The Effect of Acute Consumption of Energy Drinks on Blood Pressure, Heart Rate and Blood Glucose in the Group of Young Adults

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Study Protocol
2.3. Statistical Analysis
3. Results
4. Discussion
4.1. Cardiovascular Changes
4.2. Metabolic Changes
4.3. Discomfort after EDs Consumption
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Breda, J.J.; Whiting, H.S.; Encarnacao, R.; Norberg, S.; Jones, R.; Reinap, M.; Jewell, J. Energy drink consumption in Europe: A review of the risks, adverse health effects, and policy options to respond. Front. Public Health 2014, 134, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Nowak, D.; Jasionowski, A. Analysis of the consumptions of caffeinated energy drinks among Polish adolescents. Int. J. Environ. Res. Public Health 2015, 12, 7910–7921. [Google Scholar] [CrossRef] [PubMed]
- Malinauskas, B.M.; Aeby, V.G.; Overton, R.F.; Carpenter-Aeby, T.; Barber-Heidal, K. A survey of energy drink consumption patterns among college students. Nutr. J. 2007, 6, 35–41. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, M.C.; McCoy, T.P.; Rhodes, S.D.; Wagoner, A.; Wolfson, M. Caffeinated coctails: Energy drink consumption, high-risk drinking, and alcohol-related consequences among college students. Acad. Emerg. Med. 2008, 15, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Gallucci, A.R.; Martin, R.J.; Morgan, G.B. The consumption of energy drinks among a sample of college students and college student athletes. J. Community Health 2016, 41, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Reissig, C.J.; Strain, E.C.; Griffiths, R.R. Caffeinated energy drinks—A growing problem. Drug Alcohol Depend. 