Access to Street Markets and Consumption of Fruits and Vegetables by Adolescents Living in São Paulo, Brazil

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample
2.2. Data Collection and Processing
2.3. Food Consumption Data
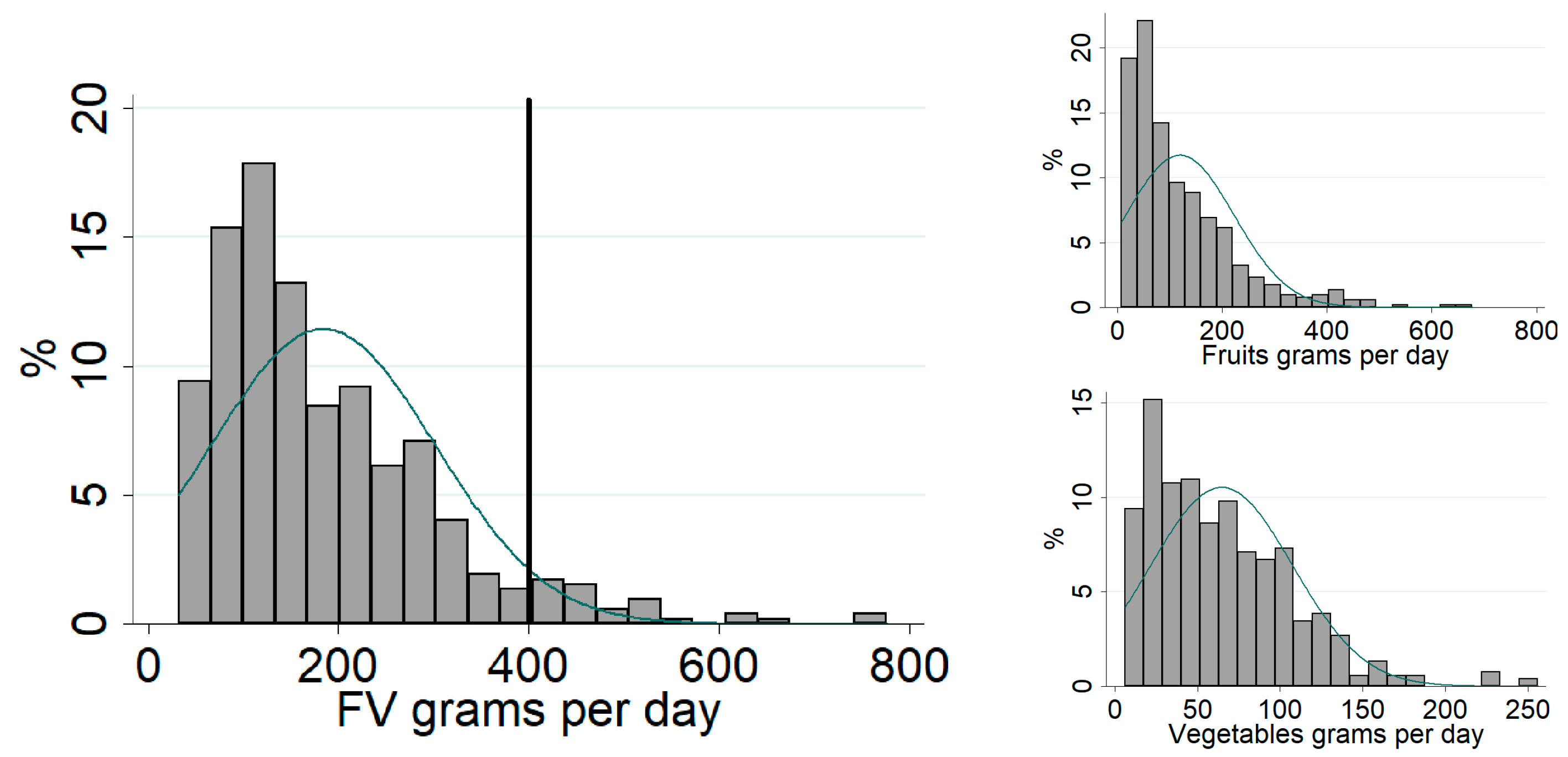
2.4. Fruits and Vegetables
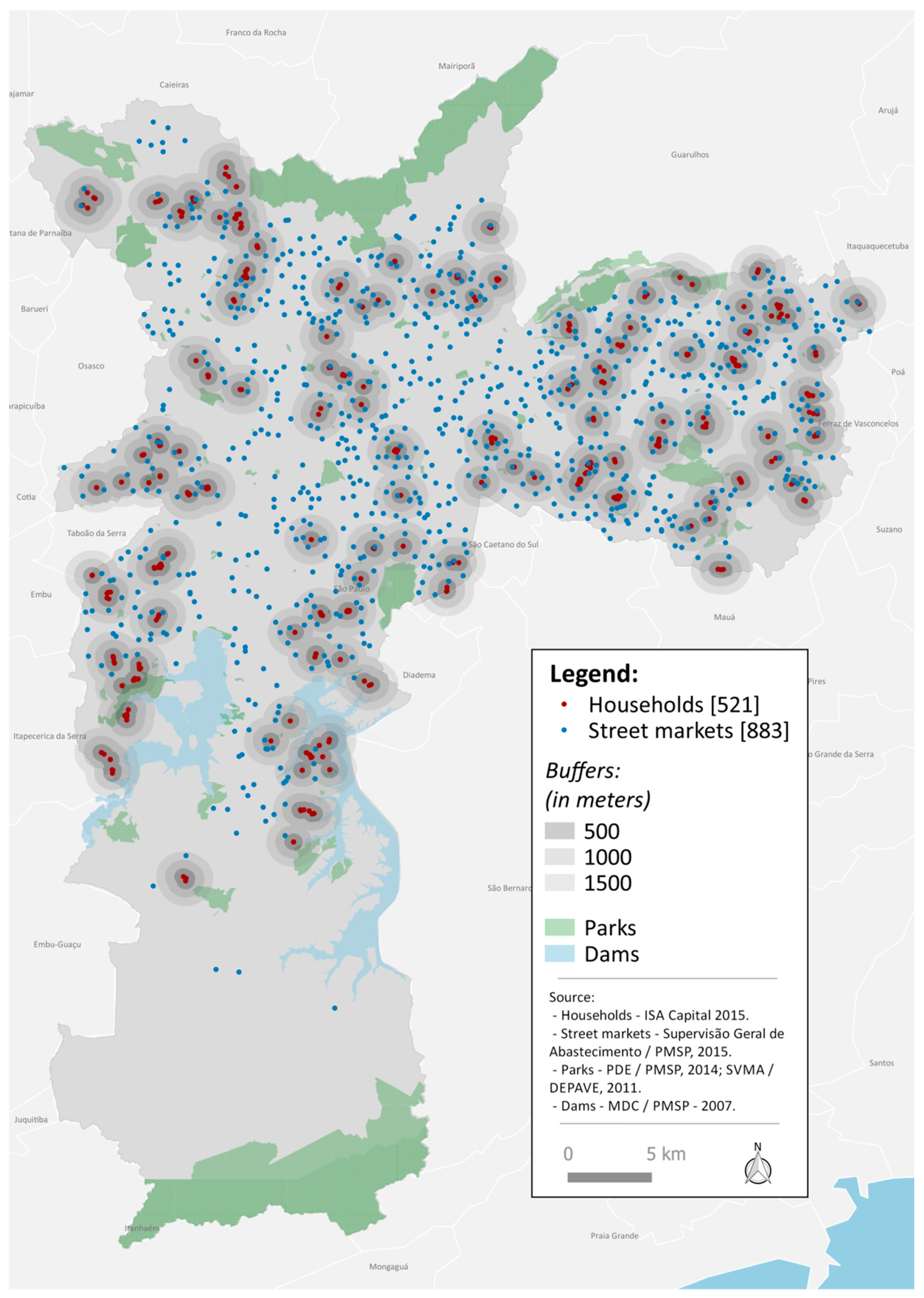
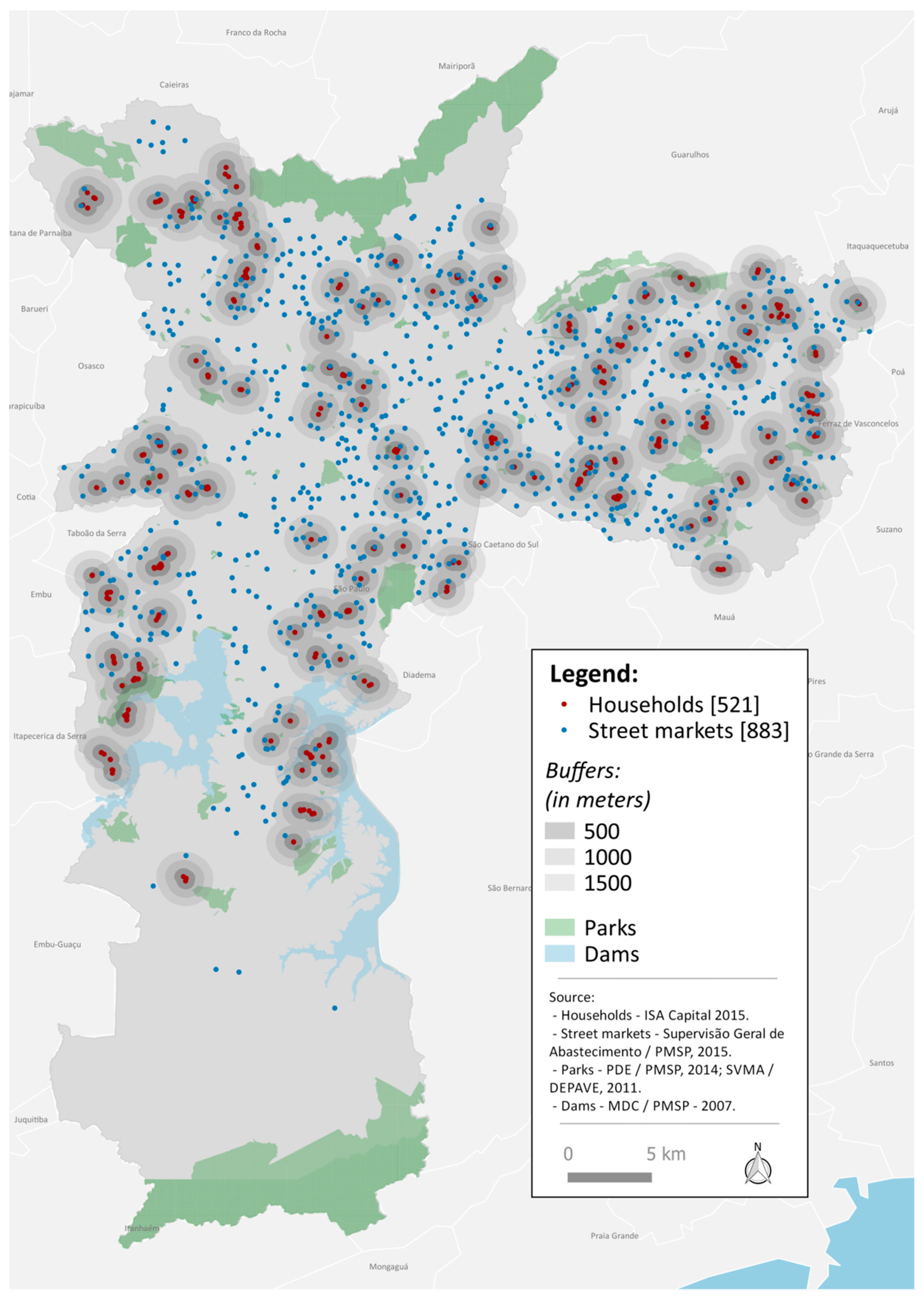
2.5. Street Markets and Households
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization. Fruit and Vegetables for Health. In Proceedings of the Joint FAO/WHO Workshop on Fruit and Vegetables for Health, Kobe, Japan, 1–3 September 2004; WHO: Geneva, Switzerland, 2004. [Google Scholar]
- GBD 2013 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 2287–2323. [Google Scholar]
- Boeing, H.; Bechthold, A.; Bub, A.; Ellinger, S.; Haller, D.; Kroke, A.; Leschik-Bonnet, E.; Müller, M.J.; Oberritter, H.; Schulze, M.; et al. Critical review: Vegetables and fruit in the prevention of chronic diseases. Eur. J. Nutr. 2012, 51, 637–663. [Google Scholar] [CrossRef] [PubMed]
- Neumark-Sztainer, D.; Wall, M.; Perry, C.; Story, M. Correlates of fruit and vegetable intake among adolescents Findings from Project EAT. Prev. Med. 2003, 37, 198–208. [Google Scholar] [CrossRef]
- Paz, C.J.R.; de Sousa Leite, K.B.; dos Anjos, N.A.; Fagundes, L.C.; de Souza, M.F.N.S.; Freitas, D.A. A influência da nutrição adequada e da prática de atividades física na saúde dos adolescentes. Rev. Portal Saúde Soc. 2017, 2, 332–346. [Google Scholar]
