
Food and Beverage Availability in Small Food Stores Located in Healthy Food Financing Initiative Eligible Communities

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Selected Communities
2.2. Data Collection and Food Store Observation Tool
2.3. Measures
2.3.1. General Store Features
2.3.2. Food and Beverage Availability
2.4. Statistical Analysis
3. Results
3.1. Store Features
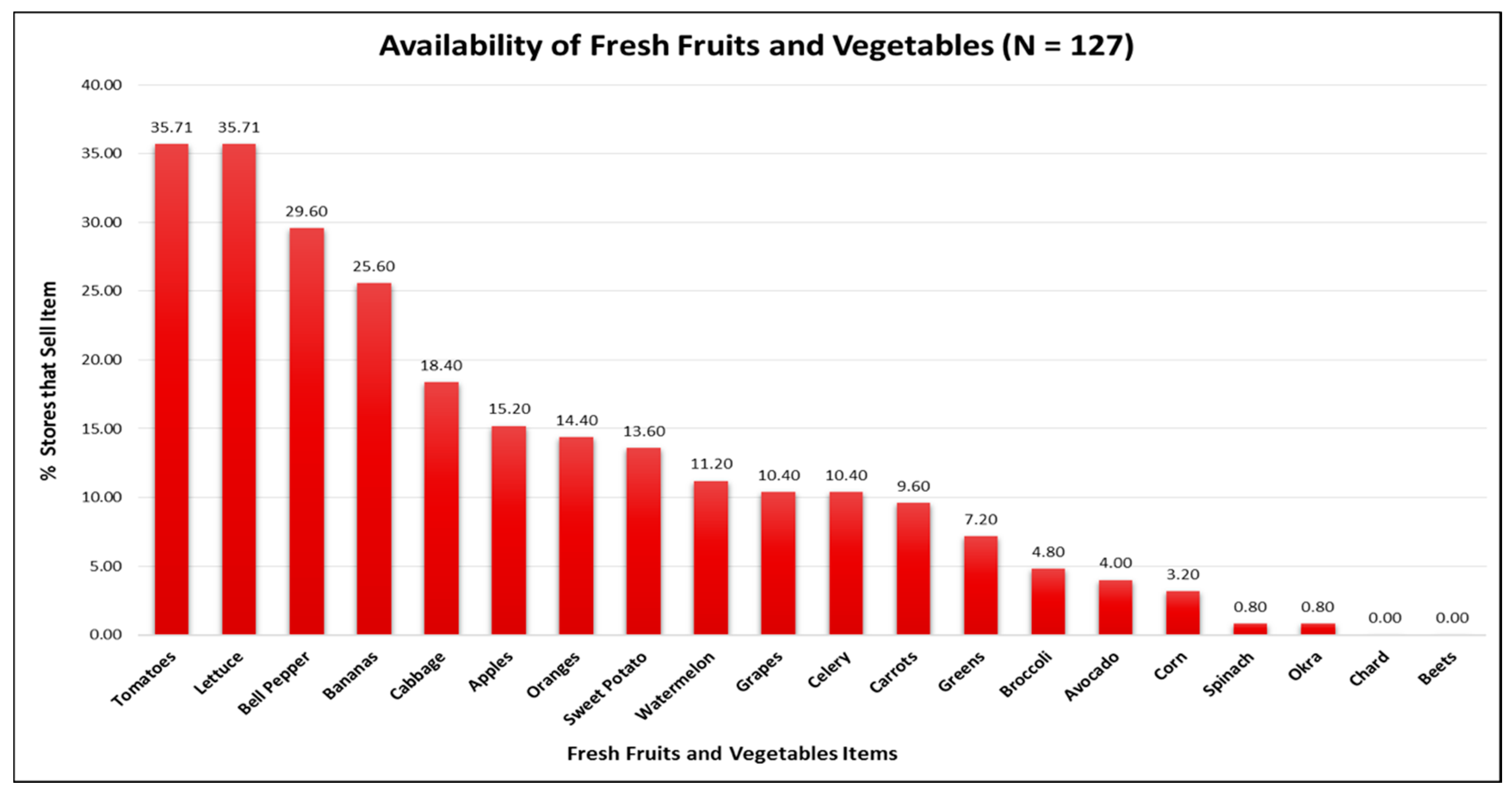
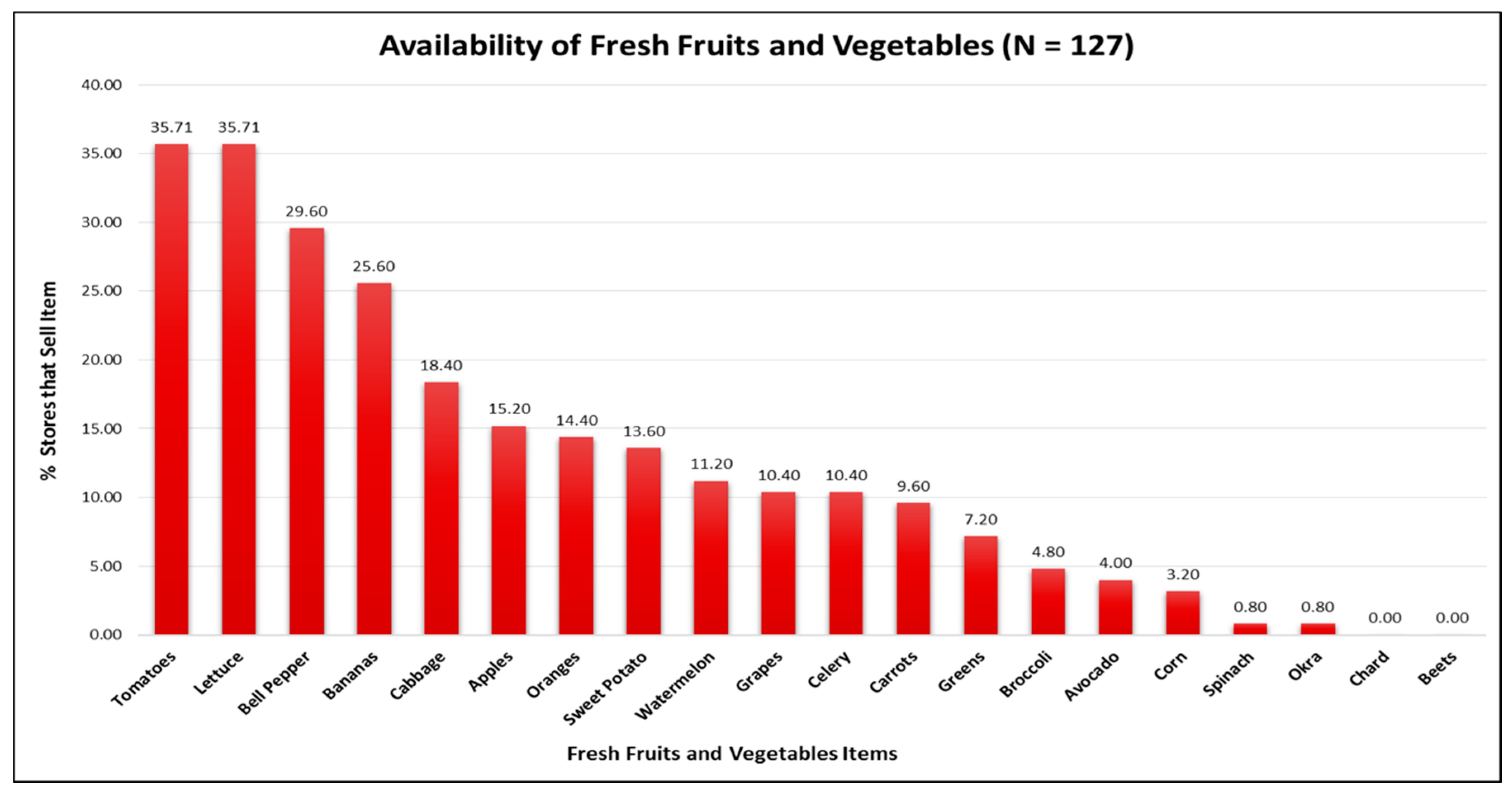
3.2. Fruit and Vegetable Availability
3.3. Food and Beverage Availability
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Morland, K.; Wing, S.; Diez Roux, A.; Poole, C. Neighborhood characteristics associated with the location of food stores and food service places. Am. J. Prev. Med. 2002, 22, 23–29. [Google Scholar] [CrossRef]
- Franco, M.; Diez Roux, A.V.; Glass, T.A. Neighborhood characteristics and availability of healthy foods in Baltimore. Am. J. Prev. Med. 2008, 35, 561–577. [Google Scholar] [CrossRef] [PubMed]
- Larson, N.I.; Story, M.T.; Nelson, M.C. Neighborhood environments: Disparities in access to healthy foods in the U.S. Am. J. Prev. Med. 2009, 36, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Powell, L.M.; Slater, S.; Mirtcheva, D.; Bao, Y.; Chaloupka, F.J. Food store availability ad neighborhood characteristics in the United States. Prev. Med. 2007, 44, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Morland, K.; Philomena, S. Disparities in the availability of fruits and vegetables between racially segregated urban neighborhoods. Public Health Nutr. 2007, 10, 1481–1489. [Google Scholar] [CrossRef] [PubMed]
- Hilmers, A.; Hilmers, D.C.; Dave, J. Neighborhood disparities in access to healthy foods and their effects on environmental justice. Am. J. Public Health 2012, 102, 1644–1654. [Google Scholar] [CrossRef] [PubMed]
