Prenatal Exposure to Environmental Tobacco Smoke and Early Development of Children in Rural Guizhou Province, China

Abstract
:1. Introduction
2. Materials and Methods
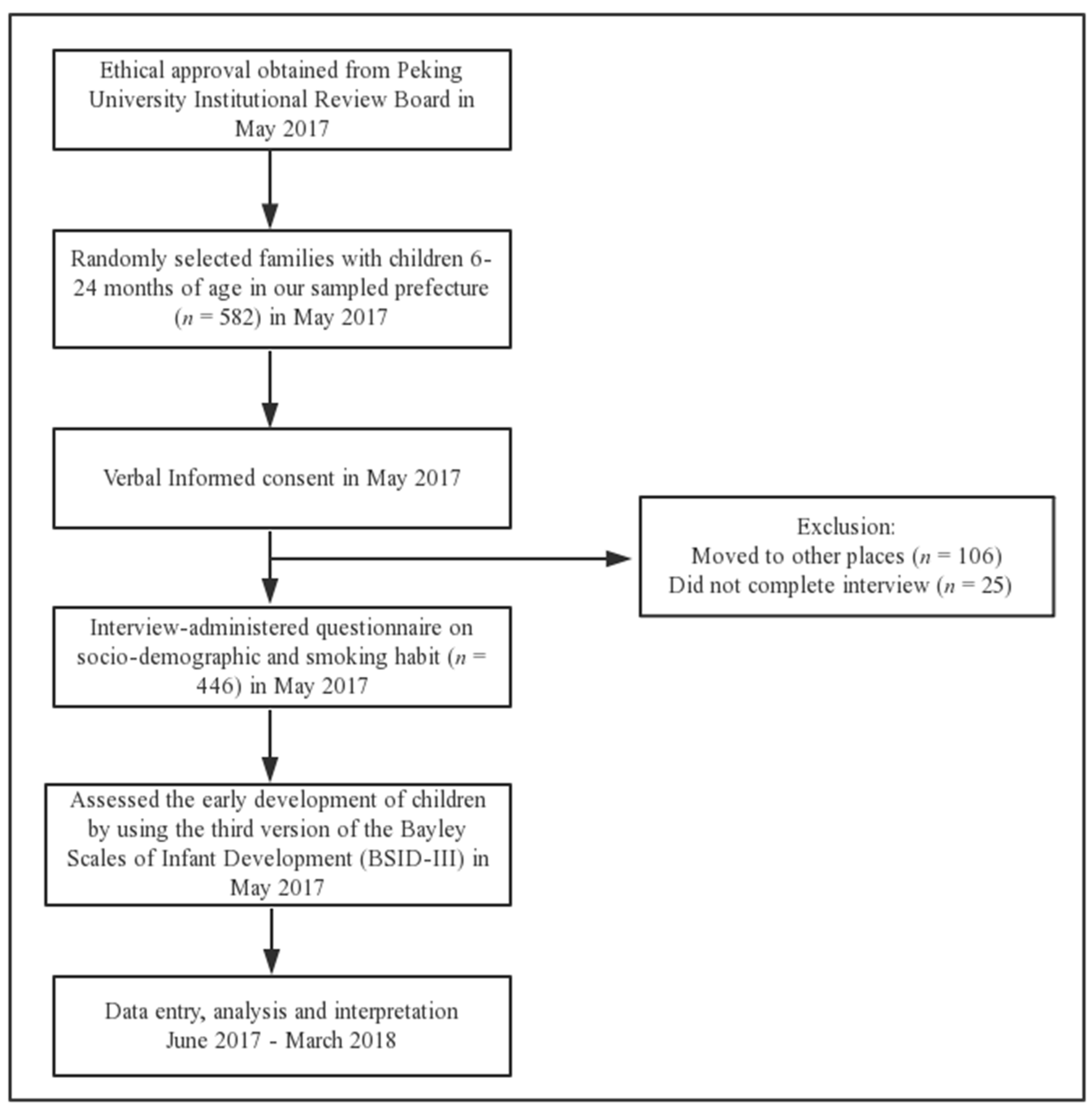
2.1. Study Participants
2.2. Data Collection
2.2.1. Socioeconomic Survey and Prenatal Exposure to ETS
2.2.2. Outcome Measures
2.2.3. Confounding Factors
2.3. Statistical Analysis
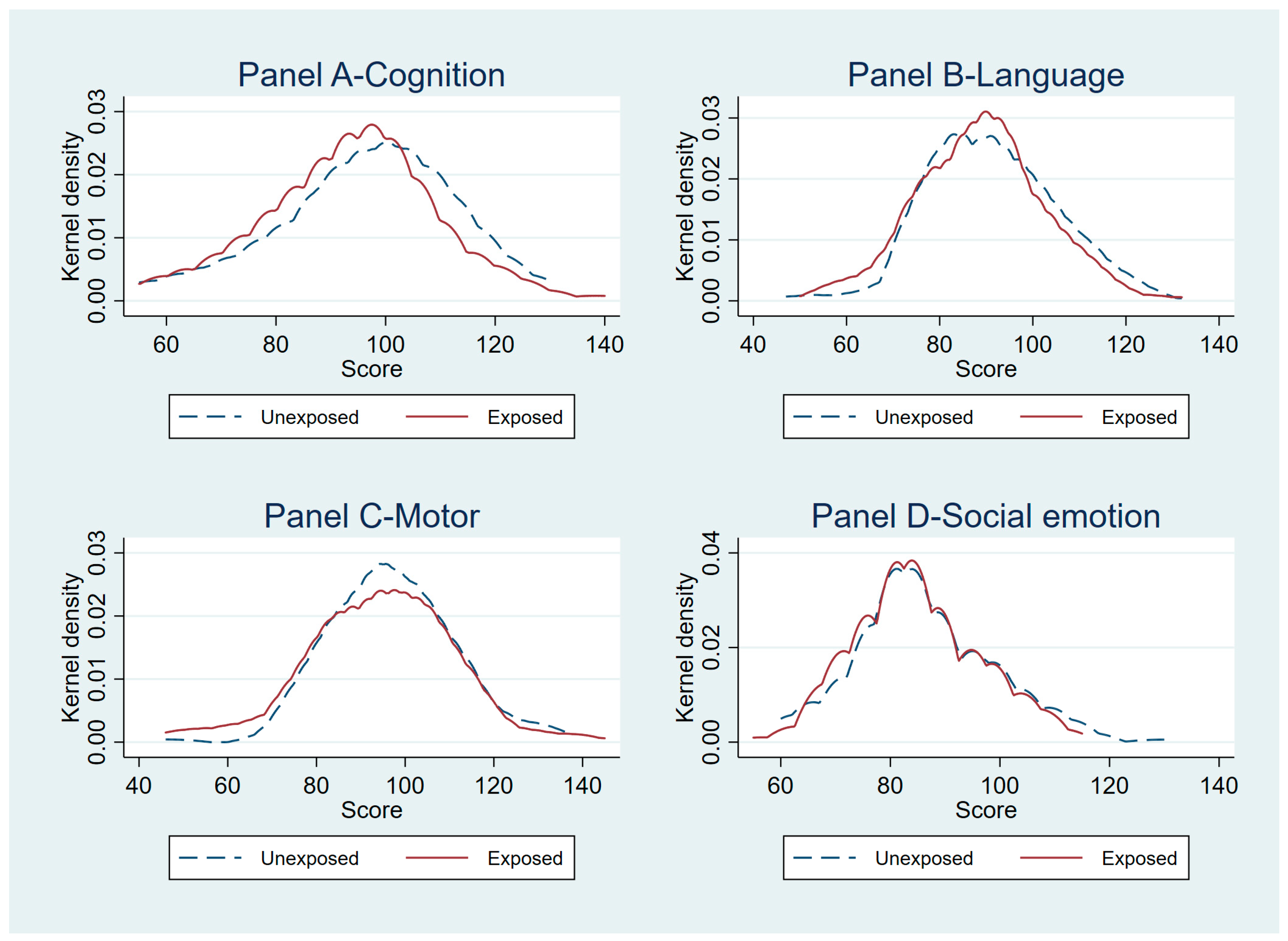
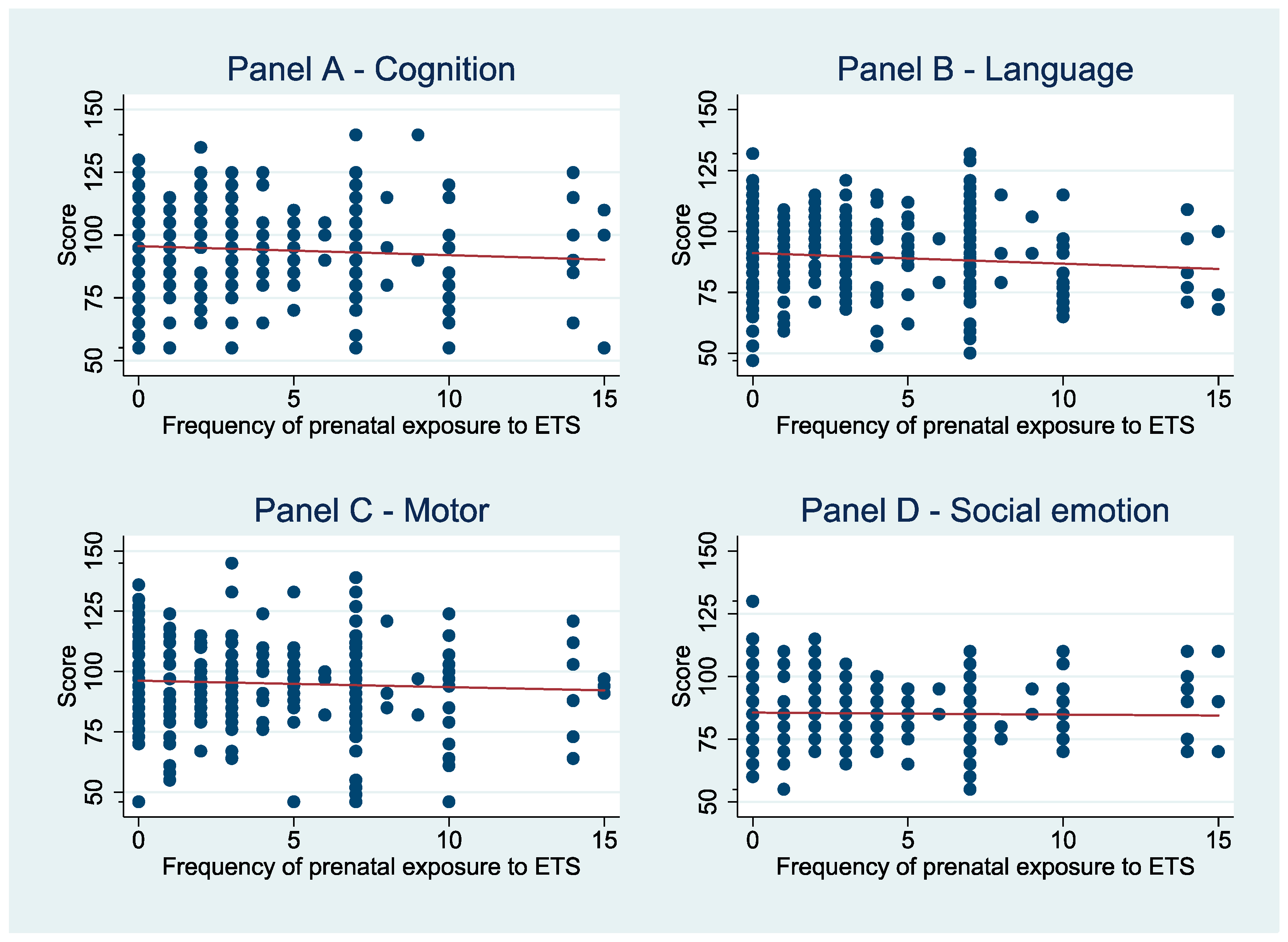
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A



{kind=link}
{kind=link}
{kind=link}
| Variables | VIF Values |
|---|---|
| ETS/ Packs of cigarettes per week | 1.06 |
| Child’s gender (male = 1) | 1.10 |
| Age of child in months | 1.57 |
| Low birth weight (yes = 1) | 1.08 |
| Mother’s age in years | 1.15 |
| Education attainment of the mother | 1.09 |
| If mother is the primary caregiver of the child | 1.19 |
| Family income in the last year | 1.12 |
| Mean VIF | 1.50 |
| Independent Variables | Model 1 | Model 2 | ||
|---|---|---|---|---|
| Coefficient (95% CI) | p-Value | Coefficient (95% CI) | p-Value | |
| Panel A: Cognition score | ||||
| Prenatal exposure to ETS (Yes = 1; No = 0) | −2.75 (−5.40, −0.11) | 0.04 | −3.41 (−6.39, −0.42) | 0.03 |
| Child characteristics | N | Y | ||
| Mother characteristics | N | Y | ||
| Household characteristics | N | Y | ||
| Constant | Y | Y | ||
| Frequency of prenatal exposure to ETS | −0.33 (−0.80, 0.14) | 0.17 | 0.33 (−0.76, 0.11) | 0.14 |
| Child characteristics | N | Y | ||
| Mother characteristics | N | Y | ||
| Household characteristics | N | Y | ||
| Constant | Y | Y | ||
