The Effects of Tai Chi on Heart Rate Variability in Older Chinese Individuals with Depression

 ,
,  and
and
Abstract
:1. Introduction
2. Methods
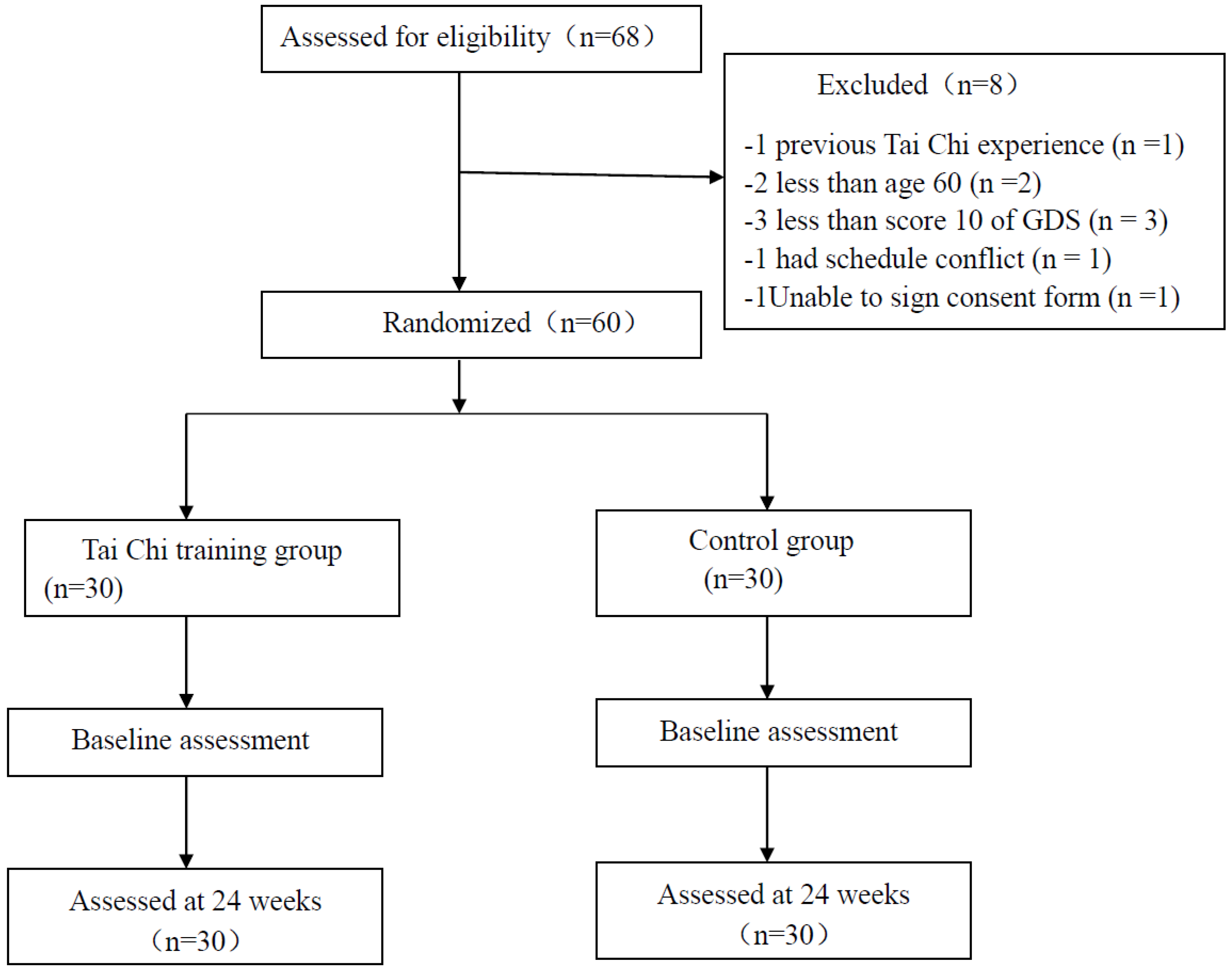
2.1. Study Participantsand Randomization
2.2. Tai Chi Intervention Program
2.3. Outcome Measures
2.3.1. Depressive Symptom Measured by the Geriatric Depression Scale
2.3.2. Both Time- and Frequency-Domains of Heart Rate Variability
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lebowitz, B.D.; Pearson, J.L.; Schneider, L.S.; Reynolds, C.F.; Alexopoulos, G.S.; Bruce, M.L. Diagnosis and treatment of depression in late life: Consensus statement update. JAMA 1997, 278, 1186–1190. [Google Scholar] [CrossRef] [PubMed]
- Baiyewu, O.; Smith-Gamble, V.; Lane, K.A.; Gureje, O.; Gao, S.; Ogunniyi, A.; Unverzagt, F.W.; Hall, K.S.; Hendrie, H.C. Prevalence estimates of depression in elderly community dwelling African Americans in Indianapolis and Yoruba in Ibadan, Nigeria. Int. Psychogeriatr. 2007, 19, 679–689. [Google Scholar] [CrossRef] [PubMed]
- Alexopoulos, S.G. Depression in the elderly. Lancet 2005, 365, 1961–1970. [Google Scholar] [CrossRef]
- Meats, P.; Timol, M.; Jolley, D. Prognosis of depression in the elderly. Br. J. Psychiatry 1991, 159, 659–663. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, A.J. Why do physicians have difficulty diagnosing depression in the elderly? Aging Health 2011, 7, 99–101. [Google Scholar] [CrossRef] [Green Version]
- Lyness, J.M.; Cox, C.; Curry, J.; Conwell, Y.; King, D.A.; Caine, E.D. Older age and the underreporting of depressive symptoms. J. Am. Geriatr. Soc. 1995, 43, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Kovess-Masfety, V.; Saragoussi, D.; Sevilla-Dedieu, C. What makes people decide who to turn to when faced with a mental health problem? Results from a French survey. BMC Public Health 2007, 7, 118. [Google Scholar] [CrossRef] [PubMed]
- Mickus, M.; Colenda, C.C.; Hogan, A.J. Knowledge of mental health benefits and preferences for type of mental health providers among the general public. Psychiatr. Serv. 2000, 51, 199–203. [Google Scholar] [CrossRef]
- Berry, J.M.; Storandt, M.; Coyne, A. Age and sex differences in somatic complaints associated with depression. J. Gerontol. 1984, 39, 465–467. [Google Scholar] [CrossRef]
- Kim, H.; Cheon, E.; Bai, D.; Lee, Y.; Koo, B. Stress and heart rate variability: A meta-analysis and review of Literature. Psychiatry Investig. 2018, 15, 235–245. [Google Scholar] [CrossRef]