- Dutko, P.; Ver Ploeg, M.; Farrigan, T. Characteristics and Influential Factors of Food Deserts; USDA Economic Research Service Report No. 140; 2012. Available online: http://www.ers.usda.gov/media/883903/err140.pdf (accessed on 24 September 2016).
- US Department of Agriculture Economic Research Service. Access to Affordable and Nutrition Food: Measuring and Understanding Food Deserts and Their Consequences. 2009. Available online: http://www.ers.usda.gov/media/242675/ap036_1_.pdf (accessed on 24 September 2016).
- Bodor, J.N.; Rice, J.C.; Farley, T.A.; Swalm, C.M.; Rose, D. The association between obesity and urban food environments. J. Urban Health 2010, 87, 771–781. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Aggarwal, A.; Hurvitz, P.M.; Monsivais, P.; Moudon, A.V. Obesity and Supermarket Access: Proximity or Price? Am. J. Public Health 2012, 102, e74–e80. [Google Scholar] [CrossRef] [PubMed]
- Caspi, C.; Sorensen, G.; Subramanian, S.V. The local food environment and diet: A systematic review. Health Place 2012, 18, 1172–1787. [Google Scholar] [CrossRef] [PubMed]
- Moore, L.V.; Diez Roux, A.V.; Nettleton, J.A.; Jacobs, D.R. Associations of the Local Food Environment with Diet Quality—A Comparison of Assessments based on Surveys and Geographic Information Systems: The Multi-Ethnic Study of Atherosclerosis. Am. J. Epidemiol. 2008, 167, 917–924. [Google Scholar] [CrossRef] [PubMed]
- Bodor, J.N.; Rose, D.; Farley, T.A.; Swalm, C.; Scott, S.K. Neighborhood fruit and vegetable availability and consumption: The role of small food stores in an urban environment. Public Health Nutr. 2008, 11, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Beydoun, M.A. The Obesity Epidemic in the United States—Gender, Age, Socioeconomic, Racial/Ethnic, and Geographic Characteristics: A Systematic Review and Meta-Regression Analysis. Epidemiol. Rev. 2007, 29, 6–28. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Malarcher, A.M.; Giles, W.H.; Myers, G. Racial, ethnic and socioeconomic disparities in the clustering of cardiovascular disease risk factors. Ethn. Disp. 2004, 14, 43–48. [Google Scholar]
