
Cognitive-Motivational Determinants of Residents’ Civic Engagement and Health (Inequities) in the Context of Noise Action Planning: A Conceptual Model

 ,
,  ,
,
Abstract
:1. Introduction
2. Model on Household’s Vulnerability to the Local Environment (MOVE)
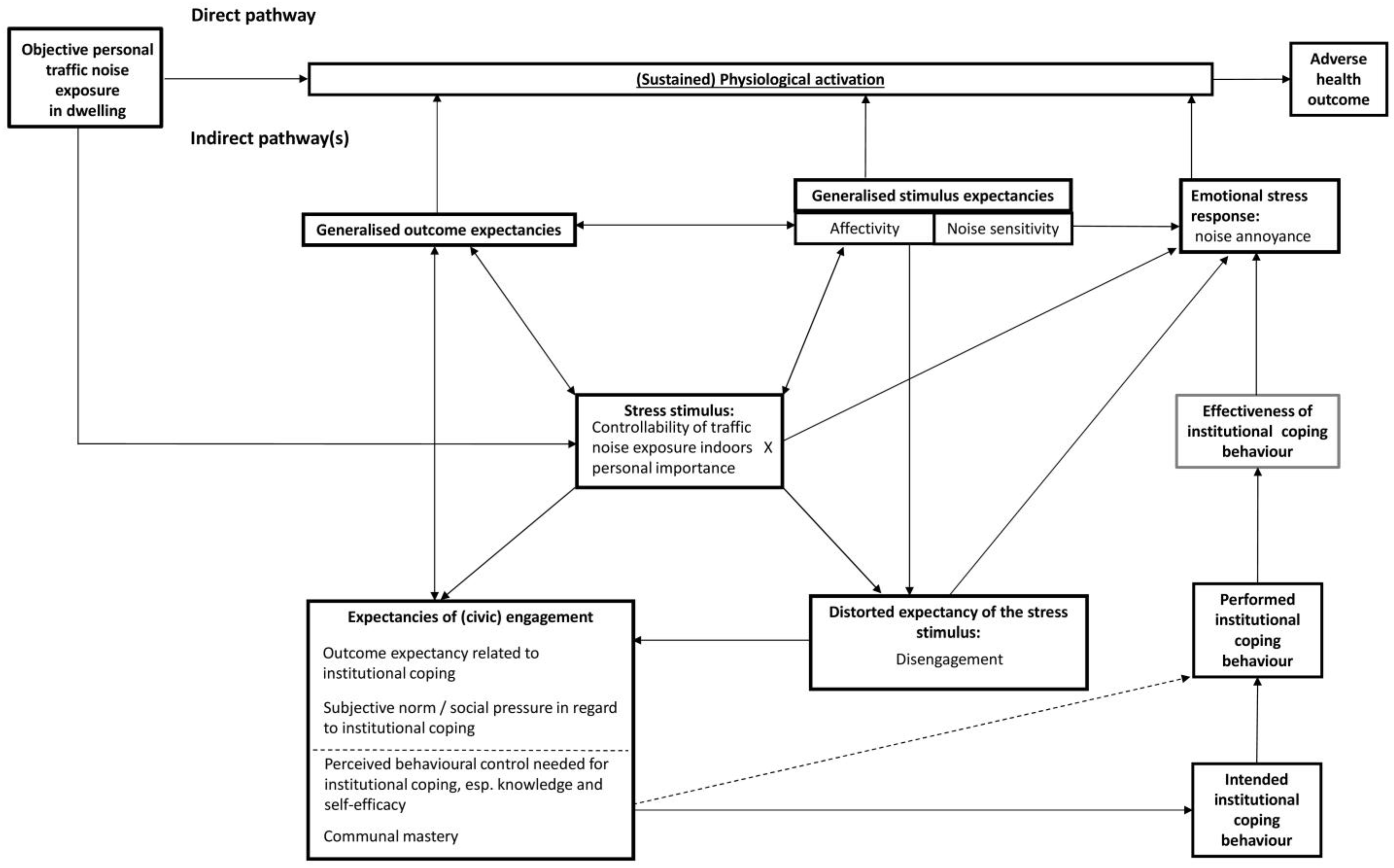
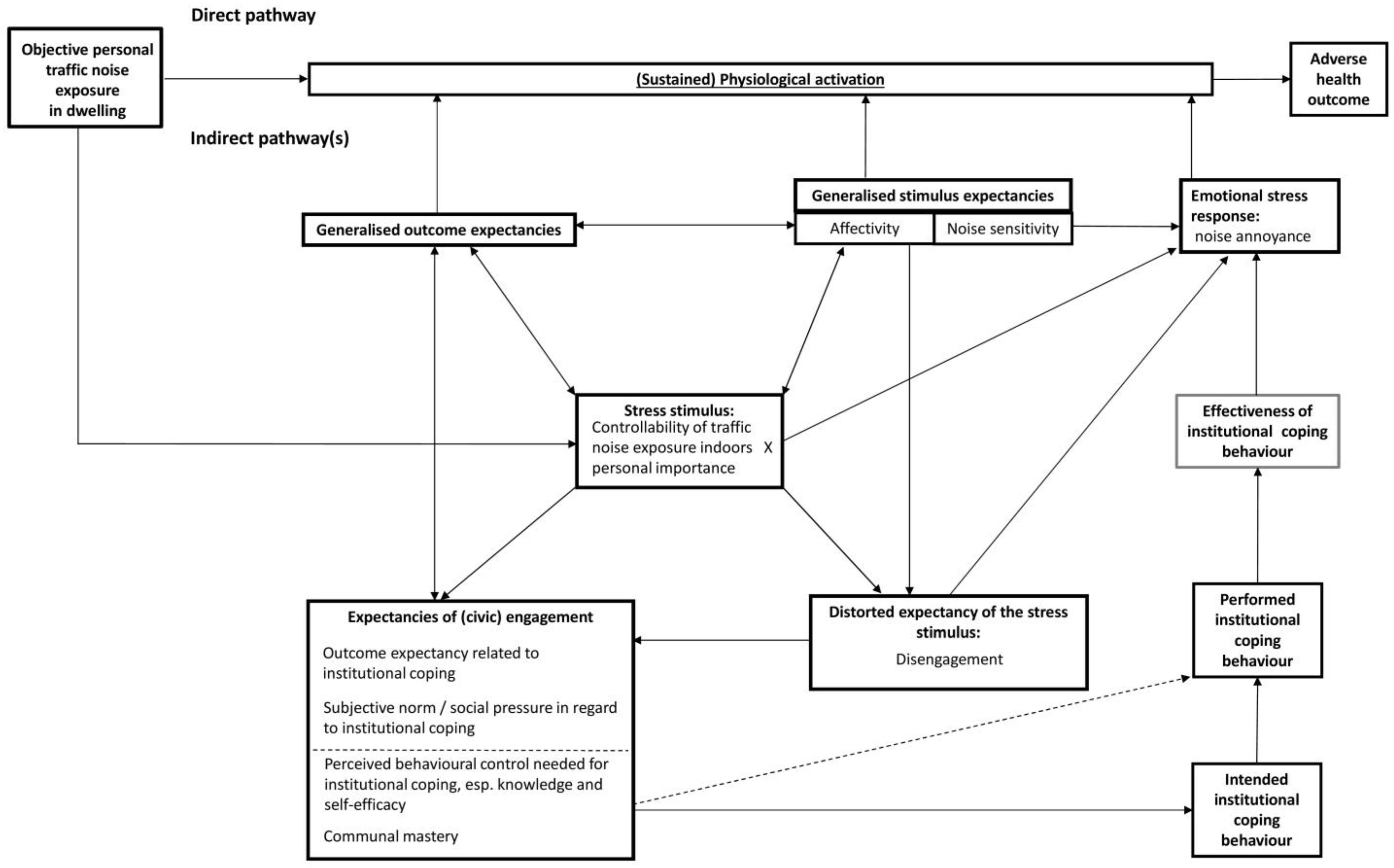
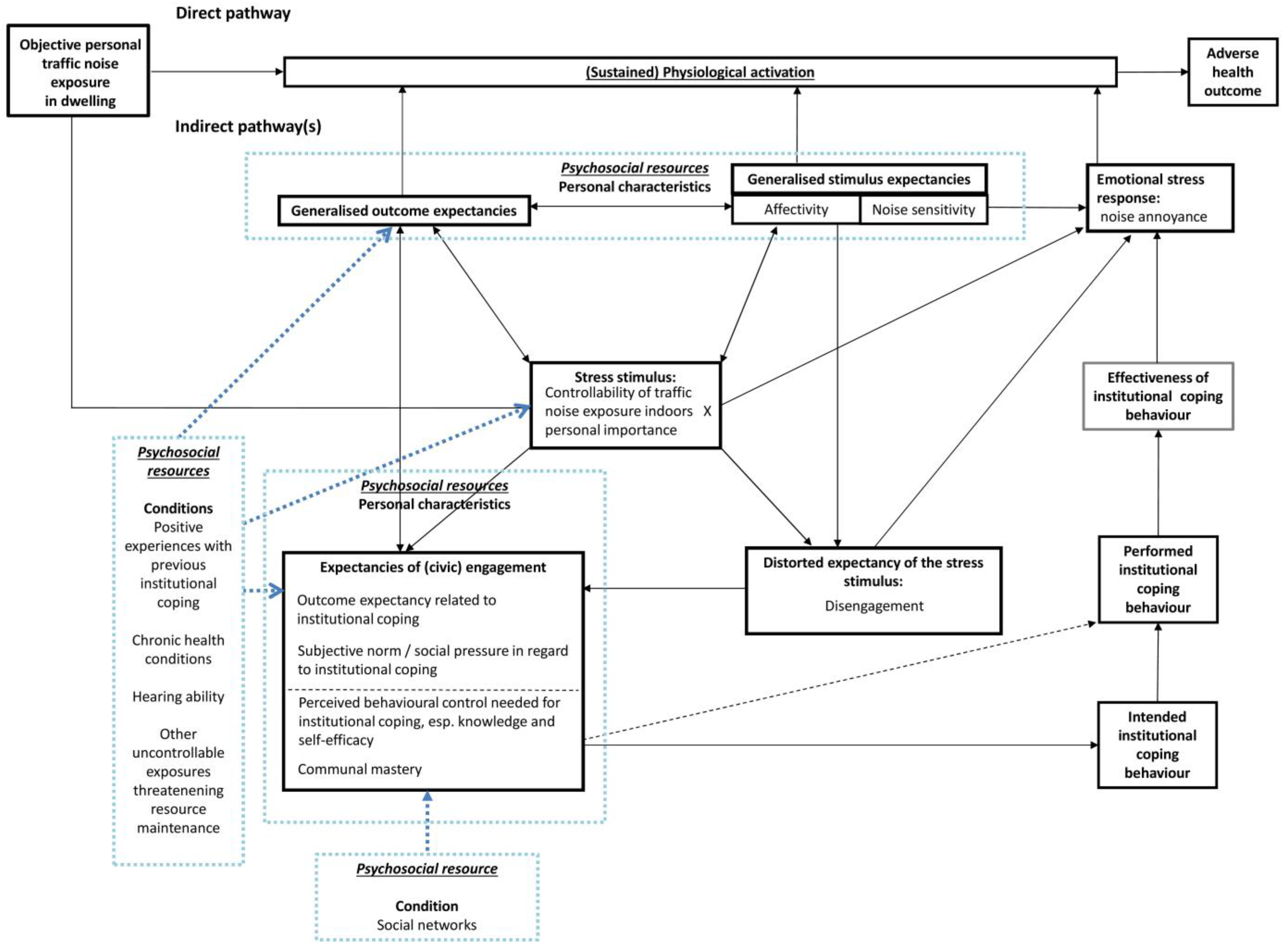
- Behavioural beliefs (“the subjective probability that the behaviour will produce a given outcome” [37]) engender a specific attitude towards institutional coping behaviour. In MOVE, a resident is more likely to choose an institutional coping strategy if she or he expects her or his engagement with environmental quality to be worthwhile (perceived value of the outcome of institutional coping behaviour), prefers quietness, and rates environmental quality as low (as measured by annoyance).
- Normative beliefs (“the perceived behavioural expectations of [..] important referent individuals” [37]) bring about residents’ subjective norm and social pressure to initiate MOVE institutional coping. A resident’s inclination to institutional coping behaviour is more pronounced if she or he anticipates positive reactions from those who are close and important to her or him. In a way, the subjective norm also represents positive outcome expectancy.
- Control beliefs (“perceived presence of factors that may facilitate or impede performance of a behaviour” [37]) become manifest in residents’ perceived behavioural control. Ajzen [35] distinguishes two aspects of perceived behavioural control: behavioural controllability (“belief about the extent to which performing behaviour is up to the actor”) and self-efficacy (“ease or difficulty of performing a behaviour”). The more a resident assumes to know about objective environmental quality and environmental rights, the greater her or his engagement-specific controllability. Equally, the more she or he feels confident and capable of civic engagement, the more self-efficacy regarding civic engagement is present. The stronger engagement-specific controllability and self-efficacy are, the higher the chance that a resident will adopt an institutional coping strategy.