- Jarczok, M.N.; Jarczok, M.; Mauss, D.; Koenig, J.; Li, J.; Herr, R.M.; Thayer, J.F. Autonomic nervous system activity and workplace stressors—A systematic review. Neurosci. Biobehav. Rev. 2013, 37, 1810–1823. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, J.A.; Quitana, D.S.; Abbott, M.; Kemp, A. Anxiety disorders are associated with reduced heart rate variability: A meta-analaysis. Front. Psychiatry 2014, 4, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sammi, R.; Chekroud, B.A.; Ralitza, G.P.; Amanda, B.; Zheutlin, L.; Martin, P.P.; Harlan, M.; Krumholz, P.; John, H.K.; Adam, M.C. Association between physical exercise and mental health in 1·2 million individuals in the USA between 2011 and 2015: A cross-sectional study. Lancet Psychiatry 2018, 5, 739–746. [Google Scholar] [CrossRef]
- Zou, L.; Han, J.; Tsang, W.; Yeung, A. Effects of Tai Chi on lower limb proprioception in adults aged over 55: A systematic review ad meta-analysis. Arch. Phys. Med. Rehabil. 2018, in press. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, C.; Chen, K.; Shu, Y.; Chen, X.; Luo, L.; Zhao, X. The Effect of Taichi Practice on Attenuating Bone Mineral Density Loss: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2017, 14, 1000. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, H.; Yu, D. Effect of a long-term modified Tai Chi-based intervention in attenuating bone mineral density in postmenopausal women in southeast China: Study protocol for a randomized controlled trial. Clin. Trials Degener. Dis. 2017, 2, 46–52. [Google Scholar] [CrossRef]
- Zou, L.; Wang, C.; Tian, Z.; Wang, H.; Shu, Y. Effect of Yang-Style Tai Chi on Gait Parameters and Musculoskeletal Flexibility in Healthy Chinese Older Women. Sports 2017, 5, 52. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, H.; Xiao, Z.; Fang, Q.; Zhang, M.; Li, T. Tai Chi for health benefits in patients with multiple sclerosis: A systematic review. PLoS ONE 2017, 12, 0170212. [Google Scholar] [CrossRef]
- Wang, C.; Bannuru, R.; Ramel, J.; Kupelnick, B.; Scott, T.; Schmid, C.H. Tai Chi on psychological well-being: Systematic review and meta-analysis. BMC Complement. Altern. Med. 2010, 10, 23. [Google Scholar] [CrossRef]
- Zou, L.; Yeung, A.; Zeng, N.; Wang, C.; Sun, L.; Thomas, G.; Wang, H. Effects of Mind-Body Exercises for Mood and Functional Capabilities in Post-Stroke Patients: An Analytical Review of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2018, 15, 721. [Google Scholar] [CrossRef]
- Zou, L.; Sasaki, J.; Zeng, N.; Wang, C.; Sun, L.A. Systematic Review with Meta-Analysis of Mindful Exercises on Rehabilitative Outcomes among post-stroke patients. Arch. Phys. Med. Rehabil. 2018, 9, 2355–2364. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Yeung, A.; Li, C.; Wei, G.; Chen, K.; Kinser, P.; Chan, J.; Ren, Z. Effects of meditative movements on major depressive disorder: A systematic Review and meta-analysis of randomized controlled trials. J. Clin. Med. 2018, 7, 195. [Google Scholar] [CrossRef] [PubMed]
- Yeung, A.; Chan, J.; Cheung, J.; Zou, L. Qigong and Tai-Chi. For mood regulation. Focus J. Lifelong Learn. Psychiatry 2017, 16, 40–47. [Google Scholar] [CrossRef]