2009, 99, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Bigard, A.X. Risks of energy drinks in youths. Arch. Pediatr. 2010, 17, 1625–1631. [Google Scholar] [CrossRef] [PubMed]
- Seifert, S.M.; Schaechter, J.L.; Hershorin, E.R.; Lipshultz, S.E. Health effects of energy drinks on children, adolescents, and young adults. Pediatrics 2011, 127, 511–528. [Google Scholar] [CrossRef] [PubMed]
- Gunja, N.; Brown, J. Energy drinks: Health risk and toxicity. Med. J. Aust. 2012, 196, 46–49. [Google Scholar] [CrossRef] [PubMed]
- Temple, J.L. Caffeine use in children: What we know, what we have left to learn, and why we should worry. Neurosci. Biobehav. Rev. 2009, 33, 793–806. [Google Scholar] [CrossRef] [PubMed]
- Cooper, C.; Atkinson, E.J.; Wahner, H.W.; O’Fallon, W.M.; Riggs, B.L.; Judd, H.L.; Melt, L.J. Is caffeine consumption a risk factor for osteoporosis? J. Bone Miner. Res. 1992, 7, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Salinero, J.J.; Lara, B.; Abian-Vicen, J.; Gonzalez-Millan, C.; Areces, F.; Gallo-Salazar, C.; Ruiz-Vicente, D.; Del Coso, J. The use of energy drinks in sport: Perceived ergogenicity and side effects in male and female athletes. Br. J. Nutr. 2014, 112, 1494–1502. [Google Scholar] [CrossRef] [PubMed]
