
Health, Well-Being and Energy Poverty in Europe: A Comparative Study of 32 European Countries

Abstract
:1. Introduction
2. Background
3. Materials and Methods
3.1. Data
3.2. Variables
3.2.1. Predictor Variable
“There are some things that many people cannot afford, even if they would like them. For each of the following things on this card, can I just check whether your household can afford it if you want it? Keeping the home adequately warm”.[63]
3.2.2. Health and Well-Being Outcomes
I have felt cheerful and in good spirits;I have felt calm and relaxed;I have felt active and vigorous;I woke up feeling fresh and rested;My daily life has been filled with things that interest me.
3.2.3. Socio-Demographic Adjustment Variables
3.3. Statistical Analysis
4. Results
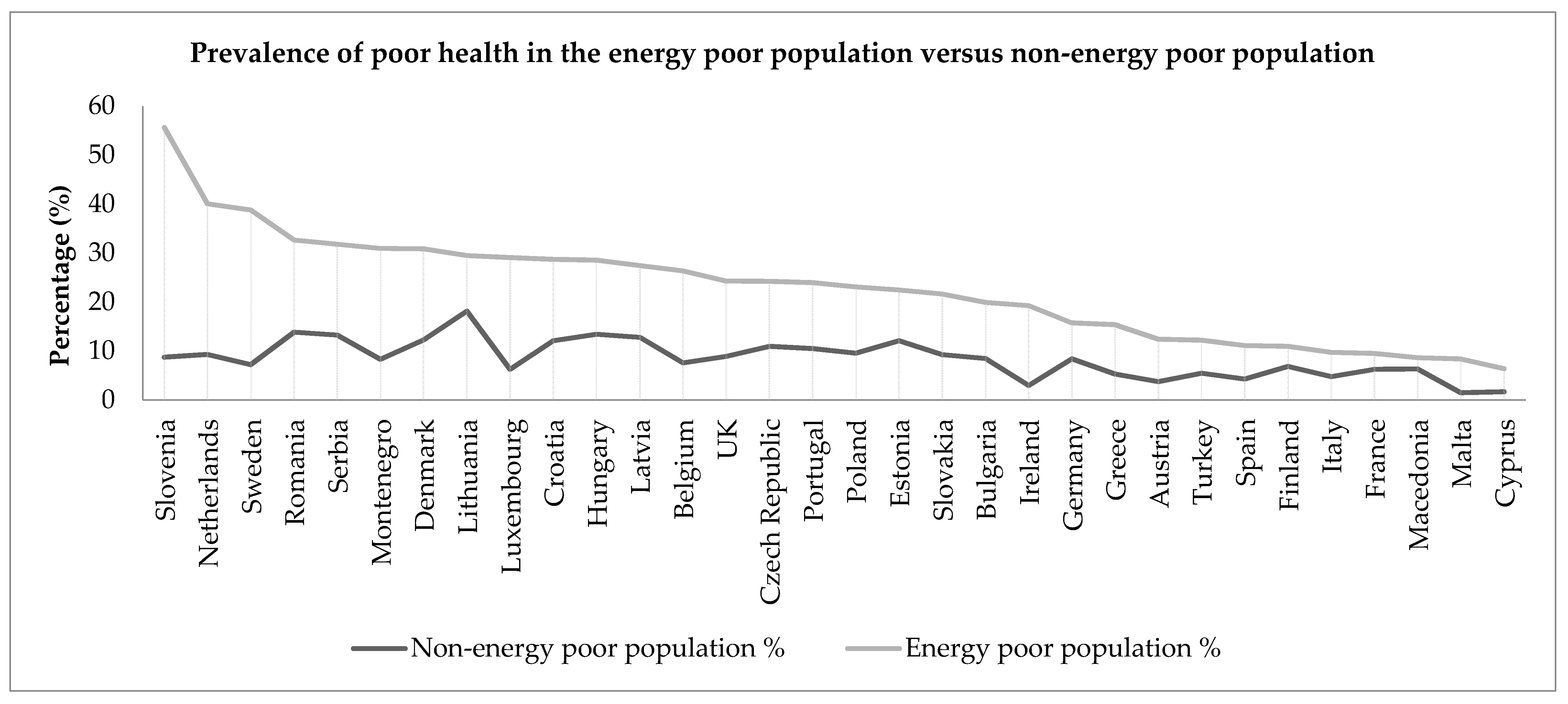
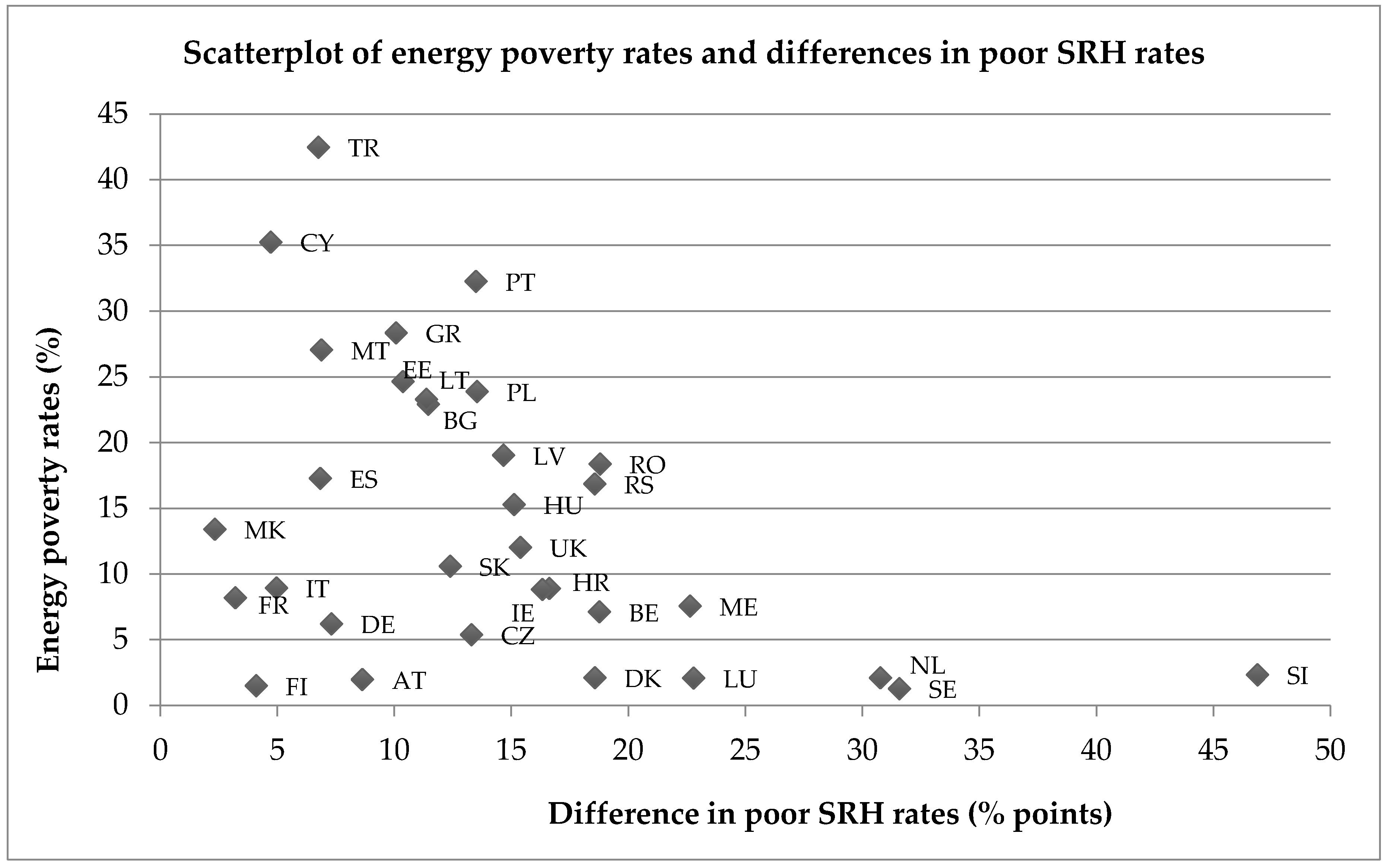
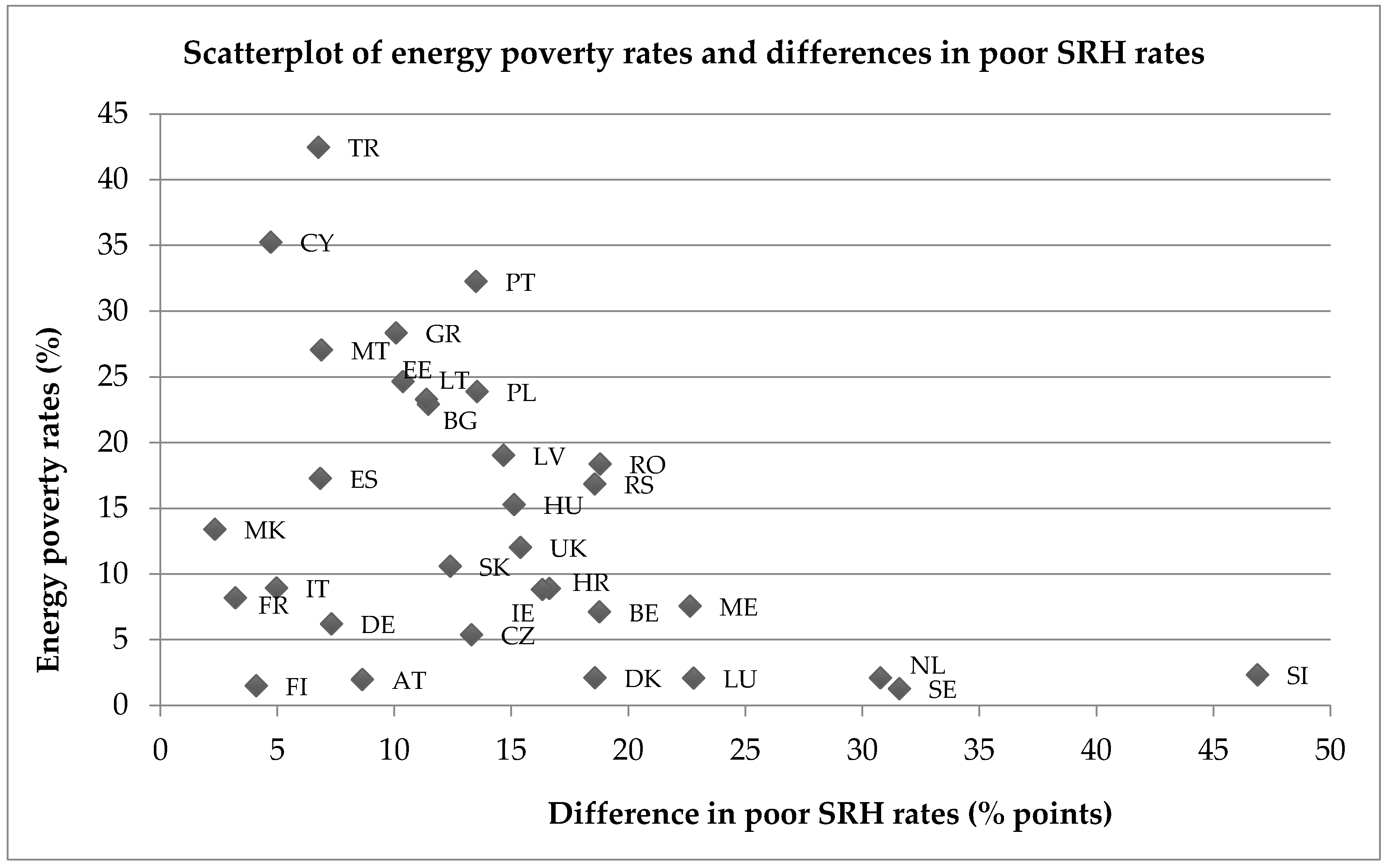
4.1. Poor SRH Status and Energy Poverty
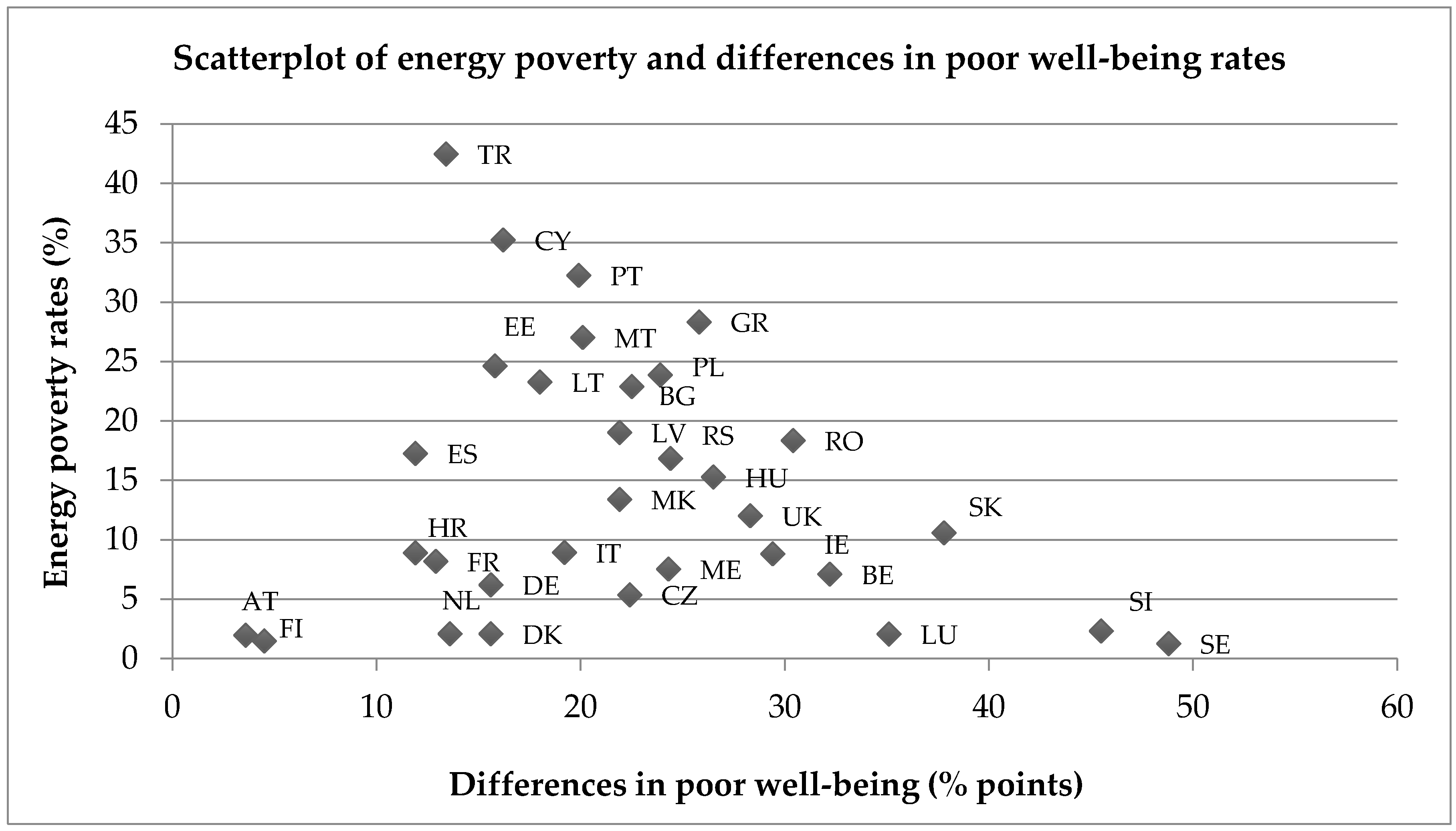
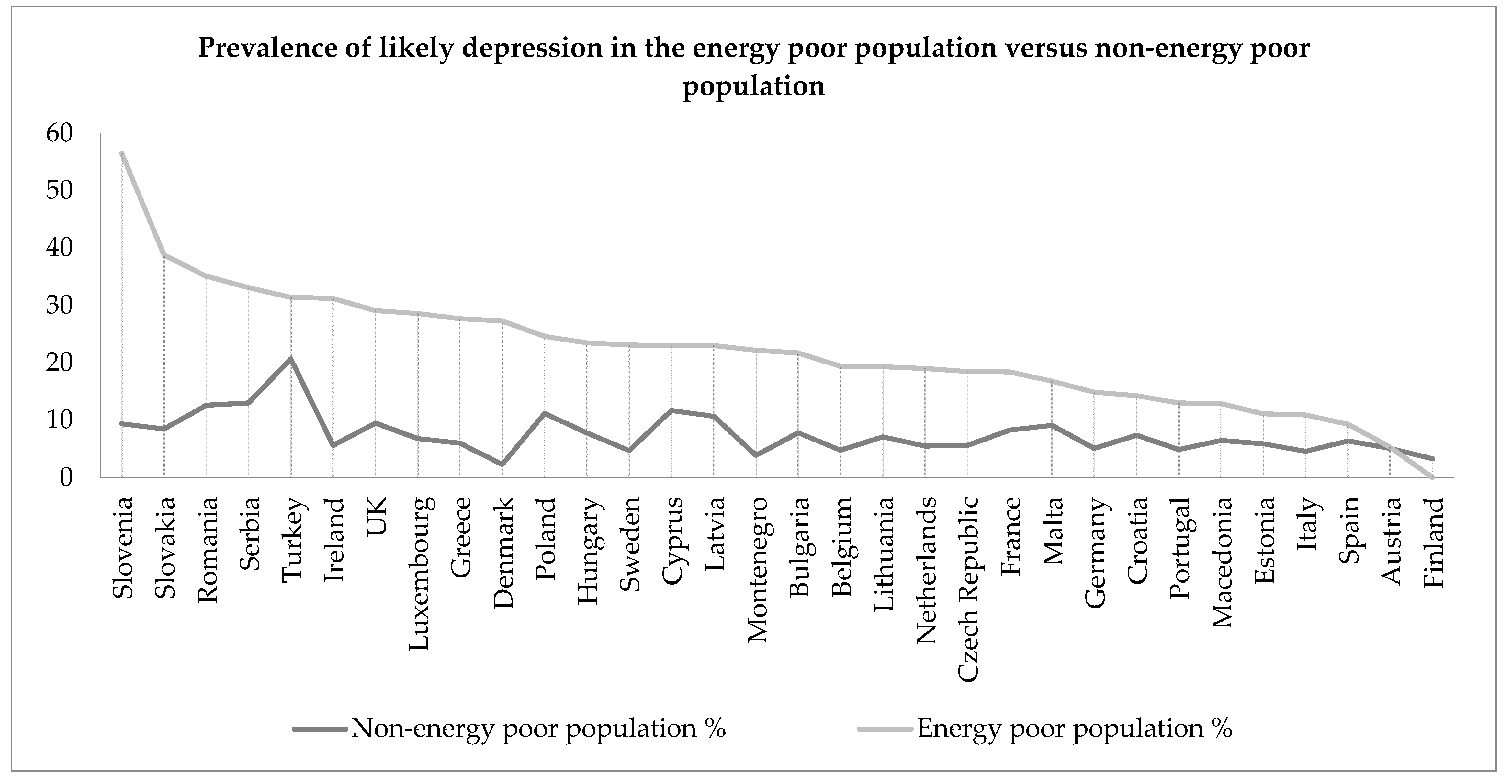
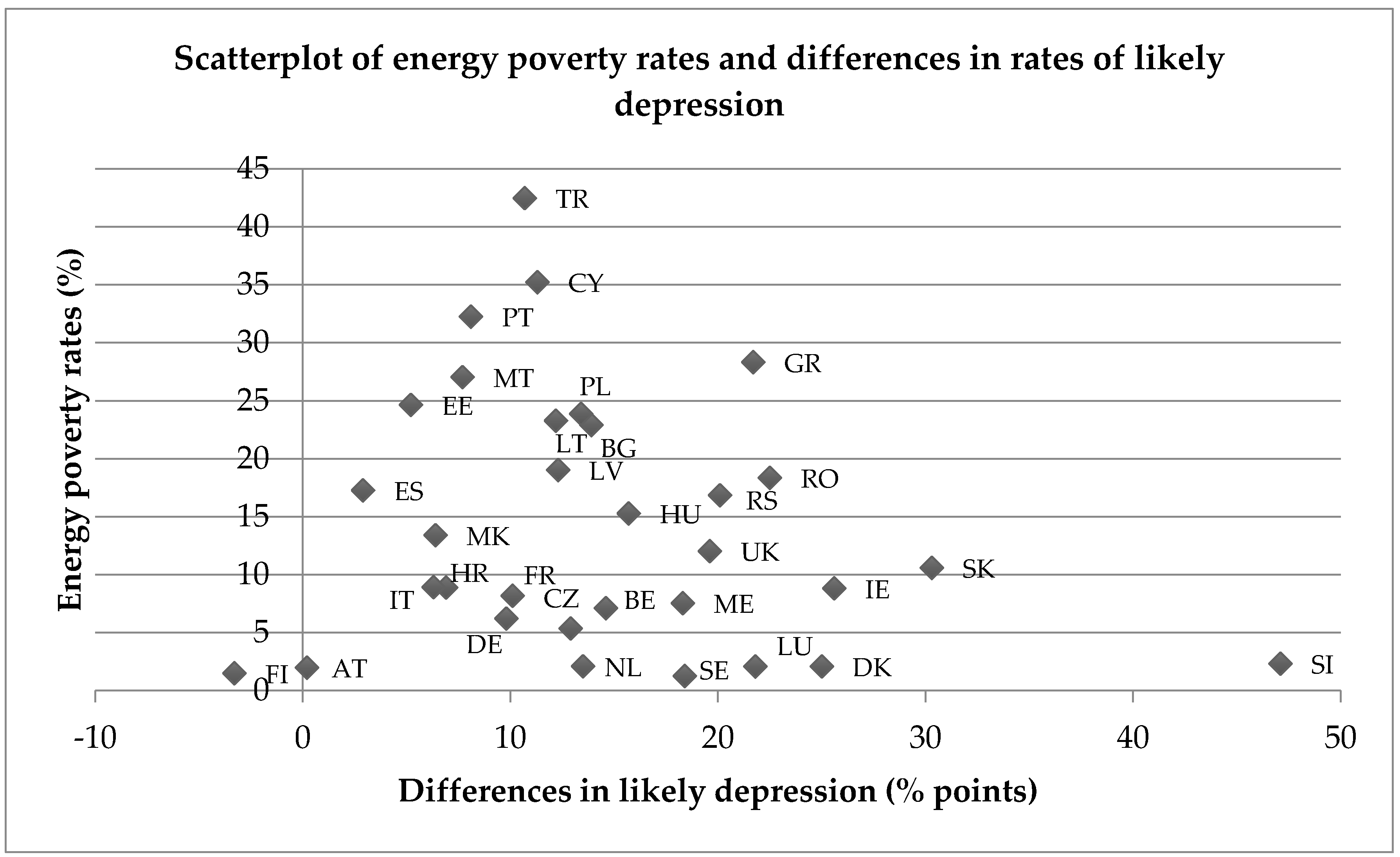
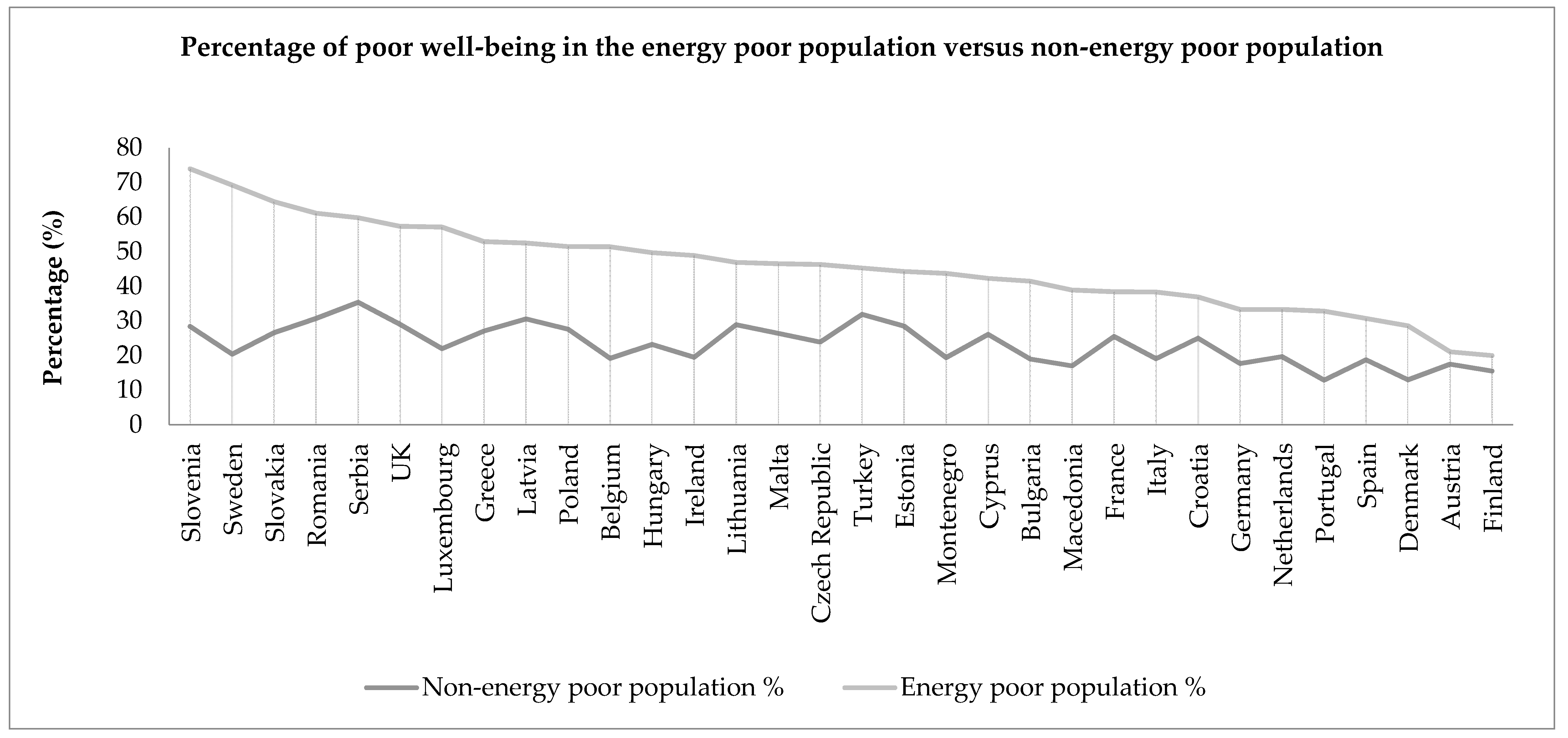
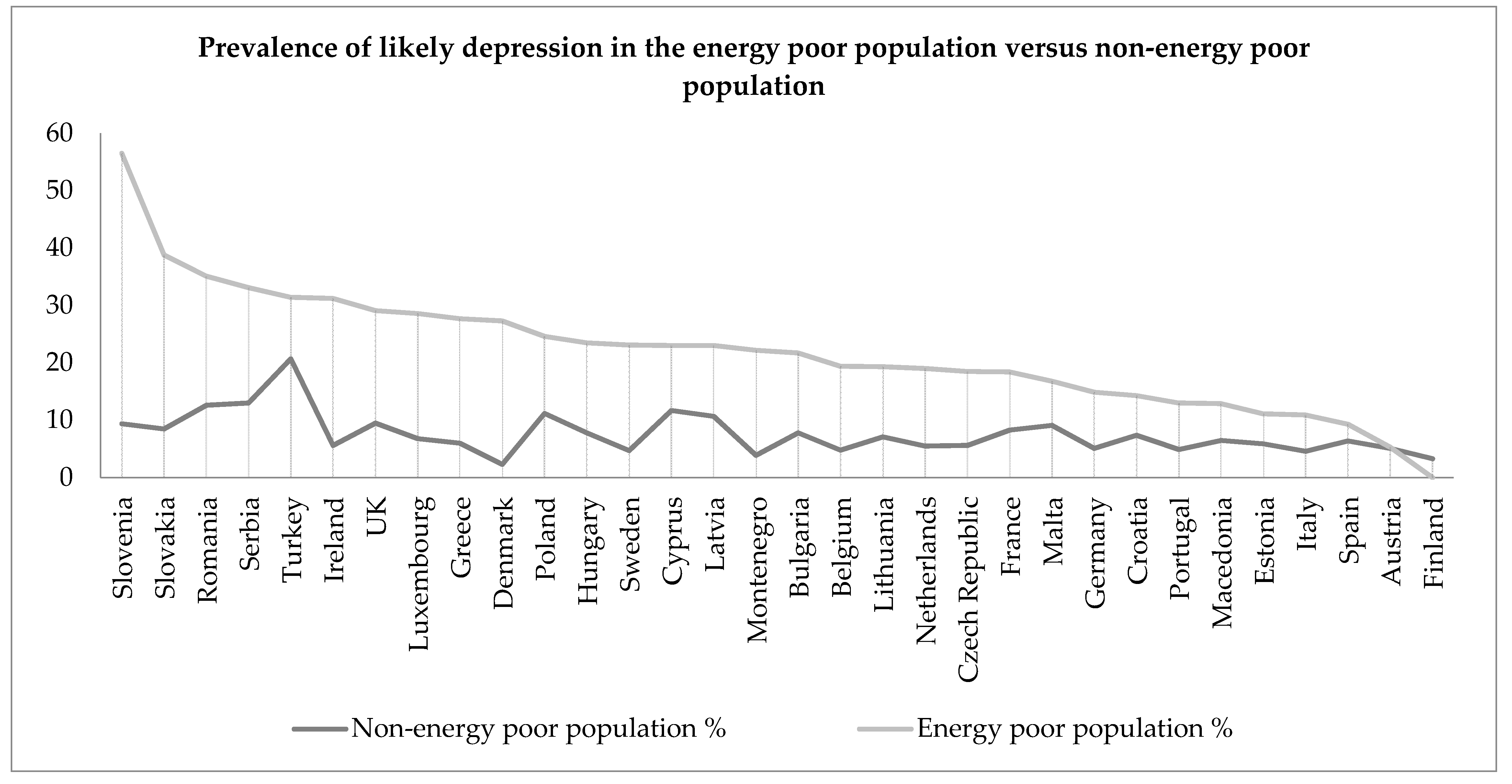
4.2. Poor Emotional Well-Being and Energy Poverty
5. Discussion
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country Name | Two-Letter Country Code |
|---|---|
| Austria | AT |
| Belgium | BE |
| Bulgaria | BG |
| Croatia | HR |
| Cyprus | CY |
| Czech Republic | CZ |
| Denmark | DK |
| Estonia | EE |
| Finland | FI |
| France | FR |
| Germany | DE |