- Zou, L.; Sasaki, J.E.; Wei, G.-X.; Huang, T.; Yeung, A.S.; Neto, O.B.; Chen, K.W.; Hui, S. Effects of Mind–Body Exercises (Tai Chi/Yoga) on Heart Rate Variability Parameters and Perceived Stress: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2018, 7, 404. [Google Scholar] [CrossRef] [PubMed]
- Yesavage, J.A.; Bink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [CrossRef]
- Koehler, M.; Rabinowitz, T.; Hirdes, J.; Stones, M.; Carpenter, G.I.; Fries, B.E.; Morris, J.N.; Jones, R.N. Measuring depression innursing home residents with the MDS and GDS: Anobservational psychometric study. BMC Geriatr. 2005, 5, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rottman, J.N.; Steinman, R.C.; Albrecht, P. Efficient estimation of the heart period power spectrum suitable for physiologic or pharmacologic studies. Am. J. Cardiol. 1990, 66, 1522–1524. [Google Scholar] [CrossRef]
- Park, M.; Unützer, J. Geriatric depression in primary care. Psychiatr. Clin. N. Am. 2011, 34, 469–487. [Google Scholar] [CrossRef]
- Bekhet, A.; Jaclene, Z. Mental Health of Elders in Retirement Communities: Is Loneliness a Key Factor? Arch. Psychiatr. Nurs. 2012, 32, 214–224. [Google Scholar] [CrossRef]
- Cornwell, B.; Edward, L.; Philip, S. The Social Connectedness of Older Adults: A National Profile. Am. Sociol. Rev. 2008, 73, 185–203. [Google Scholar] [CrossRef] [Green Version]
- Osborne, J.W. Psychological effects of the transition to retirement effects psychologiques de la transition vers laretaite. Can. J. Couns. Psychother. 2012, 46, 45–58. [Google Scholar] [CrossRef]
- Hui, S.S.; Xie, Y.J.; Woo, J.; Kwok, T.C. Effects of Tai Chi and Walking Exercises on Weight Loss, Metabolic Syndrome Parameters, and Bone Mineral Density: A Cluster Randomized Controlled Trial. Evid.-Based Complement. Altern. Med. 2015, 97, 6123–6185. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Wei, A.; Zou, L. Simplified Tai Chi Program Versus Traditional Tai Chi on the Functional Movement in Older Adults. Evid.-Based Complement. Altern. Med. 2016, 6, 212–239. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Zeng, N.; Huang, T.; Yeung, A.S.; Wei, G.X.; Liu, S.J.; Zhou, J.; Hu, R.; Hui, S.S. The Beneficial Effects of Mind-body Exercises for People with Mild Cognitive Impairment: A Systematic Review with Meta-Analysis. J. Clin. Med. 2018, in press. [Google Scholar]
- Mortimer, J.A.; Ding, D.; Borenstein, A.R.; DeCarli, C.; Guo, Q.H.; Wu, Y.G.; Zhao, Q.H.; Chu, S.G. Changes in brain volume and cognition in a randomized trial of exercise and social interaction in a community-based sample of non-demented Chinese elders. J. Alzheimer's Dis. 2012, 30, 757–766. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Yeung, A.; Quan, X. Mindfulness-based Baduanjin exercise for depression and anxiety in people with physical or mental illnesses: A Systematic Review and Meta-analysis of randomized controlled trials. Int. J. Environ. Res. Public Health 2018, 15, 321. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, C.; Yeung, A.; Liu, Y.; Pan, Z. A Review Study on the beneficial effects of Baduanjin. J. Altern. Complement. Med. 2018, 24, 324–335. [Google Scholar] [CrossRef] [PubMed]