- Albani, V.; Butler, L.T.; Traill, W.B.; Kennedy, O.B. Fruit and vegetable intake: Change with age across childhood and adolescence. Br. J. Nutr. 2017, 117, 759–765. [Google Scholar] [CrossRef] [PubMed]
- De Moura Souza, A.; Barufaldi, L.A.; de Azevedo Abreu, G.; Giannini, D.T.; de Oliveira, C.L.; dos Santos, M.M.; Leal, V.S.; de Assis Guedes Vasconcelos, F. ERICA: Intake of macro and micronutrients of Brazilian adolescents. Rev. Saude Publica 2016, 50. [Google Scholar] [CrossRef]
- Andrade, S.C.; Previdelli, A.N.; Cesar, C.L.; Marchioni, D.M.; Fisberg, R.M. Trends is diet quality among adolescents, adults and older adults: A population-based study. Prev. Med. Rep. 2016, 4, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Rose, D.; Richards, R. Food store Access and household fruit and vegetable use among participants in the US Food Stamp Program. Public Health Nutr. 2004, 7, 1081–1088. [Google Scholar] [CrossRef] [PubMed]
- Santana, P.; Santos, R.; Nogueira, H. The link between local environment and obesity: A multilevel analysis in the Lisbon metropolitan area, Portugal. Soc. Sci. Med. 2009, 68, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Carroll-Scott, A.M.; Gilstad-Hayden, K.; Rosenthal, L.; Peters, S.M.; McCaslin, C.; Joyce, R.; Ickovics, J.R. Disentangling neighbourhood contextual associations with child body mass índex, diet, and physical activity: The role of built, socioeconomic, and social environments. Soc. Sci. Med. 2013, 95, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Swinburn, B.; Vandevijvere, S.; Kraak, V.; Sacks, G.; Snowdon, W.; Hawkes, C.; Barquera, S.; Friel, S.; Kelly, B.; Kumanyika, S.; et al. Monitoring and benchmarking government policies and actions to improve the healthiness of food environments: A proposed Government Healthy Food Environment Policy Index. Obes. Rev. 2013, 14, 24–37. [Google Scholar] [CrossRef] [PubMed]
- Wrigley, N.; Warm, D.; Margetts, B. Deprivation, diet, and food-retail Access: Findings from the Leeds ‘food deserts’ study. Environ. Plan. A Econ. Space 2003, 35, 151–188. [Google Scholar] [CrossRef]
- Swinburn, B.; Sacks, G.; Vandevijvere, S.; Kumanyika, S.; Lobstein, T.; Neal, B.; Barquera, S.; Friel, S.; Hawkes, C.; Kelly, B.; et al. INFORMAS (International Network for Food and Obesity/non-communicable diseases Research, Monitoring and Action Suport): Overview and key principles. Obes. Rev. 2013, 14, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Kubik, M.Y.; Lytle, L.A.; Hannan, P.J.; Perry, C.L.; Story, M. The association of the school food environment with dietary behaviors of young adolescents. Am. J. Public Health 2003, 93, 1168–1173. [Google Scholar] [CrossRef] [PubMed]
- Hanson, N.I.; Neumark-Sztainer, D.; Eisenberg, M.E.; Story, M.; Wall, M. Associations between parental report of the home food environment and adolescent intakes of fruits, vegetables and dairy foods. Public Health Nutr. 2005, 8, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Arcan, C.; Neumark-Sztainer, D.; Hannan, P.; Berg, P.; Story, M.; Larson, N. Parental