To test the conceptual logic and the extent to which the approach could be applied based on current knowledge, data and tools, a spreadsheet-based model was developed. This section details the model and its application to a hypothetical case, using data from Dhaka (Bangladesh) [
60] based on literature only and no field research or local consultation. As additional assumptions were required for the purpose of modelling, all results presented here are solely for illustration of the modelling process and model outputs, and should not be taken as real results for Dhaka. We present the modelling steps (see
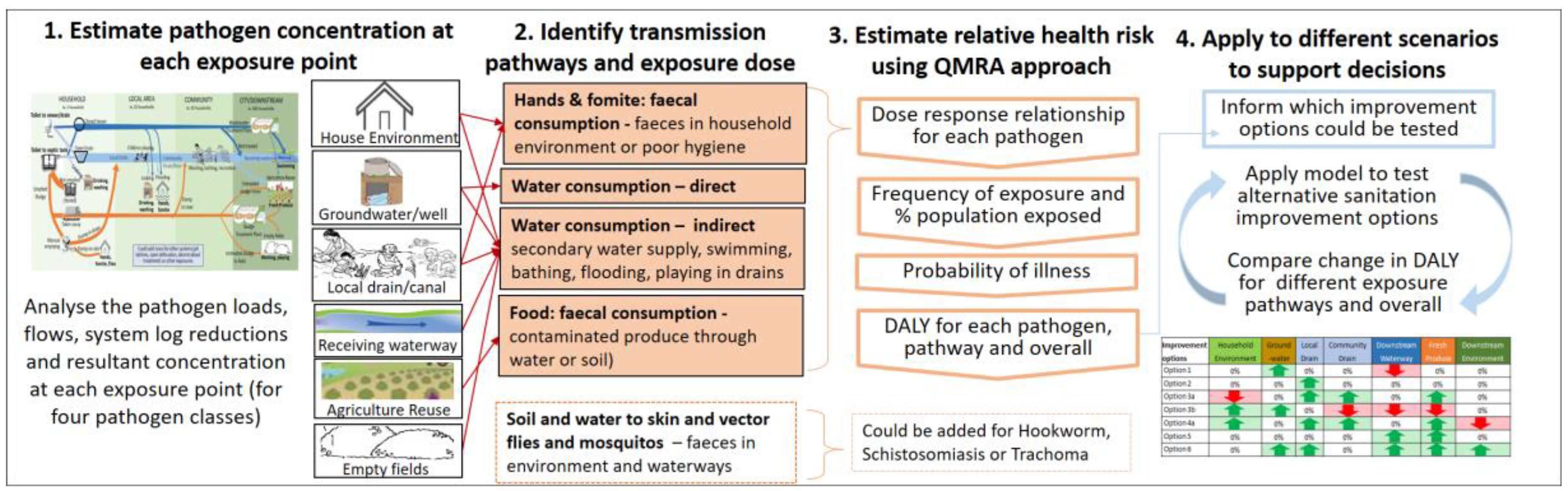
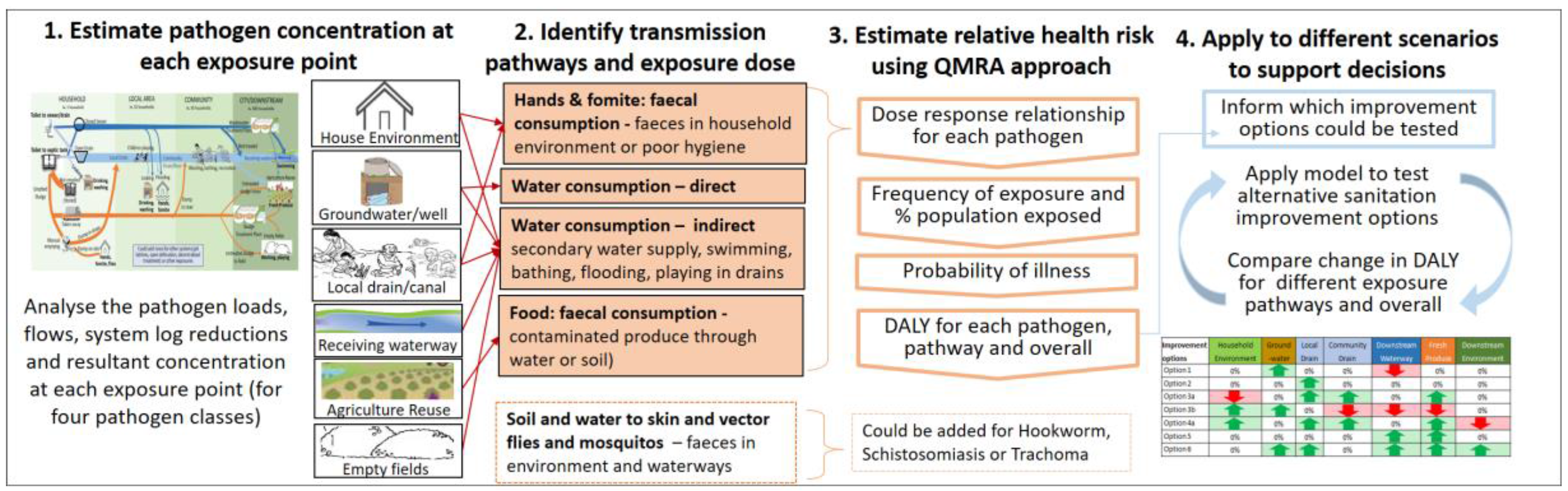