| Panel B: Language score | ||||
| Prenatal exposure to ETS (Yes = 1; No = 0) | −2.62 (−5.36, 0.13) | 0.06 | −3.01 (−5.93, −0.09) | 0.04 |
| Child characteristics | N | Y | ||
| Mother characteristics | N | Y | ||
| Household characteristics | N | Y | ||
| Constant | Y | Y | ||
| Frequency of prenatal exposure to ETS | −0.45 (−0.82, −0.08) | 0.02 | −0.48 (−0.87, −0.09) | 0.02 |
| Child characteristics | N | Y | ||
| Mother characteristics | N | Y | ||
| Household characteristics | N | Y | ||
| Constant | Y | Y | ||
| Panel C: Motor score | ||||
| Prenatal exposure to ETS (Yes = 1; No = 0) | −2.78 (−5.74, 0.71) | 0.06 | −2.52 (−5.43, 0.38) | 0.09 |
| Child characteristics | N | Y | ||
| Mother characteristics | N | Y | ||
| Household characteristics | N | Y | ||
| Constant | Y | Y | ||
| Frequency of prenatal exposure to ETS | −0.27 (−0.71, 0.17) | 0.22 | −0.31 (−0.70, 0.08) | 0.12 |
| Child characteristics | N | Y | ||
| Mother characteristics | N | Y | ||
| Household characteristics | N | Y | ||
| Constant | Y | Y | ||
| Panel D: Social emotion score | ||||
| Prenatal exposure to ETS (Yes = 1; No = 0) | −0.75 (−3.02, 1.52) | 0.51 | −0.88 (−3.29, 1.53) | 0.46 |
| Child characteristics | N | Y | ||
| Mother characteristics | N | Y | ||
| Household characteristics | N | Y | ||
| Constant | Y | Y | ||
| Frequency of prenatal exposure to ETS | 0.002 (−0.32, 0.33) | 0.99 | −0.002 (−0.36, 0.36) | 0.99 |
| Child characteristics | N | Y | ||
| Mother characteristics | N | Y | ||
| Household characteristics | N | Y | ||
| Constant | Y | Y | ||
| Independent Variables | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|
