Improving Pool Fencing Legislation in Queensland, Australia: Attitudes and Impact on Child Drowning Fatalities


Abstract
:1. Introduction
2. Materials and Methods
2.1. 2011 CATI Survey
2.2. Royal Life Saving National Fatal Drowning Database (the Database)
2.3. Data Analysis
2.4. Ethics Approval
3. Results
3.1. CATI Survey
3.1.1. Home Pool Ownership Chi Square Analysis
3.1.2. Home Pool Ownership Logistic Regression
3.1.3. Pool Fencing Legislation Effectiveness Chi Square and Logistic Regression Analysis
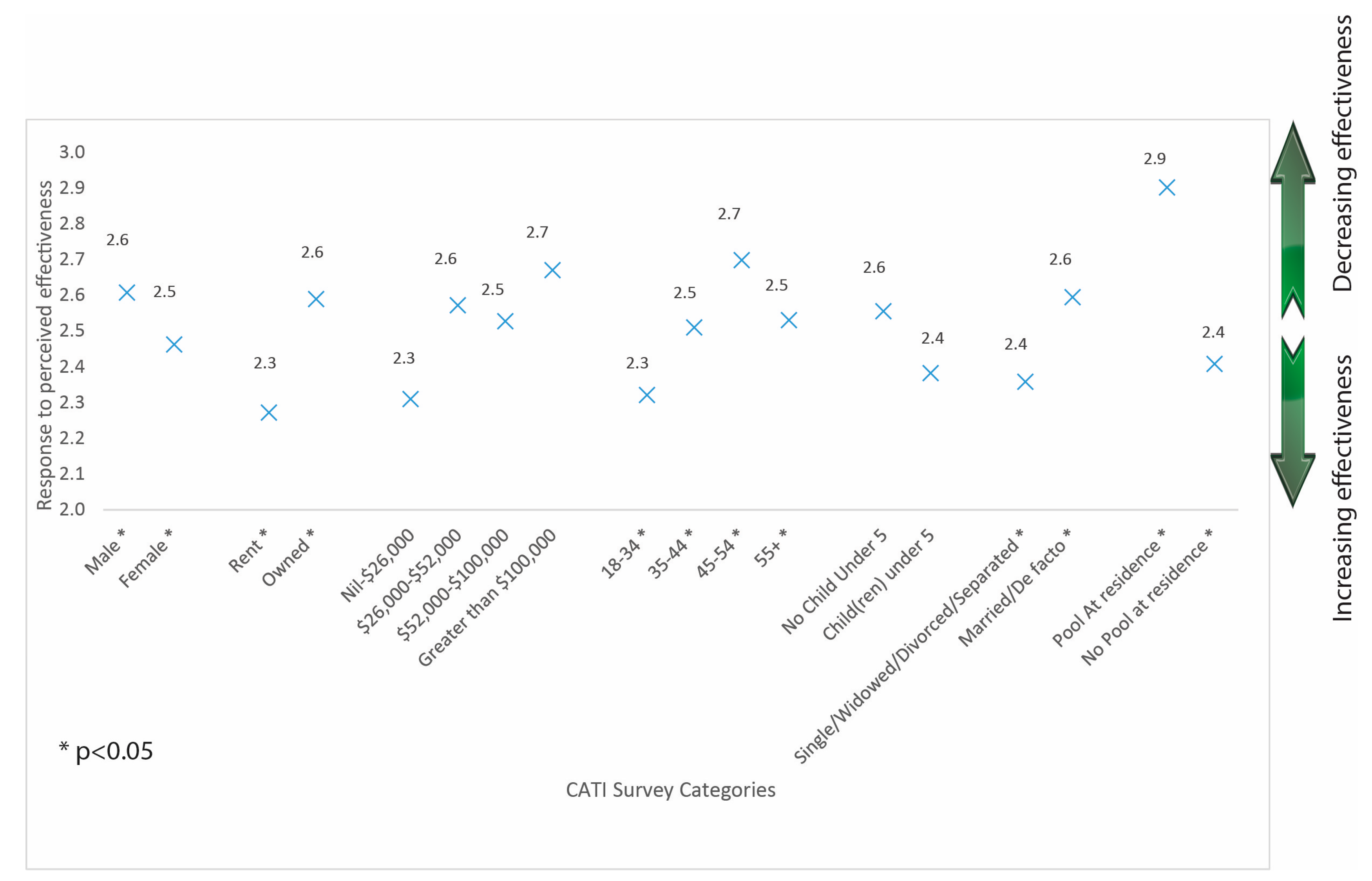
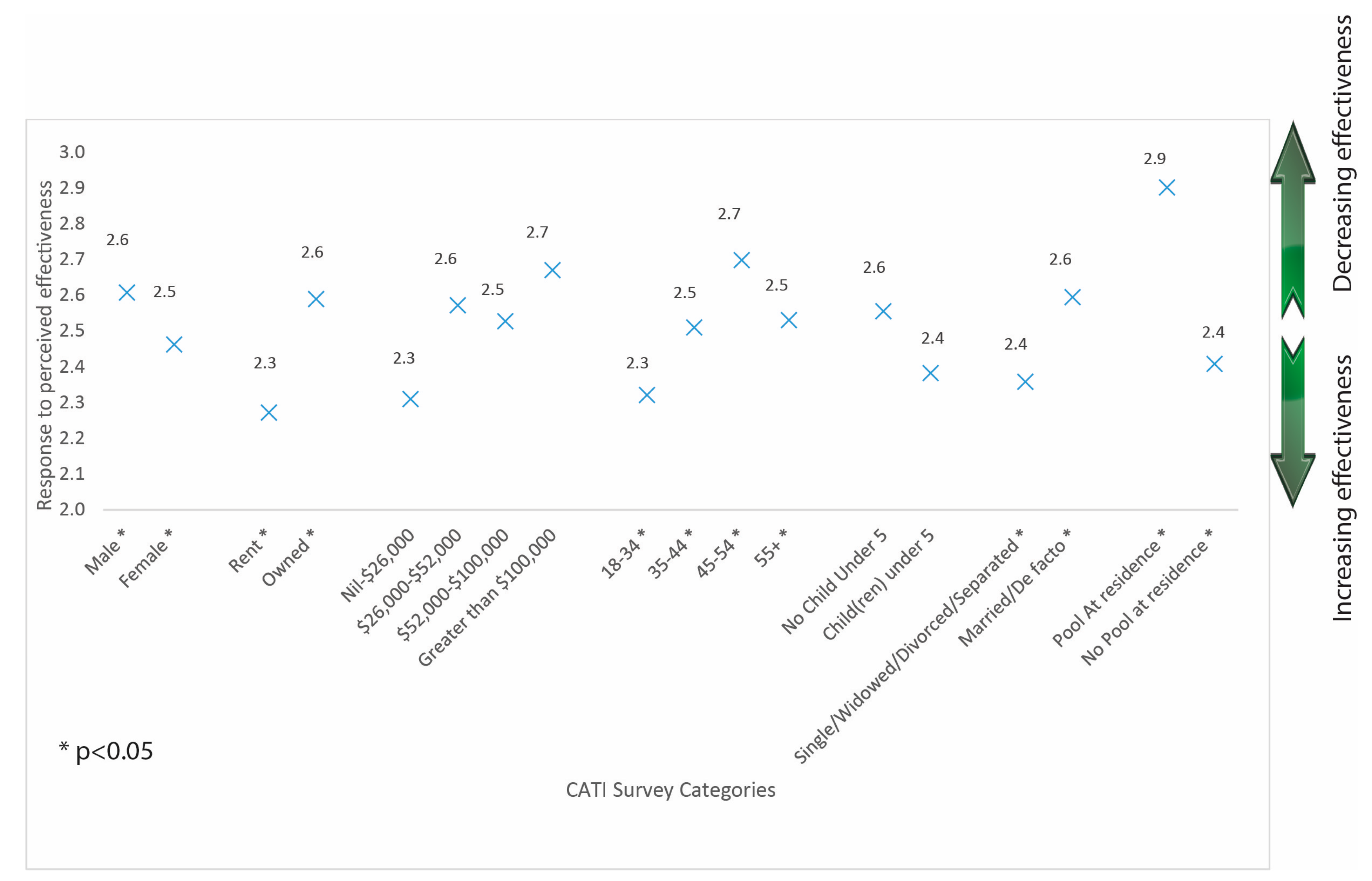
3.1.4. Home Pool Legislation Effectiveness ANOVA Analysis
3.2. Child Drowning Deaths
3.2.1. Child Drowning Deaths Relative Risk
3.2.2. Child Drowning Deaths Prevalence and Chi Square Analysis
4. Discussion
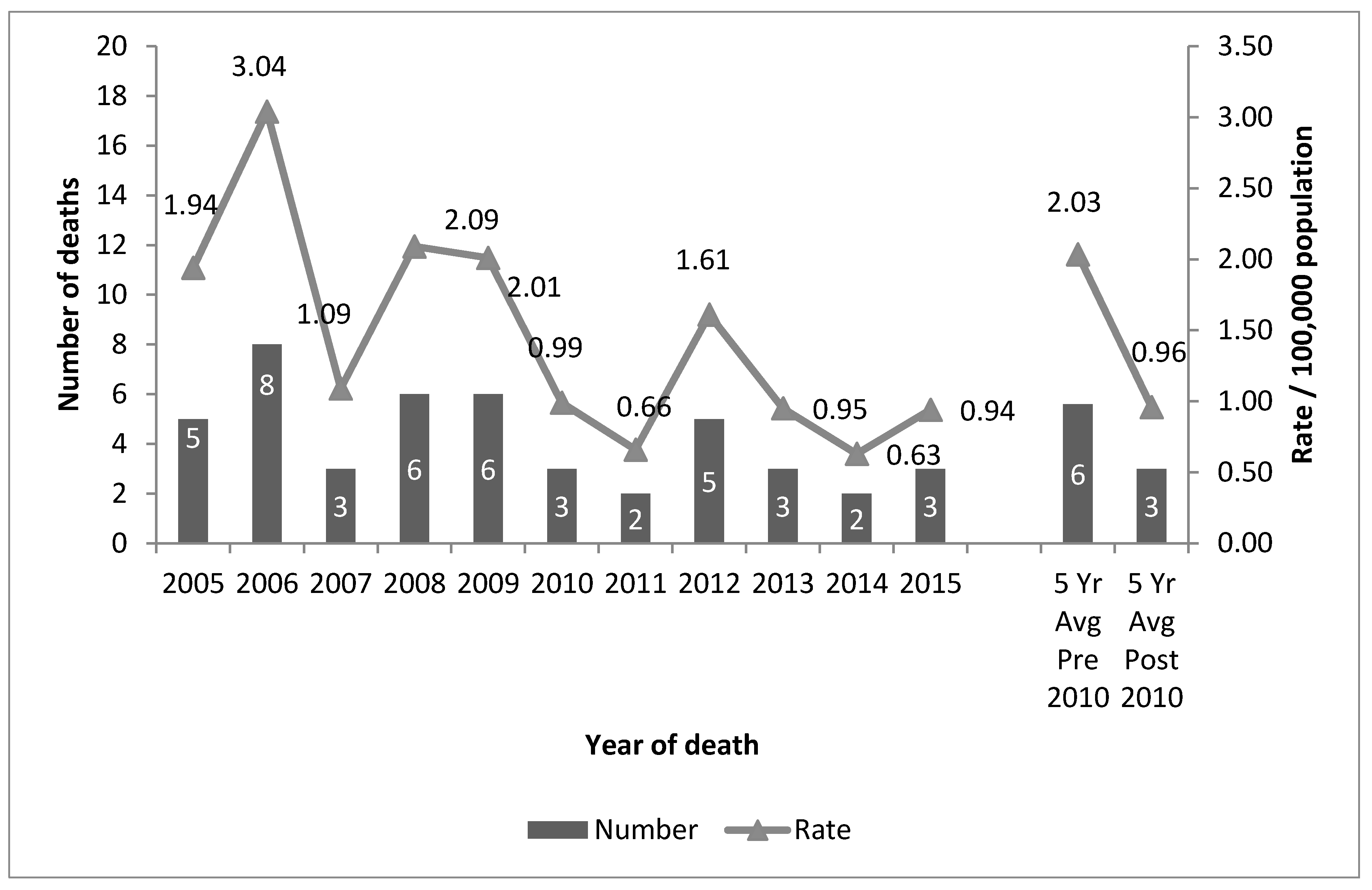