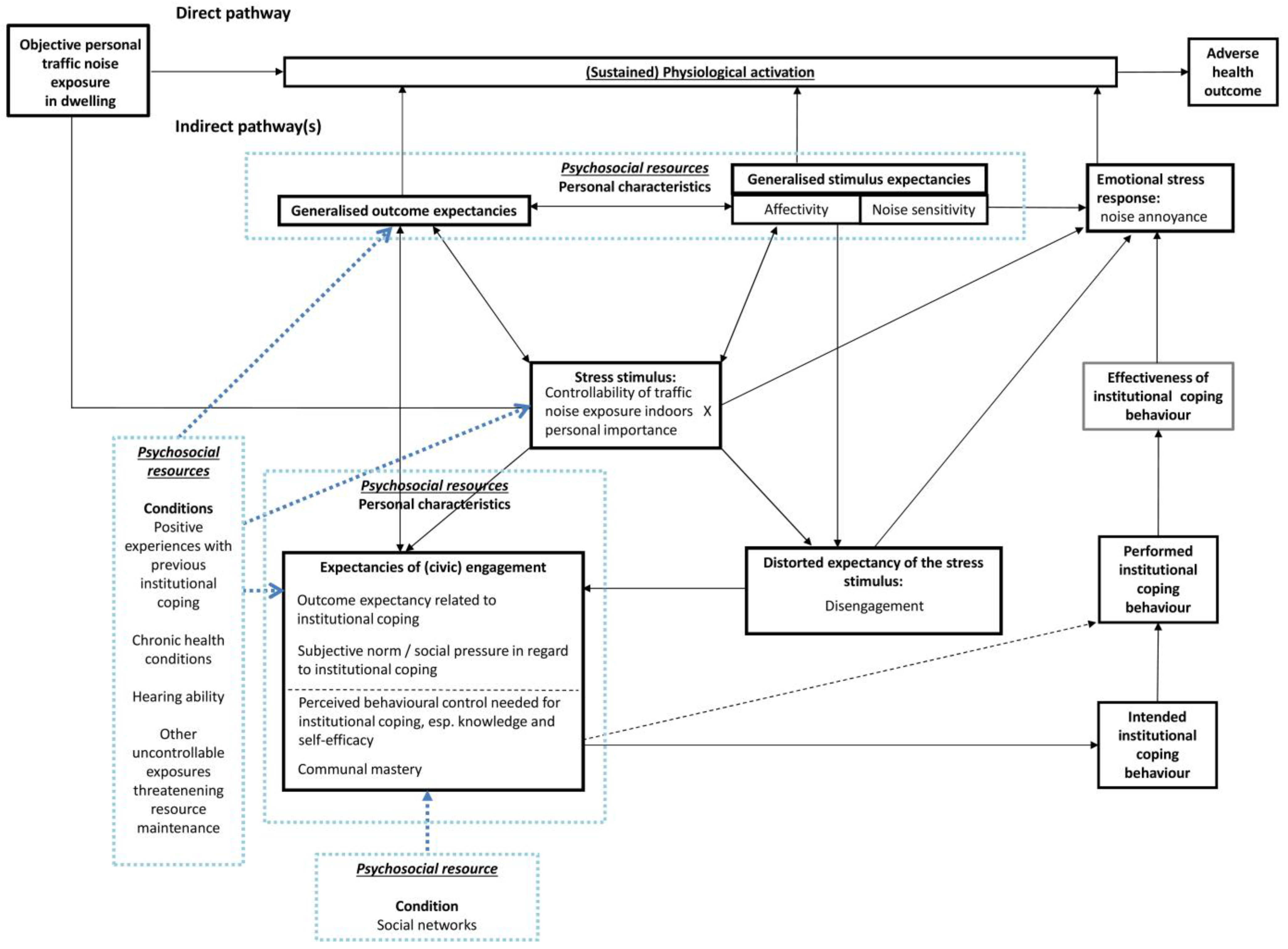
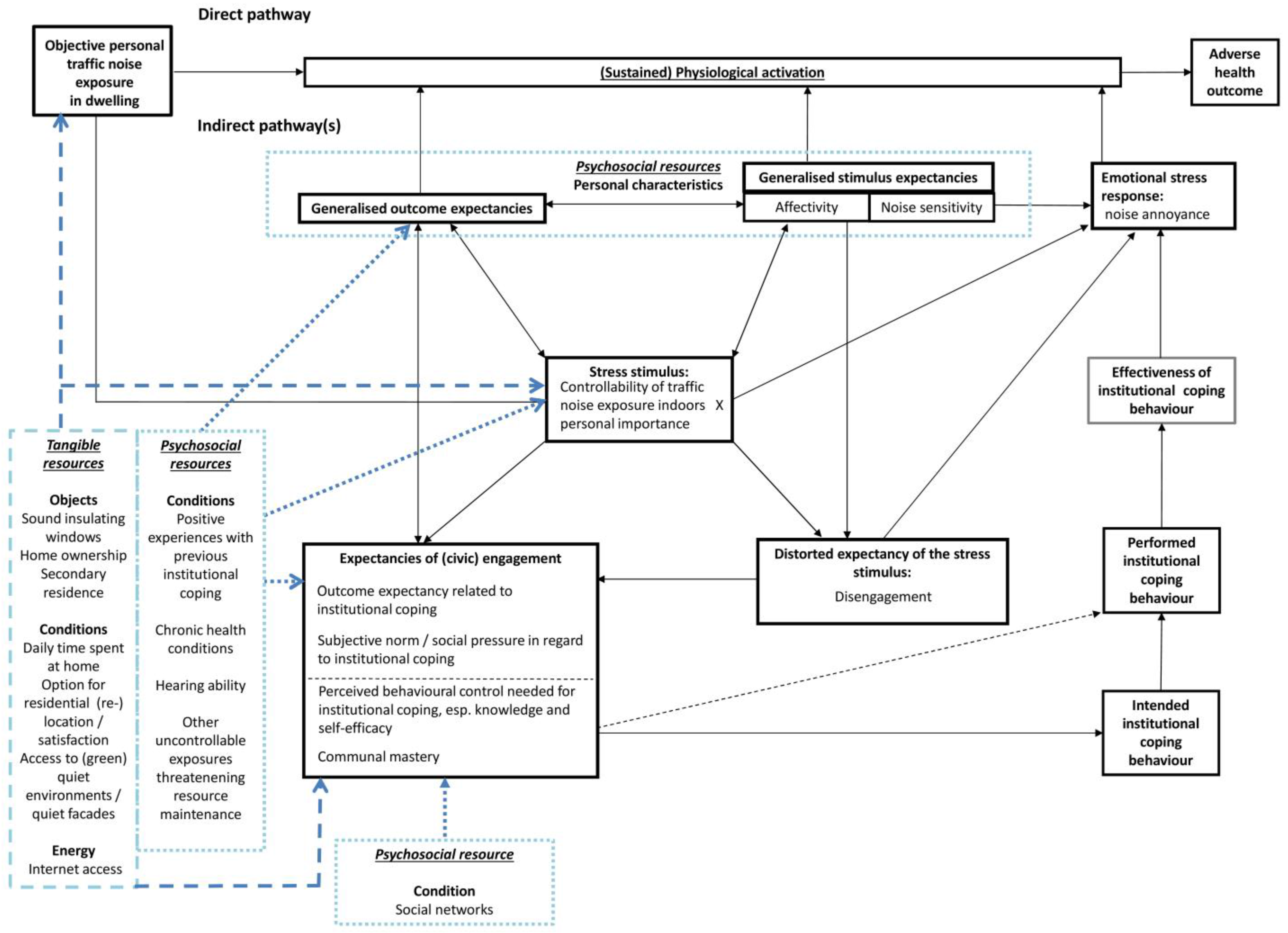
- “Objects”: They are appreciated because of their “physical nature” and/or the status that individuals attribute to their acquisition or ownership (e.g., home ownership).
