
Early Childhood Dental Caries, Mouth Pain, and Malnutrition in the Ecuadorian Amazon Region

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
2.2. Measures
2.3. Data Analysis
3. Results
3.1. Demographics
3.2. Oral Health and Nutrition Measures
3.3. Child Mouth Pain and Severe Caries
3.4. Child Mouth Pain and Malnutrition
4. Discussion
4.1. Prevalence of Caries and Mouth Pain
4.2. Prevalence of Malnutrition
4.3. Child Mouth Pain and Malnutrition
4.4. Implications for Addressing Oral Health and Malnutrition in Indigenous Communities
4.5. Strengths and Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Popkin, B.M. The nutrition transition in low-income countries: An emerging crisis. Nutr. Rev. 1994, 52, 285–298. [Google Scholar] [CrossRef] [PubMed]
- Petersen, P.E.; Bourgeois, D.; Ogawa, H.; Estupinan-Day, S.; Ndiaye, C. The global burden of oral disease and risks to oral health. Bull. World Health Organ. 2005, 83, 661–669. [Google Scholar] [PubMed]
- Malik, V.S.; Willett, W.C.; Hu, F.B. Global obesity: Trends, risk factors and policy implications. Nat. Rev. Endocrinol. 2013, 9, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Children: Reducing mortality. Fact Sheet 178. Available online: http://www.who.int/mediacentre/factsheets/fs178/en/ (accessed on 25 September 2016).
- Black, R.E.; Allen, L.H.; Bhutta, Z.A.; Caulfield, L.E.; de Onis, M.; Ezzati, M.; Mathers, C.; Rivera, J. Maternal and child undernutrition: Global and regional exposures and health consequences. Lancet 2008, 371, 243–260. [Google Scholar] [CrossRef]
- Penafiel, D.; Termote, C.; Lachat, C.; Espinel, R.; Kolsteren, P.; Van Damme, P. Barriers to eating traditional foods vary by age group in Ecuador with biodiversity loss as a key issue. J. Nutr. Educ. Behav. 2016, 48, 258–268. [Google Scholar] [CrossRef] [PubMed]
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Daar, A.S.; Singer, P.A.; Leah Persad, D.; Pramming, S.K.; Matthews, D.R.; Beaglehole, R.; Bernstein, A.; Borysiewicz, L.K.; Colagiuri, S.; Ganguly, N.; et al. Grand challenges in chronic non-communicable diseases. Nat. Publ. Gr. 2007, 450, 20–23. [Google Scholar] [CrossRef] [PubMed]
- Blinkhorn, A.S.; Davies, R.M. Caries prevention. A continued need worldwide. Int. Dent. J. 1996, 46, 119–125. [Google Scholar] [PubMed]
- Marcenes, W.; Kassebaum, N.J.; Bernabé, E.; Flaxman, A.; Naghavi, M.; Lopez, A.; Murray, C.J. Global burden of oral conditions in 1990–2010: A systematic analysis. J. Dent. Res. 2013, 92, 592–597. [Google Scholar] [CrossRef] [PubMed]
- Alm, A.; Wendt, L.K.; Koch, G.; Birkhed, D.; Nilsson, M. Caries in adolescence—Influence from early childhood. Community Dent. Oral Epidemiol. 2012, 40, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Mobley, C.C. Nutrition and dental caries. Dent. Clin. N. Am. 2003, 47, 319–336. [Google Scholar] [CrossRef]
- Khanh, L.N.; Ivey, S.L.; Sokal-Gutierrez, K.; Barkan, H.; Ngo, K.M.; Hoang, H.T.; Vuong, I.; Thai, N. Early childhood caries, mouth pain, and nutritional threats in Vietnam. Am. J. Public Health 2015, 105, 2510–2517. [Google Scholar] [CrossRef] [PubMed]
- Fisher-Owens, S.A.; Gansky, S.A.; Platt, L.J.; Weintraub, J.A.; Soobader, M.J.; Bramlett, M.D.; Newacheck, P.W. Influences on children’s oral health: A conceptual model. Pediatrics 2007, 120, e510–e520. [Google Scholar] [CrossRef] [PubMed]
- Sheiham, A. Oral health, general health and quality of life. Bull. World Health Organ. 2005, 83, 644. [Google Scholar] [PubMed]
- Vania, A.; Parisella, V.; Capasso, F.; Di Tanna, G.L.; Vestri, A.; Ferrari, M.; Polimeni, A. Early childhood caries underweight or overweight, that is the question. Eur. J. Paediatr. Dent. 2011, 12, 231–235. [Google Scholar] [PubMed]
- Walker, I.; Marini, A.; Lucchetti, L.; Waters, W.; Lapstra, A. Nutritional Failure in Ecuador: Causes Consequences and Solutions. 2007. Available online: http://www.popline.org/node/191935 (accessed on 25 September 2016).