| Greece | GR |
| Hungary | HU |
| Ireland | IE |
| Italy | IT |
| Latvia | LV |
| Lithuania | LT |
| Luxembourg | LU |
| Macedonia | MK |
| Malta | MT |
| Montenegro | ME |
| Netherlands | NL |
| Poland | PL |
| Portugal | PT |
| Romania | RO |
| Serbia | RS |
| Slovakia | SK |
| Slovenia | SI |
| Spain | ES |
| Sweden | SE |
| Turkey | TR |
| United Kingdom | UK |
References
- Boardman, B. Fuel poverty synthesis: Lessons learnt, actions needed. Energy Policy 2012, 49, 143–148. [Google Scholar]
- Fahmy, E.; Gordon, D.; Patsios, D. Predicting fuel poverty at a small-area level in England. Energy Policy 2011, 39, 4370–4377. [Google Scholar] [CrossRef]
- Kaye, A.; Jordan, H.; Baker, M. The Tipping Point: The Human and Economic Cost of Cutting Disabled People’s Support; The Hardest Hit Coalition: London, UK, 2012. [Google Scholar]
- Wood, C. Tracking the Lives of Disabled Families through the Cuts: Destination Unknown Autumn 2011; DEMOS: London, UK, 2011. [Google Scholar]
- Hills, J. Getting the Measure of Fuel Poverty: Final Report of the Fuel Poverty Review; CASE Report 72; London School of Economics and Political Science: London, UK, 2012. [Google Scholar]
- Koh, L.; Marchand, R.; Genovese, A.; Brennan, A. Fuel Poverty: Perspectives from the Front Line; Fuel Poverty Series; University of Sheffield, Centre for Energy, Environment and Sustainability: Sheffield, UK, 2012. [Google Scholar]
- Waddams, C.; Deller, D. Affordability of Utilities' Services: Extent, Practice, Policy; Centre on Regulation in Europe: Brussels, Belgium, 2015. [Google Scholar]
