
Hand-Washing: The Main Strategy for Avoiding Hand, Foot and Mouth Disease

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Settings
2.2. Questionnaire and Interview
2.3. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Risk Factor Analysis
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| HFMD | hand, foot and mouth disease |
| EV71 | enterovirus 71 |
| CA16 | coxsackievirus A16 |
| CA6 | coxsackievirus A6 |
| OR | odds ratio |
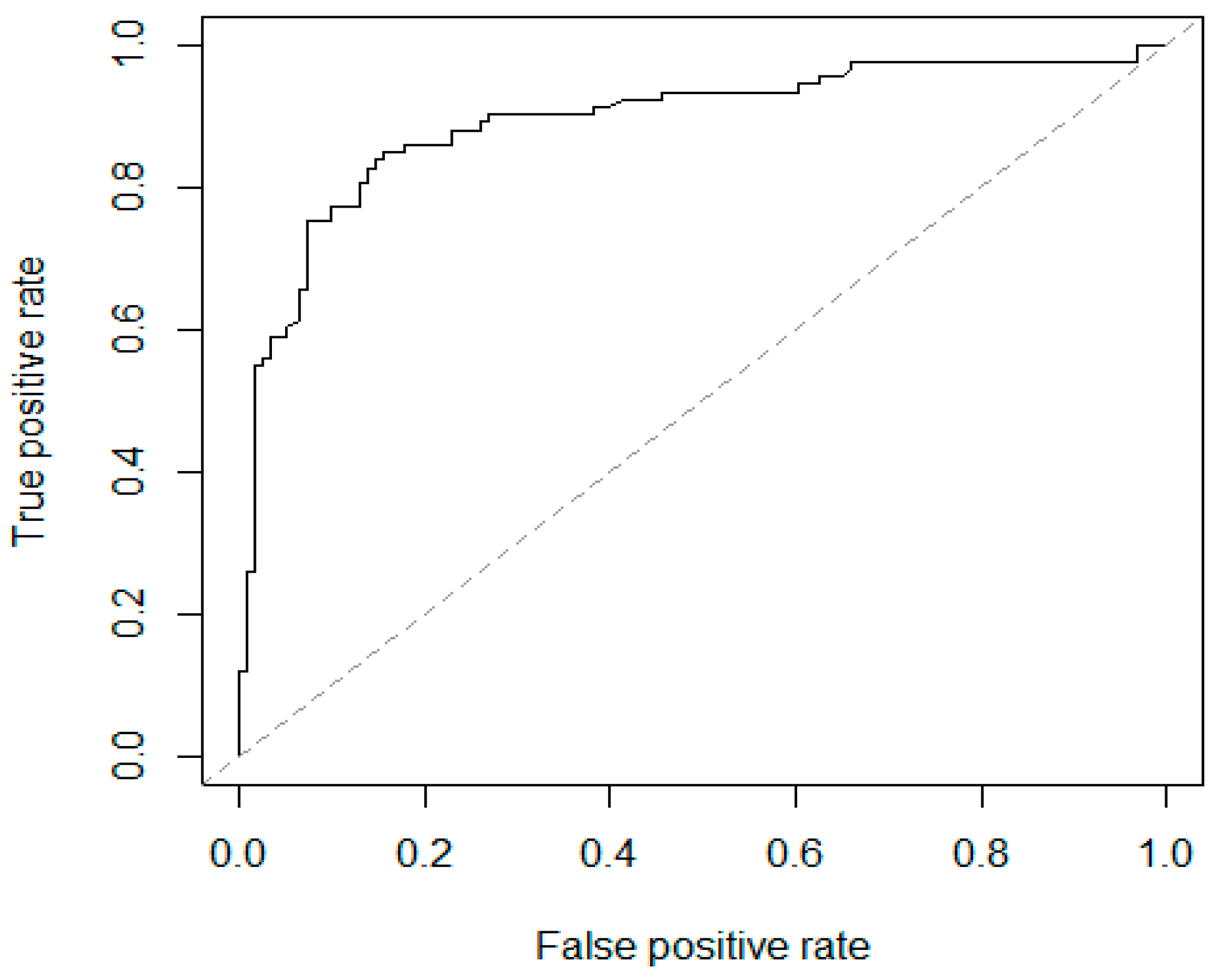
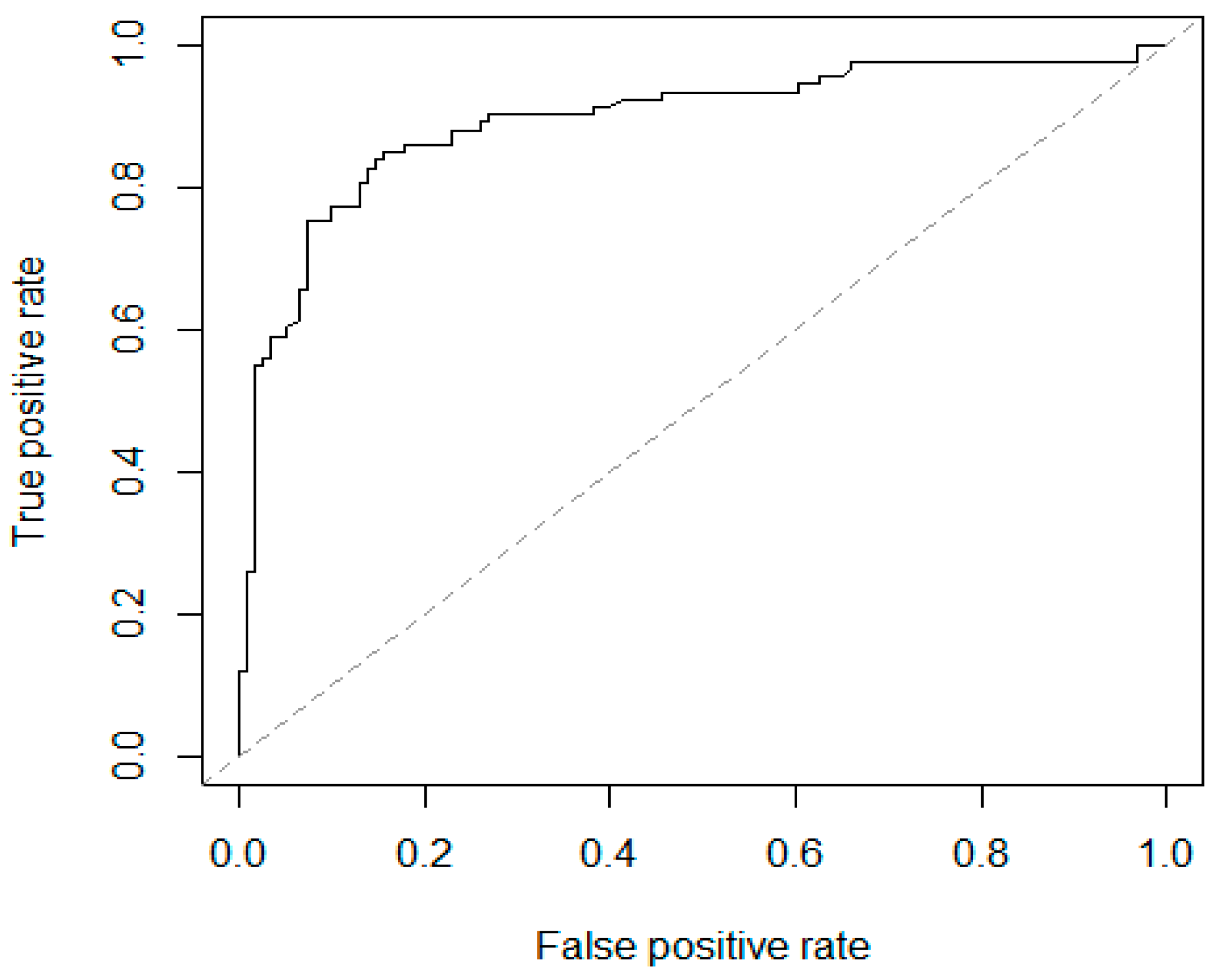
| ROC | receiver operating characteristic |
| AUC | area under the curve |
| CI | confidence interval |
References
- Bian, L.; Wang, Y.; Yao, X.; Mao, Q.; Xu, M.; Liang, Z. Coxsackievirus A6: A new emerging pathogen causing hand, foot and mouth disease outbreaks worldwide. Expert Rev. Anti-Infect. Ther. 2015, 13, 1061–1071. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Zeng, H.; Zheng, H.; Yi, L.; Guo, X.; Liu, L.; Sun, L.; Tan, X.; Li, H.; Ke, C.; et al. Hand, foot and mouth disease in guangdong, China, in 2013: New trends in the continuing epidemic. Clin. Microbiol. Infect. 2014, 20, 442–445. [Google Scholar] [CrossRef] [PubMed]
- CDC. Hand, Foot, and Mouth Disease (HFMD). Available online: http://www.cdc.gov/hand-foot-mouth/about/index.html (accessed on 16 January 2016).