eating behaviours, home food environment and adolescent intakes of fruits, vegetables and dairy foods: Longitudinal findings from Project EAT. Public Health Nutr. 2007, 10, 1257–1265. [Google Scholar] [CrossRef] [PubMed]
- Ding, D.; Sallis, J.F.; Norman, G.J.; Saelens, B.E.; Harris, S.K.; Kerr, J.; Rosenberg, D.; Durant, N.; Glanz, K. Community food environment, home food environment, and fruit and vegetable intake of children and adolescents. J. Nutr. Educ. Behav. 2012, 44, 634–638. [Google Scholar] [CrossRef] [PubMed]
- Turrel, G.; Hewitt, B.; Patterson, C.; Oldenburg, B. Measuring socio-economic position in dietary research: Is choice of socio-economic indicator important? Public Health Nutr. 2003, 6, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Darmon, N.; Drewnowski, A. Contribution of food prices and diet cost to socioeconomic disparities in diet quality and health: A systematic review and analysis. Nutr. Rev. 2015, 73, 643–660. [Google Scholar] [CrossRef] [PubMed]
- Kamphuis, C.M.B.; Giskes, K.; Bruijn, G.; Wendel-Vos, W.; Brug, W.; Lenthe, F.J. Environmental determinants of fruit and vegetable consumption among adults: A systematic review. Br. J. Nutr. 2006, 96, 620–635. [Google Scholar] [PubMed]
- Bigio, R.S.; Junior, E.V.; Castro, M.A.; César, C.L.G.; Fisberg, R.M.; Marchioni, D.M.L. Determinants of fruit and vegetable intake in adolescents using quantile regression. Rev. Saude Publica 2011, 45, 448–456. [Google Scholar] [CrossRef]