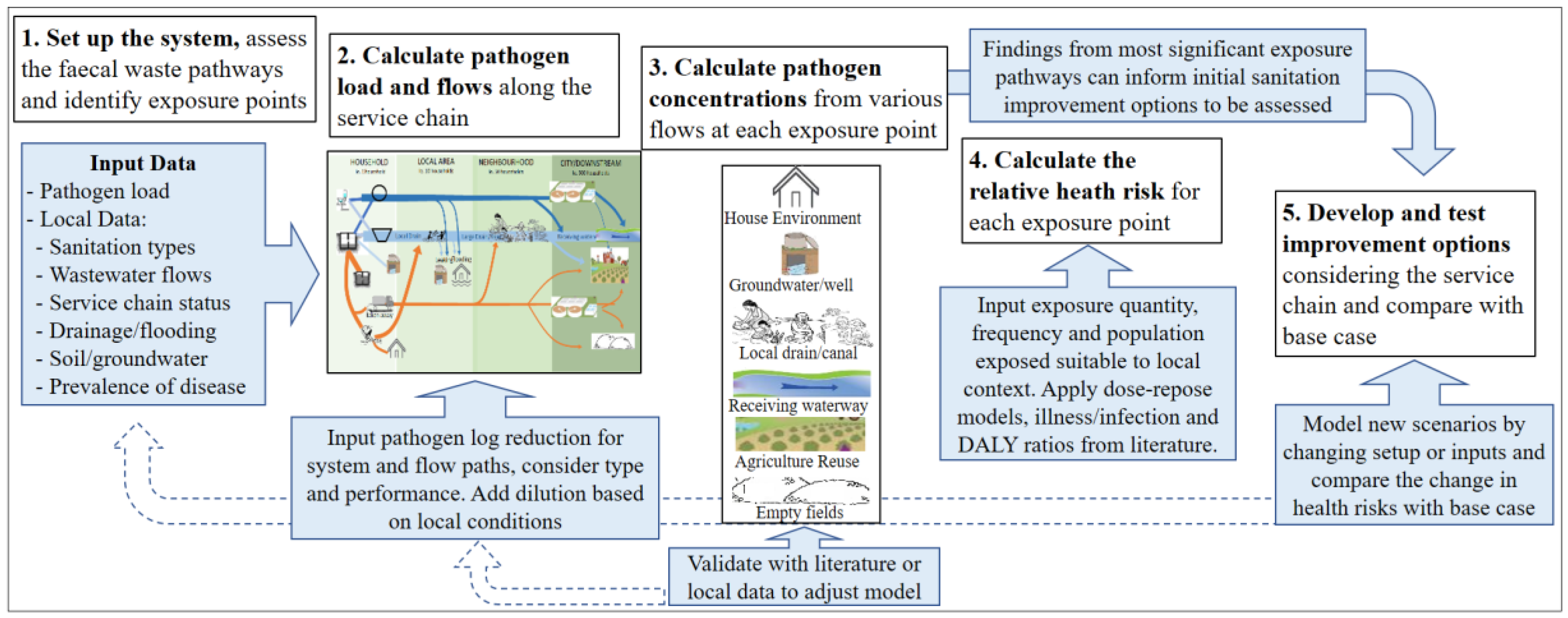
Figure 3) in the context of the hypothetical case, including the status of existing evidence and relative reliability of assumptions in each part of the model. The model is at a preliminary stage, suitable for the purposes of demonstrating and illustrating the conceptual approach only. Further development is required to test inputs and assumptions of particular urban contexts, including validation of the inputs and sensitivity testing. This paper therefore only presents an illustrative example rather than quantitative results. The intent is to demonstrate the types of model outputs and therefore show how the conceptual approach could feasibly support decision-making.