- “Personal characteristics”: They are supportive of a “positive sense of self and a view that one can master or at least see through stressful circumstances”. An example of personal characteristics is the communal mastery, which is an individual’s belief to be able to reach goals or to overcome challenging situations due to being affiliated with others [40]. MOVE specifies communal mastery by residents’ perceived collective competence to exert control over their home and neighbourhood. Communal mastery is theoretically related to the aspect of self-efficacy integrated in the perceived behavioural control of institutional coping, but expanded by a pro-social aspect of collective action.
- “Conditions”: They define either personal circumstance (e.g., age) or are desired for their own value and for being a key to other resources (e.g., social networks).
- “Energies”: They provide the means to gain resources in the previous categories (e.g., income, knowledge).
3. Integration of Noise-Induced Helplessness and Cognitive Activation Theory of Stress
3.1. Noise-Induced Learned Helplessness vs. Civic Engagement for Health?
3.2. The Cognitive Activation Theory of Stress (CATS)
4. First Step towards a Refined Model: Reframing MOVE Based on CATS
4.1. General Considerations: Reframing MOVE Based on CATS
4.2. Specification of Our Model: Hypothetical Patterns of Cognitive-Motivational Determinants
- perceived high controllability of traffic noise exposure indoors x low personal importance (affective value),
- perceived high controllability of traffic noise exposure indoors x high personal importance,
- perceived low controllability of traffic noise exposure indoors x low personal importance, and
- perceived low controllability of traffic noise exposure indoors x high personal importance.
5. Second Step towards a Refined Model: Adding Resources
5.1. Psychosocial Resources
- social gradients in the three kinds of outcome expectancies (positive, no control and negative) in the expected directions, and
- positive correlations between a positive outcome expectancy and active, instrumental coping strategies, as well as between generalised no control- and negative outcome expectancies and passivity and depressiveness (see also [87]).
5.2. Tangible Resources
5.3. Social Position
6. Intervention Opportunities Based on Our Conceptual Model
- environmental and planning determinants (e.g., direct contributions to resource aggregates by means of distributional “amendments” in the soundscape of residential environment, see the project “QUADMAP QUiet Areas Definition & Management in Action Plans” [106], and inplanning procedures promoting positive behaviour-outcome relationships);
- stimulus characterisations (e.g., figuring out where noise attributions are objectively unrealistic or wrong);
- effective response options (e.g., learning new skills, expanding the coping repertoire, and rectifying expectations of outcomes during participation processes).
7. Conclusions
Notes
Acknowledgments
Author Contributions
Conflicts of Interest
References
- WHO Regional Office for Europe. Burden of Disease from Environmental Noise. Quantification of Healthy Life Years Lost in Europe; World Health Organization Regional Office for Europe: Geneva, Switzerland; Copenhagen, Denmark, 2011. [Google Scholar]
- DIRECTIVE 2002/49/EC Relating to the Assessment and Management of Environmental Noise [Internet]. European Parliament and Council. Available online: http://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2002:189:0012:0025:EN:PDF (accessed on 22 March 2017).
- Rose, G. Sick individuals and sick populations. Int. J. Epidemiol. 1985, 14, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Kruize, H. On environmental equity. In Exploring the Distribution of Environmental Quality among Socio-Economic Categories in The Netherlands; Netherlands Geographical Studies 359; Koninklijk Nederlands Aardrijkskundig Genootschap: Utrecht, The Netherlands, 2007. [Google Scholar]
- Bolte, G.; Pauli, A.; Hornberg, C. Environmental justice—Social disparities in environmental exposures and health. Overview. In Encyclopedia of environmental health; Nriagu, J.O., Ed.; Elsevier Science: Amsterdam, The Netherlands; London, UK, 2011; pp. 459–470. [Google Scholar]
- Riedel, N.; Hoffmann, B.; Fuks, K.; Jöckel, K.-H.; Dragano, N. Health inequalities in the city: Assessing the concurrence of social and environmental risks in the Ruhr Area. UMID 2011, 2, 85–90. [Google Scholar]
- Bolte, G.; Bunge, C.; Hornberg, C.; Köckler, H.; Mielck, A. Umweltgerechtigkeit durch Chancengleichheit bei Umwelt und Gesundheit. Eine Einführung in die Thematik und Zielsetzung dieses Buches. In Umweltgerechtigkeit. Chancengleichheit bei Umwelt und Gesundheit: Konzepte, Datenlage und Handlungsperspektiven, 1st ed.; Bolte, G., Bunge, C., Hornberg, C., Köckler, H., Mielck, A., Eds.; Verlag Hans Huber: Bern, Switzerland, 2012; pp. 15–37. [Google Scholar]
- D’Alessandro, F.; Schiavoni, S. A review and comparative analysis of European priority indices for noise action plans. Sci. Total Environ. 2015, 518–519, 290–301. [Google Scholar] [CrossRef] [PubMed]
- Steinbach, R.; Grundy, C.; Edwards, P.; Wilkinson, P.; Green, J. The impact of 20 mph traffic speed zones on inequalities in road casualties in London. J. Epidemiol. Community Health 2011, 65, 921–926. [Google Scholar] [CrossRef] [PubMed]
- Kruize, H. Einfluss eines neuen Verkehrsplans (VCP) auf Personen mit unterschiedlich hohem Einkommen: Erfahrungen aus der Stadt Den Haag in den Niederlanden. In Umweltgerechtigkeit. Chancengleichheit bei Umwelt und Gesundheit: Konzepte, Datenlage und Handlungsperspektiven, 1st ed.; Bolte, G., Bunge, C., Hornberg, C., Köckler, H., Mielck, A., Eds.; Verlag Hans Huber: Bern, Switzerland, 2012; pp. 419–420. [Google Scholar]