- Boardman, B. Fuel Poverty: From Cold Homes to Affordable Warmth; Belhaven Press: London, UK, 1991. [Google Scholar]
- Lewis, P. Fuel Poverty Can Be Stopped; National Right to Fuel Campaign: Bradford, UK, 1982. [Google Scholar]
- Tirado Herrero, S.; Jiménez Meneses, L.; López Fernández, J.L.; Martín García, J. Pobreza Energética en España. Análisis de Tendencias; Asociación de Ciencias Ambientales: Madrid, Spain, 2014. [Google Scholar]
- Bouzarovski, S.; Petrova, S. A global perspective on domestic energy deprivation: Overcoming the energy poverty–fuel poverty binary. Energy Res. Soc. Sci. 2015, 10, 31–40. [Google Scholar] [CrossRef]
- Thomson, H.; Snell, C.; Liddell, C. Fuel poverty in the European Union: A concept in need of definition? People Place Policy 2016, 10, 5–24. [Google Scholar] [CrossRef]
- Bouzarovski, S.; Tirado Herrero, S.; Petrova, S.; Ürge-Vorsatz, D. Unpacking the spaces and politics of energy poverty: Path-dependencies, deprivation and fuel switching in post-communist Hungary. Local Environ. 2016, 21, 1151–1170. [Google Scholar] [CrossRef]
- Katsoulakos, N. Combating Energy Poverty in Mountainous Areas Through Energy-saving Interventions. Mt. Res. Dev. 2011, 31, 284–292. [Google Scholar] [CrossRef]
- Legendre, B.; Ricci, O. Measuring fuel poverty in France: Which households are the most fuel vulnerable? Energy Econ. 2015, 49, 620–628. [Google Scholar] [CrossRef]