Description of Illustrative Case
The illustrative case was primarily based on data from the Dhaka Bangladesh SFD report [
60] shown in
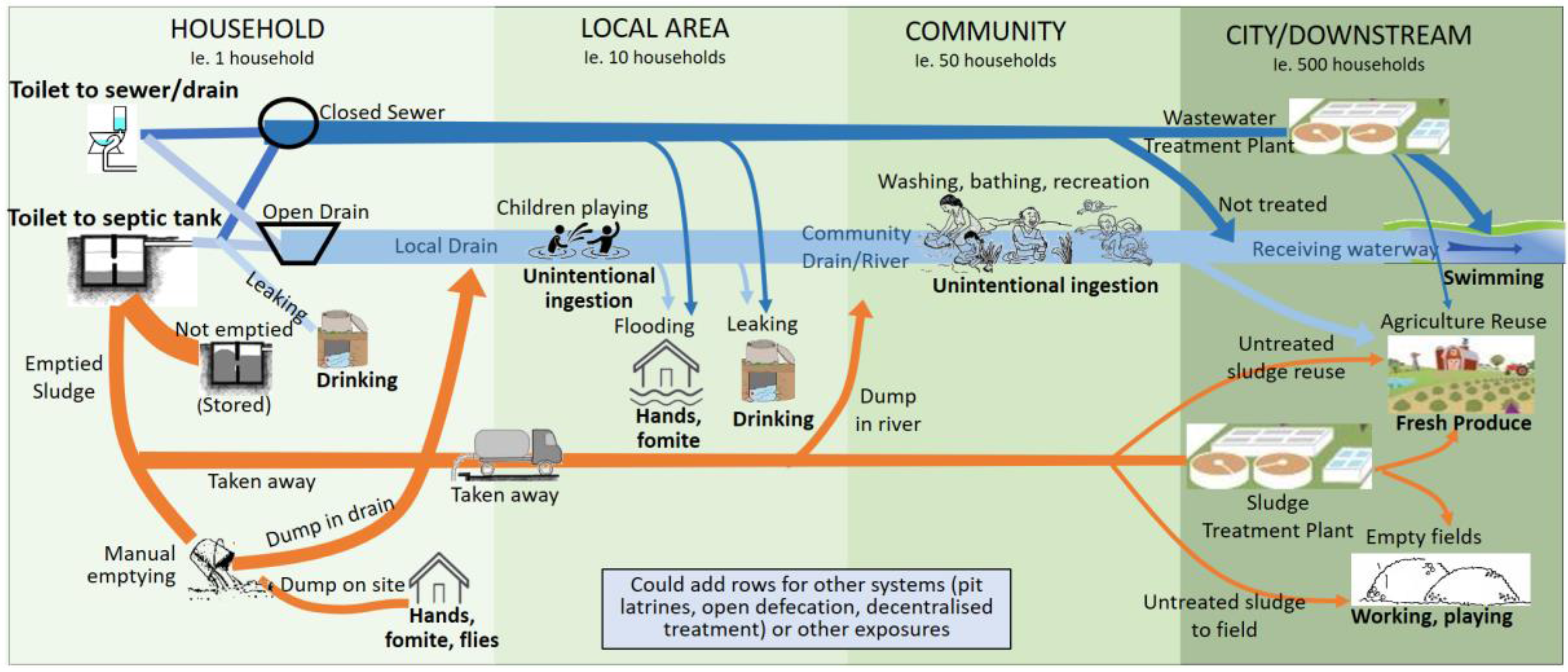
Table 2 with additional parameters added for the purposes of the modelling exercise. This case represents a typical situation in which significant proportions of faecal matter are discharged to the urban environment, at each of the containment, conveyance and disposal steps in the service chain.