- Tonne, C.; Beevers, S.; Armstrong, B.; Kelly, F.; Wilkinson, P. Air pollution and mortality benefits of the London Congestion Charge: Spatial and socioeconomic inequalities. Occup. Environ. Med. 2008, 65, 620–627. [Google Scholar] [CrossRef] [PubMed]
- Schulze-Fielitz, H. Brauchen wir eine Verordnung zur Lärmaktionsplanung? NuR 2009, 31, 87–93. [Google Scholar] [CrossRef]
- Mietlicki, F.; Mietlicki, C.; Ribeiro, C.; Gaudibert, P.; Vincent, B.; Gissinger, B. www.noiseineu.eu: New Tools to Inform the Public about Environmental Noise in Cities and to Assist Decision-Making. In Proceedings of the Euronoise Conference, Maastricht, The Netherlands, 31 May–3 June 2015; pp. 251–256. [Google Scholar]
- Schiewe, J.; Weninger, B.; Kornfeld, A.L. Forschungsprojekt OptiLAP—Evaluierung und Optimierung der Lärmaktionsplanung nach der Umgebungslärmrichtlinie 2002/49/EG. Arbeitspaket 2.1 Analyse und Verbesserung der Gebrauchstauglichkeit von Lärmkarten in der Öffentlichkeitsbeteiligung; Umweltbundesamt: Dessau-Roßlau, Germany, 2012. [Google Scholar]
- Luzzi, S.; Bellomini, R.; Natale, R.; Bartalucci, C.; Borchi, F.; Carfagni, M.; Governi, L. Importance of public participation in END implementation: Some experiences from Italian agglomerates and infrastructures. In Proceedings of the Euronoise Conference, Hamburg, Germany, 21–24 August 2016; pp. 1248–1255. [Google Scholar]
- Supplies, T.; Elsässer, R.; Mothes, F. Lärmminderung durch Bürgerbeteiligung Das Modellprojekt: Mach's—Mitwirken bei der Lärmaktionsplanung in Leipzig; Umweltbundesamt: Dessau-Roßlau, Germany, 2013. [Google Scholar]
- Heinrichs, E.; Kumsteller, F.; Rath, S.; Seidel, P.; Gurok, S. Lärmbilanz 2015. In Wissenschaftlich-Technische Unterstützung bei der Datenberichterstattung zur Lärmaktionsplanung; Umweltbundesamt: Dessau-Roßlau, Germany, 2015. [Google Scholar]
- Märker, O.; Basedow, S.; Wessel, M.; Lindloff, C.; Kuhlmann, W.; Cremer, N. Elektronische Partizipation zur Lärmaktionsplanung in Essen. Essen-soll-Leiser-Werden.de; Stadt Essen, Zebralog: Essen, Germany, 2010. [Google Scholar]
- Köckler, H. Nur die Einladung reicht nicht. Teilhabe als Schlüssel umweltbezogener Gerechtigkeit. Politische Ökol. 2014, 32, 43–48. [Google Scholar]
- Lercher, P.; Pfeiffer, C.; Botteldooren, D.; Dekoninck, L. Traffic noise exposure, education, and annoyance: Longitudinal experiences from cross-sectional studies over time (1989–2004). In Proceedings of the Forum Acusticum, Budapest, Hungary, 29 August–2 September 2005; pp. 1795–1799. [Google Scholar]
- McLaren, L.; McIntyre, L.; Kirkpatrick, S. Rose’s population strategy of prevention need not increase social inequalities in health. Int. J. Epidemiol. 2010, 39, 372–377. [Google Scholar] [CrossRef] [PubMed]
- De Fur, P.L.; Evans, G.W.; Cohen Hubal, E.A.; Kyle, A.D.; Morello-Frosch, R.A.; Williams, D.R. Vulnerability as a function of individual and group resources in cumulative risk assessment. EHP 2007, 115, 817–824. [Google Scholar] [CrossRef] [PubMed]
- Köckler, H.; Hornberg, C. Vulnerabilität als Erklärungsmodell einer sozial differenzierten Debatte um Risiken und Chancen im Kontext von Umweltgerechtigkeit. In Umweltgerechtigkeit. Chancengleichheit bei Umwelt und Gesundheit: Konzepte, Datenlage und Handlungsperspektiven, 1st ed.; Bolte, G., Bunge, C., Hornberg, C., Köckler, H., Mielck, A., Eds.; Verlag Hans Huber: Bern, Switzerland, 2012; pp. 73–86. [Google Scholar]
- Kruize, H.; Droomers, M.; van Kamp, I.; Ruijsbroek, A. What causes environmental inequalities and related health effects? An analysis of evolving concepts. Int. J. Environ. Res. Public Health 2014, 11, 5807–5827. [Google Scholar] [CrossRef] [PubMed]
- Baxter, S.; Killoran, A.; Kelly, M.P.; Goyder, E. Synthesizing diverse evidence: The use of primary qualitative data analysis methods and logic models in public health reviews. Public Health 2010, 124, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.M.; Petticrew, M.; Rehfuess, E.; Armstrong, R.; Ueffing, E.; Baker, P.; Francis, D.; Tugwell, P. Using logic models to capture complexity in systematic reviews. Res. Synth. Methods 2011, 2, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Köckler, H. Vulnerabilität von Haushalten Gegenüber Ihrer Lokalen Umweltgute. Eine Analyse aus Planerischer Perspektive vor dem Hintergrund Umweltbezogener Gerechtigkeit; Habilitation University of Kassel: Kassel, Germany, in press.
- Köckler, H. MOVE: Ein Modell zur Analyse umweltbezogener Verfahrensgerechtigkeit. Umweltpsychologie 2011, 15, 93–113. [Google Scholar]
- Ursin, H.; Eriksen, H.R. The cognitive activation theory of stress. Psychoneuroendocrinology 2004, 9, 567–592. [Google Scholar] [CrossRef]
- Ursin, H.; Eriksen, H.R. Cognitive activation theory of stress (CATS). Neurosci. Biobehav. Rev. 2010, 34, 877–881. [Google Scholar] [CrossRef] [PubMed]
- Matthews, K.A.; Gallo, L.C.; Taylor, S.E. Are psychosocial factors mediators of socioeconomic status and health connections? A progress report and blueprint for the future. Ann. N. Y. Acad. Sci. 2010, 1186, 146–173. [Google Scholar] [CrossRef] [PubMed]
- Gallo, L.C.; Matthews, K.A. Understanding the association between socioeconomic status and physical health. Do negative emotions play a role? Psychol. Bull. 2003, 129, 10–51. [Google Scholar] [CrossRef] [PubMed]
- Gallo, L.C. The reserve capacity model as a framework for understanding psychosocial factors in health disparities. Appl. Psychol. Health Well-Being 2009, 1, 62–72. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Ajzen, I. Perceived behavioral control, self-efficacy, locus of control, and the theory of planned behavior1. J. Appl. Soc. Pyschol. 2002, 32, 665–683. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behavior. In Handbook of Theories of Social Psychology; Lange, P.A.M., Kruglanski, A.W., Higgins, E.T., Eds.; Sage: London, UK, 2012; Volume 1, pp. 438–459. [Google Scholar]
- Ajzen, I. The Theory of Planned Behavior. Available online: http://people.umass.edu/aizen/tpb.diag.html#null-link (accessed on 22 March 2017).