- Phimister, E.; Vera-Toscano, E.; Roberts, D. The Dynamics of Energy Poverty: Evidence from Spain. Econ. Energy Environ. Policy 2015, 4. [Google Scholar] [CrossRef]
- Bouzarovski, S.; Tirado Herrero, S. The energy divide: Integrating energy transitions, regional inequalities and poverty trends in the European Union. Eur. Urban Reg. Stud. 2017, 24, 69–86. [Google Scholar] [CrossRef]
- Dubois, U.; Meier, H. Energy affordability and energy inequality in Europe: Implications for policymaking. Energy Res. Soc. Sci. 2016, 18, 21–35. [Google Scholar] [CrossRef]
- Rademaekers, K.; Yearwood, J.; Ferreira, A.; Pye, S.; Hamilton, I.; Agnolucci, P.; Grover, D.; Karásek, J.; Anisimova, N. Selecting Indicators to Measure Energy Poverty; Trinomics: Rotterdam, The Netherlands, 2016. [Google Scholar]
- Thomson, H.; Snell, C. Quantifying the prevalence of fuel poverty across the European Union. Energy Policy 2013, 52, 563–572. [Google Scholar] [CrossRef]
- Lacroix, E.; Chaton, C. Fuel poverty as a major determinant of perceived health: The case of France. Public Health 2015, 129, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Liddell, C.; Guiney, C. Living in a cold and damp home: Frameworks for understanding impacts on mental well-being. Public Health 2015, 129, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Green, G.; Gilbertson, J. Health Impact Evaluation of the Warm Front Scheme; Centre for Regional, Economic and Social Research: Sheffield, UK, 2008. [Google Scholar]