- Bönecker, M.; Cleaton-Jones, P. Trends in dental caries in Latin American and Caribbean 5–6- and 11–13-year-old children: A systematic review. Community Dent. Oral Epidemiol. 2003, 31, 152–157. [Google Scholar] [CrossRef] [PubMed]
- De Onis, M.; Blössner, M.; Borghi, E. Prevalence and trends of stunting among pre-school children, 1990–2020. Public Health Nutr. 2012, 15, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Lutter, C.; Chaparro, C. Malnutrition in Infants and Young Children in Latin America and the Caribbean: Achieving the and Millennium Development Goals. Available online: http://iris.paho.org/xmlui/bitstream/handle/123456789/18641/9789275129289_eng.pdf?sequence=1&isAllowed=y (accessed on 25 September 2016).
- Pan, W.K.Y.; Erlien, C.; Bilsborrow, R.E. Morbidity and mortality disparities among colonist and indigenous populations in the Ecuadorian Amazon. Soc. Sci. Med. 2010, 70, 401–411. [Google Scholar]
- Sokal-Gutierrez, K.; Turton, B.; Husby, H.; Paz, C.L. Early childhood caries and malnutrition: Baseline and two-year follow-up results of a community-based prevention intervention in rural Ecuador. BMC Nutr. 2016, 2, 73. [Google Scholar] [CrossRef]
- Alkarimi, H.A.; Watt, R.G.; Pikhart, H.; Sheiham, A.; Tsakos, G. Dental caries and growth in school-age children. Pediatrics 2014, 133, e616–e623. [Google Scholar] [CrossRef] [PubMed]
- Sheiham, A.; Watt, R.G. The common risk factor approach: A rational basis for promoting oral health. Community Dent. Oral Epidemiol. 2000, 28, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.; Blinkhorn, A.; Irving, M. Oral Health Programmes in Indigenous Communities Worldwide-Lessons learned from the field: A qualitative systematic review. Community Dent. Oral Epidemiol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Available online: http://www.who.int/oral_health/publications/9789241548649/en/ (accessed on 25 September 2016).
- Drury, T.F.; Horowitz, A.M.; Ismail, A.I.; Maertens, M.P.; Rozier, R.G.; Selwitz, R.H. Diagnosing and reporting early childhood caries for research purposes. J. Public Health Dent. 1999, 59, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Cypriano, S.; de Sousa, M.L.R.; Wada, R.S. Avaliação de índices CPOD simplificados em levantamentos epidemiológicos de cárie dentária. Rev. Saude Publica 2005, 39, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Ismail, A.I.; Sohn, W.; Tellez, M.; Amaya, M.; Sen, A.; Hasson, H.; Pitts, N.B. The international caries detection and assessment system (ICDAS): An integrated system for measuring dental caries: Methods. Community Dent. Oral Epidemiol. 2007, 35, 170–178. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization; United Nations Children’s Fund. WHO Child Growth Standards and the Identification of Severe Acute Malnutrition in Infants and Children: A Joint Statement. 2009. Available online: http://www.who.int/nutrition/publications/severemalnutrition/9789241598163/en/ (accessed on 7 March 2017).