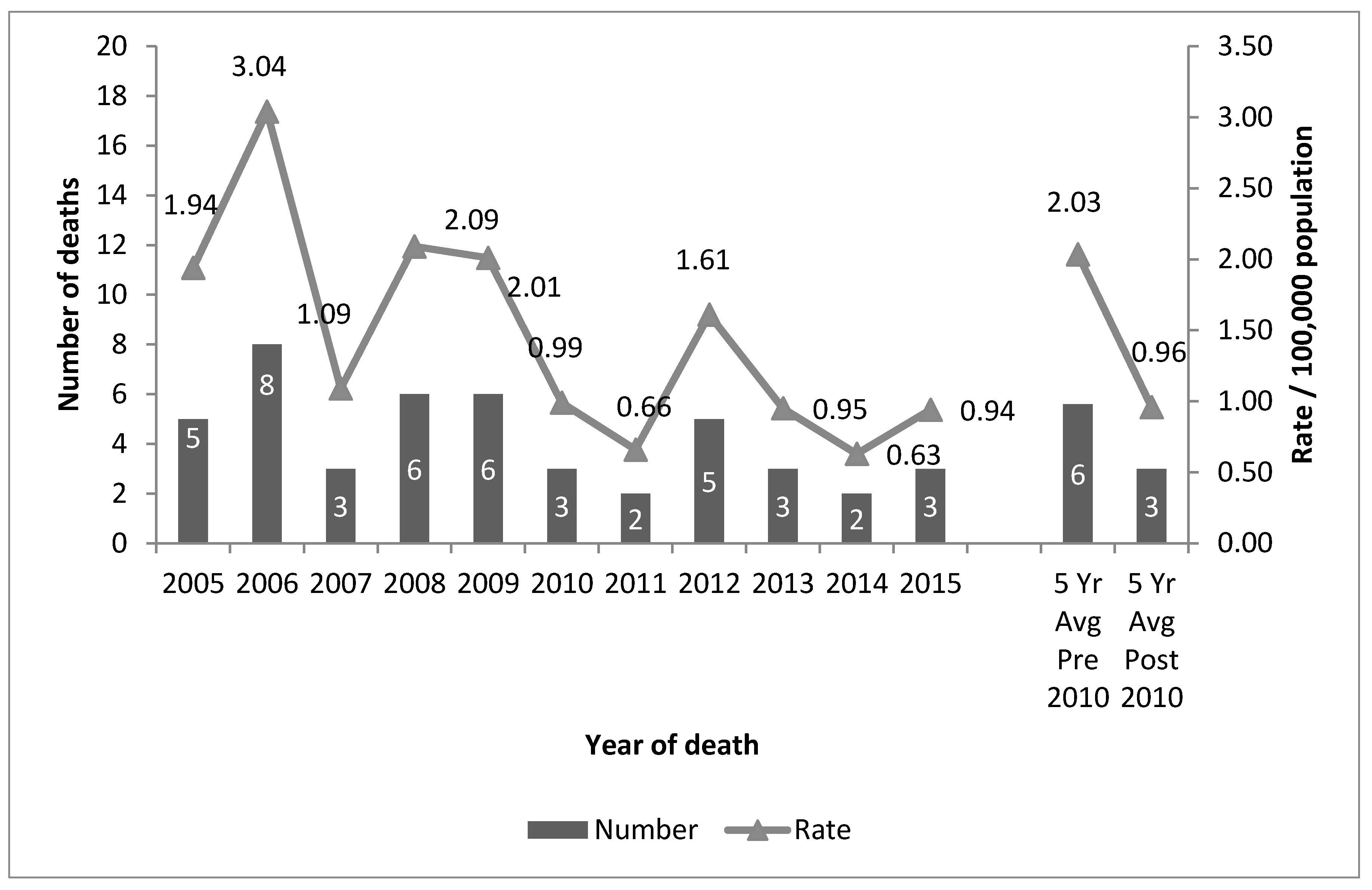
4.1. Trends in Drowning Deaths
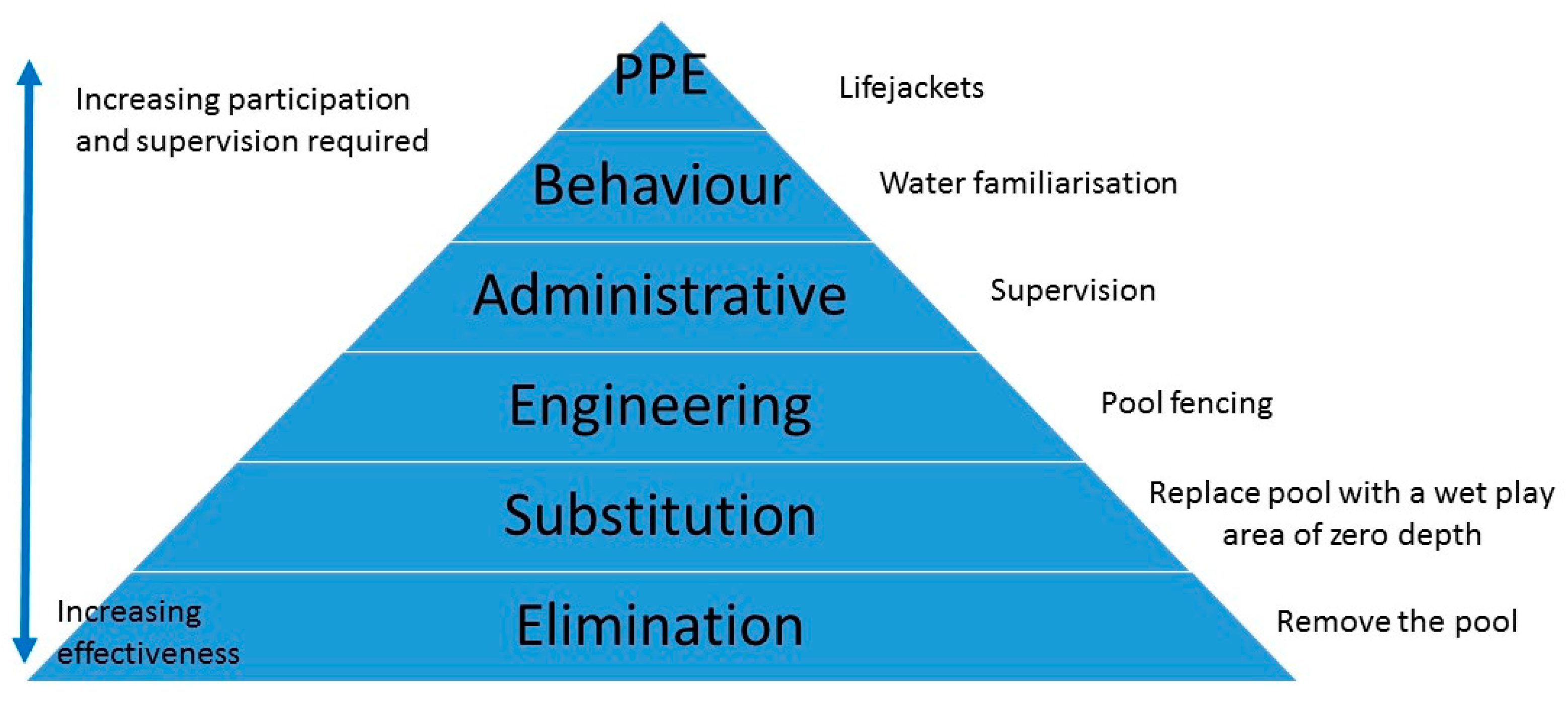
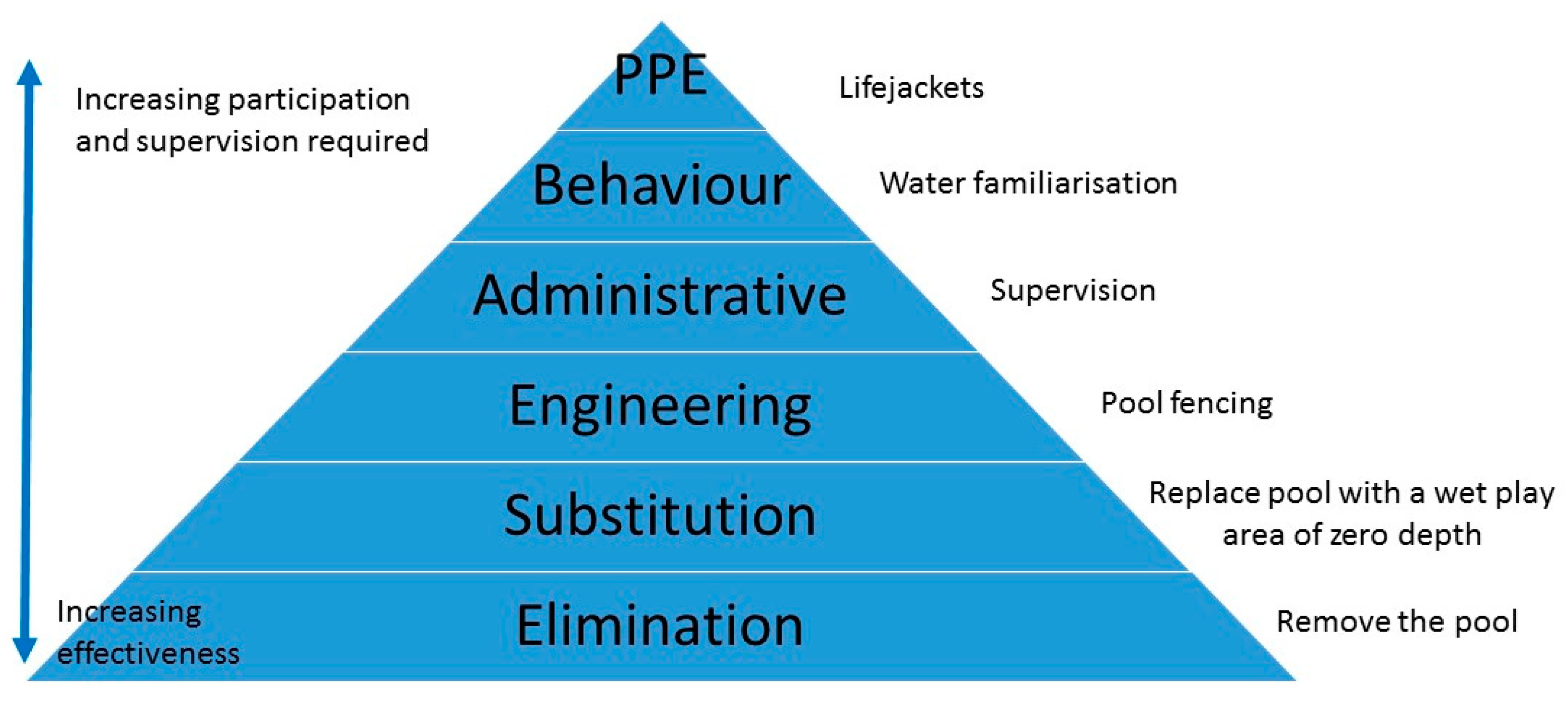
4.2. The Socio-Ecological Model
4.3. Exposure
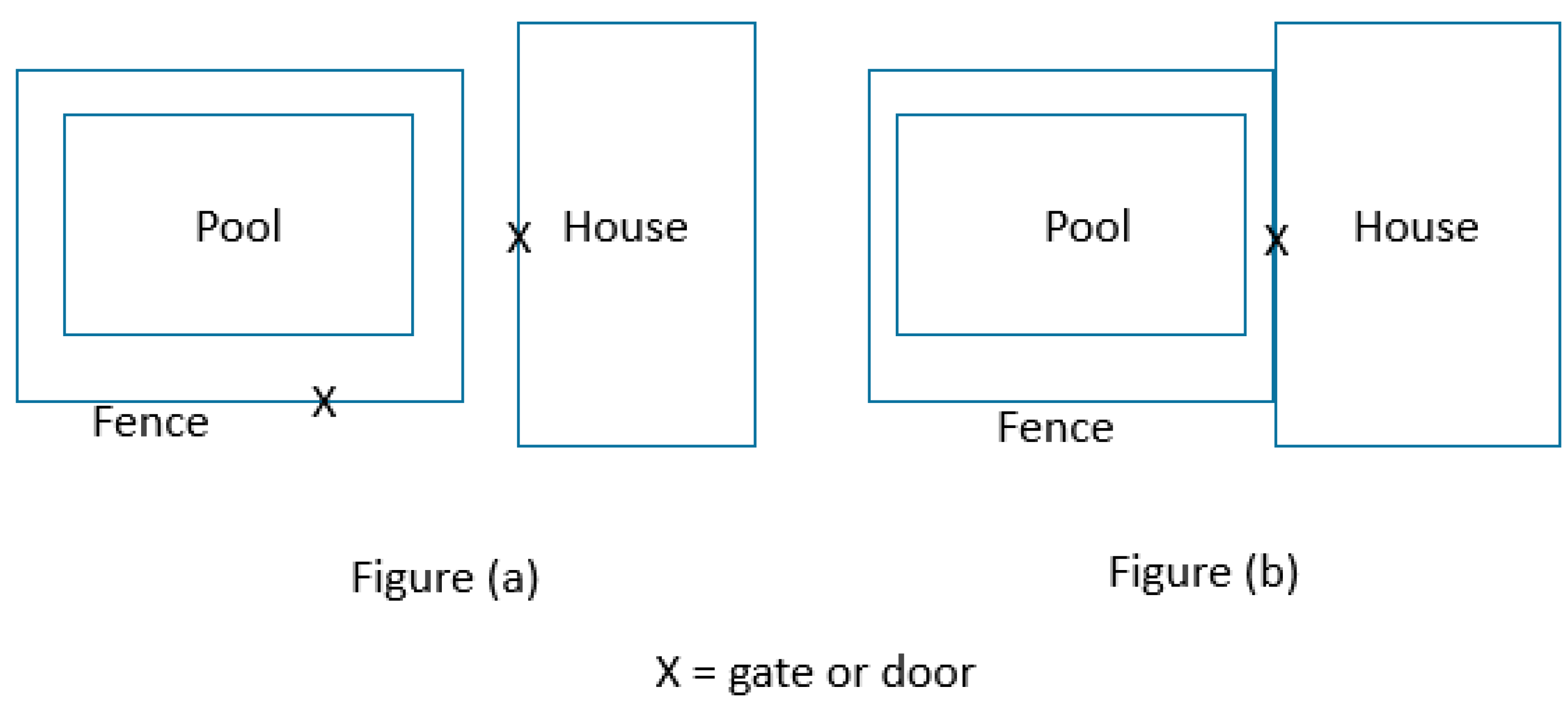
4.4. Legislation
5. Limitations
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Nixon, J.; Pearn, J.; Wilkey, I.; Corcoran, A. Fifteen years of child drowning—A 1967–1981 analysis of all fatal cases from the Brisbane drowning study and an 11 year study of consecutive near-drowning cases. Accid. Anal. Prev. 1986, 18, 199–203. [Google Scholar] [CrossRef]
- Royal Life Saving Society—Australia. Royal Life Saving National Drowning Report 2016; Royal Life Saving Society: Sydney, Australia, 2016. [Google Scholar]
- Thompson, D.C.; Rivara, F.P. Pool fencing for preventing drowning in children. Cochrane Database Syst. Rev. 2000, 2, CD001047. [Google Scholar]