- Fisberg, R.M.; Sales, C.H.; Fontanelli, M.M.; Pereira, J.L.; Alves, M.C.G.P.; Escuder, M.M.L.; César, C.L.G.; Goldbaum, M. 2015 Health Survey of São Paulo with focus in Nutrition: Rationale, Design, and Procedures. Nutrient 2018, 10, 169. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Matsudo, S.; Araujo, T.; Matsudo, V.; Andrade, D.; Andrade, E.; Oliveira, L.C.; Braggion, G. Questionário internacional de atividade física (IPAQ) estudo de validade e reprodutibilidade no Brasil. Rev. Bras. Ativ. Fis. Saude 2001, 6, 5–18. [Google Scholar] [CrossRef]
- World Health Organization. Global Recommendations on Physical Activity for Health. Available online: http://www.who.int/dietphysicalactivity/factsheet_recommendations/en/ (accessed on 15 January 2018).
- World Health Organization. Child and Growth Standards: Length/Height-Forage, Weight-for-Age, Weight-for-Length, Weight-for-Height and Body Mass Index-Forage: Methods and Development. Available online: http://www.who.int/childgrowth/standards/Technical_report.pdf?ua=1 (accessed on 15 January 2018).
- Carvalho, A.M.; Piovezan, L.G.; Selem, S.S.C.; Fisberg, R.M.; Marchioni, D.M.L. Validation and calibration of self-reported weight and height from individuals in the city of São Paulo. Rev. Bras. Epidemiol. 2014, 17, 735–746. [Google Scholar] [CrossRef] [PubMed]
- Programa das Nações Unidas para o Desenvolvimento. Available online: http://atlasbrasil.org.br/2013 (accessed on 20 November 2017).