- Yeung, A.; Slipp, L.E.; Jacquart, J.; Fava, M.; Denninger, J.W.; Benson, H.; Fricchione, G.L. The treatment of depressed Chinese Americans using qigong in a health care setting: A pilot study. Evid.-Based Complement. Altern. Med. 2013, 16, 8784. [Google Scholar] [CrossRef]
- Yeung, A.; Lepoutre, V.; Wayne, P.; Yeh, G.; Slipp, L.E.; Fava, M.; Denninger, J.W.; Benson, H.; Fricchione, G.L. Tai Chi treatment for depression in Chinese Americans: A pilot study. Am. J. Phys. Med. Rehabil. 2012, 91, 863–870. [Google Scholar] [CrossRef]
- Yeung, A.S.; Feng, R.; Kim, D.J.; Wayne, P.M.; Yeh, G.Y.; Baer, L.; Lee, O.E.; Denninger, J.W.; Benson, H.; Fricchione, G.L.; et al. A Pilot, Randomized Controlled Study of Tai Chi with Passive and Active Controls in the Treatment of Depressed Chinese Americans. J. Clin. Psychiatry 2017, 78, 522–528. [Google Scholar] [CrossRef]
- Chan, J.S.; Li, A.; Ng, S.M.; Ho, R.T.; Xu, A.; Yao, T.J.; Wang, X.M.; So, K.F.; Chan, C.L. Adiponectin Potentially Contributes to the Antidepressive Effects of Baduanjin Qigong Exercise in Women with Chronic Fatigue Syndrome-Like Illness. Cell Transplant. 2017, 26, 493–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeragani, V.K.; Sobolewski, K.; Kay, J.; Jampala, V.C.; Igel, G. Effect of age on long-term heart rate variability. Cardiovasc. Res. 1997, 35, 35–42. [Google Scholar] [CrossRef] [Green Version]
- Rottenberg, J. Cardiac vagal control in depression: Acritical analysis. Biol. Psychol. 2007, 74, 200–211. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, F.; McCraty, R.; Zerr, C.L. A healthy heart is not a metronome: An integrative review of the heart’s anatomy and heart rate variability. Front. Psychol. 2014, 5, 1040. [Google Scholar] [CrossRef] [PubMed]
- Bigger, J.T.; Albrecht, P.; Steinman, R.C.; Rolnitzky, L.M.; Fleiss, J.L.; Cohen, R.J. Comparison of time- and frequency domain-based measures of cardiac parasympathetic activity in Holter recordings after myocardial infarction. Am. J. Cardiol. 1989, 64, 536–538. [Google Scholar] [CrossRef]
- Telles, S.; ShaRma, S.; Gupta, R.; Bhardwaj, A.; Balkrishna, A. Heart rate variability in chronic low back pain patients randomized to yoga or standard care. BMC Complement. Altern. Med. 2016, 16, 279. [Google Scholar] [CrossRef] [PubMed]
- ChuDuc, H.; NgyyenPhan, K.; Nguyen, V. A review of heart rate variability and its applications. APCBEE Procedia 2017, 7, 80–85. [Google Scholar] [CrossRef]