- Government of New South Wales. Swimming Pool Register—Information. 2016. Available online: http://www.swimmingpoolregister.nsw.gov.au/information (accessed on 29 July 2017).
- Haddon, W., Jr. On the escape of tigers an ecologic note—Strategy options in reducing losses in energy damaged people and property. Am. J. Public Health Nations Health 1970, 60, 2229–2234. [Google Scholar] [CrossRef] [PubMed]
- Frieden, T.R. A Framework for Public Health Action: The Health Impact Pyramid. Am. J. Public Health 2010, 100, 590–595. [Google Scholar] [CrossRef] [PubMed]
- Haddon, W., Jr. Approaches to Prevention of Injuries. In Proceedings of the American Medical Association Conference on Prevention of Disabling Injuries, Miami, FL, USA, 20 May 1983. [Google Scholar]
- Scott, I. Prevention of drowning in home pools—Lessons from Australia. Inj. Control Saf. Promot. 2003, 10, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Royal Life Saving National Fatal Drowning Database, 2002–2015. Available online: https://www.royallifesaving.com.au/facts-and-figures/research-and-reports/royal-life-saving-national-fatal-drowning-database (accessed on 10 June 2017).
- Stevenson, M.R.; Rimajova, M.; Edgecombe, D.; Vickery, K. Childhood Drowning: Barriers Surrounding Private Swimming Pools. Pediatrics 2003, 111, e115–e119. [Google Scholar] [CrossRef] [PubMed]
- Pitt, R.; Balanda, K.P. Childhood drowning and near-drowning in Brisbane: The contribution of domestic pools. Med. J. Aust. 1991, 154, 661–665. [Google Scholar] [PubMed]
- Williamson, A.; Irvine, P.; Sadural, S. Analysis of Drownings Involving Children Aged Five Years and Under in NSW; NSW Injury Risk Management Research Centre: Sydney, Australia, 2002; p. 34. [Google Scholar]
- Peden, A.; Mahony, A. Drowning Deaths of Children Under Five in Private Swimming Pools in NSW: A 13 Year Review; Royal Life Saving Society: Sydney, Australia, 2016. [Google Scholar]
- Standards Australia. Australian Standard 1926 Swimming Pool Safety Part 2: Location of Safety Barriers for Swimming Pools; Standards Australia: Sydney, Australia, 2007. [Google Scholar]
- Nixon, J.W.; Pearn, J.H.; Petrie, G.M. Childproof Safety Barriers An ergonomic study to reduce child trauma due to environmental hazards. J. Paediatr. Child Health 1979, 15, 260–262. [Google Scholar] [CrossRef]
- Government of Queensland. MP 3.4—Swimming Pool Barriers; Government of Queensland: Queensland, Australia, 2010.