| Coefficient (95% CI) | p-Value | Coefficient (95% CI) | p-Value | Coefficient (95% CI) | p-Value | |
| Panel A: Cognition score | ||||||
| Prenatal exposure to ETS (Yes = 1; No = 0) | −3.41 (−6.32, −0.50) | 0.02 | −2.71 (−5.47, 0.04) | 0.05 | −3.00 (−5.82, -0.18) | 0.04 |
| Child characteristics | Y | N | N | |||
| Mother characteristics | N | Y | N | |||
| Household characteristics | N | N | Y | |||
| Constant | Y | Y | Y | |||
| Frequency of prenatal exposure to ETS | −0.33 (−0.78, 0.12) | 0.14 | −0.32 (−0.78, 0.15) | 0.17 | −0.33 (−0.79, 0.12) | 0.14 |
| Child characteristics | Y | N | N | |||
| Mother characteristics | N | Y | N | |||
| Household characteristics | N | N | Y | |||
| Constant | Y | Y | Y | |||
| Panel B: Language score | ||||||
| Prenatal exposure to ETS (Yes = 1; No = 0) | −2.97 (−5.82, −0.12) | 0.04 | −2.61 (−5.42, 0.12) | 0.07 | −2.89 (−5.74, −0.04) | 0.05 |
| Child characteristics | Y | N | N | |||
| Mother characteristics | N | Y | N | |||
| Household characteristics | N | N | Y | |||
| Constant | Y | Y | Y | |||
| Frequency of prenatal exposure to ETS | −0.48 (−0.86, −0.11) | 0.01 | −0.45 (−0.83, −0.07) | 0.02 | −0.46 (−0.83, −0.09) | 0.02 |
| Child characteristics | Y | N | N | |||
| Mother characteristics | N | Y | N | |||
| Household characteristics | N | N | Y | |||
| Constant | Y | Y | Y | |||
| Panel C: Motor score | ||||||
| Prenatal exposure to ETS (Yes = 1; No = 0) | −0.32 (−0.70, 0.08) | 0.11 | −0.26 (−0.71, 0.18) | 0.24 | −0.28 (−0.72, 0.16) | 0.20 |
| Child characteristics | Y | N | N | |||
| Mother characteristics | N | Y | N | |||
| Household characteristics | N | N | Y | |||