- Hernández, D. Understanding “energy insecurity” and why it matters to health. Soc. Sci. Med. 2016, 167, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Howden-Chapman, P.; Matheson, A.; Crane, J.; Viggers, H.; Cunningham, M.; Blakely, T.; Cunningham, C.; Woodward, A.; Saville-Smith, K.; O’Dea, D.; et al. Effect of insulating existing houses on health inequality: Cluster randomised study in the community. BMJ 2007, 334, 460. [Google Scholar] [CrossRef] [PubMed]
- Liddell, C.; Morris, C. Fuel poverty and human health: A review of recent evidence. Energy Policy 2010, 38, 2987–2997. [Google Scholar] [CrossRef]
- Marmot Review Team. The Health Impacts of Cold Homes and Fuel Poverty; Friends of the Earth and the Marmot Review Team: London, UK, 2011. [Google Scholar]
- Snell, C.; Bevan, M.; Thomson, H. Justice, fuel poverty and disabled people in England. Energy Res. Soc. Sci. 2015, 10, 123–132. [Google Scholar] [CrossRef]
- Snell, C.; Bevan, M.; Thomson, H. Welfare reform, disabled people and fuel poverty. J. Poverty Soc. Justice 2015, 23, 229–244. [Google Scholar] [CrossRef]
- Thomson, H.; Petticrew, M.; Morrison, D. Health effects of housing improvement: Systematic review of intervention studies. BMJ 2001, 323, 187–190. [Google Scholar] [CrossRef] [PubMed]
- Health Service Executive Minister Naughten announces €10m for Warmth & Wellbeing in 2017. Available online: https://www.hse.ie/eng/services/news/media/pressrel/minister-naughten-announces-€10m-for-warmth-wellbeing-in-2017.html (accessed on 17 January 2017).