- Queensland Government. Pool Safety Laws. 2016. Available online: http://www.hpw.qld.gov.au/construction/BuildingPlumbing/PoolSafety/PoolSafetyLaws/Pages/default.aspx (accessed on 21 July 2017).
- McLeroy, K.R.; Steckler, A.; Bibeau, D. The Social Ecology of Health Promotion Interventions. Health Educ. Q. 1988, 15, 351–377. [Google Scholar] [CrossRef] [PubMed]
- Central Queensland (CQ) University Australia Population Research Laboratory. Final Sampling Report—2011 Queensland Social Survey; Institute for Health and Social Science Research: Rockhampton, Australia, 2010. [Google Scholar]
- Australian Bureau of Statistics. 2011 Census QuickStats—Queensland. Available online: http://www.censusdata.abs.gov.au/census_services/getproduct/census/2011/quickstat/3?opendocument (accessed on 29 July 2017).
- Peden, A.E.; Franklin, R.C.; Leggat, P.A. The Hidden Tragedy of Rivers: A Decade of Unintentional Fatal Drowning in Australia. PLoS ONE 2016, 11, e0160709. [Google Scholar] [CrossRef] [PubMed]
- Australian Government Department of Health. Doctor Locator. 2010. Available online: http://www.doctorconnect.gov.au/internet/otd/Publishing.nsf/Content/locator (accessed on 26 June 2015).
- Pink, B. Australian Standard Geographical Classification (ASGC)—July 2007; Australian Bureau of Statistics: Canberra, Australia, 2007.
- Australian Bureau of Statistics. 3101.0—Australian Demographic Statistics, December 2016. Table 53. Estimates Resident Population by Single Year of Age, Queensland; Australian Bureau of Statistics: Canberra, Australia, 2016.
- Royal Life Saving Society—Australia. Drowning Database Definitions and Coding Manual 2016; Peden, A.E., Ed.; Royal Life Saving Society: Sydney, Australia, 2016. [Google Scholar]
- SPSS Inc. IBM SPSS Statistics 20.0.0; IBM: Chicago, IL, USA, 2010. [Google Scholar]
- Keppel, G. Design and Analysis: A Researcher's Handbook, 3rd ed.; Prentice Hall: Englewood Cliffs, NJ, USA, 1991. [Google Scholar]
- Bugeja, L.; Franklin, R.C. An analysis of stratagems to reduce drowning deaths of young children in private swimming pools and spas in Victoria, Australia. Int. J. Inj. Control Saf. Promot. 2013, 20, 282–329. [Google Scholar] [CrossRef] [PubMed]
- Franklin, R.C.; Scarr, J.P.; Pearn, J.H. Reducing Drowning Deaths: The Continued Challenge of Immersion Fatalities in Australia. Med. J. Aust. 2010, 192, 123–126. [Google Scholar] [PubMed]
- Mitchell, R.J.; Williamson, A.M.; Olivier, J. Estimates of drowning morbidity and mortality adjusted for exposure to risk. Inj. Prev. 2010, 16, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Peden, A.E.; Franklin, R.C.; Leggat, P.A. Fatal River Drowning: Identification of Research Gaps through a Systematic Literature Review. Inj. Prev. 2016, 22, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Morgan, D.; Ozanne-Smith, J.; Triggs, T. Descriptive epidemiology of drowning deaths in a surf beach swimmer and surfer population. Inj. Prev. 2008, 14, 62–65. [Google Scholar] [CrossRef] [PubMed]
- Van Weerdenburg, K.; Mitchell, R.; Wallner, F. Backyard swimming pool safety inspections: A comparison of management approaches and compliance levels in three local government areas in NSW. Health Promot. J. Aust. 2006, 17, 37–42. [Google Scholar]
- Barker, R.; Spinks, D.; Hockey, R.; Pitt, R. Discussion Paper: Pool Fencing Legislation in Australia in 2003: The Way Forward; Queensland Injury Surveillance Unit: Brisbane, Australia, 2003; p. 10. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Pool Ownership—Yes | Pool Ownership—No | Degrees of Freedom, X2 Analysis Comparing Pool Ownership Yes to Pool Ownership No (p-Value) | ||||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||
| 1263 | 100.0 | 324 | 25.7 | 939 | 74.3 | ||
| Sex | |||||||
| Male | 632 | 50.0 | 163 | 25.8 | 469 | 74.2 | df = 1, 0.01 (p = 0.91) |
| Female | 631 | 50.0 | 161 | 25.5 | 470 | 74.5 | |
| Age Group | |||||||
| 18–34 years | 175 | 13.9 | 32 | 18.3 | 143 | 81.7 | df = 1, 5.74 (p = 0.02) |
| 35–44 years | 202 | 16.0 | 66 | 32.7 | 136 | 67.3 | df = 1, 6.29 (p = 0.01) |
| 45–54 years | 241 | 19.1 | 80 | 33.2 | 161 | 66.8 | df = 1, 8.99 (p < 0.01) |