- Singleton, C.R.; Affuso, O.; Sen, B. Decomposing Racial Disparities in Obesity Prevalence: Variations in Retail Food Environment. Am. J. Prev. Med. 2016, 50, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Powell, L.M.; Wada, R.; Krauss, R.C.; Wang, Y. Ethnic disparities in adolescent body mass index in the United States: The role of parental socioeconomic status and economic contextual factors. Soc. Sci. Med. 2012, 75, 467–476. [Google Scholar] [CrossRef] [PubMed]
- Zenk, S.N.; Powell, L.M.; Rimkus, L.; Isgor, Z.; Barker, D.C.; Ohri-Vachaspati, P.; Chaloupka, F. Relative and absolute availability of healthier food and beverage alternatives across communities in the United States. Am. J. Public Health 2014, 104, 2170–2178. [Google Scholar] [CrossRef] [PubMed]
- Andreyeva, T.; Blumenthal, D.M.; Schwartz, M.B.; Long, M.W.; Brownell, K.D. Availability and prices of food across stores and neighborhoods: The case of New Haven, Connecticut. Health Aff. 2008, 27, 1381–1388. [Google Scholar] [CrossRef] [PubMed]
- Leone, A.F.; Rigby, S.; Betterley, C.; Park, S.; Kurtz, H.; Johnson, M.A.; Lee, J.S. Store type and demographic influence on the availability and price of healthful foods, Leon County, Florida, 2008. Prev. Chronic. Dis. 2011, 8, A140. [Google Scholar] [PubMed]
- Laska, M.N.; Caspi, C.; Pelletier, J.E.; Friebur, R.; Harnack, L.J. Lack of Healthy Food in Small-Size to Mid-Size Retailers Participating in the Supplemental Nutrition Assistance Program, Minneapolis-St. Paul, Minnesota, 2014. Prev. Chronic. Dis. 2015, 12. [Google Scholar] [CrossRef] [PubMed]