- Lanthier-Veilleux, M.; Généreux, M.; Baron, G. Prevalence of Residential Dampness and Mold Exposure in a University Student Population. Int. J. Environ. Res. Public. Health 2016, 13, 194. [Google Scholar] [CrossRef] [PubMed]
- Hernández, D.; Phillips, D.; Siegel, E.L. Exploring the Housing and Household Energy Pathways to Stress: A Mixed Methods Study. Int. J. Environ. Res. Public. Health 2016, 13, 916. [Google Scholar] [CrossRef] [PubMed]
- Department of Trade and Industry. UK Fuel Poverty Strategy; HMSO: London, UK, 2001.
- Fuel Poverty Action Group Taking Action on Fuel Poverty. Available online: www.dpac.uk/net/2012/06/taking-action-on-fuel-poverty (accessed on 29 November 2012).
- Harrington, B.E.; Heyman, B.; Merleau-Ponty, N.; Stockton, H.; Ritchie, N.; Heyman, A. Keeping warm and staying well: Findings from the qualitative arm of the Warm Homes Project. Health Soc. Care Community 2005, 13, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Gilbertson, J.; Grimsley, M.; Green, G. Psychosocial routes from housing investment to health: Evidence from England’s home energy efficiency scheme. Energy Policy 2012, 49, 122–133. [Google Scholar] [CrossRef]
- World Health Organization. Health Impact of Low Indoor Temperatures; WHO Regional Office for Europe: Copenhagen, Denmark, 1985. [Google Scholar]
- National Institute for Health and Care Excellence. Excess Winter Deaths and Illness and the Health Risks Associated with Cold Homes; National Institute for Health and Care Excellence: London, UK, 2015.
- Rowlingson, K. Does Income Inequality Cause Health and Social Problems? Joseph Rowntree Foundation: York, UK, 2011. [Google Scholar]
- Wilkinson, R.; Pickett, K. The Spirit Level: Why Greater Equality Makes Societies Stronger; Bloomsbury Press: London, UK, 2009. [Google Scholar]
- Peate, I. Keeping Warm: Health Risks and Vulnerable People. Nurs. Resid. Care 2008, 10, 606–610. [Google Scholar] [CrossRef]
- Day, R.; Hitchings, R. “Only old ladies would do that”: Age stigma and older people’s strategies for dealing with winter cold. Health Place 2011, 17, 885–894. [Google Scholar] [CrossRef] [PubMed]
- Disability Rights UK. Disability Rights UK Signs up to the Energy Revolution. Available online: https://www.disabilityrightsuk.org/policy-campaigns/campaigns/disability-rights-uk-signs-energy-revolution (accessed on 29 November 2012).
- El Ansari, W.; El-Silimy, S. Are fuel poverty reduction schemes associated with decreased excess winter mortality in elders? A case study from London, U.K. Chronic Illn. 2008, 4, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Goodman, P.; McAvoy, H.; Cotter, N.; Monahan, E.; Barrett, E.; Browne, S.; Zeke, A. Fuel Poverty, Older People and Cold Weather: An All-Island Analysis; Dublin Institute of Technology: Dublin, Ireland, 2011. [Google Scholar]
- Howden-Chapman, P. Housing standards: A glossary of housing and health. J. Epidemiol. Community Health 2004, 58, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Stewart, J.; Habgood, V. Benefits of a health impact assessment in relation to fuel poverty: Assessing Luton’s Affordable Warmth Strategy and the need for a national mandatory strategy. J. R. Soc. Promot. Health 2008, 128, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Osman, L.M.; Ayres, J.G.; Garden, C.; Reglitz, K.; Lyon, J.; Douglas, J.G. Home warmth and health status of COPD patients. Eur. J. Public Health 2008, 18, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Ormandy, D.; Ezratty, V. Health and thermal comfort: From WHO guidance to housing strategies. Energy Policy 2012, 49, 116–121. [Google Scholar] [CrossRef]
- Rudge, J.; Gilchrist, R. Excess winter morbidity among older people at risk of cold homes: A population-based study in a London borough. J. Public Health 2005, 27, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Bøkenes, L.; Mercer, J.B.; MacEvilly, S.; Andrews, J.F.; Bolle, R. Annual variations in indoor climate in the homes of elderly persons living in Dublin, Ireland and Tromsø, Norway. Eur. J. Public Health 2011, 21, 526–531. [Google Scholar] [CrossRef] [PubMed]
- Department of Health. How to Reduce the Risk of Seasonal Excess Deaths Systematically in Vulnerable Older People to Impact at Population Level; Department of Health: London, UK, 2010.
- Department of Health. Improving Outcomes and Supporting Transparency: Part 1: A Public Health Outcomes Framework for England 2013–2016; Department of Health: London, UK, 2012.