| 55+ years | 635 | 50.3 | 143 | 22.5 | 492 | 77.5 | df = 1, 6.49 (p = 0.01) |
| No response | 10 | 0.8 | 3 | 0.9 | 7 | 0.7 | - |
| Born in Australia | |||||||
| Yes | 980 | 77.6 | 243 | 24.8 | 737 | 75.2 | df = 1, 1.69 (p = 0.19) |
| No | 283 | 22.4 | 81 | 28.6 | 202 | 71.4 | |
| Years of Education | |||||||
| 1–10 years | 307 | 24.3 | 46 | 15.0 | 261 | 85.0 | df = 1, 25.12 (p < 0.001) |
| 11–12 years | 283 | 22.4 | 82 | 29.0 | 201 | 71.0 | df = 1, 1.85 (p = 0.17) |
| 13–14 years | 138 | 10.9 | 39 | 28.3 | 99 | 71.7 | df = 1, 0.47 (p = 0.50) |
| 15+ years | 521 | 41.3 | 156 | 29.9 | 365 | 70.1 | df = 1, 7.77 (p = 0.01) |
| Don’t know/No response | 14 | 1.1 | 1 | 7.1 | 13 | 92.9 | - |
| Household Income Level | |||||||
| Nil–$26,000 | 145 | 11.5 | 27 | 18.6 | 118 | 81.4 | df = 1, 5.21 (p = 0.02) |
| $26,001–$52,000 | 161 | 12.7 | 24 | 14.9 | 137 | 85.1 | df = 1, 13.21 (p < 0.001) |
| $52,001–$100,000 | 206 | 16.3 | 48 | 23.3 | 158 | 76.7 | df = 1, 1.17 (p = 0.28) |
| Greater than $100,000 | 287 | 22.7 | 110 | 38.3 | 177 | 61.7 | df = 1, 34.34 (p < 0.001) |
| Don’t know/No response | 464 | 36.7 | 115 | 24.8 | 349 | 75.2 | - |
| Have a Child Under the Age of Five | |||||||
| Yes | 154 | 12.2 | 37 | 24.0 | 117 | 76.0 | df = 1, 0.24 (p = 0.63) |
| No | 1109 | 87.8 | 287 | 25.9 | 822 | 74.1 | |
| Child Under the Age of 18 in the Household | |||||||
| Yes | 417 | 33.0 | 139 | 33.3 | 278 | 66.7 | df = 1, 19.48 (p < 0.001) |
| No | 844 | 66.8 | 184 | 21.8 | 660 | 78.2 | |
| No response | 2 | 0.2 | 1 | 50.0 | 1 | 50.0 | - |
| Household Ownership | |||||||
| Rent | 210 | 16.6 | 20 | 9.5 | 190 | 90.5 | df = 1, 34.13 (p < 0.001) |
| Own | 1038 | 82.2 | 299 | 28.8 | 739 | 71.2 | |
| No response | 15 | 1.2 | 5 | 33.3 | 10 | 66.7 | - |
| Marital Status | |||||||
| Single/Widowed/Divorced/Separated | 326 | 25.8 | 62 | 19.0 | 264 | 81.0 | df = 1, 10.26 (p = 0.001) |
| Married/De facto | 935 | 74.0 | 262 | 28.0 | 673 | 72.0 | |
| No response | 2 | 0.2 | 0 | 0.0 | 2 | 100.0 | - |
| Total | Pool Fencing Effective | No Response | Pool Fencing Ineffective | Degrees of Freedom, X2 Analysis Comparing Pool Fencing Effective to Pool Fencing Ineffective (p-Value) | |||||
|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | ||
| 1263 | 100.0 | 726 | 57.5 | 38 | 3.0 | 499 | 39.5 | ||
| Sex | |||||||||
| Male | 632 | 50.0 | 345 | 54.6 | 25 | 4.0 | 262 | 41.5 | df = 1, 2.94 (p = 0.09) |
| Female | 631 | 50.0 | 381 | 60.4 | 13 | 2.1 | 237 | 37.6 | |
| Age Group | |||||||||
| 18–34 years | 175 | 13.9 | 109 | 62.3 | 10 | 5.7 | 56 | 32.0 | df = 3, 8.04 (p = 0.45) |
| 35–44 years | 202 | 16.0 | 116 | 57.4 | 8 | 4.0 | 78 | 38.6 | |
| 45–54 years | 241 | 19.1 | 123 | 51.0 | 6 | 2.5 | 112 | 46.5 | |
| 55+ years | 635 | 50.3 | 374 | 58.9 | 13 | 2.0 | 248 | 39.1 | |
| No response | 10 | 0.8 | 4 | 40.0 | 5 | 50.0 | 1 | 10.0 | - |
| Born in Australia | |||||||||
| Yes | 980 | 77.6 | 571 | 58.3 | 28 | 2.9 | 381 | 38.9 | df = 1, 0.90 (p = 0.34) |
| No | 283 | 22.4 | 155 | 54.8 | 10 | 3.5 | 118 | 41.7 | |
| Years of Education | |||||||||
| 1–10 years | 307 | 24.3 | 189 | 61.6 | 5 | 1.6 | 113 | 36.8 | df = 3, 4.80 (p = 0.19) |
| 11–12 years | 283 | 22.4 | 163 | 57.6 | 5 | 1.8 | 115 | 40.6 | |
| 13–14 years | 138 | 10.9 | 69 | 50.0 | 4 | 2.9 | 65 | 47.1 | |
| 15+ years | 521 | 41.3 | 297 | 57.0 | 23 | 4.4 | 201 | 38.6 | |
| Don’t know/No response | 14 | 1.1 | 8 | 57.1 | 1 | 7.1 | 5 | 35.7 | - |
| Household Income Level | |||||||||
| Nil–$26,000 | 145 | 11.5 | 96 | 66.2 | 3 | 2.1 | 46 | 31.7 | df = 1, 5.77 (p = 0.02) |
| $26,001–$52,000 | 161 | 12.7 | 96 | 59.6 | 2 | 1.2 | 63 | 39.1 | df = 1, 0.25 (p = 0.62) |
| $52,001–$100,000 | 206 | 16.3 | 118 | 57.3 | 7 | 3.4 | 81 | 39.3 | df = 1, 0.05 (p = 0.83) |
| Greater than $100,000 | 287 | 22.7 | 145 | 50.5 | 11 | 3.8 | 131 | 45.6 | df = 1, 6.57 (p = 0.01) |
| Don’t know/No response | 464 | 36.7 | 271 | 58.4 | 15 | 3.2 | 178 | 38.4 | - |
| Have a Child Under the Age of Five | |||||||||
| Yes | 154 | 12.2 | 93 | 60.4 | 5 | 3.2 | 56 | 36.4 | df = 1, 0.70 (p = 0.40) |
| No | 1109 | 87.8 | 633 | 57.1 | 33 | 3.0 | 443 | 39.9 | |
| Children Under the Age of 18 in the Household | |||||||||
