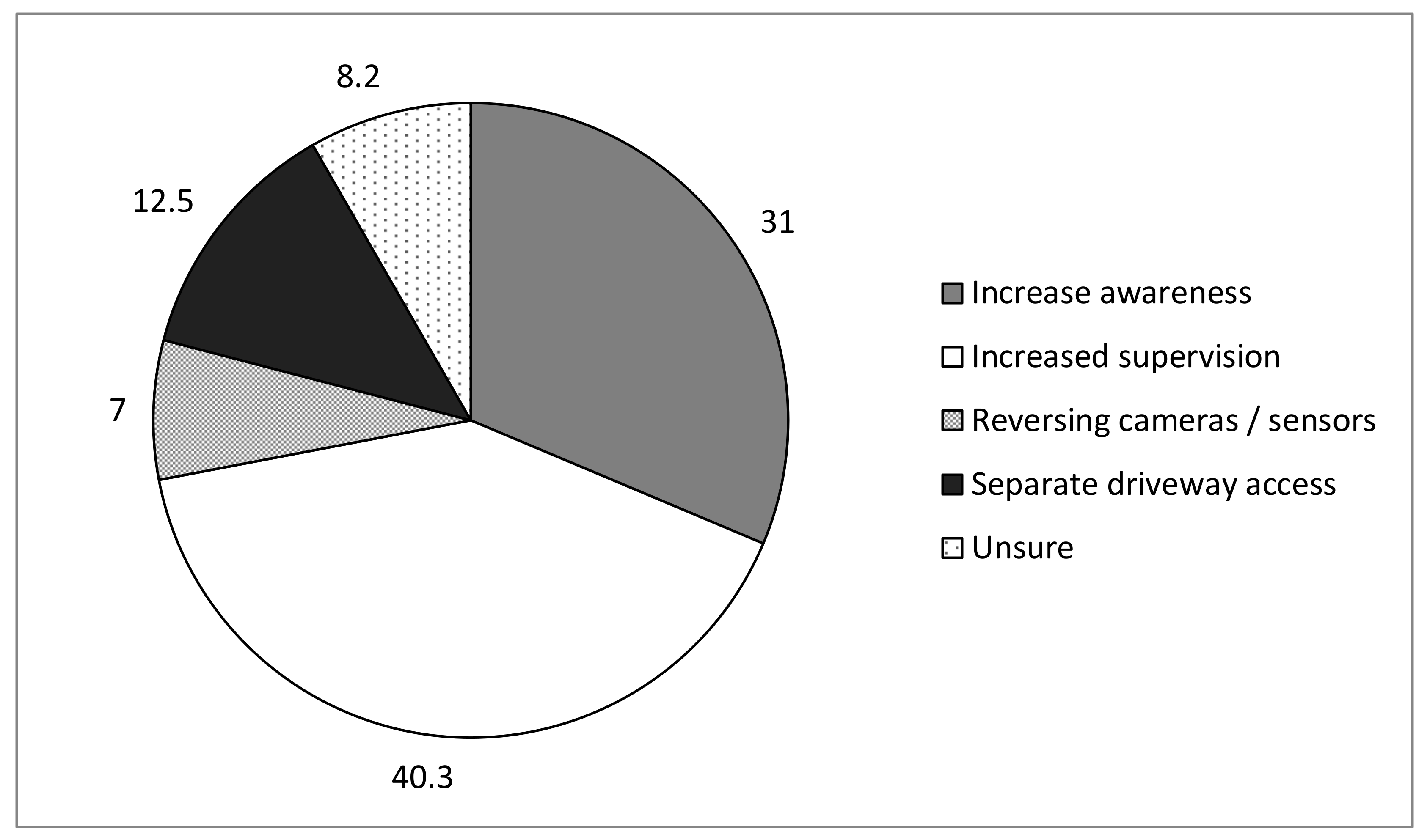
3.5. Strategies for Preventing LSVROs
3.6. Awareness of Intervention
4. Discussion
4.1. Effective Strategies to Increase Awareness
4.2. Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A


References
- Bugeja, L.; Franklin, R.C. An analysis of stratagems to reduce drowning deaths of young children in private swimming pools and spas in Victoria, Australia. Int. J. Inj. Contr. Saf. Promot. 2013, 20, 282–294. [Google Scholar] [CrossRef] [PubMed]
- Klassen, T.; Mackay, M.; Moher, D.; Walker, A.; Jones, A. Community-Based Injury Prevention Intervention. Future Child. 2000, 10, 83–110. [Google Scholar] [CrossRef] [PubMed]
- McClure, R.; Stevenson, M.; McEvoy, S. The Scientific Basis of Inury Prevention and Control; IP Communications: Melbourne, Australia, 2004. [Google Scholar]
- CCYPCG. Annual Report Deaths of Children and Young People, Queensland 2004–2005; Commission for children and Young People and Child Guardian: Brisbane, Australian, 2005.