| Constant | Y | Y | Y | |||
| Frequency of prenatal exposure to ETS | −0.32 (−0.70, 0.08) | 0.11 | −0.26 (−0.71, 0.18) | 0.24 | −0.28 (−0.72, 0.16) | 0.20 |
| Child characteristics | Y | N | N | |||
| Mother characteristics | N | Y | N | |||
| Household characteristics | N | N | Y | |||
| Constant | Y | Y | Y | |||
| Panel D: Social emotion score | ||||||
| Prenatal exposure to ETS (Yes = 1; No = 0) | −0.87 (−3.28, 1.54) | 0.47 | −0.74 (−3.04, 1.56) | 0.52 | −0.91 (−3.18, 1.36) | 0.43 |
| Child characteristics | Y | N | N | |||
| Mother characteristics | N | Y | N | |||
| Household characteristics | N | N | Y | |||
| Constant | Y | Y | Y | |||
| Frequency of prenatal exposure to ETS | −0.0001 (−0.36, 0.36) | 1.00 | −0.006 (−0.31, 0.32) | 0.97 | −0.13 (−0.34, 0.32) | 0.94 |
| Child characteristics | Y | N | N | |||
| Mother characteristics | N | Y | N | |||
| Household characteristics | N | N | Y | |||
| Constant | Y | Y | Y | |||
References
- Reitsma, M.; Fullman, N.; Ng, M.; Salama, J. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990–2015: A systematic analysis from the Global Burden of Disease Study 2015. Lancet 2017, 389, 1885–1906. [Google Scholar] [CrossRef]
- Öberg, M.; Jaakkola, M.S.; Woodward, A.; Peruga, A.; Prüss-Ustün, A. Worldwide burden of disease from exposure to second-hand smoke: A retrospective analysis of data from 192 countries. Lancet 2011, 377, 139–146. [Google Scholar] [CrossRef]
- Global Adults Tobacco Survey (GATS) China 2010 Country Report. Available online: http://www.who.int/tobacco/surveillance/survey/gats/en_gats_china_report.pdf (accessed on 23 April 2018).