- Clementino, M.A.; Gomes, M.C.; de Pinto-Sarmento, A.T.C.; Martins, C.C.; Granville-Garcia, A.F.; Paiva, S.M. Perceived impact of dental pain on the quality of life of preschool children and their families. PLoS ONE 2015, 10, e0130602. [Google Scholar] [CrossRef] [PubMed]
- Pahel, B.; Rozier, R.G.; Slade, G. Parental perceptions of children’s oral health: The early childhood oral health impact scale (ECOHIS). Health Qual. Life Outcomes 2007, 5, 6. [Google Scholar] [CrossRef] [PubMed]
- Galobardes, B.; Shaw, M.; Lawlor, D.A.; Lynch, J.W.; Davey Smith, G. Indicators of socioeconomic position (part 1). J. Epidemiol. Community Health 2006, 60, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Medina, W.; Hurtig, A.K.; San Sebastián, M.; Quizhpe, E.; Romero, C. Dental caries in 6–12-year-old indigenous and non-indigenous schoolchildren in the Amazon basin of Ecuador. Braz. Dent. J. 2008, 19, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Beltrán-Aguilar, E.D.; Estupiñán-Day, S.; Báez, R. Analysis of prevalence and trends of dental caries in the Americas between the 1970s and 1990s. Int. Dent. J. 1999, 49, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Abanto, J.; Carvalho, T.S.; Mendes, F.M.; Wanderley, M.T.; Bönecker, M.; Raggio, D.P. Impact of oral diseases and disorders on oral health-related quality of life of preschool children. Community Dent. Oral Epidemiol. 2011, 39, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Chambers, C.; Reid, C.; Craig, K.; McGrath, P.; Finley, G. Agreement between child and parent reports of pain. Clin. J. Pain 1998, 14, 336–342. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Global Database on Child Growth and Malnutrition: 2001–2005. Available online: http://www.who.int/nutgrowthdb/en/ (accessed on 25 September 2016).
- Houck, K.; Sorensen, M.V.; Lu, F.; Alban, D.; Alvarez, K.; Hidobro, D.; Doljanin, C.; Ona, A.I. The effects of market integration on childhood growth and nutritional status: The dual burden of under- and over-nutrition in the northern Ecuadorian Amazon. Am. J. Hum. Biol. 2013, 25, 524–533. [Google Scholar] [CrossRef] [PubMed]