- Raper, N.; Perloff, B.; Ingwersen, L.; Steinfeldt, L.; Anand, J. An overview of USDA’s Dietary Intake Data System. J. Food Compos. Anal. 2004, 17, 545–555. [Google Scholar] [CrossRef]
- Núcleo de Estudos e Pesquisas em Alimentação (NEPA), Universidade Estadual de Campinas. Tabela Brasileira de Composição de Alimentos, 4rd ed.; NEPA-UNICAMP: Campinas, Brazil, 2011. [Google Scholar]
- Haubrock, J.; Nöthlings, U.; Volatier, J.L.; Dekkers, A.; Ocké, M.; Harting, U.; Illner, A.K.; Knüppel, S.; Andersen, L.F.; Boeing, H.; et al. Estimating usual food intake distributions by using the multiple source method in the EPIC-Potsdam Calibration Study. J. Nutr. 2011, 141, 914–920. [Google Scholar] [CrossRef] [PubMed]
- Municipality of Sao Paulo. GeoSampa. Available online: http://geosampa.prefeitura.sp.gov.br/PaginasPublicas/_SBC.aspx (accessed on 26 November 2017).
- Florindo, A.A.; Barrozo, L.V.; Cabral-Miranda, W.; Rodrigues, E.Q.; Turrell, G.; Goldbaum, M.; Cesar, C.L.G.; Giles-Corti, B. Public open spaces and leisure-time walking in Brazilian adults. Int. J. Environ. Res. Public Health 2017, 14, 553. [Google Scholar] [CrossRef] [PubMed]
- Duran, A.C.; Almeida, S.L.; Latorre, M.R.; Jaime, P.C. The role of the local retail food environment in fruit, vegetable and sugar-sweetened beverage consumption in Brazil. Public Health Nutr. 2015, 19, 1093–1102. [Google Scholar] [CrossRef] [PubMed]
- Ministério da Saúde. Guia Alimentar para a População Brasileira: Promovendo a Alimentação Saudável; Ministério da Saúde, Secretaria de Atenção à Saúde, Departamento de Atenção Básica: Brasília, Brazil, 2008; pp. 1–210.
- Machado, P.P.; Claro, R.M.; Martins, A.P.B.; Costa, J.C.; Levy, R.B. Is food store type associated with the consumption of ultra-processed food and drink products in Brazil? Public Health Nutr. 2018, 21, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Passos, J.A.; Freitas, M.C.S.; Santos, L.A.S.; Soares, M.D. Meanings attributed to healthy eating by consumers of a street market. Rev. Nutr. 2017, 30, 261–270. [Google Scholar] [CrossRef]
- Florido, J.M.P. Avaliação da Diversidade de Frutas e Hortaliças Frutosas Comercializadas no Município de São Paulo: Composição Nutricional de Macro e Micronutrientes; Universidade de São Paulo: São Paulo, Brazil, 2015. [Google Scholar]
- Hill, L.; Casswell, S.; Maskill, C.; Jones, S.; Wyllie, A. Fruit and vegetables as adolescent food choices in New Zealand. Health Promot. Int. 1998, 35, 55–65. [Google Scholar] [CrossRef]
- Cowburn, G.; Mathews, A.; Doherty, A.; Hamilton, A.; Kelly, P.; Williams, J.; Foster, C.; Nelson, M. Exploring the opportunities for food and drink purchasing and consumption by teenagers during their journeys between home and school: A feasibility study using a novel method. Public Health Nutr. 2016, 19, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Engler-Stringer, R.; Schaefer, J.; Ridalls, T. An examination of the roles played by early adolescent children in interactions with their local food environment. Can. J. Public Health 2016, 107 (Suppl. 1), eS48–eS52. [Google Scholar] [CrossRef] [PubMed]
- Rasmussem, M.; Krølner, R.; Klepp, K.; Lytle, L.; Brug, J.; Due, P. Determinants of fruit and vegetable consumption among children and adolescents: A review of the literature. Part I: Quantitative studies. Int. J. Behav. Nutr. Phys. Act. 2006, 3, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministério da Saúde. Política Nacional de Alimentação e Nutrição. Available online: http://dab.saude.gov.br/portaldab/pnan.php (accessed on 9 March 2018).