- Zenk, S.N.; Grigsby-Toussaint, D.S.; Curry, S.J.; Berbaum, M.; Schneider, L. Short-Term Temporal Stability in Observed Retail Food Characteristics. J. Nutr. Educ. Behav. 2010, 42, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Rimkus, L.; Isgor, Z.; Ohri-Vachaspati, P.; Zenk, S.N.; Powell, L.M.; Barker, D.C.; Chaloupka, F.J. Disparities in the Availability and Price of Low-Fat and Higher-Fat Milk in U.S. Food Stores by Community Characteristics. J. Acad. Nutr. Diet. 2015, 115, 1975–1985. [Google Scholar] [CrossRef] [PubMed]
- Jetter, K.M.; Cassady, D.L. The availability and cost of healthier food alternatives. Am. J. Prev. Med. 2006, 30, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Laska, M.N.; Borradaile, K.E.; Tester, J.; Foster, G.D.; Gittelsohn, J. Healthy food availability in small urban food stores: A comparison of four US cities. Public Health Nutr. 2010, 13, 1031–1035. [Google Scholar] [CrossRef] [PubMed]
- Bustillos, B.; Sharkey, J.R.; Anding, J.; McIntosh, A. Availability of more healthful food alternatives in traditional, convenience, and nontraditional types of food stores in two rural Texas counties. J. Am. Diet. Assoc. 2009, 109, 883–889. [Google Scholar] [CrossRef] [PubMed]
- Caspi, C.; Pelletier, J.E.; Harnack, L.; Erickson, D.J.; Laska, M.N. Differences in healthy food supply and stocking practices between small grocery stores, gas-marts, pharmacies and dollar stores. Public Health Nutr. 2016, 19, 540–547. [Google Scholar] [CrossRef] [PubMed]
- Liese, A.D.; Weis, K.E.; Pluto, D.; Smith, E.; Lawson, A. Food store types, availability, and cost of foods in a rural environment. J. Am. Diet. Assoc. 2007, 107, 1916–1923. [Google Scholar] [CrossRef] [PubMed]
- The Food Trust. A Healthy Food Financing Initiative: An Innovative Approach to Improve Health and Spark Economic Development. 2012. Available online: http://thefoodtrust.org/uploads/media_items/hffi-one-pager.original.pdf (accessed on 29 August 2016).