- Aldabal, L.; Bahammam, A.S. Metabolic, endocrine, and immune consequences of sleep deprivation. Open Respir. Med. J. 2011, 5, 31–43. [Google Scholar] [CrossRef] [PubMed]
- Alkarimi, H.A.; Watt, R.G.; Pikhart, H.; Jawadi, A.H.; Sheiham, A.; Tsakos, G. Impact of treating dental caries on schoolchildren’s anthropometric, dental, satisfaction and appetite outcomes: A randomized controlled trial. BMC Public Health 2012, 12, 706. [Google Scholar] [CrossRef] [PubMed]
- Estupiñán-Day, S. Promoting Oral Health: The Use of Salt Fluoridation to Prevent Dental Caries; Pan American Health Organization: Washington, DC, USA, 2005. [Google Scholar]
- Gussy, M.G.; Waters, E.G.; Walsh, O.; Kilpatrick, N.M. Early childhood caries: Current evidence for aetiology and prevention. J. Paediatr. Child Health 2006, 42, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Van Gemert-Schriks, M.C.M.; van Amerongen, E.W.; Aartman, I.H.A.; Wennink, J.M.B.; ten Cate, J.M.; de Soet, J.J. The influence of dental caries on body growth in prepubertal children. Clin. Oral Investig. 2011, 15, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Bhutta, Z.A.; Ahmed, T.; Black, R.E.; Cousens, S.; Dewey, K.; Giugliani, E.; Haider, B.A.; Kirkwood, B.; Morris, S.S.; Sachdev, H.P.S.; et al. What works? Interventions for maternal and child undernutrition and survival. Lancet 2008, 371, 417–440. [Google Scholar] [CrossRef]
- Slade, G.D.; Bailie, R.S.; Roberts-Thomson, K.; Leach, A.J.; Raye, I.; Endean, C.; Simmons, B.; Morris, P. Effect of health promotion and fluoride varnish on dental caries among Australian Aboriginal children: Results from a community-randomized controlled trial. Community Dent. Oral Epidemiol. 2011, 39, 29–43. [Google Scholar] [CrossRef] [PubMed]
- Stinson, J.N.; Kavanagh, T.; Yamada, J.; Gill, N.; Stevens, B. Systematic review of the psychometric properties, interpretability and feasibility of self-report pain intensity measures for use in clinical trials in children and adolescents. Pain 2006, 125, 143–157. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristic | 2011 (N = 731) | 2012 (N = 373) | 2013 (N = 305) | Total |