Step 1. Set up the system: The scale of this assessment was set at the city level as per the SFD, noting that smaller community/sub-sections such as an urban slum could also be modelled where more appropriate. The SFD approach was used as a basis to estimate the division of faecal waste flows for each type of sanitation in the service chain, the types of conveyance (e.g., vacuum tanker), the location of sludge discharge or dumping (e.g., next to the pit, in the local drain, to downstream waterway or land), and the destinations of flows not reaching the treatment system (i.e., leaking, flooding, diverted to river). This example was limited to water-based sanitation including toilet-to-drain, toilet-to-sewer and toilet-to-septic-tank, although other sanitation systems and scales are feasible. Pathogen inputs were estimated from available literature. A representative pathogen was chosen for each pathogen class (bacteria (pathogenic
E. coli), protozoa (Cryptosporidium), virus (rotavirus) and helminth (Ascaris)) with a load of 10
5–11/person/day (see
Supplementary Materials Table S1), with an infection prevalence ranging from 2% to 24% [
61]. While the conceptual approach did not include population density, this dimension is considered important for predicting pathogen dilution factors, concentrations and exposure, and could be added into future versions of the model.
Step 2. Calculate the flows: In the absence of local data, to translate SFD per-population figures to volumes and flows, we used a standard assumption of 100 L/p/d water use with 30% discharged to the toilet [
62]. Pathogen reduction by removal (i.e., containment, or filtration by soil) or inactivation (e.g., die-off, treatment) was estimated on the basis of available literature and expert opinion (see
Supplementary Materials Table S2). Similar to the SFD process, working from left to right for each type of sanitation infrastructure, we used the SFD flow divisions to calculate the wastewater flow and pathogen load for each stream and we applied the system log
10 reductions as pathogens passed through various treatment systems (septic tank, soil, etc.) or to account for die-off (i.e., in drains, groundwater, fields, etc.). A base flow and a dilution factor were used to account for additional inflows or dispersion when faecal waste enters the environment (such as discharging to local or community-scale drains, entering groundwater, or discharging to land or produce). While the preliminary dilution inputs were based on expected greywater flows, the dilution in the environment was recognised as a factor that requires understanding of local conditions and waste disposal practices. Our chosen approach for this illustrative case is described below as a part of Step 3.
Step 3. Calculate the pathogen concentration: The pathogen concentration at each exposure point was calculated as the sum of pathogen loads divided by the flows discharged to that exposure point via the different pathways, calculated separately for each pathogen. These values were compared with pathogen concentrations noted in the literature (
Supplementary Materials Table S6) and adjustments made to the dilution to ensure the calculated concentrations were of a similar order of magnitude to those noted in literature. Available literature for different pathogen classes and pathways was limited, for some pathways only
E. coli data was available. Use of local data and better consideration of the hydrological factors would improve the modelling of dilution, while local environmental monitoring would be valuable to test the validity of inputs and approach.
Step 4. Calculate the probability of illness: Along with the calculated concentration for each pathogen at each exposure point, we used data from the literature to estimate exposure volume, frequency and exposed population (see
Supplementary Materials Tables S3–S5). For each pathogen and each exposure pathway we calculated the dose, daily probability of infection and illness, annual probability of illness, and annual DALY per person; the annual DALY per person was multiplied by the percentage of population exposed to each exposure point for adults and children separately. The results across the four pathogen groups were then summed to estimate a “DALY per exposure point”, and summed to estimate the overall DALY for the base case.