- Giang, T.; Karpyn, A.; Laurison, H.B. Closing the grocery gap in underserved communities: The creation of the Pennsylvania Fresh Food Financing Initiative. J. Public Health Manag. Pract. 2008, 14, 272–279. [Google Scholar] [CrossRef] [PubMed]
- Cummins, S.; Flint, E.; Matthews, S.A. New neighborhood grocery store increased awareness of food access by did not alter dietary habits or obesity. Health Aff. 2014, 33, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Chrisinger, B. A Mixed-Methods Assessment of a New Supermarket in a Food Desert: Contributions to Everyday Life and Health. J. Urban Health 2016, 93, 425–437. [Google Scholar] [CrossRef] [PubMed]
- Honeycutt, S.; Leeman, J.; McCarthy, W.J.; Bastani, R.; Carter-Edwards, L.; Clark, H.; Garney, W.; Gustat, J.; Hites, L.; Nothwehr, F.; et al. Evaluating Policy, Systems, and Environmental Change Interventions: Lessons Learned from CDC’s Prevention Research Centers. Prev. Chronic. Dis. 2015, 12. [Google Scholar] [CrossRef] [PubMed]
- Bunnell, R.; O’Neil, D.; Soler, R.; Payne, R.; Giles, W.H.; Collins, J.; Bauer, U.; Communities Putting Prevention to Work Program Group. Fifty communities putting prevention to work: Accelerating chronic disease prevention through policy, systems and environmental change. J. Community Health 2012, 37, 1081–1090. [Google Scholar] [CrossRef] [PubMed]
- Karypn, A.; Manon, M.; Treuhaft, S.; Giang, T.; Harries, C.; McCoubrey, K. Policy solutions to the “grocery gap”. Health Aff. 2010, 29, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Ulmer, V.M.; Rathert, A.R.; Rose, D. Understanding policy enactment: The New Orleans Fresh Food Retailer Initiative. Am. J. Prev. Med. 2012, 43, S116–S122. [Google Scholar] [CrossRef] [PubMed]
- Holzman, D.C. White House proposes Healthy Food Financing Initiative. Environ. Health Perspect. 2010, 118. [Google Scholar] [CrossRef] [PubMed]
- US Department of Health & Human Services Office of Community Services. Healthy Food Financing Initiative. 2016. Available online: http://www.acf.hhs.gov/ocs/programs/community-economic-development/healthy-food-financing (accessed on 28 July 2016).
- Karpyn, A.; Young, C.; Weiss, S. Re-establishing healthy food retail: Changing the landscape of food deserts. Child. Obes. 2012, 8, 28–30. [Google Scholar] [CrossRef] [PubMed]
- Rimkus, L.; Powell, L.M.; Zenk, S.N.; Han, E.; Ohri-Vachaspati, P.; Pugach, O.; Barker, D.C.; Resnick, E.A.; Quinn, C.M.; Myllyluoma, J.; et al. Development and reliability testing of a food store observation form. J. Nutr. Educ. Behav. 2013, 45, 540–548. [Google Scholar] [CrossRef] [PubMed]
- US Department of Agriculture. Enhancing Retailer Standards in Supplemental Nutrition Assistance Program (SNAP). 2017. Available online: https://www.fns.usda.gov/snap/enhancing-retailer-standards-supplemental-nutrition-assistance-program-snap (accessed on 20 September 2017).