- Agran, P.; Winn, D.; Anderson, C. Differences in child pedestrian injury events by location. Pediatrics 1994, 93, 284–288. [Google Scholar] [PubMed]
- Barker, R. Putting the Brakes on Low Speed Vehicle Run Over: An Opportunity to Act; Queensland Government, Ed.; Queensland Injury Prevention Council: Brisbane, Australia, 2012.
- Bell, M.; Ternberg, J.; Bower, R. Low velocity vehicular injuries in children—“Run-over” accidents. Pediatrics 1980, 66, 628–631. [Google Scholar] [PubMed]
- Brison, R.; Wicklund, K.; Mueller, B. Fatal pedestrian injuries to young children: A different pattern of injury. Am. J. Public Health 1988, 78, 793–795. [Google Scholar] [CrossRef] [PubMed]
- CCYPCG. Deaths of Children and Young People 2011–2012, in Annual Report; Commission for Children, Ed.; The State of Queensland: Brisbane, Australia, 2012.
- Davey, J.D.G.; Clark, M.J.; Freeman, J.; Johnston, T.C.; White, J.; Woods, S.D. The Prevalence and Characteristics of Paediatric Driveway Accidents in Queensland. J. Australas. Coll. Road Saf. 2007, 18, 34–40. [Google Scholar]
- Griffin, B.; Watt, K.; Wallis, B.; Shields, L.; Kimble, R. Paediatric low speed vehicle run-over fatalities in Queensland. Inj. Prev. 2011, 17 (Suppl. I), i10–i13. [Google Scholar] [CrossRef] [PubMed]
- Griffin, B.; Watt, K.; Wallis, B.; Shields, L.; Kimble, R. Systematic Literature Review of Incidence Rates of Low Speed Vehicle Run Over Incidents in Children. Worldviews Evid. Based Nurs. 2014, 11, 98–106. [Google Scholar] [CrossRef] [PubMed]
- Griffin, B.; Watt, K.; Shields, L.; Wallis, B.; Kimble, R. Low speed vehicle run-over incidents: Methodological issues in describing incidence and characteristics in Queensland children aged 0–15 years. Aust. Epidemiol. Assoc. J. 2013, 20, 29–33. [Google Scholar]
- Griffin, B.; Watt, K.; Wallis, B.; Shields, L.; Kimble, R. Incidence of paediatric fatal and non-fatal low speed vehicle run over events in Queensland, Australia: Eleven year analysis. BMC Public Health 2014, 14, 245. [Google Scholar] [CrossRef] [PubMed]
- Griffin, B.; Watt, K.; Shields, L.; Kimble, R. Characteristics of Low Speed Vehicle Run Over Events in Children: An Eleven Year Review. Inj. Prev. 2014, 20, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Hsun-Hsiao, K.; Newbury, C.; Bartlett, N.; Dansey, R.; Morreau, P.; Hamill, J. Paediatric driveway run-over injuries: Time to redesign? J. N. Z. Med. Assoc. 2009, 122, 1298. [Google Scholar]
- Murphy, F.; White, S.; Morreau, P. Driveway-related motor vehicle injuries in the paediatric population: A preventable tragedy. N. Z. Med. J. 2002, 115, U148. [Google Scholar] [PubMed]
- Pinkney, K.A.; Smith, A.; Mann, N.C.; Mower, G.D.; Davis, A.; Dean, J.M. Risk of pediatric back-over injuries in residential driveways by vehicle type. Pediatr. Emerg. Care 2006, 22, 402–407. [Google Scholar] [CrossRef] [PubMed]
- Roberts, I.; Kolbe, A.; White, J. Non-traffic child pedestrian injuries. J. Paediatr. Child Health 1993, 29, 233–234. [Google Scholar] [CrossRef] [PubMed]
- Anthikkat, A.P.; Page, A.; Barker, R. Low-speed vehicle run over fatalities in Australian children aged 0–5 years. J. Paediatr. Child Health 2013, 49, 388–393. [Google Scholar] [CrossRef] [PubMed]
- Nadler, E.P.; Courcoulas, A.P.; Gardner, M.J.; Ford, H.R. Driveway injuries in children: Risk factors, morbidity, and mortality. Pediatrics 2001, 108, 326–328. [Google Scholar] [CrossRef] [PubMed]