- Grasser, E.K.; Yepuri, G.; Dulloo, A.G.; Montani, J.P. Cardio- and cerebrovascular responses to the energy drink Red Bull in young adults: A randomized cross-over study. Eur. J. Nutr. 2014, 53, 1561–1571. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Yarlagadda, S.; Yang, B. Cardiovascular complications of energy drinks. Beverages 2015, 1, 104–126. [Google Scholar] [CrossRef]
- Rotstein, J.; Barber, J.; Strtowbridge, C.; Hayward, S.; Huang, R.; Godefroy, S.B. Energy drinks: An assessment of the potential health risks in the Canadian context. Int. Food Risk Anal. J. 2013, 4, 1–29. [Google Scholar] [CrossRef]
- Marks, R. Energy drinks: A potentially overlooked obesity correlate. Adv. Obes. Weight Manag. Control 2015, 2, 00019. [Google Scholar] [CrossRef]
- Gray, B.; Das, J.K.; Semsarian, C. Consumption of energy drinks: A new provocation test for primary arrhythmogenic diseases? Int. J. Cardiol. 2012, 159, 77–78. [Google Scholar] [CrossRef] [PubMed]
- Rush, E.; Schulz, S.; Obolonkin, V.; Simmons, D.; Plank, L. Are energy drinks contributing to the obesity epidemic? Asia Pac. J. Clin. Nutr. 2006, 15, 242–244. [Google Scholar] [PubMed]
- Reid, S.D.; Ramsarran, J.; Brathwaite, R.; Lyman, S.; Baker, A.; Cornish, D.C.; Ganga, S.; Mohammed, Z.; Sookdeo, A.T.; Thapelo, S.C. Energy drink usage among university students in a Caribbean country: Patterns of use and adverse effects. J. Epidemiol. Glob. Health 2015, 5, 103–116. [Google Scholar] [CrossRef] [PubMed]
- Monnard, C.; Jean-Pierre, M.; Grasser, K.E. Cerebro- and cardio-vascular responses to energy drink in young adults: Is there a gender effect? Front. Physiol. 2016, 346, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Miles-Chan, J.L.; Charriere, N.; Grasser, E.K.; Montani, J.-P.; Dulloo, A.G. The blood pressure-elevating effect of Red Bull energy drink is mimicked by caffeine but through different hemodynamic pathways. Physiol. Rep. 2015, 3, e12290. [Google Scholar] [CrossRef] [PubMed]