- Hobfoll, S.E. Conservation of Resources. A New Attempt at Conceptualizing Stress. Am. Psychol. 1989, 44, 513–524. [Google Scholar] [CrossRef] [PubMed]
- Hobfoll, S.E.; Jackson, A.P. Conservation of resources in community intervention. Am. J. Community Psychol. 1991, 19, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Hobfoll, S.E.; Jackson, A.P.; Hobfoll, I.; Pierce, C.; Young, S. The impact of communal-mastery versus self-mastery on emotional outcomes during stressful conditions: A prospective study of native American women. Am. J. Community Psychol. 2002, 30, 853–871. [Google Scholar] [CrossRef] [PubMed]
- Hiroto, D.S. Locus of control and learned helplessness. J. Exp. Psychol. 1974, 102, 187–193. [Google Scholar] [CrossRef]
- Job, R.F.S. The influence of subjective reactions to noise on health effects the noise. Environ. Int. 1996, 22, 93–104. [Google Scholar] [CrossRef]
- Evans, G.W. Environmental stress and health. In Handbook of Health Psychology, 1st ed.; Baum, A., Revenson, T.A., Singer, J.E., Eds.; Lawrence Erlbaum Associates Inc.: Nahwah, NJ, USA, 2001; pp. 365–385. [Google Scholar]
- Evans, G.W.; Cohen, S. Environmental stress. In Encyclopedia of Applied Psychology; Spielberger, C.D., Ed.; Elsevier Academic Press: Oxford, UK; Boston, MA, USA, 2004; pp. 815–824. [Google Scholar]
- Evans, G.W.; Stecker, R. Motivational consequences of environmental stress. J. Environ. Psychol. 2004, 24, 143–165. [Google Scholar] [CrossRef]
- Hiroto, D.S.; Seligman, M.E. Generality of learned helplessness in man. J. Personal. Soc. Psychol. 1975, 31, 311–327. [Google Scholar] [CrossRef]
- Abramson, L.Y.; Seligman, M.E.; Teasdale, J.D. Learned helplessness in humans. Critique and reformulation. J. Abnorm. Psychol. 1978, 87, 49–74. [Google Scholar] [CrossRef] [PubMed]
- Peterson, C.; Maier, S.F.; Seligman, M.E. Learned Helplessness. A Theory for the Age of Personal Control; Oxford University Press: New York, NY, USA, 1993. [Google Scholar]
- Peterson, C.; Park, C. Learned helplessness and explanatory style. In Advanced Personality; Barone, D.F., Hersen, M., van Hasselt, V.B., Eds.; Springer: Boston, MA, USA, 1998; pp. 287–310. [Google Scholar]
- Peterson, P.; Park, N. Explanatory style and emotion regulation. In Handbook of Emotion Regulation, 2nd ed.; Gross, J.J., Ed.; Guilford Press: London, UK, 2007; pp. 159–179. [Google Scholar]
- Campbell, J.M. Ambient stressors. Environ. Behav. 1983, 15, 355–380. [Google Scholar] [CrossRef]
- WHO Regional Office for Europe. Guidelines for Community Noise; World Health Organisation Regional Office for Europe: Geneva, Switzerland; Copenhagen, Denmark, 1999. [Google Scholar]
- Flade, A. Die sozialen Kosten des Verkehrs. In Handbuch Verkehrspolitik; Schöller, O., Canzler, W., Knie, A., Eds.; VS Verlag für Sozialwissenschaften: Wiesbaden, Germany, 2007; pp. 490–509. [Google Scholar]
- Claßen, T. Lärm macht krank—Gesundheitliche Wirkungen von Lärmbelastungen in den Städten. IzR 2013, 3, 223–234. [Google Scholar]
- Stallen, P.J.M. A theoretical framework for environmental noise annoyance. Noise Health 1999, 1, 69–80. [Google Scholar] [PubMed]
- Klæboe, R. Noise and health—Annoyance and Interference. In Encyclopedia of Environmental Health; Nriagu, J.O., Ed.; Elsevier Science: Amsterdam, The Netherlands; London, UK, 2011; pp. 152–163. [Google Scholar]
- Van Kamp, I. Coping with Noise and Its Health Consequences; The University of Groningen: Groningen, The Netherlands, 1990. [Google Scholar]
- Hatfield, J.; Job, R.; Soames, F.; Hede, A.J.; Carter, N.L.; Peploe, P.; Taylor, R.; Morrell, S. Human response to environmental noise: The role of perceived control. IJBM 2002, 9, 341–359. [Google Scholar] [CrossRef]
- Kroesen, M.; Molin, E.J.E.; van Wee, B. Testing a theory of aircraft noise annoyance. A structural equation analysis. JASA 2008, 123, 4250. [Google Scholar] [CrossRef] [PubMed]
- Schreckenberg, D.; Meis, M.; Kahl, C.; Peschel, C.; Eikmann, T. Aircraft noise and quality of life around Frankfurt airport. Int. J. Environ. Res. Public Health 2010, 7, 3382–3405. [Google Scholar] [CrossRef] [PubMed]
- Guski, R. Personal and social variables as co-determinants of noise annoyance. Noise Health 1999, 1, 45–56. [Google Scholar] [PubMed]
- Flindell, I.H.; Stallen, P.J.M. Non-acoustical factors in environmental noise. Noise Health 1999, 1, 11–16. [Google Scholar] [PubMed]
- Kroesen, M.; Molin, E.J.E.; van Wee, B. Determining the direction of causality between psychological factors and aircraft noise annoyance. Noise Health 2010, 12, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, H.R.; Ursin, H. Social inequalities in health: biological, cognitive and learning theory perspectives. Nor. Epidemiol. 2002, 12, 33–38. [Google Scholar] [CrossRef]
- Kristenson, M.; Eriksen, H.R.; Sluiter, J.K.; Starke, D.; Ursin, H. Psychobiological mechanisms of socioeconomic differences in health. Soc. Sci. Med. 2004, 58, 1511–1522. [Google Scholar] [CrossRef]
- Ree, E.; Odeen, M.; Eriksen, H.R.; Indahl, A.; Ihlebaek, C.; Hetland, J.; Harris, A. Subjective health complaints and self-rated health: Are expectancies more important than socioeconomic status and workload? IJBM 2014, 21, 411–420. [Google Scholar] [CrossRef] [PubMed]
- McEwen, B.S. Stress, Adaptation, and disease. allostasis and allostatic load. Ann. N. Y. Acad. Sci. 1998, 840, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Von Lindern, E.; Hartig, T.; Lercher, P. Traffic-related exposures, constrained restoration, and health in the residential context. Health Place 2016, 39, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Freudenberg, N.; Pastor, M.; Israel, B. Strengthening community capacity to participate in making decisions to reduce disproportionate environmental exposures. Am. J. Public Health 2011, 101, S123–S130. [Google Scholar] [CrossRef] [PubMed]
- Smith, A. The concept of noise sensitivity: Implications for noise control. Noise Health 2013, 5, 57–59. [Google Scholar]
- Miedema, H.M.E. Annoyance caused by environmental noise: Elements for evidence-based noise policies. J. Soc. Issues 2007, 63, 41–57. [Google Scholar] [CrossRef]