- Grigsby-Toussaint, D.S.; Zenk, S.N.; Odoms-Young, A.; Ruggiero, L.; Moise, I. Availability of commonly consumed and culturally specific fruits and vegetables in African-American and Latino neighborhoods. J. Am. Diet. Assoc. 2010, 110, 746–752. [Google Scholar] [CrossRef] [PubMed]
- Dubowitz, T.; Ncube, C.; Leuschner, K.; Tharp-Gilliam, S. A natural experiment opportunity in two low-income urban food desert communities: Research design, community engagement methods, and baseline results. Health Educ. Behav. 2015, 42, S87–S96. [Google Scholar] [CrossRef] [PubMed]
- Dubowitz, T.; Zenk, S.N.; Ghosh-Dastidar, B.; Cohen, D.A.; Beckman, R.; Hunter, G.; Steiner, E.D.; Collins, R.L. Healthy food access for urban food desert residents: Examination of the food environment, food purchasing practices, diet, and body mass index. Public Health Nutr. 2015, 18, 2220–2230. [Google Scholar] [CrossRef] [PubMed]
- Dubowitz, T.; Ghosh-Dastidar, M.; Cohen, D.A.; Beckman, R.; Steiner, E.D.; Hunter, G.P.; Florez, K.R.; Huang, C.; Vaughan, C.A.; Sloan, J.C.; et al. Diet and Perceptions Change with Supermarket Introduction in a Food Desert, but Not Because of Supermarket Use. Health Aff. 2015, 34, 1858–1868. [Google Scholar] [CrossRef] [PubMed]
- Harries, C.; Koprak, J.; Young, C.; Weiss, S.; Parker, K.M.; Karpyn, A. Moving from policy to implementation: A methodology and lessons learned to determine eligibility for healthy food financing projects. J. Public Health Manag. Pract. 2014, 20, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Fleischhacker, S.E.; Flournoy, R.; Moore, L.V. Meaningful, measurable, and manageable approaches to evaluating Healthy Food Financing Initiatives: An overview of resources and approaches. J. Public Health Manag. Pract. 2013, 19, 541–549. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Store Feature | All Stores N = 127 | Small Grocery N = 34 | Limited Service N = 93 | p-Value b | SNAP Authorized N = 108 |
|---|---|---|---|---|---|
| Limited Service Store Type: | |||||
| Convenience Store | 52.8% | - | 72.0% | - | 50.9% |
| Other a | 20.5% | - | 28.0% | - | 18.5% |
| Number of Cash Registers | 1.6 (0.9) | 1.7 (1.0) | 1.6 (0.9) | 0.64 | 1.7 (0.9) |
| Accepts SNAP Benefits | 86.4% | 100.0% | 81.5% | 0.008 | 100% |
| Butcher, Bakery, or Deli Available | 26.2% | 75.8% | 8.6% | <0.0001 | 28.7% |
| Parking On-Site Available | 54.4% | 43.8% | 58.1% | 0.16 | 52.3% |
| Presentation | All Stores N = 127 | Small Grocery N = 34 | Limited Service N = 93 | p-Value a | SNAP Authorized N = 108 |
|---|---|---|---|---|---|
| Fresh: | |||||
| Number of Fruit Options | 1.8 (4.0) | 4.8 (6.0) | 0.7 (2.2) | <0.0001 | 1.7 (3.7) |
| Number of Vegetable Options | 2.9 (4.6) | 8.8 (5.2) | 0.8 (1.7) | <0.0001 | 2.7 (4.8) |
| Frozen: | |||||
| Number of Fruit Options | 0.2 (0.9) | 0.6 (1.6) | 0 (0.0) | 0.0003 | 0.1 (0.6) |