- Hales, S.; Blakely, T.; Foster, R.H.; Baker, M.G.; Howden-Chapman, P. Seasonal patterns of mortality in relation to social factors. J. Epidemiol. Community Health 2012, 66, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Liddell, C.; Morris, C.; Thomson, H.; Guiney, C. Excess winter deaths in 30 European countries 1980–2013: A critical review of methods. J. Public Health 2016, 38, 806–814. [Google Scholar] [CrossRef] [PubMed]
- Fowler, T.; Southgate, R.J.; Waite, T.; Harrell, R.; Kovats, S.; Bone, A.; Doyle, Y.; Murray, V. Excess winter deaths in Europe: A multi-country descriptive analysis. Eur. J. Public Health 2015, 25, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Healy, J.D. Excess winter mortality in Europe: A cross country analysis identifying key risk factors. J. Epidemiol. Community Health 2003, 57, 784–789. [Google Scholar] [CrossRef] [PubMed]
- Braubach, M.; Jacobs, D.E.; Ormandy, D. Environmental Burden of Disease Associated with Inadequate Housing; WHO Regional Office for Europe: Copenhagen, Denmark, 2011. [Google Scholar]
- Healy, J.D. Housing, Fuel Poverty and Health: A Pan-European Analysis; Ashgate: Aldershot, UK, 2004. [Google Scholar]
- Eurofound. European Quality of Life Survey, 2011–2012 [Computer File], 2nd ed.; UK Data Archive [distributor]: Colchester, UK, January 2014. [Google Scholar]
- Eurofound. Second European Quality of Life Survey: Overview; Office for Official Publications of the European Communities: Luxembourg, 2009. [Google Scholar]
- Eurofound. Third European Quality of Life Survey—Quality of Life in Europe: Impacts of the Crisis; Publications Office of the European Union: Luxembourg, 2012. [Google Scholar]
- Thomson, H.; Bouzarovski, S.; Snell, C. Rethinking the measurement of energy poverty in Europe: A critical analysis of indicators and data. Indoor Built Environ. 2017. [Google Scholar] [CrossRef]
- Healy, J.D.; Clinch, J.P. Fuel Poverty in Europe: A Cross-Country Analysis Using a New Composite Measure; Environmental Studies Research Series; University College Dublin: Dublin, Ireland, 2002. [Google Scholar]
- Dunn, S.L.; Arslanian-Engoren, C.; DeKoekkoek, T.; Jadack, R.; Scott, L.D. Secondary Data Analysis as an Efficient and Effective Approach to Nursing Research. West. J. Nurs. Res. 2015, 37, 1295–1307. [Google Scholar] [CrossRef] [PubMed]
- Artazcoz, L.; Cortès, I.; Benavides, F.G.; Escribà-Agüir, V.; Bartoll, X.; Vargas, H.; Borrell, C. Long working hours and health in Europe: Gender and welfare state differences in a context of economic crisis. Health Place 2016, 40, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Mulinari, S.; Bredström, A.; Merlo, J. Questioning the discriminatory accuracy of broad migrant categories in public health: Self-Rated health in Sweden. Eur. J. Public Health 2015, 25, 911–917. [Google Scholar] [CrossRef] [PubMed]
- Lundberg, O.; Manderbacka, K. Assessing reliability of a measure of self-rated health. Scand. J. Soc. Med. 1996, 24, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Maheswaran, H.; Kupek, E.; Petrou, S. Self-reported health and socio-economic inequalities in England, 1996–2009: Repeated national cross-sectional study. Soc. Sci. Med. 2015, 136–137, 135–146. [Google Scholar] [CrossRef] [PubMed]
- Mishra, S.; Carleton, R.N. Subjective relative deprivation is associated with poorer physical and mental health. Soc. Sci. Med. 2015, 147, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Miilunpalo, S.; Vuori, I.; Oja, P.; Pasanen, M.; Urponen, H. Self-rated health status as a health measure: The predictive value of self-reported health status on the use of physician services and on mortality in the working-age population. J. Clin. Epidemiol. 1997, 50, 517–528. [Google Scholar] [CrossRef]
- Mossey, J.M.; Shapiro, E. Self-rated health: A predictor of mortality among the elderly. Am. J. Public Health 1982, 72, 800–808. [Google Scholar] [CrossRef] [PubMed]
- Eurostat. Description of Target Variables: Cross-sectional and Longitudinal. EU-SILC 065/08; Publications Office of the European Union: Luxembourg, 2010. [Google Scholar]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Krieger, T.; Zimmermann, J.; Huffziger, S.; Ubl, B.; Diener, C.; Kuehner, C.; Grosse Holtforth, M. Measuring depression with a well-being index: Further evidence for the validity of the WHO Well-Being Index (WHO-5) as a measure of the severity of depression. J. Affect. Disord. 2014, 156, 240–244. [Google Scholar] [CrossRef] [PubMed]
- McDowell, I. Measures of self-perceived well-being. J. Psychosom. Res. 2010, 69, 69–79. [Google Scholar] [CrossRef] [PubMed]
- De Wit, M.; Pouwer, F.; Gemke, R.J.; Delemarre-van de Waal, H.A.; Snoek, F.J. Validation of the WHO-5 Well-Being Index in adolescents with type 1 diabetes. Diabetes Care 2007, 30, 2003–2006. [Google Scholar] [CrossRef] [PubMed]
- Dreger, C.; Lopez-Bazo, E.; Ramos, R.; Royuela, V.; Surinach, J. Wage and Income Inequality in the European Union; European Union: Brussels, Belgium, 2015. [Google Scholar]
- Smith, H.J.; Huo, Y.J. Relative Deprivation: How Subjective Experiences of Inequality Influence Social Behavior and Health. Policy Insights Behav. Brain Sci. 2014, 1, 231–238. [Google Scholar] [CrossRef]
- Åberg Yngwe, M.; Kondo, N.; Hägg, S.; Kawachi, I. Relative deprivation and mortality—A longitudinal study in a Swedish population of 4.7 million, 1990–2006. BMC Public Health 2012, 12, 664. [Google Scholar] [CrossRef] [PubMed]
- Tkalec, T.; Živčič, L. Report on National Situation in the Field of Energy Poverty: Slovenia. Available online: http://reach-energy.eu/wordpress/wp-content/uploads/2014/12/D2.2-Focus_EN.pdf (accessed on 20 June 2016).
- Friberg, D. The Swedish policy case for Cogeneration and District Heating. In Proceedings of the National snapshot of DH and CHP IEA, Paris, France, 12–13 February 2013. [Google Scholar]
- Euroheat & Power. Statistics Overview 2013; Euroheat & Power: Brussels, Belgium, 2015. [Google Scholar]