- Zou, L.; Yeung, A.; Li, C.; Chiou, S.; Zeng, N.; Tzeng, H. Effects of mind-body movement on balance function in stroke survivors: A meta-analysis of randomized controlled trials. Int. J. Environ. Res. Public Health 2018, 15, 1292. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Tai Chi (n = 30) | Control (n = 30) | p |
|---|---|---|---|
| Female (%) | 53.3 | 53.3 | 1.00 * |
| Age (year) | 60.90 ± 4.28 | 61.72 ± 3.54 | 0.37 # |
| Body weight | 60.73 ± 2.14 | 57.59 ± 1.45 | 0.28 # |
| Height | 164.33 ± 2.09 | 165.28 ± 0.95 | 0.52 # |
| Parameters | Tai Chi | Control | ||
|---|---|---|---|---|
| Pre (t = 0) | Post (t = 24 Weeks) | Pre (t = 0) | Post (t = 24 Weeks) | |
| GDS | 11.97 ± 4.32 | 4.70 ± 3.90 * | 12.00 ± 3.08 | 12.40 ± 3.38 ▲ |
| Time Domains | ||||
| M-HRT (bpm) | 82.26 ± 9.85 | 74.81 ± 6.58 * | 81.85 ± 9.75 | 80.69 ± 7.57 ▲ |
| SDNN (ms) | 32.33 ± 15.21 | 37.24 ± 1.02 | 33.95 ± 12.27 | 31.73 ± 1.66 |
| RMSSD (ms) | 10.27 ± 6.67 | 15.97 ± 5.35 * | 10.69 ± 5.97 | 10.05 ± 7.07 ▲ |
| pNN50 (%) | 0.64 ± 1.55 | 1.04 ± 1.15 | 0.67 ± 1.36 | 0.54 ± 1.06 |
| Frequency Domains | ||||
| TP (ms²) | 149.22 ± 156.36 | 167.33 ± 48.71 | 150.76 ± 113.32 | 146.22 ± 152.40 |
| VLF (ms²) | 53.96 ± 43.13 | 49.11 ± 11.18 | 50.51 ± 33.56 | 55.56 ± 13.82 |
| LF (ms²) | 80.41 ± 25.52 | 70.48 ± 12.45 * | 77.57 ± 17.26 | 81.14 ± 42.39 |
| HF (ms²) | 22.21 ± 17.50 | 34.30 ± 12.45 * | 24.07 ± 8.19 | 21.92 ± 23.72 ▲ |
| LF/HF | 2.32 ± 1.21 | 1.90 ± 0.99 | 2.41 ± 1.01 | 2.58 ± 1.10 |
| LFnorm | 82.00 ± 9.38 | 75.48 ± 9.74 * | 79.71 ± 10.72 | 81.08 ± 11.20 ▲ |
| HFnorm | 19.56 ± 7.92 | 25.01 ± 6.51 * | 20.62 ± 8.93 | 18.91 ± 11.20 ▲ |
| HRV Measures | M-HRT (bpm) | SDNN (ms) | RMSSD (ms) | pNN50 (%) | TP (ms2) | VLF (ms2) | LF (ms2) | HF (ms2) | LF/HF | LFnorm (nu) | HFnorm (nu) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| r | 0.16 | −0.06 | −0.17 | −0.03 | 0.01 | 0.30 | 0.14 | −0.38 | 0.10 | 0.23 | −0.15 |
| p | 0.21 | 0.64 | 0.2 | 0.82 | 0.97 | 0.02 * | 0.28 | 0.00 ** | 0.44 | 0.08 | 0.27 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, J.; Xie, H.; Liu, M.; Wang, Z.; Zou, L.; Yeung, A.S.; Hui, S.S.-c.; Yang, Q. The Effects of Tai Chi on Heart Rate Variability in Older Chinese Individuals with Depression. Int. J. Environ. Res. Public Health 2018, 15, 2771. https://doi.org/10.3390/ijerph15122771
Liu J, Xie H, Liu M, Wang Z, Zou L, Yeung AS, Hui SS-c, Yang Q. The Effects of Tai Chi on Heart Rate Variability in Older Chinese Individuals with Depression. International Journal of Environmental Research and Public Health. 2018; 15(12):2771. https://doi.org/10.3390/ijerph15122771
Chicago/Turabian StyleLiu, Jing, Huihui Xie, Ming Liu, Zongbao Wang, Liye Zou, Albert S. Yeung, Stanley Sai-chuen Hui, and Qing Yang. 2018. "The Effects of Tai Chi on Heart Rate Variability in Older Chinese Individuals with Depression" International Journal of Environmental Research and Public Health 15, no. 12: 2771. https://doi.org/10.3390/ijerph15122771