- Worthley, M.I.; Prabhu, A.; De Sciscio, P.; Schultz, C.; Sanders, P.; Willoughby, S.R. Detrimental effects of energy drink consumption on platelet and endothelial function. Am. J. Med. 2010, 123, 184–187. [Google Scholar] [CrossRef] [PubMed]
- Manchia, G.; Fagard, R.; Narkiewicz, K.; Redon, J.; Zanchetti, A.; Bohm, M.; Christiaens, T.; Cifkova, R.; De Bucker, G.; Dominiczak, A.; et al. ESH/ESC guidelines on conduct in hypertension in 2013. Pol. Heart J. 2013, 71, 27–118. (In Polish) [Google Scholar] [CrossRef]
- Kallioinen, N.; Hill, A.; Horswill, M.S.; Ward, H.E.; Watson, M.O. Sources of inaccuracy in the measurement of adult patients’ resting blood pressure in clinical settings: A systematic review. J. Hypertens. 2017, 35, 421–441. [Google Scholar] [CrossRef] [PubMed]
- Franks, A.M.; Schmidt, J.M.; McCain, K.R.; Fraer, M. Comparison of the effects of energy drink versus caffeine suplementation on indices of 24-hour ambulatory blood pressure. Ann. Pharmacother. 2012, 46, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Elitok, A.; Oz, F.; Panc, C.; Sarikaya, R.; Sezikli, S.; Pala, Y.; Bugan, Ö.S.; Ateş, M.; Parıldar, H.; Ayaz, M.B.; et al. Acute effects of Red Bull energy drink on ventricular repolarization in healthy young volunteers: A prospective study. Anatol. J. Cardiol. 2015, 15, 919–922. [Google Scholar] [CrossRef] [PubMed]