- Partrick, D.; Bensard, D.; Moore, E.; Partington, M.; Karrer, F. Driveway crush injuries in young children: A highly lethal, devastating, and potentially preventable event. J. Pediatr. Surg. 1998, 33, 1712–1715. [Google Scholar] [CrossRef]
- Robinson, P.; Nolan, T. Paediatric slow-speed non-traffic fatalities: Victoria, Australia, 1985–1995. Accid. Anal. Prev. 1997, 29, 731–737. [Google Scholar] [CrossRef]
- Saluja, G.; Brenner, R.; Morrongiello, B.; Haynie, D.; Rivera, M.; Cheng, T. The rold of supervision in child injury risk: Definition, conceptual and measurement issures. Inj. Control Saf. Promot. 2004, 11, 17–22. [Google Scholar] [CrossRef] [PubMed]
- SPSS Inc. IBM SPSS Statistics for Windows, Version 21.0; IBM Corp.: Armonk, NY, USA, 2012. [Google Scholar]
- Hanson, D.; Hanson, J.; Vardon, P.; McFarlane, K.; Lloyd, J.; Muller, R.; Durrheim, D. The injury iceberg: An ecological approach to planning sustainable community safety interventions. Health Promot. J. Austr. 2005, 16, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Morris, B.; Trimble, N. Promotion of bicycle helmet use among school children: A randomized clinical trial. Can. J. Public Health 1991, 82, 92–94. [Google Scholar] [PubMed]
- Hunter, K.; Keay, L.; Clapham, K.; Lyford, M.; Brown, J.; Bilston, L.; Simpson, J.M.; Stevenson, M.; Ivers, R.Q. Buckle up safely (shoalhaven): A process and impact evaluation of a pragmatic, multifaceted preschool-based pilot program to increase correct use of age-appropriate child restraints. Traffic Inj. Prev. 2014, 15, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Burgess, J.D.; Kimble, R.M.; Watt, K.; Cameron, C.M. The Adoption of Social Media to Recruit Participants for the Cool Runnings Randomized Controlled Trial in Australia. JMIR Res. Protoc. 2017, 6, e200. [Google Scholar] [CrossRef] [PubMed]
- Burgess, J.D.; Watt, K.A.; Kimble, R.M.; Cameron, C.M. Knowledge of childhood burn risks and burn first aid: Cool Runnings. Inj. Prev. 2018. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristics | Pre-Intervention n = 135 | Post-Intervention n = 206 | |
|---|---|---|---|
| n (%) | n (%) | ||
| Gender X2 = 1.29; df = 1; p > 0.05 | Male Female | 53 (39.3%) 81 (60.4%) | 69 (33.5%) 137 (66.5%) |
| Age * (n = 3 missing) X2 = 11.29; df = 3; p < 0.01) | 16–25 years 26–35 years 36–45 years 46+ years | 35 (23.6%) 37 (27.8%) 33 (24.8%) 28 (21.1%) | 32 (15.6%) 91 (44.4%) 42 (20.5%) 40 (19.5%) |
| Remoteness a (n = 21 missing) X2 = 4.97; df = 1; p > 0.05 | Highly accessible Not highly accessible | 114 (95%) 6 (5%) | 189 (94.5%) 11 (5.5%) |
| Relationship status * (n = 8 missing) X2 = 35.92; df = 1; p < 0.001 | Living with a partner Not living with a partner | 45 (34.4%) 86 (65.6%) | 137 (67.8%) 65 (32.2%) |
| Education (n = 13 missing) X2 = 3.47; df = 3; p > 0.05 | ≤Grade 10 Grade 12 TAFE University | 22 (16.4%) 35 (26.1%) 27 (20.1%) 50 (37.3%) | 21 (10.8%) 49 (25.3%) 35 (18.0%) 89 (45.9%) |
| Main language at home (n = 3 missing) X2 = 1.78; df = 1; p > 0.05) | English Other | 120 (90.9%) 12 (9.1%) | 195 (94.7%) 11 (5.3%) |
| Household income (Gross, per annum) (n = 38 missing) X2 = 1.76; df = 3; p > 0.05) | <$26,000 $26,000–67,499 $67,500–114,999 $115,000+ | 14 (11.2%) 44 (35.2%) 39 (31.2%) 28 (22.4%) | 18 (10.1%) 52 (29.2%) 59 (33.2%) 49 (27.5%) |
| Employment (n = 16 missing) X2 = 1.03; df = 2; p > 0.05) | Full-time Part-time/Casual Not employed | 69 (51.5%) 27 (20.1%) 38 (28.4%) | 98 (50.8%) 32 (16.6%) 61 (32.6%) |