- Schreckenberg, D.; Griefahn, B.; Meis, M. The associations between noise sensitivity, reported physical and mental health, perceived environmental quality, and noise annoyance. Noise Health 2010, 12, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Leganger, A.; Kraft, P.; RØysamb, E. Perceived self-efficacy in health behaviour research. Conceptualisation, measurement and correlates. Psychol. Health 2000, 15, 51–69. [Google Scholar] [CrossRef]
- Steptoe, A.; Dockray, S.; Wardle, J. Positive affect and psychobiological processes relevant to health. J. Pers. 2009, 77, 1747–1776. [Google Scholar] [CrossRef] [PubMed]
- Ward, M.M. Sense of control and self-reported health in a population-based sample of older Americans: Assessment of potential confounding by affect, personality, and social support. IJBM 2013, 20, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Basner, M.; Babisch, W.; Davis, A.; Brink, M.; Clark, C.; Janssen, S.; Stansfeld, S. Auditory and non-auditory effects of noise on health. Lancet 2014, 383, 1325–1332. [Google Scholar] [CrossRef]
- Recio, A.; Linares, C.; Banegas, J.R.; Diaz, J. Road traffic noise effects on cardiovascular, respiratory, and metabolic health: An integrative model of biological mechanisms. Environ. Res. 2016, 146, 359–370. [Google Scholar] [CrossRef] [PubMed]
- Babisch, W. The noise/stress concept, risk assessment and research needs. Noise Health 2002, 4, 1–11. [Google Scholar] [PubMed]
- Babisch, W.; Pershagen, G.; Selander, J.; Houthuijs, D.; Breugelmans, O.; Cadum, E.; Vigna-Taglianti, F.; Katsouyanni, K.; Haralabidis, A.S.; Dimakopoulou, K.; et al. Noise annoyance—A modifier of the association between noise level and cardiovascular health? Sci. Total Environ. 2013, 452–453, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Brunner, E. Socioeconomic determinants of health: Stress and the biology of inequality. BMJ 1997, 314, 1472. [Google Scholar] [CrossRef] [PubMed]
- Brunner, E. Biology and health inequality. PLoS Biol. 2007, 5, 2449–2452. [Google Scholar] [CrossRef] [PubMed]
- Brunner, E.; Marmot, M. Social organization, stress, and health. In Social Determinants of Health; Marmot, M., Wilkinson, R.G., Eds.; Oxford University Press: Oxford, UK, 2006; pp. 6–30. [Google Scholar]
- McEwen, B.S.; Gianaros, P.J. Central role of the brain in stress and adaption: Links to socio-economic status, health, and disease. Ann. N. Y. Acad. Sci. 2010, 1186, 190–222. [Google Scholar] [CrossRef] [PubMed]
- Krieger, N. Epidemiology and the People's Health. Theory and Context; Oxford University Press: New York, NY, USA, 2011. [Google Scholar]
- Daniel, M.; Moore, S.; Kestens, Y. Framing the biosocial pathways underlying associations between place and cardiometabolic disease. Health Place 2008, 14, 117–132. [Google Scholar] [CrossRef] [PubMed]
- Odeen, M.; Westerlund, H.; Theorell, T.; Leineweber, C.; Eriksen, H.R.; Ursin, H. Expectancies, socioeconomic status, and self-rated health: Use of the simplified TOMCATS Questionnaire. IJBM 2013, 20, 242–251. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.E.; Seeman, T.E. Psychosocial resources and the SES-health relationship. Ann. N. Y. Acad. Sci. 1999, 896, 210–225. [Google Scholar] [CrossRef] [PubMed]
- Gee, G.C.; Payne-Sturges, D.C. Environmental health disparities: A framework integrating psychosocial and environmental concepts. EHP 2004, 112, 1645–1653. [Google Scholar] [CrossRef] [PubMed]
- Morello-Frosch, R.; Shenassa, E.D. The environmental “riskscape” and social inequality: Implications for explaining maternal and child health disparities. EHP 2006, 114, 1150–1153. [Google Scholar] [CrossRef] [PubMed]
- McEwen, B.S.; Tucker, P. Chemical biological pathways for chronic psychosocial stress and research opportunities to advance the consideration of stress in chemical risk assessment. Am. J. Public Health 2011, S1, S131–S139. [Google Scholar] [CrossRef] [PubMed]
- Van Gerven, P.W.M.; Vos, H.; van Boxtel, M.P.J.; Janssen, S.A.; Miedema, H.M.E. Annoyance from environmental noise across the lifespan. JASA 2009, 126, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Riedel, N.; Loerbroks, A.; Bolte, G.; Li, J. Do perceived job insecurity and annoyance due to air and noise pollution predict self-rated poor health? A prospective analysis of independent and joint associations using a German national representative cohort study. BMJ Open 2017, 23, e012815. [Google Scholar] [CrossRef] [PubMed]
- Babisch, W.; Swart, W.; Houthuijs, D.; Selander, J.; Bluhm, G.; Pershagen, G.; Dimakopoulou, K.; Haralabidis, A.S.; Katsouyanni, K.; Davou, E.; et al. Exposure modifiers of the relationships of transportation noise with high blood pressure and noise annoyance. JASA 2012, 132, 3788–3808. [Google Scholar] [CrossRef] [PubMed]
- Foraster, M.; Künzli, N.; Aguilera, I.; Rivera, M.; Agis, D.; Vila, J.; Bouso, L.; Deltell, A.; Marrugat, J.; Ramos, R.; et al. High blood pressure and long-term exposure to indoor noise and air pollution from road traffic. EHP 2014, 122, 1193–1200. [Google Scholar] [CrossRef] [PubMed]
- Forastiere, F.; Stafoggia, M.; Tasco, C.; Picciotto, S.; Agabiti, N.; Cesaroni, G.; Perucci, C.A. Socioeconomic status, particulate air pollution, and daily mortality: Differential exposure or differential susceptibility. Am. J. Ind. Med. 2007, 50, 208–216. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.; Schulte-Fortkamp, B. Soundscape and the Built Environment; CRC Press, Taylor & Francis Group: Abdington, UK, 2016. [Google Scholar]
- de Kluizenaar, Y.; Salomons, E.M.; Janssen, S.A.; van Lenthe, F.J.; Vos, H.; Zhou, H.; Miedema, H.M.E.; Mackenbach, J.P. Urban road traffic noise and annoyance: The effect of a quiet façade. JASA 2011, 130, 1936–1942. [Google Scholar] [CrossRef] [PubMed]
- Gidlöf-Gunnarsson, A.; Öhrström, E. Noise and well-being in urban residential environments: The potential role of perceived availability to nearby green areas. Landsc. Urban Plan. 2007, 83, 115–126. [Google Scholar] [CrossRef]