- Ragsdale, F.R.; Gronli, T.D.; Batool, N.; Haight, N.; Mehaffey, A.; McMahon, E.C.; Nalli, T.W.; Mannello, C.M.; Sell, C.J.; McCann, P.J.; et al. Effect of Red Bull energy drink on cardiovascular and renal function. Amino Acids 2010, 38, 1193–1200. [Google Scholar] [CrossRef] [PubMed]
- Hajsadeghi, S.; Mohammadpour, F.; Manteghi, M.J.; Kordshakeri, K.; Tokazebani, M.; Rahmani, E.; Hassanzadeh, M. Effects of energy drinks on blood pressure, heart rate, and electrocardiographic parameters: An experimental study on healthy young adults. Anatol. J. Cardiol. 2016, 16, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Steinke, L.; Lanfear, D.E.; Dhanapal, V.; Kalus, J.S. Effect of “energy drink” consumption on hemodynamic and electrocardiographic parameters in healthy young adults. Ann. Pharmacother. 2009, 43, 596–602. [Google Scholar] [CrossRef] [PubMed]
- Del Coso, J.; Salinero, J.J.; Gonzales-Millan, C.; Abian-Vicen, J.; Perez-Gonzalez, B. Dose response effects of a caffeine-containing energy drink on muscle performance: A repeated measures design. J. Int. Soc. Sports Nutr. 2012, 9, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Grasser, E.K.; Miles-Chan, L.J.; Charrière, N.; Loonam, C.R.; Dulloo, A.G.; Montani, J.-P. Energy drinks and their impact on the cardiovascular system: Potential mechanisms. Adv. Nutr. 2016, 7, 950–960. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, I.A. A review of recent evidence relating to sugars, insulin resistance and diabetes. Eur. J. Nutr. 2016, 55, 17–23. [Google Scholar] [CrossRef] [PubMed]