|---|---|---|---|---|
| Demographics | ||||
| Maternal Age, Mean Years (SD) | 30.0 (10.3) | 30.3 (8.8) | 30.0 (8.6) | 30.1 |
| Maternal Education, Mean Years Completed (SD) | 6.9 (4.93) | 8.4 (3.9) | 9.3 (3.7) | 8.2 |
| Number of People per Household, Mean (SD) | 7.0 (2.96) | 6.7 (2.8) | 6.5 (2.9) | 6.7 |
| Families Cooking with Wood Only a, % | 13.4 | 12.3 | 12.2 | 12.6 |
| Number of Children per Mother, Mean (SD) | 3.6 (2.6) | 3.7 (2.4) | 3.6 (2.3) | 3.7 |
| Child Age, % | ||||
| 0–2 Years | 15.5 | 17.6 | 18.3 | 17.1 |
| 3–6 Years | 84.6 | 82.4 | 81.7 | 82.9 |
| Child Sex, % | ||||
| Male | 50.5 | 48.3 | 50.1 | 49.6 |
| Female | 49.5 | 51.7 | 49.9 | 50.4 |
| Child Oral Health and Oral Health Practices | ||||
| Caries Prevalence by dmft Score b, % | ||||
| Dmft ≥ 1 | 73.9 | 63.0 | 59.3 | 65.4 |
| D2 or D3 | 47.5 | 41.3 | 45.2 | 44.7 |
| D3 | 39.9 | 32.6 | 30.5 | 34.3 |
| Parent-Reported Mouth Pain by Type, % | ||||
| No Mouth Pain | 57.1 | 63.4 | 66.3 | 62.3 |
| Any Mouth Pain | 42.9 | 36.6 | 33.7 | 37.7 |
| Mouth Pain Interfering with Eating | 33.2 | 26.6 | 23.6 | 27.8 |
| Mouth Pain Interfering with Sleeping | 27.5 | 24.6 | 16.1 | 22.8 |
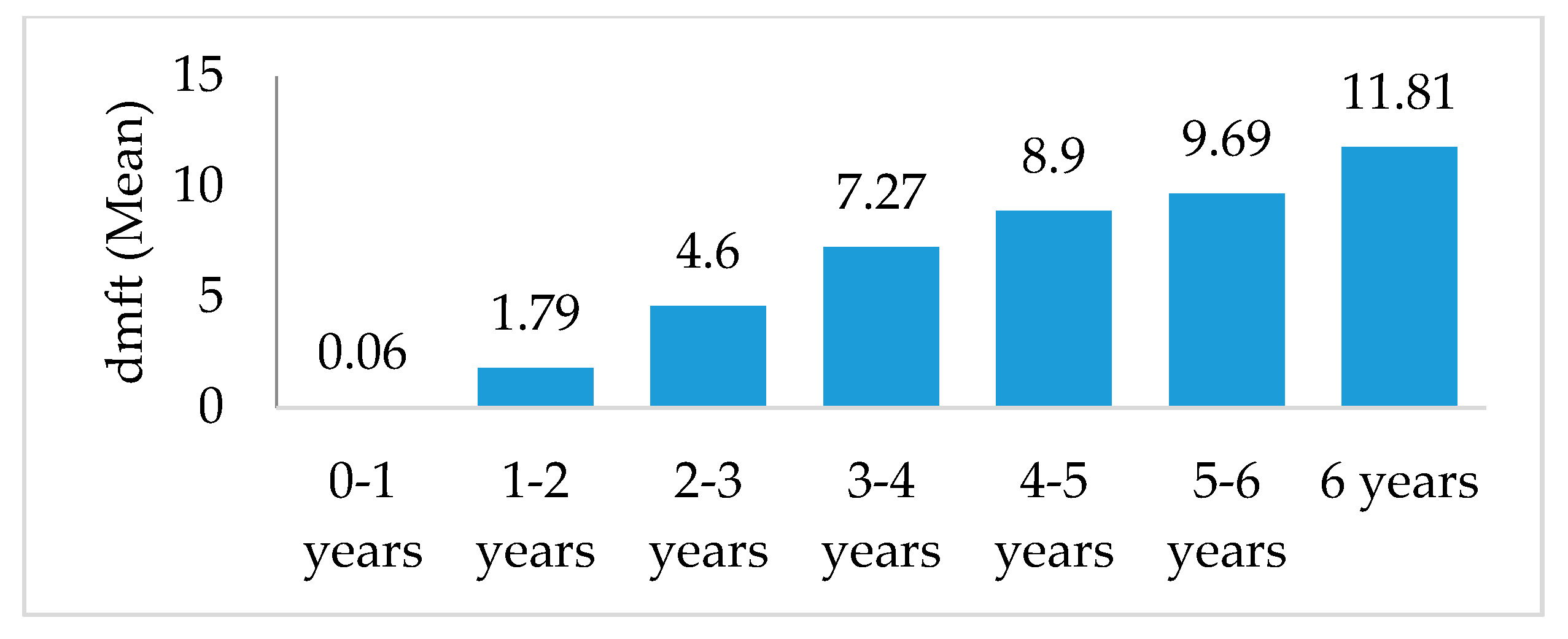
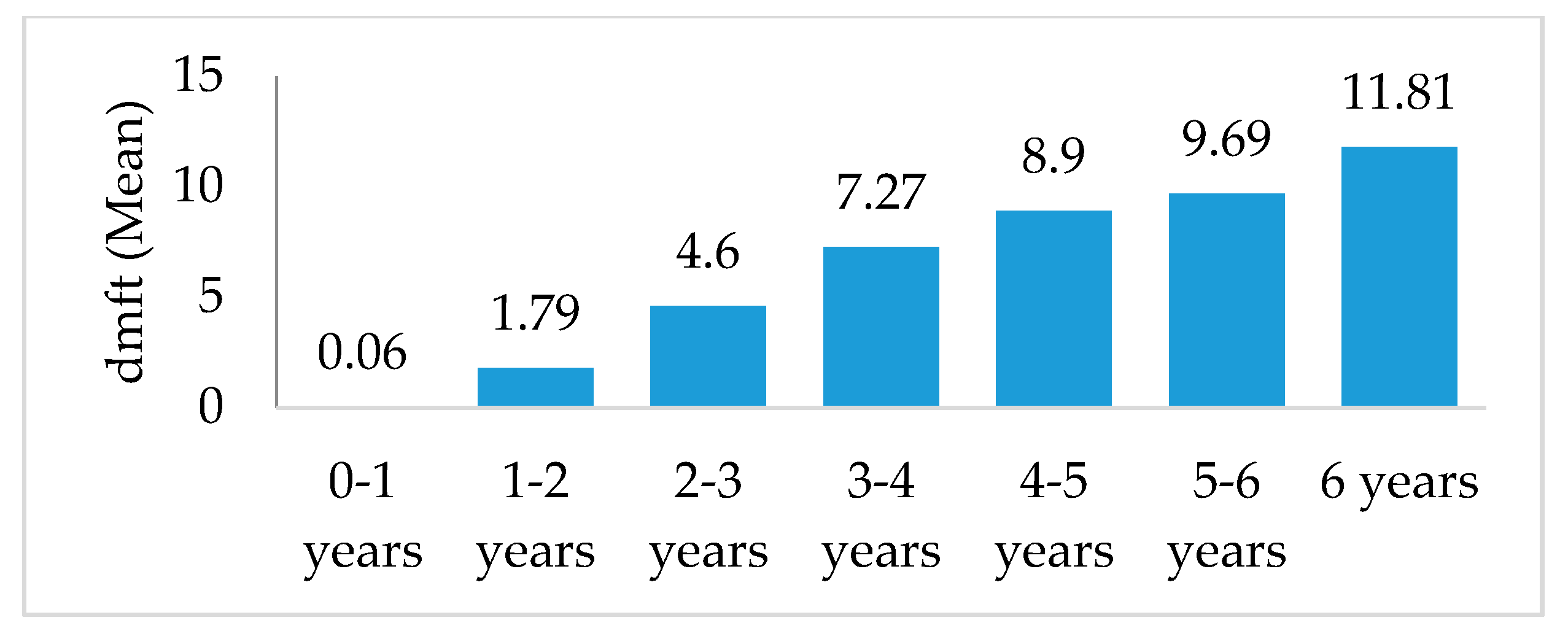
| Number of decayed, missing and filled teeth (dmft), Mean (SD) | ||||
| 0–1 years | 0.0 (0.3) | 0.1 (0.3) | 0.1 (0.3) | 0.1 |
| 1–2 years | 1.7 (2.8) | 1.7 (2.8) | 2.0 (2.8) | 1.8 |
| 2–3 years | 4.5 (4.3) | 4.7 (4.3) | 4.6 (4.3) | 4.6 |
| 3–4 years | 7.2 (4.7) | 7.3 (4.7) | 7.3 (4.7) | 7.3 |
| 4–5 years | 8.9 (4.7) | 8.8 (4.7) | 9.0 (4.7) | 8.9 |
| 5–6 years | 9.5 (4.3) | 9.0 (4.3) | 10.6 (4.3) | 9.7 |
| 6 years | 11.2 (5.2) | 12.0 (5.1) | 12.2 (5.2) | 11.8 |
| Mothers Help with Child Toothbrushing, % | 54.9 | 53.5 | 51.1 | 51.8 |
| Child Ever Been to the Dentist, % | 52.0 | 47.4 | 47.8 | 49.1 |
| Child Nutrition and Nutrition Practices | ||||