- Tirado Herrero, S.; Ürge-Vorsatz, D. Trapped in the heat: A post-communist type of fuel poverty. Energy Policy 2012, 49, 60–68. [Google Scholar] [CrossRef]
- Lindén, A.-L.; Carlsson-Kanyama, A.; Eriksson, B. Efficient and inefficient aspects of residential energy behaviour: What are the policy instruments for change? Energy Policy 2006, 34, 1918–1927. [Google Scholar] [CrossRef]
- Thomson, H.; Liddell, C. The suitability of wood pellet heating for domestic households: A review of literature. Renew. Sustain. Energy Rev. 2015, 42, 1362–1369. [Google Scholar] [CrossRef]
- Hamilton, I.; Milner, J.; Chalabi, Z.; Das, P.; Jones, B.; Shrubsole, C.; Davies, M.; Wilkinson, P. Health effects of home energy efficiency interventions in England: A modelling study. BMJ Open 2015, 5, e007298. [Google Scholar] [CrossRef] [PubMed]


| Country | Unweighted Sample Size | Energy Poverty (%) | Poor SRH (%) | Poor Well-Being (%) | Likely Depression (%) |
|---|---|---|---|---|---|
| Sweden | 1007 | 1.3 | 7.7 | 21.3 | 5.0 |
| Finland | 1020 | 1.5 | 7.0 | 15.6 | 3.2 |
| Austria | 1032 | 2.0 | 3.9 | 17.6 | 5.1 |
| Denmark | 1024 | 2.1 | 12.7 | 13.3 | 2.8 |
| Luxembourg | 1005 | 2.1 | 6.7 | 22.6 | 7.2 |
| Netherlands | 1008 | 2.1 | 9.9 | 20.0 | 5.8 |
| Slovenia | 1008 | 2.3 | 9.8 | 29.8 | 10.4 |
| Czech Republic | 1012 | 5.4 | 11.7 | 25.2 | 6.5 |
| Germany | 3055 | 6.2 | 8.9 | 18.7 | 5.8 |
| Belgium | 1013 | 7.1 | 8.9 | 21.7 | 5.9 |
| Montenegro | 1000 | 7.5 | 9.9 | 21.7 | 5.5 |
| France | 2270 | 8.2 | 6.6 | 26.7 | 9.1 |
| Ireland | 1051 | 8.8 | 4.4 | 22.2 | 7.9 |
| Croatia | 1001 | 8.9 | 13.5 | 25.9 | 8.0 |
| Italy | 2250 | 8.9 | 5.6 | 21.0 | 5.2 |
| Slovakia | 1000 | 10.6 | 10.6 | 30.5 | 11.8 |
| UK | 2252 | 12.0 | 11.0 | 32.6 | 11.9 |
| Macedonia | 1006 | 13.4 | 6.5 | 19.9 | 7.3 |
| Hungary | 1024 | 15.3 | 16.0 | 27.3 | 10.2 |
| Serbia | 1002 | 16.9 | 16.4 | 39.6 | 16.4 |
| Spain | 1512 | 17.3 | 5.6 | 20.9 | 7.0 |
| Romania | 1542 | 18.4 | 17.2 | 36.6 | 16.8 |
| Latvia | 1009 | 19.0 | 16.1 | 34.8 | 13.1 |
| Bulgaria | 1000 | 22.9 | 11.1 | 24.5 | 11.0 |
| Lithuania | 1134 | 23.3 | 20.8 | 33.3 | 10.0 |
| Poland | 2262 | 23.9 | 13.0 | 33.4 | 14.4 |
| Estonia | 1002 | 24.7 | 14.9 | 33.1 | 7.6 |
| Malta | 1001 | 27.1 | 3.2 | 31.3 | 11.1 |
| Greece | 1004 | 28.3 | 8.1 | 34.3 | 12.0 |
| Portugal | 1013 | 32.3 | 14.9 | 19.3 | 7.5 |
| Cyprus | 1006 | 35.2 | 3.3 | 31.8 | 15.6 |
| Turkey | 2035 | 42.5 | 8.6 | 37.6 | 25.4 |
| Country | OR | 95% CI |
|---|---|---|
| Austria | 3.19 | 0.52–19.65 |
| Belgium | 3.11 | 1.50–6.43 |
| Bulgaria | 2.10 | 1.24–3.53 |
| Croatia | 1.33 | 0.67–2.64 |
| Cyprus | 2.22 | 1.00–5.15 |
| Czech Republic | 1.99 | 0.92–4.30 |
| Denmark | 2.81 | 0.96–8.24 |
| Estonia | 1.20 | 0.76–1.91 |
| Finland | 1.03 | 0.18–5.89 |
| France | 1.10 | 0.61–1.99 |
| Germany | 1.70 | 1.04–2.78 |
| Greece | 2.44 | 1.31–4.56 |
| Hungary | 2.43 | 1.41–4.19 |
| Ireland | 6.52 | 3.10–13.71 |
| Italy | 1.51 | 0.77–2.95 |
| Latvia | 1.73 | 1.11–2.70 |
| Lithuania | 1.70 | 1.17–2.46 |
| Luxembourg | 3.72 | 0.83–16.60 |
| Macedonia | 1.59 | 0.70–3.61 |
| Malta | 5.63 | 2.11–15.05 |
| Montenegro | 3.82 | 1.77–8.22 |
| Netherlands | 4.70 | 1.76–12.59 |
| Poland | 1.63 | 1.17–2.27 |
| Portugal | 2.23 | 1.30–3.80 |
| Romania | 1.91 | 1.31–2.77 |
| Serbia | 1.70 | 0.98–2.95 |
| Slovakia | 2.32 | 1.18–4.60 |
| Slovenia | 26.32 | 4.76–145.68 |
| Spain | 2.80 | 1.48–5.29 |
| Sweden | 7.12 | 1.62–31.40 |
| Turkey | 1.91 | 1.28–2.85 |
| UK | 2.18 | 1.46–3.25 |
| Country | Poor Well-Being | Likely Depression | ||
|---|---|---|---|---|
| Odds Ratio | 95% CI | Odds Ratio | 95% CI | |
| Austria | 0.91 | 0.27–3.12 | 1.05 | 0.13–8.16 |
| Belgium | 3.68 | 2.00–6.76 | 3.19 | 1.41–7.23 |
| Bulgaria | 2.93 | 1.95–4.39 | 2.69 | 1.63–4.45 |
| Croatia | 1.09 | 0.61–1.94 | 1.06 | 0.47–2.39 |
| Cyprus | 1.36 | 0.94–1.98 | 1.51 | 0.95–2.41 |
| Czech Republic | 2.15 | 1.16–4.00 | 2.63 | 1.10–6.29 |
| Denmark | 2.35 | 0.81–6.77 | 34.58 | 8.36–143.01 |
| Estonia | 1.49 | 1.03–2.15 | 1.44 | 0.81–2.57 |
| Finland | 1.71 | 0.43–6.71 | 0.00 | 0.00–0.00 |
| France | 1.59 | 1.13–2.24 | 2.01 | 1.28–3.14 |
| Germany | 1.95 | 1.35–2.81 | 2.29 | 1.39–3.78 |
| Greece | 3.80 | 2.56–5.65 | 4.56 | 2.71–7.68 |
| Hungary | 2.49 | 1.63–3.82 | 2.69 | 1.55–4.66 |
| Ireland | 3.76 | 2.28–6.19 | 6.42 | 3.48–11.84 |
| Italy | 1.78 | 1.19–2.67 | 1.47 | 0.76–2.84 |
| Latvia | 2.26 | 1.56–3.27 | 2.00 | 1.25–3.21 |
| Lithuania | 1.97 | 1.44–2.70 | 2.57 | 1.65–4.00 |
| Luxembourg | 1.38 | 0.38–5.04 | 2.18 | 0.44–10.78 |
| Macedonia | 3.36 | 2.05–5.48 | 2.53 | 1.20–5.34 |
| Malta | 2.01 | 1.32–3.05 | 1.79 | 1.01–3.18 |
| Montenegro | 2.09 | 1.09–4.02 | 3.91 | 1.66–9.19 |
| Netherlands | 1.72 | 0.65–4.52 | 2.67 | 0.75–9.43 |
| Poland | 2.10 | 1.64–2.68 | 1.67 | 1.23–2.28 |
| Portugal | 3.00 | 1.91–4.72 | 2.30 | 1.20–4.40 |
| Romania | 2.62 | 1.91–3.58 | 2.54 | 1.80–3.59 |
| Serbia | 2.02 | 1.25–3.27 | 1.99 | 1.18–3.35 |
| Slovakia | 2.58 | 1.50–4.46 | 3.08 | 1.65–5.76 |
| Slovenia | 3.36 | 1.02–11.03 | 19.93 | 5.29–75.09 |
| Spain | 1.74 | 1.15–2.64 | 1.79 | 0.93–3.45 |
| Sweden | 7.84 | 1.62–38.02 | 3.39 | 0.64–18.00 |
| Turkey | 1.65 | 1.32–2.05 | 1.47 | 1.15–1.87 |
| UK | 2.64 | 1.91–3.64 | 2.76 | 1.89–4.03 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thomson, H.; Snell, C.; Bouzarovski, S. Health, Well-Being and Energy Poverty in Europe: A Comparative Study of 32 European Countries. Int. J. Environ. Res. Public Health 2017, 14, 584. https://doi.org/10.3390/ijerph14060584
Thomson H, Snell C, Bouzarovski S. Health, Well-Being and Energy Poverty in Europe: A Comparative Study of 32 European Countries. International Journal of Environmental Research and Public Health. 2017; 14(6):584. https://doi.org/10.3390/ijerph14060584
Chicago/Turabian StyleThomson, Harriet, Carolyn Snell, and Stefan Bouzarovski. 2017. "Health, Well-Being and Energy Poverty in Europe: A Comparative Study of 32 European Countries" International Journal of Environmental Research and Public Health 14, no. 6: 584. https://doi.org/10.3390/ijerph14060584