- González-Domínguez, R.; Mateos, R.M.; Lechuga-Sancho, A.M.; González-Cortés, J.J.; Corrales-Cuevas, M.; Rojas-Cots, J.A.; Segundo, C.; Schwarz, M. Synergic effects of sugar and caffeine on insulin-mediated metabolomic alterations after an acute consumption of soft drinks. Electrophoresis 2017, 38, 2313–2322. [Google Scholar] [CrossRef] [PubMed]
- Nagai, R.; Shirakawa, J.; Fujiwara, Y.; Ohno, R.; Moroishi, N.; Sakata, N.; Nagai, M. Detection of AGEs as markers for carbohydrate metabolism and protein denaturation. J. Clin. Biochem. Nutr. 2014, 55, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Szotowska, M.; Bartmańska, M.; Wyskida, K.; Bąba, M.; Tarski, M.; Adamczak, M.; Więcek, A. The influence of so-called “energy drinks” on the blood pressure and the pulse rate in young, healthy adults. Arterial Hypertension 2013, 17, 169–174. (In Polish) [Google Scholar]
- Costa, B.M.; Hayley, A.; Miller, P. Young adolescents’ perceptions, patterns, and contexts of energy drink use: A focus group study. Appetite 2014, 80, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Nowak, D.; Jasionowski, A. Analysis of consumption of energy drinks by a group of adolescent athletes. Int. J. Environ. Res. Public Health 2016, 13, 768. [Google Scholar] [CrossRef] [PubMed]
- Rahamathulla, M.P. Prevalence, side effects and awareness about energy drinks among the female university students in Saudi Arabia. Pak. J. Med. Sci. 2017, 33, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Monnard, C.R.; Grasser, E.K. Water ingestion decreases cardiac workload time-dependent in healthy adults with no effect of gender. Sci. Rep. 2017, 7, 7939. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Ingredients | Unit | Per 100 mL |