- Li, Q.; Jason, H.; Yang, G. Prevalence of smoking in China in 2010. N. Engl. J. Med. 2011, 364, 2469–2470. [Google Scholar] [CrossRef] [PubMed]
- Davis, E.P.; Sandman, C.A. The Timing of Prenatal Exposure to Maternal Cortisol and Psychosocial Stress Is Associated With Human Infant Cognitive Development. Child Dev. 2010, 81, 131–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wachs, T.D.; Georgieff, M.; Cusick, S.; Mcewen, B.S. Issues in the timing of integrated early interventions: Contributions from nutrition, neuroscience, and psychological research. Ann. N. Y. Acad. Sci. 2014, 1308, 89–106. [Google Scholar] [CrossRef]
- Kolb, B.; Whishaw, I.Q. An Introduction to Brain and Behavior; Worth Publishers: New York, NY, USA, 2001; ISBN 0716751690. [Google Scholar]
- Walker, S.P.; Wachs, T.D.; Sally, G.M.; Black, M.M.; Nelson, C.A.; Huffman, S.L.; Helen, B.H.; Chang, S.M.; Hamadani, J.D.; Betsy, L. Inequality in early childhood: Risk and protective factors for early child development. Lancet 2011, 378, 1325–1338. [Google Scholar] [CrossRef]
- Jedrychowski, W.; Perera, F.P.; Jankowski, J.; Mrozek-Budzyn, D.; Mroz, E.; Flak, E.; Edwards, S.; Skarupa, A.; Lisowska-Miszczyk, I. Very Low Prenatal Exposure to Lead and Mental Development of Children in Infancy and Early Childhood. Neuroepidemiology 2009, 32, 270–278. [Google Scholar] [CrossRef] [Green Version]
- Lee, B.E.; Hong, Y.C.; Park, H.; Ha, M.; Kim, J.H.; Chang, N.; Roh, Y.M.; Kim, B.N.; Kim, Y.; Oh, S.Y. Secondhand smoke exposure during pregnancy and infantile neurodevelopment. Environ. Res. 2011, 111, 539–544. [Google Scholar] [CrossRef]
- Herrmann, M.; King, K.; Weitzman, M. Prenatal tobacco smoke and postnatal secondhand smoke exposure and child neurodevelopment. Curr. Opin. Pediatr. 2008, 20, 184–190. [Google Scholar] [CrossRef]
- Perera, F.P.; Rauh, V.; Whyatt, R.M.; Tang, D.; Tsai, W.Y.; Bernert, J.T.; Tu, Y.H.; Andrews, H.; Barr, D.B.; Camann, D.E. A Summary of Recent Findings on Birth Outcomes and Developmental Effects of Prenatal ETS, PAH, and Pesticide Exposures. Neurotoxicology 2005, 26, 573–587. [Google Scholar] [CrossRef]
- Weitzman, M.; Byrd, R.S.; Aligne, C.A.; Moss, M. The effects of tobacco exposure on children’s behavioral and cognitive functioning: Implications for clinical and public health policy and future research. Neurotoxicol. Teratol. 2002, 24, 397–406. [Google Scholar] [CrossRef]
- Eskenazi, B.; Castorina, R. Association of Prenatal Maternal or Postnatal Child Environmental Tobacco Smoke Exposure and Neurodevelopmental and Behavioral Problems in Children. Environ. Health Perspect. 1999, 107, 991–1000. [Google Scholar] [CrossRef] [PubMed]
- Jordi, J.; Núria, R.F.; Maties, T.; Maria, F.; Raquel, G.E.; Jordi, S. Maternal smoking habits and cognitive development of children at age 4 years in a population-based birth cohort. Int. J. Epidemiol. 2007, 36, 825. [Google Scholar] [CrossRef]
- Key, A.P.; Ferguson, M.; Molfese, D.L.; Peach, K.; Lehman, C.; Molfese, V.J. Smoking during pregnancy affects speech-processing ability in newborn infants. Environ. Health Perspect. 2007, 115, 623–629. [Google Scholar] [CrossRef] [PubMed]
- Ott, A.; Andersen, K.; Dewey, M.E.; Letenneur, L.; Brayne, C.; Copeland, J.R.M.; Dartigues, J.F.; Kragh-Sorensen, P.; Lobo, A.; Martinez-Lage, J.M. Effect of smoking on global cognitive function in nondemented elderly. Neurology 2004, 62, 920–924. [Google Scholar] [CrossRef]
- Anstey, K.J.; von Sanden, C.; Salim, A.; O’kearney, R. Smoking as a risk factor for dementia and cognitive decline: A meta-analysis of prospective studies. Am. J. Epidemiol. 2007, 166, 367–378. [Google Scholar] [CrossRef]
- Slykerman, R.F.; Thompson, J.M.D.; Clark, P.M.; Becroft, D.M.O.; Elizabeth, R.; Pryor, J.E.; Wild, C.J.; Mitchell, E.A. Determinants of developmental delay in infants aged 12 months. Paediatr. Périnat. Epidemiol. 2010, 21, 121–128. [Google Scholar] [CrossRef]
- Courtney, R. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General, 2014. Drug Alcohol Rev. 2015, 34, 694–695. [Google Scholar] [CrossRef]
- Chen, R.; Angela, C.; Linda, L.; Kaarin, J.A. Is exposure to secondhand smoke associated with cognitive parameters of children and adolescents?—A systematic literature review. Ann. Epidemiol. 2013, 23, 652–661. [Google Scholar] [CrossRef]
- Cornelius, M.D.; Ryan, C.M.; Day, N.L.; Goldschmidt, L.; Willford, J.A. Prenatal tobacco effects on neuropsychological outcomes among preadolescents. J. Dev. Behav. Pediatr. 2001, 22, 217–225. [Google Scholar] [CrossRef]