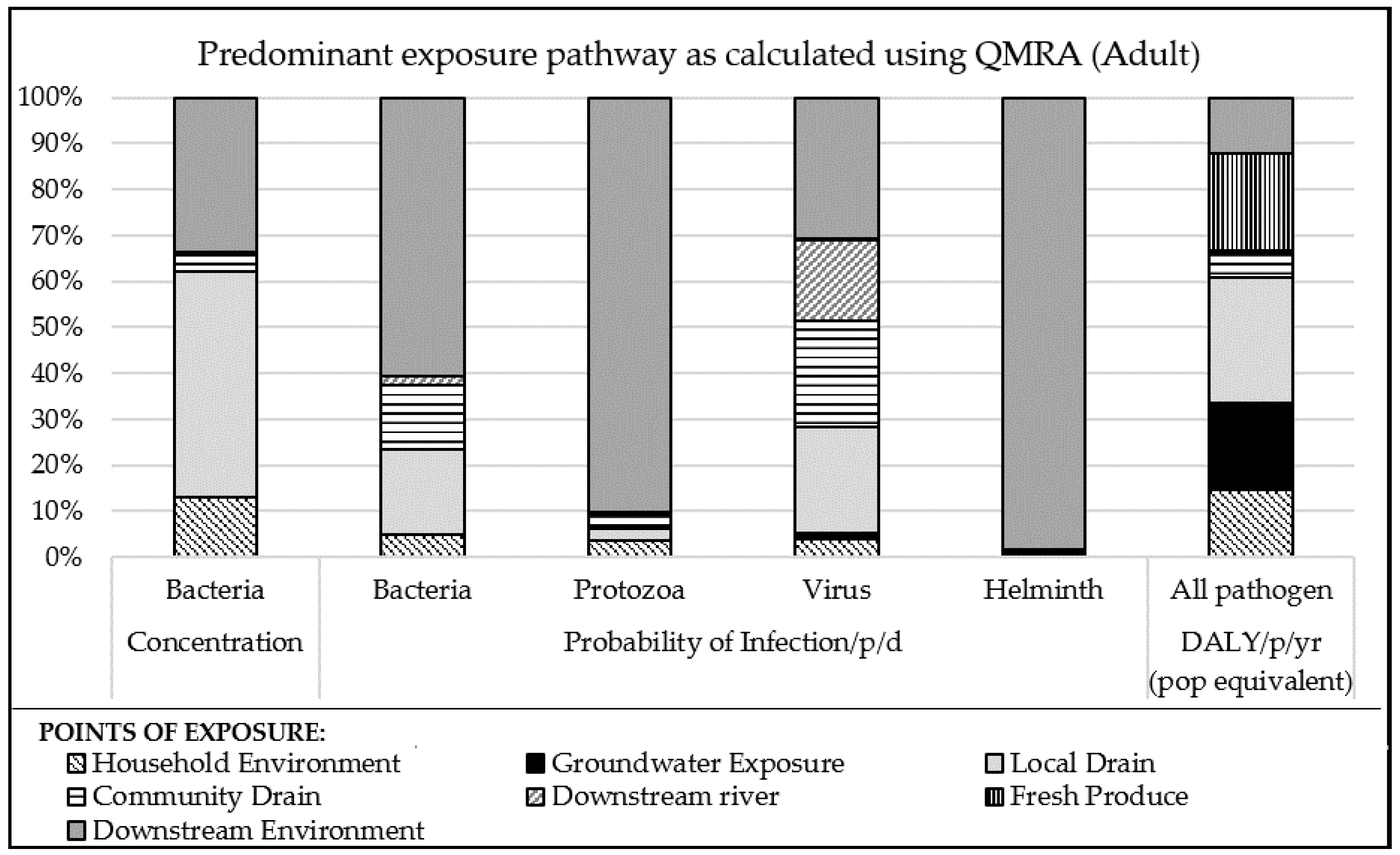
Figure 4 presents one possible type of output from the model, which identifies the change in priority pathways depending on which of three parameters is considered: bacteria concentration, pathogen specific infection probability, and the resultant overall DALYs using QMRA.
The results in
Figure 4 highlight that inferences based on indicator bacteria concentration will result in different conclusions than inferences based on probability of infection or DALY. For example, in this case considering bacteria concentration alone could lead to the local drain being assessed as most important, and other important pathways are likely to be missed. The results of the probability of infection (considering dose and dose response) for the four pathogen types also demonstrates that the most important pathways varied for different pathogens, and highlights the importance of this aspect to the conceptual approach described in this paper. The health risk (based on illness and DALY ratios, exposure frequency and proportion of population exposed) demonstrates that there are contributions to this relative health risk through many different pathways, which help point to alternative sanitation options that could address these risks. The high proportion of DALYs from Groundwater and Fresh Produce exposure is influenced by the high assumed frequency of exposure (every day for Groundwater, 5 instances per week for Produce) and high proportion of the population exposed (35% population use groundwater, 65% consume fresh produce directly or indirectly irrigated or fertilised with faecal waste). The sensitivity of the model to exposure inputs should be assessed and highlights the need for local data, as is argued by Robb [
7].