| Number of Vegetable Options | 2.0 (2.8) | 4.8 (3.2) | 1.0 (1.8) | <0.0001 | 1.9 (3.0) |
| Canned and Shelf-Stable: | |||||
| Number of Fruit Options | 3.7 (2.3) | 5.1 (2.5) | 3.2 (2.1) | <0.0001 | 3.8 (2.4) |
| Number of Vegetable Options | 6.8 (3.3) | 8.7 (2.5) | 6.1 (3.2) | <0.0001 | 6.8 (3.1) |
| Item | All Stores N = 127 | Small Grocery N = 34 | Limited Service N = 93 | p-Value a | SNAP Authorized N = 108 |
|---|---|---|---|---|---|
| Bread: | |||||
| 100% Whole Wheat Bread | 12.1% | 21.2% | 8.8% | 0.06 | 14.2% |
| White Bread | 84.0% | 93.9% | 80.4% | 0.07 | 90.7% |
| Cereal: | |||||
| Low-Sugar (<6 g) | 55.2% | 66.7% | 51.1% | 0.12 | 59.8% |
| High-Sugar (≥6 g) | 88.8% | 90.9% | 88.0% | 0.28 | 94.4% |
| Rice: | |||||
| Brown Rice | 21.0% | 33.3% | 16.5% | 0.04 | 23.6% |
| White Rice | 88.8% | 93.9% | 87.0% | 0.28 | 90.7% |
| Cheese: | |||||
| Low or Reduced-Fat | 31.8% | 60.6% | 21.5% | <0.0001 | 35.2% |
| Regular-Fat | 46.5% | 82.4% | 33.3% | <0.0001 | 50.9% |
| Yogurt: | |||||
| Low-Fat or Non-Fat | 4.8% | 8.8% | 3.3% | 0.19 | 4.7% |
| Whole-Fat or Regular | 1.6% | 2.9% | 1.1% | 0.46 | 0.9% |
| Ground Beef: | |||||
| Extra Lean (≤10% Fat) | 6.3% | 23.5% | 0.0% | <0.0001 | 7.4% |
| Regular (≥20% Fat) | 18.1% | 67.7% | 0.0% | <0.0001 | 20.4% |
| Potato Chips (Plain): | |||||
| Baked or Low-Fat | 9.0% | 9.1% | 9.0% | 0.99 | 10.4% |
| Regular | 96.0% | 90.9% | 97.9% | 0.08 | 96.3% |
| Milk: | |||||
| 1% or Skim | 11.8% | 14.7% | 10.8% | 0.54 | 12.0% |
| Whole or 2% | 85.8% | 94.1% | 82.8% | 0.11 | 92.6% |
| Juice: | |||||
| 100% Juice | 88.7% | 84.9% | 90.1% | 0.41 | 89.6% |
| <50% Juice or Fruit Punch | 96.8% | 97.0% | 96.7% | 0.94 | 97.2% |
| Soda: | |||||
| Diet | 76.6% | 63.6% | 81.3% | 0.04 | 75.5% |
| Regular | 97.6% | 97.0% | 97.8% | 0.94 | 98.1% |
| Water: | |||||
| Plain | 98.8% | 97.0% | 98.9% | 0.45 | 99.1% |
| Enhanced | 42.7% | 27.3% | 48.4% | 0.04 | 43.4% |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Singleton, C.R.; Li, Y.; Duran, A.C.; Zenk, S.N.; Odoms-Young, A.; Powell, L.M. Food and Beverage Availability in Small Food Stores Located in Healthy Food Financing Initiative Eligible Communities. Int. J. Environ. Res. Public Health 2017, 14, 1242. https://doi.org/10.3390/ijerph14101242
Singleton CR, Li Y, Duran AC, Zenk SN, Odoms-Young A, Powell LM. Food and Beverage Availability in Small Food Stores Located in Healthy Food Financing Initiative Eligible Communities. International Journal of Environmental Research and Public Health. 2017; 14(10):1242. https://doi.org/10.3390/ijerph14101242
Chicago/Turabian StyleSingleton, Chelsea R., Yu Li, Ana Clara Duran, Shannon N. Zenk, Angela Odoms-Young, and Lisa M. Powell. 2017. "Food and Beverage Availability in Small Food Stores Located in Healthy Food Financing Initiative Eligible Communities" International Journal of Environmental Research and Public Health 14, no. 10: 1242. https://doi.org/10.3390/ijerph14101242