- Cornelius, M.D.; Genna, N.M.D.; Leech, S.L.; Willford, J.A.; Goldschmidt, L.; Day, N.L. Effects of prenatal cigarette smoke exposure on neurobehavioral outcomes in 10-year-old children of adolescent mothers. Neurotoxicol. Teratol. 2011, 33, 137–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, R.P.; Dombrowski, S.C.; Mullis, C.; Wisenbaker, J.; Huttunen, M.O. Smoking during pregnancy: Association with childhood temperament, behavior, and academic performance. J. Pediatr. Psychol. 2006, 31, 490–500. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.-J.; Liao, H.-F.; Wu, K.-Y.; Hsieh, W.-S.; Su, Y.-N.; Jeng, S.-F.; Yu, S.-N.; Chen, P.-C. CYP1A1 Ile462Val and GSTT1 modify the effect of cord blood cotinine on neurodevelopment at 2 years of age. Neurotoxicology 2008, 29, 839–845. [Google Scholar] [CrossRef] [PubMed]
- Polanska, K.; Hanke, W.; Sobala, W.; Trzcinka-Ochocka, M.; Ligocka, D.; Brzeznicki, S.; Strugala-Stawik, H.; Magnus, P. Developmental Effects of Exposures to Environmental Factors: The Polish Mother and Child Cohort Study. BioMed Res. Int. 2013, 2013, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Martínez, C.; Moreso, N.V.; Serra, B.R.; Val, V.A.; Macías, J.E.; Sans, J.C. Effects of Prenatal Nicotine Exposure on Infant Language Development: A Cohort Follow Up Study. Matern. Child Health J. 2017, 21, 734–744. [Google Scholar] [CrossRef] [PubMed]
- Jedrychowski, W.; Perera, F.P.; Jankowski, J.; Maugeri, U.; Mrozek-Budzyn, D.; Mroz, E.; Flak, E.; Skarupa, A.; Edwards, S.; Lisowska-Miszczyk, I. Early wheezing phenotypes and cognitive development of 3-year-olds. Community-recruited birth cohort study. Pediatr. Allergy Immunol. 2010, 21, 550–556. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Wu, T.; Geng, X.; Wu, C.; Cai, Z. Effect of passive smoking during pregnancy on fetal growth and neurodevelopment of infants. Chin. J. Fam. Plan. 2015, 23, 337–338. [Google Scholar]
- Gilman, S.E.; Hannah, G.; Buka, S.L. Maternal smoking during pregnancy and children’s cognitive and physical development: A causal risk factor? Am. J. Epidemiol. 2008, 168, 522–531. [Google Scholar] [CrossRef]
- Roza, S.J.; Verhulst, F.C.; Jaddoe, V.W.V.; Steegers, E.A.P.; Mackenbach, J.P.; Hofman, A.; Tiemeier, H. Maternal smoking during pregnancy and child behaviour problems: The Generation R Study. Int. J. Epidemiol. 2009, 38, 680–689. [Google Scholar] [CrossRef]
- Huijbregts, S.C.J.; Séguin, J.R.; Zelazo, P.D.; Parent, S.; Japel, C.; Tremblay, R.E. Interrelations between maternal smoking during pregnancy, birth weight and sociodemographic factors in the prediction of early cognitive abilities. Infant Child Dev. 2010, 15, 593–607. [Google Scholar] [CrossRef]
- Hu, A.; Wang, F.; Hao, M.; Li, Y. The influence of passive smoking during pregnancy on the ability of cognitive and behavior of attention-deficit hyperactivity disorder children. Chin. J. Prim. Med. Pharm. 2010, 17, 3. [Google Scholar] [CrossRef]
- Xu, Y.; Xu, J.; Yang, Q. A cohort study on the relationship between passive smoking in early pregnancy and adverse pregnancy outcomes. Matern. Child Health Care China 2006, 21, 3. [Google Scholar]
- Wang, C.; Wang, S.; Dong, X. The Harm of Passive Smoking in Pregnant Women to Pregnancy Outcome and Infant Health. Chin. J. Dis. Control. Prev. 2010, 14, 1142–1145. [Google Scholar]
- Guizhou Statistical Bureau. Guizhou Statistical Yearbook; China Statistics Press: Beijing, China, 2017; ISBN 978-7-5037-8258-9.
- Moore, T.; Johnson, S.; Haider, S.; Hennessy, E.; Marlow, N. Relationship between Test Scores Using the Second and Third Editions of the Bayley Scales in Extremely Preterm Children. J. Pediatr. 2012, 160, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Bayley, N. Bayley Scales of Infant and Toddler Development: Bayley-III; Harcourt Assessment, Psych. Corporation: San Antonio, TX, USA, 2006. [Google Scholar] [CrossRef]
- Weiss, L.G.; Oakland, T.; Aylward, G.P. Bayley-III Clinical Use and Interpretation; Academic Press: San Diego, CA, USA, 2008; ISBN 9780123741776. [Google Scholar]
- Luo, R.; Yue, A.; Zhou, H.; Shi, Y.; Zhang, L.; Martorell, R.; Medina, A.; Rozelle, S.; Sylvia, S. The effect of a micronutrient powder home fortification program on anemia and cognitive outcomes among young children in rural China: A cluster randomized trial. BMC Public Health 2017, 17, 738. [Google Scholar] [CrossRef] [PubMed]
- Altonji, J.G.; Elder, T.E.; Taber, C.R. Selection on Observed and Unobserved Variables: Assessing the Effectiveness of Catholic Schools. J. Political. Econ. 2005, 113, 151–184. [Google Scholar] [CrossRef] [Green Version]
- Hughes, M.M.; Black, R.E.; Katz, J. 2500-g Low Birth Weight Cutoff: History and Implications for Future Research and Policy. Matern. Child Health J. 2017, 21, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Ramsey, J.B. Tests for Specification Errors in Classical Linear Least-Squares Regression Analysis. J. R. Stat. Soc. 1969, 31, 350–371. [Google Scholar] [CrossRef]
- Jiang, Y.; Eltonmarshall, T.; Fong, G.T.; Li, Q. Quitting smoking in China: Findings from the ITC China Survey. Tob. Control. 2010, 19, 12–17. [Google Scholar] [CrossRef]
- Ministry of Health, PRC. China Report on the Health Hazards of Smoking Executive Summary; People’s Medical Publishing House: Beijing, China, 2012; ISBN 9787117159517.