Due to the high infectivity of rotavirus and high excreted load, the probability of infection was high across all pathways (the reason these appear equally important in
Figure 4). The subsequent step of calculating the annual probability of illness increased the probability to close to one (100% probability) and resulted in little change in the DALYs from viruses between improvement options. On review of the model results, we propose that the use of an annualised probability (maximum one illness per year) should be compared with a daily probability (each day has equal risk of illness) to understand the influence of the very high probability of annual illness on the results.
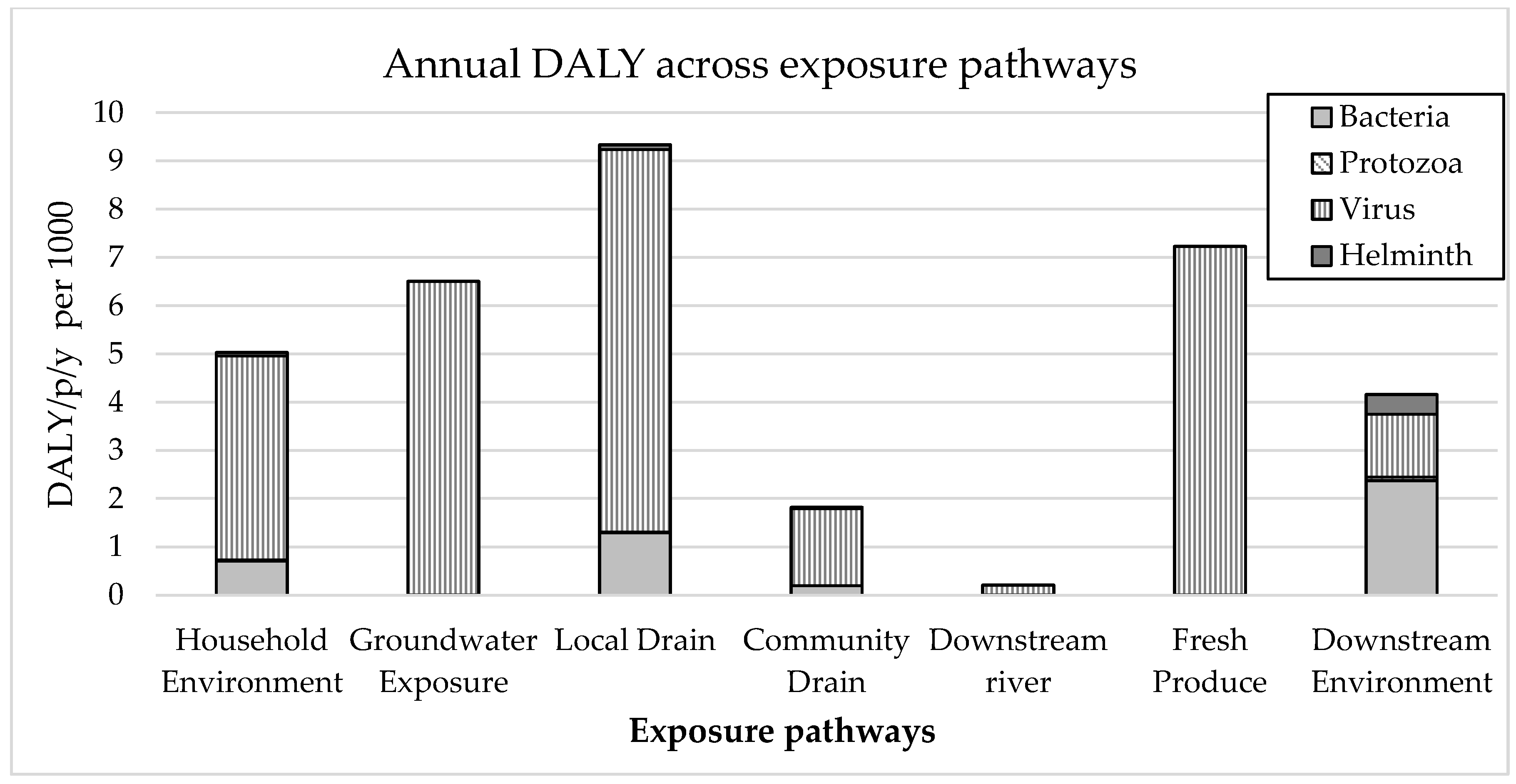
Figure 5 shows an example model output of the contribution of each pathogen type to relative health risks for each exposure point. This output is illustrative only, and demonstrates that using such a model, it is possible to estimate the relative importance (in terms of health risk) of different pathogens at different exposure points, which can subsequently inform identification of appropriate sanitation options that best prevent or treat this situation.