| Prevalence of Malnutrition by Type c, % | ||||
| Shortness/Stunting (HAZ < −2 SD) | 35.8 | 34.1 | 37.8 | 35.9 |
| Wasting/Thinness (WHZ < −2 SD) | 1.5 | 1.1 | 0.7 | 1.1 |
| Underweight (WAZ < −2 SD) | 8.2 | 6.8 | 7.4 | 7.4 |
| Overweight (WHZ > +2 SD) | 5.6 | 11.7 | 3.1 | 6.8 |
| Junk Food Consumption Frequency d, % | ||||
| Every 2–4 Weeks | 32.8 | 50.0 | 48.7 | 43.8 |
| At Least Once a Week | 58.9 | 55.0 | 43.6 | 52.5 |
| At Least Once a Day | 36.2 | 23.5 | 22.5 | 27.4 |
| Child was Ever Breastfed, % | 95.8 | 98.9 | 95.2 | 97.7 |
| Child was Ever Bottlefed, % | 40.3 | 41.6 | 37.4 | 39.0 |
| What Child Drank in Baby Bottle e, % | ||||
| Milk or Formula | 39.9 | 39.7 | 52.1 | 43.2 |
| Water | 20.8 | 15.5 | 10.8 | 16.5 |
| Sugar-Sweetened Beverage | 28.5 | 29.6 | 32.2 | 29.1 |
| Child Slept with Bottle f, % | ||||
| Never | 77.0 | 57.3 | 64.7 | 71.3 |
| Sometimes | 16.1 | 28.2 | 18.7 | 19.5 |
| Frequently or Almost Always | 6.9 | 14.6 | 10.6 | 9.1 |
| Age Category | Any Mouth Pain (N = 476) | Mouth Pain Interfering with Eating (N = 378) | Mouth Pain Interfering with Sleeping (N = 303) | |||
|---|---|---|---|---|---|---|
| N (%) | AOR (95% CI) | N (%) | AOR (95% CI) | N (%) | AOR (95% CI) | |
| All | 329 | 2.59 ** (2.04–3.27) | 206 | 2.23 ** (1.86–2.65) | 162 | 1.92 ** (1.53–2.29) |
| 0–2 year olds | 74 (22.5) | 2.52 (1.68–3.31) | 46 (22.3) | 1.40 (1.02–1.94) | 36 (22.2) | 1.58 (1.16–1.84) |
| 3–6 year olds | 255 (77.5) | 2.77 ** (2.30–3.18) | 160 (77.7) | 2.08 * (1.67–2.59) | 126 (77.8) | 2.07 ** (1.74–2.42) |
| Measure of Malnutrition | Any Mouth Pain (N = 476) | Mouth Pain Interfering with Eating (N = 378) | Mouth Pain Interfering with Sleeping (N = 303) | |||
|---|---|---|---|---|---|---|
| N (%) | AOR (95% CI) | N (%) | AOR (95% CI) | N (%) | AOR (95% CI) | |
| Stunting/Shortness Height-for-Age z ≤ −2 | 256 | 0.97 (0.67–1.24) | 207 | 0.94 (0.65–1.23) | 165 | 0.88 (0.62–1.12) |
| 0–2 year olds | 42 (16.4) | 1.15 (0.87–1.32) | 34 (16.4) | 1.09 (0.87–1.30) | 28 (17.0) | 1.12 (0.86–1.36) |