- Fundo Nacional de Desenvolvimento da Educação, Ministério da Educação. Programa Nacional de Alimentação Escolar. Available online: http://www.fnde.gov.br/programas/pnae (accessed on 9 March 2018).
- Ministério do Desenvolvimento Social e Combate à Fome. Secretaria Nacional de Segurança Alimentar e Nutricional. In Marco de Referência de Educação Alimentar e Nutricional para as Políticas Públicas; Ministério do Desenvolvimento Social e Combate à Fome: Brasília, Brazil, 2012. [Google Scholar]
- Claro, R.M.; Monteiro, C.A. Family income, food prices, and household purchases of fruits and vegetables in Brazil. Rev. Saude Publica 2010, 44, 1014–1020. [Google Scholar] [CrossRef]
- United States Department of Agriculture. Economic Research Service. Low-Income Households Expenditures on Fruits and Vegetables. Available online: https://www.ers.usda.gov/publications/pub-details/?pubid=41663 (accessed on 15 January 2018).
- Winkler, E.; Turrell, G.; Patterson, C. Does living in a disadvantaged area mean fewer opportunities to purchase fresh fruit and vegetables in the area? Findings from the Brisbane food study. Health Place 2006, 12, 306–319. [Google Scholar] [CrossRef] [PubMed]
- John, J.; Ziebland, S. Reported barriers to eating more fruit and vegetables before and after participation in a randomized controlled trial: A qualitative study. Health Educ. Res. 2004, 62, 387–395. [Google Scholar] [CrossRef] [PubMed]
- Moore, L.V.; Roux, A.V.D.; Nettleton, J.A.; Jacobs, D.R.; Franco, M. Fast-food consumption, diet quality, and neighborhood exposure to fast-food. Am. J. Epidemiol. 2009, 170, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Fleischhacker, S.E.; Evenson, K.R.; Rodriguez, D.A.; Ammerman, A.S. A systematic review of fast food access studies. Obes. Rev. 2011, 12, e460–e471. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Variables | n (%) | <P75 | ≥P75 | p Value |
|---|---|---|---|---|
| n (%) | n (%) | |||
| Age (years, n = 521) | ||||
| 12–15 | 270 (51.8) | 208 (77.1) | 62 (22.9) | 0.227 |
| 16–19 | 251 (48.2) | 183 (72.9) | 68 (27.1) | |
| Sex (n = 521) | ||||
| Male | 264 (50.7) | 197 (74.6) | 67 (25.4) | 0.820 |
| Female | 257 (49.3) | 194 (75.4) | 63 (24.6) | |
| Race (n = 517) | ||||
| White | 221 (42.7) | 158 (71.5) | 63 (28.5) | 0.088 |
| Non-white | 296 (57.3) | 231 (78.0) | 65 (22.0) | |
| Family income per capita (n = 497) * | ||||
| ≤1 Minimum wage | 296 (59.6) | 235 (79.4) | 61 (20.6) | 0.039 |
| >1 Minimum wage | 121 (24.3) | 82 (67.8) | 39 (32.2) | |
| No response | 80 (16.1) | |||
| Education of the household head (n = 495) | ||||
| ≤9 years | 242 (48.9) | 194 (80.2) | 48 (19.8) | 0.003 |
| 10–12 years | 157 (31.7) | 103 (65.6) | 54 (34.4) | |
| >12 years | 96 (19.4) | 76 (79.2) | 20 (20.8) | |
| Leisure physical activity (n = 521) | ||||
| Does not comply with recommendation | 418 (80.2) | 323 (77.3) | 95 (22.7) | 0.018 |