Figure 5 demonstrates that virus is the predominant pathogen class, as expected due to the high rate of infection and high DALY per illness of the modelled rotavirus. There is some variation of the relative significance of other pathogens between pathways with bacteria contributing to DALYs at household environment and local drain exposures, while helminths are a risk in downstream environment. The high risk of Local Drain could be expected, given the base case involves 34% of the population’s faecal waste discharging directly to drains, including 21% direct from toilet without any pre-treatment, while also contributing to high household environment risk due to the reported frequent flooding of sewers and drains. The source of faecal waste that reaches Fresh Produce is predominantly from septic tank effluent only, and not sludge, due to very low sludge emptying rates (
Table 2) which could explain the low levels of Helminth attributed diseases for Fresh Produce as Helminths are often reported to be more highly associated with the sludge than effluent.
The results shown in
Figure 5 also align with other QMRA assessments which found the exposure to open drain caused the highest contribution to the annual health risk [
5,
34]. Other studies concluded open drains were the second highest contributor, after fresh produce [
35] or after urban farmers working in wetlands [
33]. The findings on the predominance of viruses in contributing to health risks also aligns with findings in the literature. In three recent field studies viruses and also bacteria were found to contribute to a greater portion of the overall health risk than protozoa and helminths [
5,
33,
34].
These results are based on assumptions for the hypothetical base case and should not be interpreted as real findings for Dhaka or applied to other situations without further sensitivity testing and validation. The sensitivity of the model to the system log10 reduction assumptions should be further tested by considering the range of possible removal rates due to environmental and other variables. While the findings align with other studies, there is high uncertainty regarding the system log10 reduction assumptions due to a lack of available data for all pathogen classes. This required estimations to be made for some system log10 reductions, particularly for groundwater and for local drains. This reiterates the need to consider local conditions, as well as agricultural and consumption practices that affect log10 reduction, as well as further empirical research on the pathogen log10 reduction for all pathogen classes. These findings are illustrative only, presented to demonstrate how a model of this type can be used.
Step 5. Develop and test improvement options: Alternative sanitation improvement options were developed on the basis of the most significant exposure pathways determined from the base case assessment. For the hypothetical case above,
Figure 5 shows that exposure to local drains, household environment, groundwater and produce contribute the highest proportion of DALY for the adult population, therefore options that address these risks were developed and tested in the model. Specifically, six alternative sanitation options (including variations on these) were tested by revising the model set-up or inputs such as the flow division (i.e., reducing % sewer flows flooding), adjusting pathogen log
10 reductions (i.e., improving treatment efficacy) or exposure to reflect actual system improvements. Changes in the DALY were then compared with the base case (
Table 2). In
Table 3 we focus on the relative changes in health risk. We do not show quantitative results due to the uncertainties associated with certain aspects of the model and input data limitations (see
Section 4).
The illustrative findings demonstrate the use of the model in understanding how changes in technical, service and exposure could affect different exposure points or overall relative health risk. The results highlight that: (i) improvements can shift pathogen flows and health risks downstream (1, 3b, 4a); (ii) downstream interventions may have minimal overall impact (5) if, as was the case in this hypothetical study, the health risks are predominately in the upstream local area; (iii) increasing emptying may have little health impact (4a) if the base case assumes no exposure to unemptied/stored septic sludge. The options that demonstrated a highest potential overall impact were: reducing exposure by covering drains (2), addressing wastewater conveyance issue to reduce flows in open drains and increase those flows reaching treatment systems (3d) and a non-traditional option (cover drains, reduce groundwater use and discontinue reuse of untreated sludge and wastewater for food production) to address the key exposure pathways (6). This example shows the value of the model in systematically identifying preferable interventions from a health risk perspective and assessing their relative improvement at specific exposure points and overall.















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}