|---|---|---|
| Water | ||
| Energy | kcal | 46 |
| Protein | g | 0 |
| Total lipid | g | 0 |
| Carbohydrates | g | 11 |
| In it sugar | g | 11 |
| Minerals: | ||
| sodium, Na | mg | 70 |
| Vitamins: | ||
| niacin | mg | 7.0 |
| pantothenic acid | mg | 2.0 |
| vitamin B-6 | mg | 0.7 |
| vitamin B-12 | µg | 0.5 |
| Others: | ||
| Caffeine | mg | 32 |
| Taurine | mg | 400 |
| Inositol | mg | 20 |
| Acidity regulator | ||
| sodium citrate | ||
| citric acid | ||
| Carbon dioxide | ||
| Flavor | ||
| Color | ||
| riboflavin (E101) | ||
| caramel (E150d) |
| Parameter | ED Group (n = 36) | Control Group (n = 32) |
|---|---|---|
| Sex | ||
| Female | 28 | 25 |
| Male | 8 | 7 |
| Age, years | 24.8 ± 6.9 a | 25.0 ± 7.3 a |
| Height (m) | 1.70 ± 0.08 a | 1.71 ± 0.08 a |
| Weight (kg) | 65.4 ± 11.9 a | 65.1 ± 11.9 a |
| BMI | ||
| >24.9 | 5 | 4 |
| 18.5–24.9 | 30 | 27 |
| <18.5 | 1 | 1 |
| Parameter | ED Group (n = 36) | Control Group (n = 32) | ||||
|---|---|---|---|---|---|---|
| Before EDs | After 3 EDs | p | Before Water | After 3 Waters | p | |
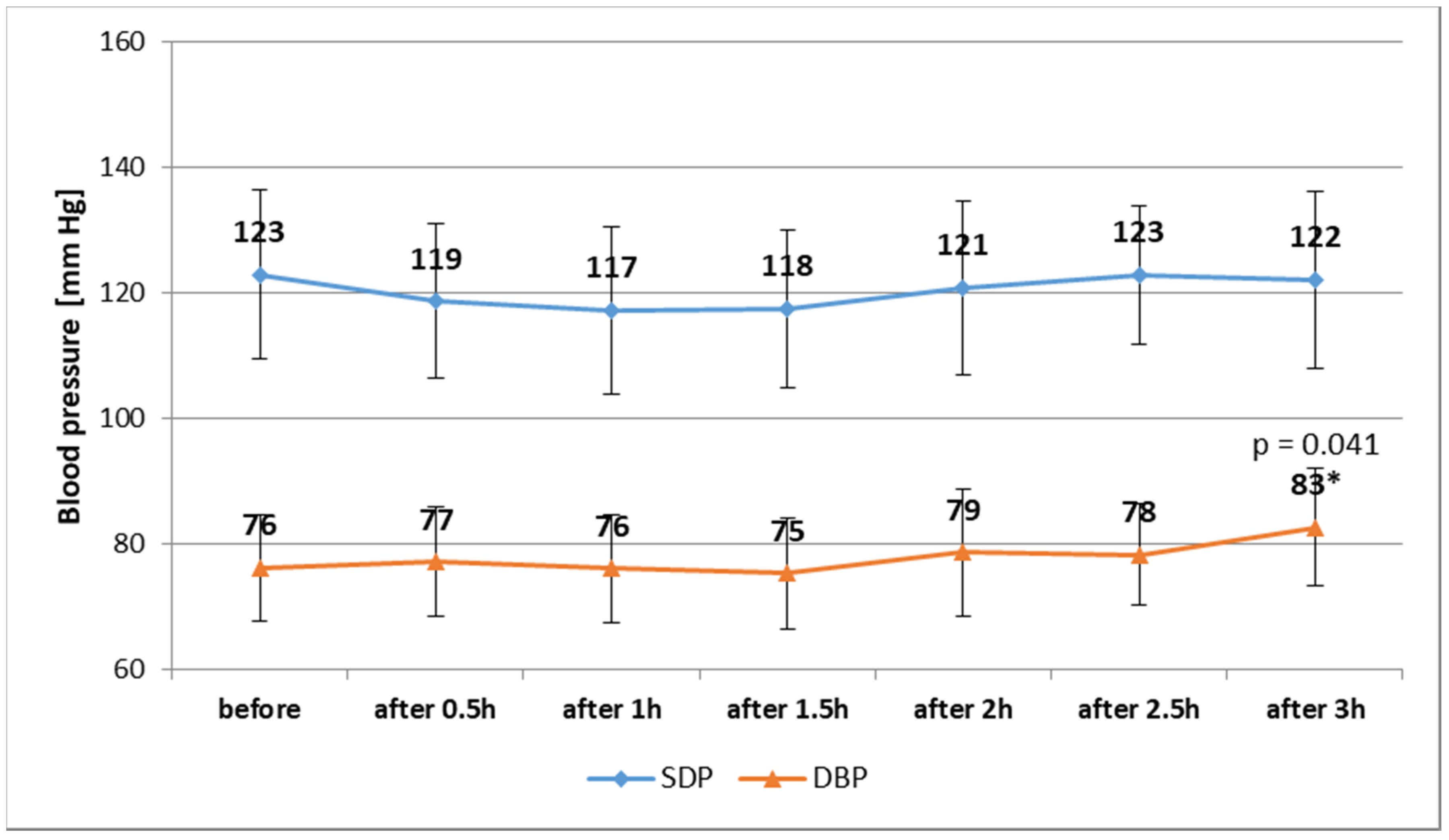
| SBP (mm Hg) | 123.0 ± 13.4 | 122.2 ± 14.0 | 0.809 | 121.2 ± 12.3 | 121.7 ± 10.7 | 0.863 |
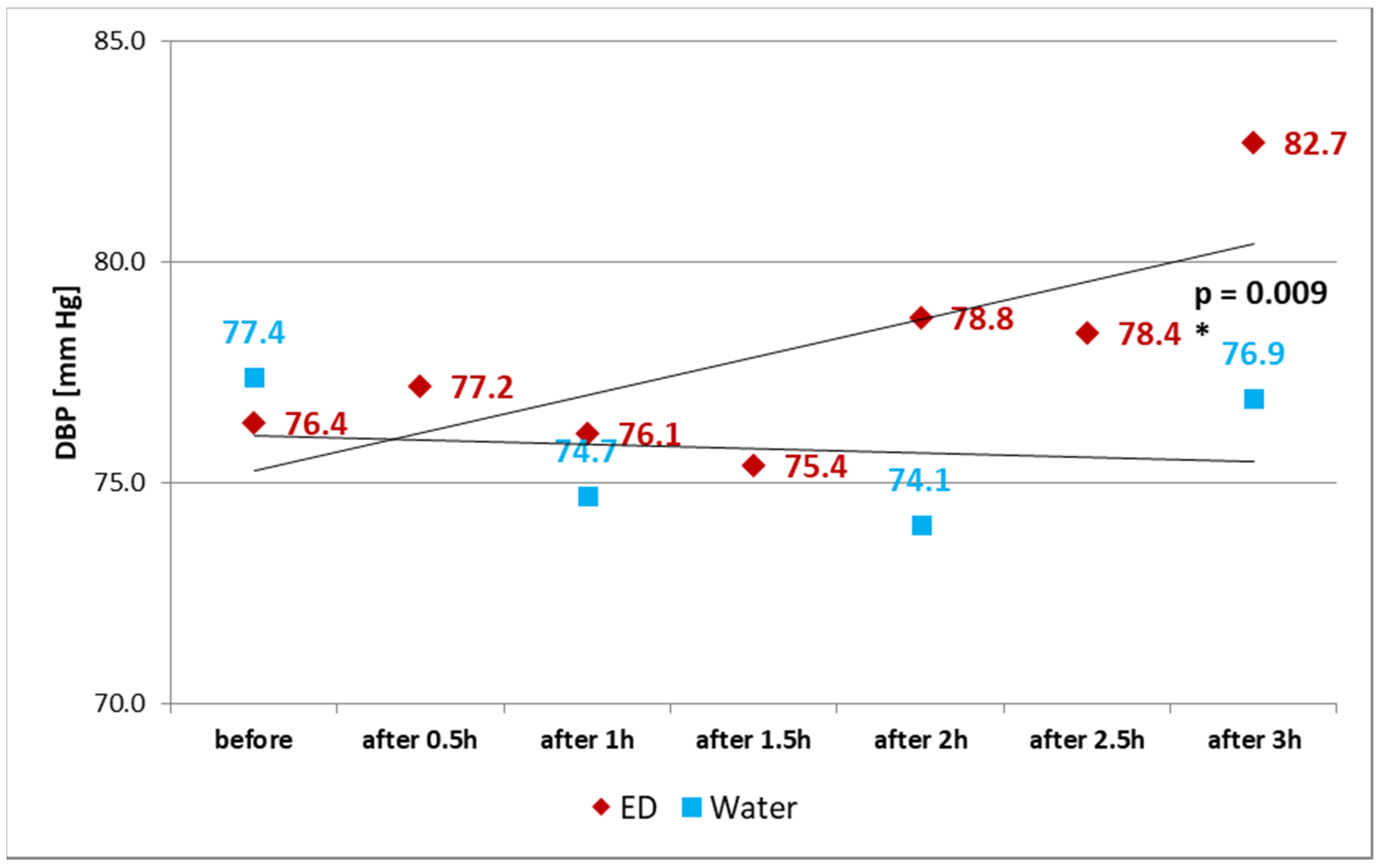
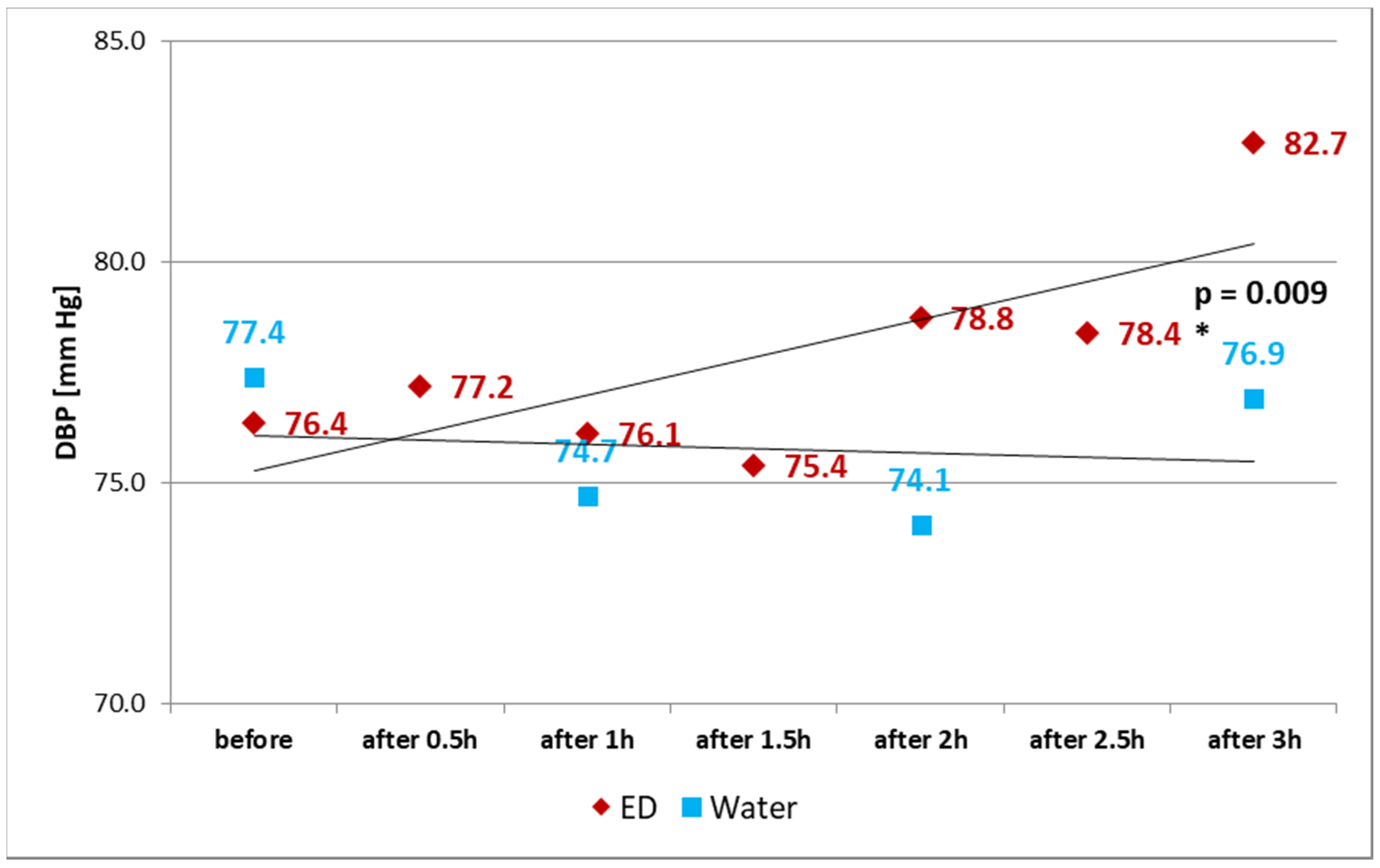
| DBP (mm Hg) | 76.4 ± 8.5 | 82.7 ± 9.3 | 0.003 | 77.4 ± 7.8 | 76.9 ± 8.6 | 0.820 |
| HR (beats per minute) | 79.7 ± 13.6 | 78.7 ± 12.1 | 0.750 | 74.0 ± 9.6 | 75.8 ± 10.9 | 0.491 |