| 3–6 year olds | 212 (82.8) | 0.96 (0.73–1.12) | 183 (88.4) | 0.93 (0.72–1.14) | 137 (83.0) | 0.85 (0.61–1.05) |
| Wasting/Thinness Weight-for-Height z ≤ −2 | 27 | 0.86 (0.59–1.05) | 28 | 0.63 (0.43–0.82) | 21 | 1.13 (0.84–1.32) |
| 0–2 year olds | 6 (22.2) | 0.93 (0.68–1.22) | 6 (21.4) | 0.82 (0.52–1.02) | 4 (19.0) | 1.47 (1.06–1.72) |
| 3–6 year olds | 21 (80.8) | 0.66 (0.43–0.81) | 22 (78.6) | N/A | 17 (81.0) | N/A |
| Under-weight Weight-for-Age z ≤ −2 | 106 | 1.08 (0.94–1.20) | 87 | 0.96 (0.72–1.15) | 73 | 1.27 ** (1.02–1.54) |
| 0–2 year olds | 22 (20.8) | 1.54 (1.21–1.79) | 20 (23.0) | 1.02 (0.84–1.13) | 19 (26.0) | 1.10 (0.91–1.32) |
| 3–6 year olds | 84 (78.5) | 0.95 (0.77–1.11) | 67 (77.0) | 0.77 (0.53–0.95) | 54 (74.0) | 1.45 ** (1.24–1.66) |
| Over-weight Weight-for-Height z ≥ 2 | 87 | 1.06 (0.87–1.32) | 56 | 1.10 (0.84–1.32) | 44 | 0.76 * (0.58–0.97) |
| 0–2 year olds | 23 (26.4) | 1.19 (0.87–1.32) | 11 (19.6) | 1.12 (0.82–1.32) | 8 (18.2) | 1.03 (0.67–1.37) |
| 3–6 year olds | 64 (73.6) | 1.06 (0.72–1.38) | 45 (80.4) | 1.18 (0.86–1.34) | 36 (81.8) | 0.78 ** (0.67–0.94) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
So, M.; Ellenikiotis, Y.A.; Husby, H.M.; Paz, C.L.; Seymour, B.; Sokal-Gutierrez, K. Early Childhood Dental Caries, Mouth Pain, and Malnutrition in the Ecuadorian Amazon Region. Int. J. Environ. Res. Public Health 2017, 14, 550. https://doi.org/10.3390/ijerph14050550
So M, Ellenikiotis YA, Husby HM, Paz CL, Seymour B, Sokal-Gutierrez K. Early Childhood Dental Caries, Mouth Pain, and Malnutrition in the Ecuadorian Amazon Region. International Journal of Environmental Research and Public Health. 2017; 14(5):550. https://doi.org/10.3390/ijerph14050550
Chicago/Turabian StyleSo, Marvin, Yianni A. Ellenikiotis, Hannah M. Husby, Cecilia Leonor Paz, Brittany Seymour, and Karen Sokal-Gutierrez. 2017. "Early Childhood Dental Caries, Mouth Pain, and Malnutrition in the Ecuadorian Amazon Region" International Journal of Environmental Research and Public Health 14, no. 5: 550. https://doi.org/10.3390/ijerph14050550