- Gidlöf-Gunnarsson, A.; Öhrström, E. Attractive “quiet” courtyards: A potential modifier of urban residents’ responses to road traffic noise? Int. J. Environ. Res. Public Health 2010, 9, 3359–3375. [Google Scholar] [CrossRef] [PubMed]
- Dzhambov, A.M.; Dimitrova, D.D. Urban green spaces’ effectiveness as a psychological buffer for the negative health impact of noise pollution: A systematic review. Noise Health 2014, 16, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Claßen, T.; Jäcker-Cüppers, M.; Riedel, N. Weniger Lärm. In Ökosystemleistungen in der Stadt Gesundheit schützen und Lebensqualität erhöhen. Stadtbericht. Naturkapital Deutschland—TEEB DE; Kowarik, I., Bartz, R., Brenck, M., Eds.; Technische Universität: Berlin, Germany; Helmholtz-Zentrum für Umweltforschung: Leipzig, Germany, 2016; pp. 80–85. [Google Scholar]
- Van Kamp, I.; Klaeboe, R.; Brown, A.L.; Lercher, P. Soundscapes, human restoration and quality of life. In Soundscape and the Built Environment; Kang, J., Schulte-Fortkamp, B., Eds.; CRC Press, Taylor & Francis Group: Abdington, UK, 2016; pp. 43–68. [Google Scholar]
- Musterd, S.; Murie, A.; Kesteloot, C. Neighbourhoods of Poverty. Urban Social Exclusion and Integration in Comparison; Palgrave Macmillan: Basingstoke, UK, 2006. [Google Scholar]
- Bernard, P.; Charafeddine, R.; Frohlich, K.L.; Daniel, M.; Kestens, Y.; Potvin, L. Health inequalities and place: A theoretical conception of neighbourhood. Soc. Sci. Med. 2007, 65, 839–852. [Google Scholar] [CrossRef] [PubMed]
- Riedel, N.; Fuks, K.; Hoffmann, B.; Weyers, S.; Siegrist, J.; Erbel, R.; Viehmann, A.; Stang, A.; Scheiner, J.; Dragano, N. Insomnia and urban neighbourhood contexts—Are associations modified by individual social characteristics and change of residence? Results from a population-based study using residential histories. BMC Public Health 2012, 12, 810. [Google Scholar] [CrossRef] [PubMed]
- QUADMAP QUiet Areas Definition and Management in Action Plans Project Group. Guidelines for the Identification, Selection, Analysis, and Management of Quiet Urban Areas, Update Version 2.0 March 2015. Available online: http://www.quadmap.eu/wp-content/uploads/2012/01/Guidelines_QUADMAP_ver2.0.pdf (accessed on 22 March 2017).
- Zimmerman, M.A. Toward a theory of learned hopefulness: A structural model analysis of participation and empowerment. J. Res. Pers. 1990, 24, 71–86. [Google Scholar] [CrossRef]
- Lercher, P. Environmental noise: A contextual health perspective. In Noise and its Effects; Luxon, L.M., Deepak, P., Eds.; Wiley: London, UK, 2007; pp. 345–377. [Google Scholar]
- Umweltbundesamt. Verkehr in Zahlen 2012. Available online: http://www.umweltbundesamt.de/sites/default/files/medien/publikation/long/4364.pdf (accessed on 22 March 2017).
- European Commission. White Paper 2011. Roadmap to a Single European Transport Area—Towards a Competitive and Resource Efficient Transport System. Available online: http://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:52011DC0144&from=EN (accessed on 22 March 2017).
- European Commission. EU Transport in Figures. Statistical Pocketbook 2016. Available online: https://ec.europa.eu/transport/facts-fundings/statistics/pocketbook-2016_en (accessed on 22 March 2017).
- Riedel, N.; Köckler, H.; Scheiner, J.; Berger, K. Residential road traffic exposure, noise annoyance, and self-rated poor health—A proposal for an analytical concept framing the relationship between noise and health as a matter of multiple stressors and resources in urban neighbourhoods. J. Environ. Plan. Manag. 2015, 58, 336–356. [Google Scholar] [CrossRef]
- Lercher, P.; van Kamp, I.; von Lindern, E. Transportation noise and health-related quality of life: Perceptions of soundscapes, coping, and restoration. In Proceedings of the EuroNoise 2015, Maastricht, The Netherlands, 31 May–3 June 2015; pp. 803–808. [Google Scholar]
- Shepherd, D.; Heinonen-Guzejev, M.; Heikkila, K.M.; Dirks, K.N.; Hautus, M.J.; Welch, D.; McBride, D. The negative affect hypothesis of noise sensitivity. Int. J. Environ. Res. Public Health 2015, 12, 5284–5303. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Determinant | High Controllability x Low Personal Importance (Group 1) | High Controllability x High Personal Importance (Group 2) | Low Controllability x Low Personal Importance (Group 3) | Low Controllability x High Personal Importance (Group 4) | ||
|---|---|---|---|---|---|---|
| noise annoyance | low | moderate | moderate | high | ||
| noise sensitivity | low | high | low | high | ||
| A | B | - | - | A | B | |
| generalised outcome expectancy | positive | no control | positive | no control | negative | positive |
| negative affect | low | high | low | high | high | low |
| positive affect | high | low | high | low | low | high |
| positive expectancies of institutional coping (civic engagement) | moderate | low | high | low | low | high |
| disengagement (cognitive distortion) | moderate | high | low | high | high | low |
| physiological activation 1 | low | moderate | moderate | moderate | high | moderate |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riedel, N.; Van Kamp, I.; Köckler, H.; Scheiner, J.; Loerbroks, A.; Claßen, T.; Bolte, G. Cognitive-Motivational Determinants of Residents’ Civic Engagement and Health (Inequities) in the Context of Noise Action Planning: A Conceptual Model. Int. J. Environ. Res. Public Health 2017, 14, 578. https://doi.org/10.3390/ijerph14060578
Riedel N, Van Kamp I, Köckler H, Scheiner J, Loerbroks A, Claßen T, Bolte G. Cognitive-Motivational Determinants of Residents’ Civic Engagement and Health (Inequities) in the Context of Noise Action Planning: A Conceptual Model. International Journal of Environmental Research and Public Health. 2017; 14(6):578. https://doi.org/10.3390/ijerph14060578
Chicago/Turabian StyleRiedel, Natalie, Irene Van Kamp, Heike Köckler, Joachim Scheiner, Adrian Loerbroks, Thomas Claßen, and Gabriele Bolte. 2017. "Cognitive-Motivational Determinants of Residents’ Civic Engagement and Health (Inequities) in the Context of Noise Action Planning: A Conceptual Model" International Journal of Environmental Research and Public Health 14, no. 6: 578. https://doi.org/10.3390/ijerph14060578