| Number of children live with X2 = 0.76; df = 3; p > 0.05 | None 1 2 3+ | 74 (54.8%) 19 (14.1%) 30 (22.2%) 12 (8.9%) | 119 (57.8%) 27 (13.1%) 39 (18.9%) 21 (10.2%) |
| Care for children in OWN home (monthly or more) * (n = 5 missing); X2 = 4.62; df = 1; p < 0.05 | Yes No | 66 (50.8%) 64 (49.2%) | 80 (38.8%) 126 (61.2%) |
| Care for children in THEIR home monthly or more * (n = 4 missing); X2 = 17.64; df = 1; p < 0.001 | Yes No | 68 (51.9%) 63 (48.1%) | 60 (29.1%) 146 (70.9%) |
| Outcome Variable | Pre-Intervention n = 135 | Post-Intervention n = 206 | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Knowledge | |||||
| LSVRO Frequency * (n = 1 missing; X2 = 9.10; df = 1; p < 0.01) | Low | 103 | (76.9%) | 126 | (61.2%) |
| High | 31 | (23.1%) | 80 | (38.8%) | |
| Age group most at risk (n = 4 missing; X2 = 0.02; df = 1; p > 0.05) | Low | 33 | (25%) | 53 | (25.7%) |
| High | 99 | (75%) | 153 | (74.3%) | |
| Behaviour | |||||
| Driveway Behaviour * (n = 11 missing) | Inadequate | 129 | (100%) | 99 | (49.3%) |
| Adequate | 0 | (0%) | 102 | (50.7%) | |
| Perceived behaviour of others * (n = 11 missing; X2 = 3.96; df = 1; p < 0.05) | Inadequate | 102 | (81.6%) | 177 | (89.4%) |
| Adequate | 23 | (18.4%) | 21 | (10.6%) | |
| Attitudes | |||||
| Perceived others’ use of reversing camera * (n = 17; X2 = 3.84; df = 1; p = 0.05) | Infrequent Frequent | 119 7 | 174 24 | (94.4%) (5.6%) | (87.9%) (12.1%) |
| Perceived effectiveness of LSVRO strategies (n = 7 missing; X2 = 3.31; df = 1; p > 0.05) | Low | 54 | (40.9%) | 63 | (31.2%) |
| High | 78 | (59.1%) | 139 | (68.8%) | |
| LSVRO Environmental Risk Factor | Pre-Interventionn = 135 | Post-Interventionn = 206 | |
|---|---|---|---|
| n (%) | n (%) | ||
| Driveway—separate access a (n = 23 missing; X2 = 1.88; df = 1; p > 0.05) | Never Other | 71 (59.7%) 48 (40.3%) | 103 (51.8%) 96 (48.2%) |
| Driveway—play area b (n = 3 missing; X2 = 1.73; df = 1; p > 0.05) | Never Other | 90 (68.2%) 42 (31.8%) | 154 (74.8%) 52 (25.2%) |
| Driveway—reversing c (n = 9 missing; X2 = 0.03; df = 1; p > 0.05) | Never Other | 4 (3.1%) 125 (96.9%) | 7(3.4%) 196 (96.6%) |
| Reversing camera in car | Yes No | 17 (12.6%) 118 (87.4%) | 19 (9.2%) 187 (90.8%) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Griffin, B.; Watt, K.; Kimble, R.; Shields, L. Development, Implementation and Evaluation of an Educational Intervention to Prevent Low Speed Vehicle Run-Over Events: Lessons Learned. Int. J. Environ. Res. Public Health 2018, 15, 685. https://doi.org/10.3390/ijerph15040685
Griffin B, Watt K, Kimble R, Shields L. Development, Implementation and Evaluation of an Educational Intervention to Prevent Low Speed Vehicle Run-Over Events: Lessons Learned. International Journal of Environmental Research and Public Health. 2018; 15(4):685. https://doi.org/10.3390/ijerph15040685
Chicago/Turabian StyleGriffin, Bronwyn, Kerrianne Watt, Roy Kimble, and Linda Shields. 2018. "Development, Implementation and Evaluation of an Educational Intervention to Prevent Low Speed Vehicle Run-Over Events: Lessons Learned" International Journal of Environmental Research and Public Health 15, no. 4: 685. https://doi.org/10.3390/ijerph15040685
APA StyleGriffin, B., Watt, K., Kimble, R., & Shields, L. (2018). Development, Implementation and Evaluation of an Educational Intervention to Prevent Low Speed Vehicle Run-Over Events: Lessons Learned. International Journal of Environmental Research and Public Health, 15(4), 685. https://doi.org/10.3390/ijerph15040685