| Complies with recommendation | 103 (19.8) | 68 (66.0) | 35 (34.0) | |
| Body Mass Index (n = 504) | ||||
| Non-overweight | 355 (70.4) | 266 (74.9) | 89 (25.1) | 0.707 |
| Overweight | 149 (29.6) | 114 (76.5) | 35 (23.5) | |
| Years of residence (n = 521) | ||||
| ≤5 | 184 (35.3) | 134 (72.8) | 50 (27.2) | 0.386 |
| >5 | 337 (64.7) | 257 (76.3) | 80 (23.7) | |
| Street market density 500 m buffer | ||||
| 0 | 258 (49.5) | 198 (76.7) | 60 (23.3) | 0.055 |
| 1 | 155 (29.8) | 106 (68.4) | 49 (31.6) | |
| ≥2 | 108 (20.7) | 87 (80.6) | 21 (19.4) | |
| Street market density 1000 m buffer | ||||
| ≤1 | 124 (23.8) | 98 (79.0) | 26 (21.0) | 0.268 |
| 2–4 | 281 (53.9) | 203 (72.2) | 78 (27.8) | |
| ≥5 | 116 (22.3) | 90 (77.6) | 26 (22.4) | |
| Street market density 1500 m buffer | ||||
| ≤2 | 101 (19.4) | 84 (83.2) | 17 (16.8) | 0.093 |
| 3–7 | 232 (44.5) | 167 (72.0) | 65 (28.0) | |
| ≥8 | 188 (36.1) | 140 (74.5) | 48 (25.5) |
| Variable | OR (95% CI) |
|---|---|
| 500 m buffer | |
| Street market density | |
| 0 | ref |
| 1 | 1.73 (1.01–3.00) * |
| ≥2 | 0.70 (0.35–1.42) |
| Family income per capita | |
| ≤1 Minimum wage | ref |
| >1 Minimum wage | 2.56 (1.47–4.45) * |
| 1000 m buffer | |
| Street market density | |
| ≤1 | ref |
| 2–4 | 1.33 (0.70–2.53) |
| ≥5 | 0.93 (0.41–2.12) |
| Family income per capita | |
| ≤1 Minimum wage | ref |
| >1 Minimum wage | 2.30 (1.33–3.96) * |
| 1500 m buffer | |
| Street market density | |
| ≤2 | ref |
| 3–7 | 1.97 (0.96–4.04) |
| ≥8 | 1.51 (0.67–3.44) |
| Family income per capita | |
| ≤1 Minimum wage | ref |
| >1 Minimum wage | 2.32 (1.35–4.00) * |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nogueira, L.R.; Fontanelli, M.D.M.; Aguiar, B.S.d.; Failla, M.A.; Florindo, A.A.; Barrozo, L.V.; Goldbaum, M.; Cesar, C.L.G.; Alves, M.C.G.P.; Fisberg, R.M. Access to Street Markets and Consumption of Fruits and Vegetables by Adolescents Living in São Paulo, Brazil. Int. J. Environ. Res. Public Health 2018, 15, 517. https://doi.org/10.3390/ijerph15030517
Nogueira LR, Fontanelli MDM, Aguiar BSd, Failla MA, Florindo AA, Barrozo LV, Goldbaum M, Cesar CLG, Alves MCGP, Fisberg RM. Access to Street Markets and Consumption of Fruits and Vegetables by Adolescents Living in São Paulo, Brazil. International Journal of Environmental Research and Public Health. 2018; 15(3):517. https://doi.org/10.3390/ijerph15030517
Chicago/Turabian StyleNogueira, Luana Romão, Mariane De Mello Fontanelli, Breno Souza de Aguiar, Marcelo Antunes Failla, Alex Antonio Florindo, Ligia Vizeu Barrozo, Moisés Goldbaum, Chester Luiz Galvão Cesar, Maria Cecilia Goi Porto Alves, and Regina Mara Fisberg. 2018. "Access to Street Markets and Consumption of Fruits and Vegetables by Adolescents Living in São Paulo, Brazil" International Journal of Environmental Research and Public Health 15, no. 3: 517. https://doi.org/10.3390/ijerph15030517