- Yue, A.; Yaojiang, S.; Renfu, L.; Jamie, C.; James, G.; Jimmy, Z.; Alexis, M.; Sarah, K.; Scott, R. China’s Invisible Crisis: Cognitive Delays among Rural Toddlers and the Absence of Modern Parenting. China J. 2017, 78, 50–80. [Google Scholar] [CrossRef]
- Christensen, L.H.; Høyer, B.B.; Pedersen, H.S.; Zinchuk, A.; Jönsson, B.A.; Lindh, C.; Dürr, D.W.; Bonde, J.P.; Toft, G. Prenatal smoking exposure, measured as maternal serum cotinine, and children’s motor developmental milestones and motor function: A follow-up study. Neurotoxicology 2016, 53, 236–245. [Google Scholar] [CrossRef] [PubMed]
- Polańska, K.; Jurewicz, J.; Hanke, W. Smoking and alcohol drinking during pregnancy as the risk factors for poor child neurodevelopment—A review of epidemiological studies. Int. J. Occup. Med. Environ. Health 2015, 28, 419. [Google Scholar] [CrossRef] [PubMed]
- Bakker, H.; Jaddoe, V.W. Cardiovascular and metabolic influences of fetal smoke exposure. Eur. J. Epidemiol. 2011, 26, 763–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinskje, T.; Thomas, S.; Ewa, F.; Jan, V.B.; Piet, W.; Antoon, O. Hazardous compounds in tobacco smoke. Int. J. Environ. Res. Public Health 2011, 8, 613–628. [Google Scholar] [CrossRef]
- Scherer, G. Carboxyhemoglobin and thiocyanate as biomarkers of exposure to carbon monoxide and hydrogen cyanide in tobacco smoke. Exp. Toxicol. Pathol. 2006, 58, 101–124. [Google Scholar] [CrossRef] [PubMed]
- Franco, P.; Chabanski, S.; Szliwowski, H.; Dramaix, M.; Kahn, A. Influence of maternal smoking on autonomic nervous system in healthy infants. Pediatr. Res. 2000, 47, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Sansone, G.; Fong, G.T.; Hall, P.A.; Guignard, R.; Beck, F.; Mons, U.; Pötschke-Langer, M.; Yong, H.; Thompson, M.; Omar, M.; et al. Time perspective as a predictor of smoking status: Findings from the;International Tobacco Control (ITC) Surveys in Scotland, France, Germany, China, and Malaysia. BMC Public Health 2013, 13, 346. [Google Scholar] [CrossRef] [PubMed]
- Hu, T.; Zhang, X.; Zheng, R. China has raised the tax on cigarettes: What’s next? Tob. Control. 2015, 25, 609. [Google Scholar] [CrossRef]
- Faber, T.; Kumar, A.; Mackenbach, J.; Millett, C.; Basu, S.; Sheikh, A.; Been, J. Effect of tobacco control policies on perinatal and child health: A systematic review and meta-analysis. Lancet Public Health 2017, 2, e420–e437. [Google Scholar] [CrossRef]

| Variables | Prenatal Exposure to ETS? | p-Value | ||
|---|---|---|---|---|
| No (n = 176) | Yes (n = 270) | |||
| Sex | Boy | 105 (59.7) | 152 (56.3) | 0.48 |
| Girl | 71 (40.3) | 118 (43.7) | ||
| Age of child in month (Mean ± SD) | 14.8 ± 5.6 | 14.5 ± 5.4 | 0.59 | |
| Low birth weight | No | 160 (91.9) | 254 (94.1) | 0.39 |
| Yes | 14 (8.1) | 16 (5.9) | ||
| Age of mother in year (Mean ± SD) | 24.7 ± 5.6 | 24.5 ± 4.9 | 0.60 | |
| Education of mother | ≤9 years | 151 (85.8) | 242 (89.6) | 0.22 |
| >9 years | 25 (14.2) | 28 (10.4) | ||
| Is mother primary caregiver | No | 90 (51.7) | 132 (48.9) | 0.56 |
| Yes | 84 (48.3) | 138 (51.1) | ||
| Family income in the last year (RMB) | ≤25,000 Yuan | 71 (40.6) | 107 (39.6) | 0.84 |
| >25,000 Yuan | 104 (59.4) | 163 (60.4) | ||
| Variables | Cognition Score | Language Score | Motor Score | Social Emotional Score | |||||
|---|---|---|---|---|---|---|---|---|---|