| Yes | 417 | 33.0 | 246 | 59.0 | 15 | 3.6 | 156 | 37.4 | df = 1, 0.91 (p = 0.34) |
| No | 844 | 66.8 | 479 | 56.8 | 23 | 2.7 | 342 | 40.5 | |
| No response | 2 | 0.2 | 1 | 50.0 | 0 | 0.0 | 1 | 50.0 | - |
| Household Ownership | |||||||||
| Rent | 210 | 16.6 | 137 | 65.2 | 8 | 3.8 | 65 | 31.0 | df = 1, 7.51 (p < 0.01) |
| Own | 1038 | 82.2 | 579 | 55.8 | 30 | 2.9 | 429 | 41.3 | |
| No response | 15 | 1.2 | 10 | 66.7 | 0 | 0.0 | 5 | 33.3 | - |
| Marital Status | |||||||||
| Single/Widowed/Divorced/Separated | 326 | 25.8 | 213 | 65.3 | 8 | 2.5 | 105 | 32.2 | df = 1, 10.56 (p = 0.001) |
| Married/De facto | 935 | 74.0 | 512 | 54.8 | 30 | 3.2 | 393 | 42.0 | |
| No response | 2 | 0.2 | 1 | 50.0 | 0 | 0.0 | 1 | 50.0 | - |
| Pool Ownership | |||||||||
| Yes | 324 | 25.7 | 144 | 44.4 | 9 | 2.8 | 171 | 52.8 | df = 1, 32.25 (p < 0.001) |
| No | 939 | 74.3 | 582 | 62.0 | 29 | 3.1 | 328 | 34.9 | |
| Total | Before Implementation (2005–2009) | Implementation Year (2010) | After Implementation (2011–2015) | Degrees of Freedom, X2 Analysis Comparing before and after Implementation (p-Value) | |||||
|---|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | N | % | ||
| Total | 46 | 100.0 | 28 | 60.9 | 3 | 6.5 | 15 | 32.6 | df = 1, 3.93 (p < 0.05) |
| Sex | |||||||||
| Male | 25 | 54.3 | 13 | 52.0 | 1 | 4.0 | 11 | 44.0 | df = 1, 2.87 (p = 0.09) |
| Female | 21 | 45.7 | 15 | 71.4 | 2 | 9.5 | 4 | 19.0 | |
| Single Year of Age | |||||||||
| 0 year | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | df = 3, 4.04 (p = 0.13) |
| 1 year | 17 | 37.0 | 8 | 47.1 | 0 | 0.0 | 9 | 52.9 | |
| 2 years | 20 | 43.5 | 13 | 65.0 | 3 | 15.0 | 4 | 20.0 | |
| 3–4 years | 9 | 19.5 | 7 | 77.8 | 0 | 0.0 | 2 | 22.2 | |
| Remoteness Classification of Drowning Incident Location | |||||||||
| Major Cities | 23 | 50.0 | 15 | 65.2 | 1 | 4.3 | 7 | 30.4 | df = 3, 1.74 (p = 0.63) |
| Inner Regional | 10 | 21.7 | 5 | 50.0 | 0 | 0.0 | 5 | 50.0 | |
| Outer Regional | 11 | 23.9 | 7 | 63.6 | 1 | 9.1 | 3 | 27.3 | |
| Remote & Very Remote | 2 | 4.3.0 | 1 | 50.0 | 1 | 50.0 | 0 | 0.0 | |
| Season of Drowning Incident | |||||||||
| Summer | 22 | 47.8 | 11 | 50.0 | 2 | 9.1 | 9 | 40.9 | df = 3, 2.34 (p = 0.51) |
| Autumn | 7 | 15.2 | 5 | 71.4 | 0 | 0.0 | 2 | 28.6 | |
| Winter | 7 | 15.2 | 6 | 85.7 | 0 | 0.0 | 1 | 14.3 | |
| Spring | 10 | 21.7 | 6 | 60.0 | 1 | 10.0 | 3 | 30.0 | |
| Time of Day of Drowning Incident * | |||||||||
| Morning | 9 | 20.0 | 5 | 55.6 | 2 | 22.2 | 2 | 22.2 | df = 2, 0.34 (p = 0.84) |
| Afternoon | 34 | 75.6 | 21 | 61.8 | 1 | 2.9 | 12 | 35.3 | |
| Evening & Early Morning | 2 | 4.4 | 1 | 50.0 | 0 | 0.0 | 1 | 50.0 | |
| Point of Entry | |||||||||
| No fence | 6 | 13.0 | 3 | 50.0 | 1 | 16.7 | 2 | 33.3 | df = 6, 12.79 (p = 0.05) |
| Gate propped open | 13 | 28.3 | 4 | 30.8 | 0 | 0.0 | 9 | 69.2 | |
| Disrepair—faulty gate, climbed under, loose panels etc. | 9 | 19.6 | 7 | 77.8 | 0 | 0.0 | 2 | 22.2 | |
| Child climbed over fence | 4 | 8.7 | 3 | 75.0 | 1 | 25.0 | 0 | 0.0 | |
| Child already in pool area | 3 | 6.5 | 2 | 66.7 | 0 | 0.0 | 1 | 33.3 | |
| No isolation fencing, child accessed pool through door, window etc. | 4 | 8.7 | 4 | 100.0 | 0 | 0.0 | 0 | 0.0 | |
| Child used an object to open gate | 3 | 6.5 | 3 | 100.0 | 0 | 0.0 | 0 | 0.0 | |
| Unknown | 4 | 8.7 | 2 | 50.0 | 1 | 25.0 | 1 | 25.0 | |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franklin, R.C.; Peden, A.E. Improving Pool Fencing Legislation in Queensland, Australia: Attitudes and Impact on Child Drowning Fatalities. Int. J. Environ. Res. Public Health 2017, 14, 1450. https://doi.org/10.3390/ijerph14121450
Franklin RC, Peden AE. Improving Pool Fencing Legislation in Queensland, Australia: Attitudes and Impact on Child Drowning Fatalities. International Journal of Environmental Research and Public Health. 2017; 14(12):1450. https://doi.org/10.3390/ijerph14121450
Chicago/Turabian StyleFranklin, Richard C., and Amy E. Peden. 2017. "Improving Pool Fencing Legislation in Queensland, Australia: Attitudes and Impact on Child Drowning Fatalities" International Journal of Environmental Research and Public Health 14, no. 12: 1450. https://doi.org/10.3390/ijerph14121450