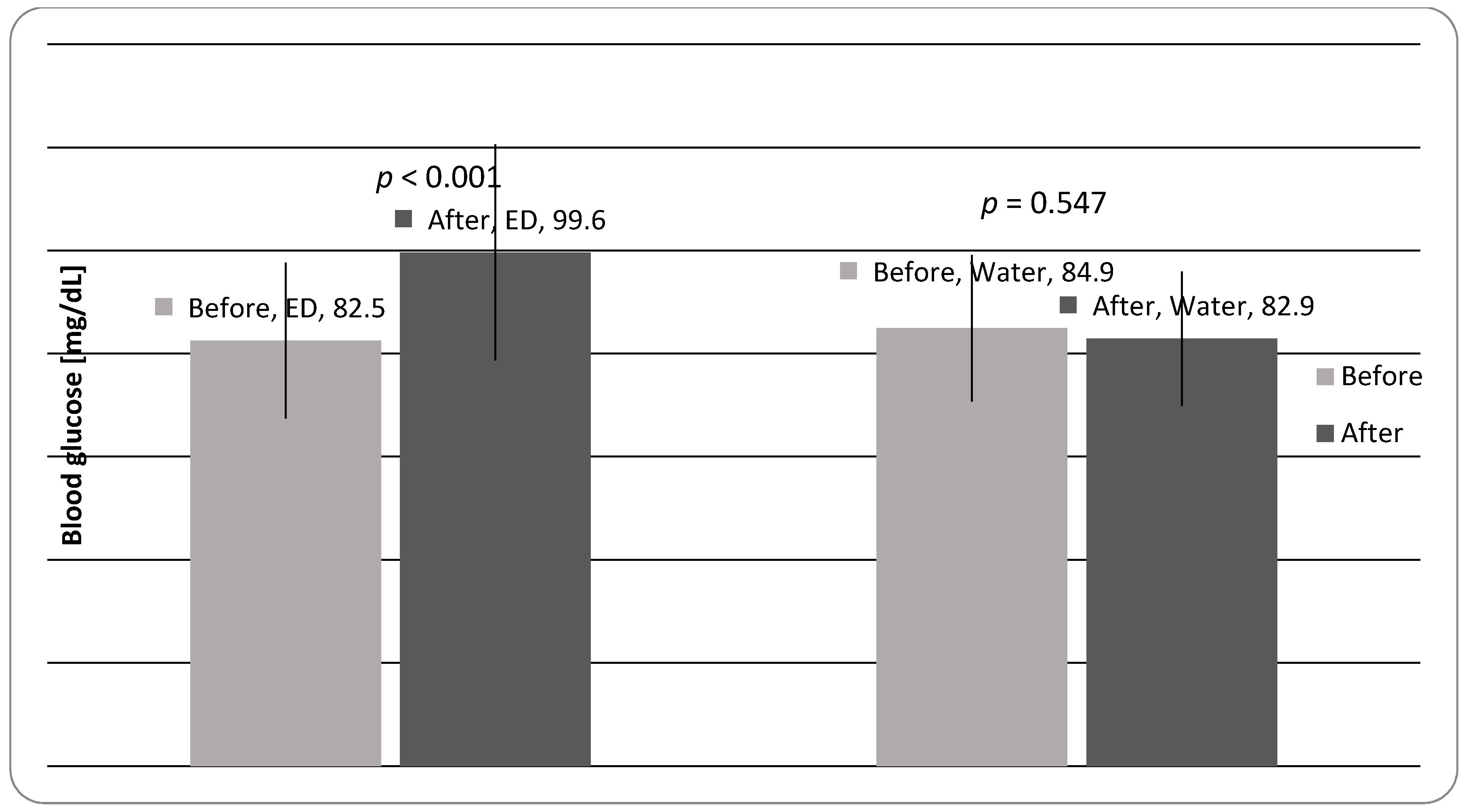
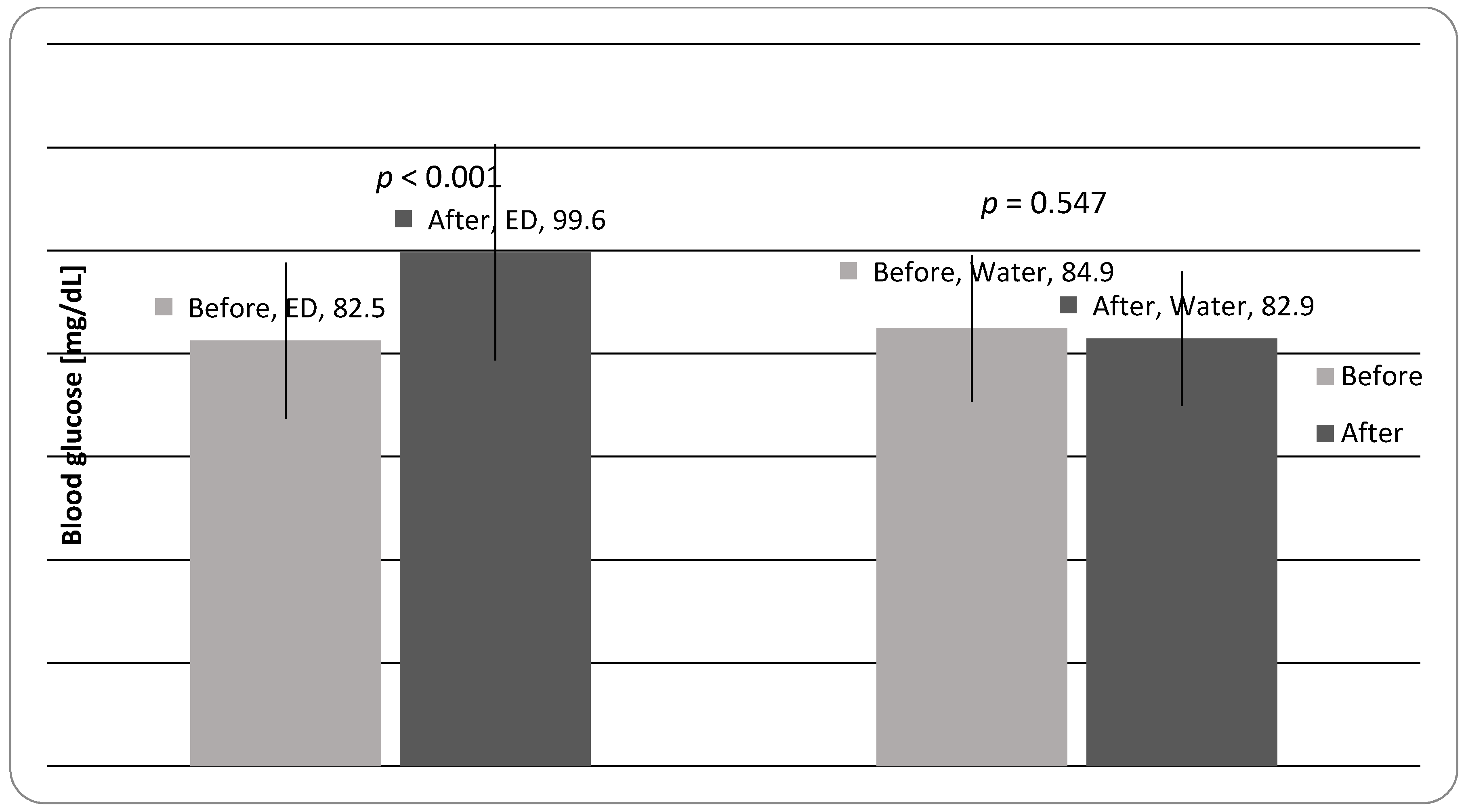
| BG (mg/dL) | 82.5 ± 15.1 | 99.6 ± 21.0 | <0.001 | 84.9 ± 14.2 | 82.9 ± 13.0 | 0.547 |
| Symptoms (Discomforts) | after 1 ED | after 2 ED | after 3 ED | n |
|---|---|---|---|---|
| headache | 3 (8%) | 7 (19%) | 3 (8%) | 13 |
| light chest pain | - | - | 2 (5%) | 2 |
| stomachache | - | 2 (5%) | 5 (14%) | 7 |
| excitation | 9 (25%) | 6 (17%) | 8 (22%) | 23 |
| anxiety | 2 (5%) | - | - | 2 |
| shaking hands | - | 1 (3%) | 4 (11%) | 5 |
| somnolence | - | 8 (22%) | 5 (14%) | 13 |
| malaise and others | 3 (8%) | 9 (25%) | 10 (28%) | 22 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nowak, D.; Gośliński, M.; Nowatkowska, K. The Effect of Acute Consumption of Energy Drinks on Blood Pressure, Heart Rate and Blood Glucose in the Group of Young Adults. Int. J. Environ. Res. Public Health 2018, 15, 544. https://doi.org/10.3390/ijerph15030544
Nowak D, Gośliński M, Nowatkowska K. The Effect of Acute Consumption of Energy Drinks on Blood Pressure, Heart Rate and Blood Glucose in the Group of Young Adults. International Journal of Environmental Research and Public Health. 2018; 15(3):544. https://doi.org/10.3390/ijerph15030544
Chicago/Turabian StyleNowak, Dariusz, Michał Gośliński, and Kamila Nowatkowska. 2018. "The Effect of Acute Consumption of Energy Drinks on Blood Pressure, Heart Rate and Blood Glucose in the Group of Young Adults" International Journal of Environmental Research and Public Health 15, no. 3: 544. https://doi.org/10.3390/ijerph15030544