| (Mean ± SD) | p-Value | (Mean ± SD) | p-Value | (Mean ± SD) | p-Value | (Mean ± SD) | p-Value | ||
| Sex | Boy | 95.6 ± 16.5 | 0.08 | 88.9 ± 13.7 | 0.17 | 96.2 ± 15.4 | 0.19 | 85.3 ± 12.3 | 0.95 |
| Girl | 92.9 ± 16.0 | 90.7 ± 14.0 | 94.2 ± 16.2 | 85.4 ± 11.4 | |||||
| Age of child | ≤15 months | 97.3 ± 16.4 | <0.01 | 91.2 ± 14.5 | 0.02 | 90.4 ± 16.0 | <0.01 | 84.4 ± 12.2 | 0.10 |
| >15 months | 91.5 ± 15.7 | 88.2 ± 12.0 | 100.5 ± 13.8 | 86.3 ± 11.5 | |||||
| Low birth weight | No | 94.9 ± 16.0 | 0.05 | 90.0 ± 13.5 | 0.13 | 95.7 ± 15.5 | 0.14 | 85.7 ± 11.7 | 0.07 |
| Yes | 89.0 ± 18.0 | 86.1 ± 16.5 | 91.3 ± 18.6 | 81.7 ± 13.7 | |||||
| Age of mother | ≤25 years | 95.2 ± 15.7 | 0.23 | 89.9 ± 13.4 | 0.65 | 95.4 ± 15.8 | 0.90 | 85.7 ± 11.9 | 0.33 |
| >25 years | 93.2 ± 17.3 | 89.3 ± 14.6 | 95.2 ± 15.8 | 84.5 ± 11.9 | |||||
| Education of mother | ≤9 years | 93.9 ± 16.5 | 0.04 | 89.4 ± 13.7 | 0.23 | 95.1 ± 15.9 | 0.33 | 85.1 ± 12.1 | 0.19 |
| >9 years | 98.8 ± 14.6 | 91.8 ± 14.5 | 97.3 ± 14.7 | 87.4 ± 10.4 | |||||
| Is mother primary caregiver | No | 92.9 ± 15.4 | 0.04 | 87.7 ± 12.5 | <0.01 | 96.1 ± 15.2 | 0.38 | 86.0 ± 12.4 | 0.32 |
| Yes | 96.1 ± 16.9 | 91.9 ± 14.5 | 94.8 ± 16.3 | 84.8 ± 11.3 | |||||
| Family income in the last year (RMB) | ≤ 25,000 Yuan | 91.7 ± 14.7 | <0.01 | 88.4 ± 13.6 | 0.11 | 93.9 ± 15.8 | 0.11 | 85.6 ± 12.4 | 0.70 |
| >25,000 Yuan | 96.3 ± 15.8 | 90.5 ± 13.9 | 96.3 ± 15.7 | 85.2 ± 11.6 | |||||
| Dependent Variables | Unadjusted Analysis (ETS = 1) a | Adjusted Analysis (ETS = 1) a,b | ||
|---|---|---|---|---|
| Coefficient (95% CI) | p-Value | Coefficient (95% CI) | p-Value | |
| Cognition score | −2.75 (−5.40, −0.11) | 0.04 | −3.41 (−6.39, −0.42) | 0.03 |
| Language score | −2.62 (−5.36, 0.13) | 0.06 | −3.01 (−5.93, −0.09) | 0.04 |
| Motor score | −2.78 (−5.74, 0.71) | 0.06 | −2.52 (−5.43, 0.38) | 0.09 |
| Social emotion score | −0.75 (−3.02, 1.52) | 0.51 | −0.88 (−3.29, 1.53) | 0.46 |
| Dependent Variables | Unadjusted Analysis (Packs of Cigarettes per Week) a | Adjusted Analysis (Packs of Cigarettes per Week) a,b | ||
|---|---|---|---|---|
| Coefficient (95% CI) | p-Value | Coefficient (95% CI) | p-Value | |
| Cognition score | −0.33 (−0.80, 0.14) | 0.17 | −0.33 (−0.76, 0.11) | 0.14 |
| Language score | −0.45 (−0.82, −0.08) | 0.02 | −0.48 (−0.87, −0.09) | 0.02 |
| Motor score | −0.27 (−0.71, 0.17) | 0.22 | −0.31 (−0.70, 0.08) | 0.12 |
| Social emotion score | 0.002 (−0.32, 0.33) | 0.99 | −0.002 (−0.36, 0.36) | 0.99 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
He, Y.; Luo, R.; Wang, T.; Gao, J.; Liu, C. Prenatal Exposure to Environmental Tobacco Smoke and Early Development of Children in Rural Guizhou Province, China. Int. J. Environ. Res. Public Health 2018, 15, 2866. https://doi.org/10.3390/ijerph15122866
He Y, Luo R, Wang T, Gao J, Liu C. Prenatal Exposure to Environmental Tobacco Smoke and Early Development of Children in Rural Guizhou Province, China. International Journal of Environmental Research and Public Health. 2018; 15(12):2866. https://doi.org/10.3390/ijerph15122866
Chicago/Turabian StyleHe, Yang, Renfu Luo, Tianyi Wang, Jingjing Gao, and Chengfang Liu. 2018. "Prenatal Exposure to Environmental Tobacco Smoke and Early Development of Children in Rural Guizhou Province, China" International Journal of Environmental Research and Public Health 15, no. 12: 2866. https://doi.org/10.3390/ijerph15122866