- Huang, C.C.; Liu, C.C.; Chang, Y.C.; Chen, C.Y.; Wang, S.T.; Yeh, T.F. Neurologic complications in children with enterovirus 71 infection. N. Engl. J. Med. 1999, 341, 936–942. [Google Scholar] [CrossRef] [PubMed]
- WPRO. Hand, Foot and Mouth Disease. Available online: http://www.wpro.who.int/mediacentre/factsheets/fs_10072012_HFMD/en/ (accessed on 16 January 2016).
- WHO. Hand, Foot and Mouth Disease in China: Evaluating an Automated System for the Detection of Outbreaks. Available online: http://www.wpro.who.int/china/topics/hand_foot_mouth_disease/en/ (accessed on 16 January 2016).
- National Notifiable Disease Situation. Available online: http://en.nhfpc.gov.cn/diseases.html (accessed on 16 January 2016).
- Deng, T.; Huang, Y.; Yu, S.C.; Gu, J.; Huang, C.R.; Xiao, G.X.; Hao, Y.T. Spatial-temporal clusters and risk factors of hand, foot, and mouth disease at the district level in Guangdong province, China. PLoS ONE 2013, 8, e56943. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.C.; Meng, F.Y.; Li, J.X.; Li, X.L.; Mao, Q.Y.; Tao, H.; Zhang, Y.T.; Yao, X.; Chu, K.; Chen, Q.H.; et al. Efficacy, safety, and immunology of an inactivated alum-adjuvant enterovirus 71 vaccine in children in China: A multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2013, 381, 2024–2032. [Google Scholar] [CrossRef]
- Liu, C.-C.; Chow, Y.-H.; Chong, P.; Klein, M. Prospect and challenges for the development of multivalent vaccines against hand, foot and mouth diseases. Vaccine 2014, 32, 6177–6182. [Google Scholar] [CrossRef] [PubMed]
- Hii, Y.L.; Rocklov, J.; Ng, N. Short term effects of weather on hand, foot and mouth disease. PLoS ONE 2011, 6, e16796. [Google Scholar] [CrossRef] [PubMed]
- Ma, E.; Wong, S.; Wong, C.; Chuang, S.K.; Tsang, T. Effects of public health interventions in reducing transmission of hand, foot, and mouth disease. Pediat. Inf. Dis. J. 2011, 30, 432–435. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.H.; Chongsuvivatwong, V.; Tan, Y.; Tang, Z.Z.; Sornsrivichai, V.; McNeil, E.B. Important roles of public playgrounds in the transmission of hand, foot, and mouth disease. Epidemiol. Infect. 2015, 143, 1432–1441. [Google Scholar] [CrossRef] [PubMed]
- Ruan, F.; Yang, T.; Ma, H.; Jin, Y.; Song, S.; Fontaine, R.E.; Zhu, B.P. Risk factors for hand, foot, and mouth disease and herpangina and the preventive effect of hand-washing. Pediatrics 2011, 127, e898–e904. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Sun, L.; Lin, J.; He, J.; Deng, A.; Kang, M.; Zeng, H.; Ma, W.; Zhang, Y. Protective effect of exclusive breastfeeding against hand, foot and mouth disease. BMC Infect. Disease. 2014, 14, 645. [Google Scholar] [CrossRef] [PubMed]
- The Ministry of Health of the People’s Republic of China. Guideline for the Diagnosis and Treatment of Hand Foot and Mouth Disease, 2010 ed.The Ministry of Health of the People’s Republic of China: Beijing, China, 2010.
- Hanley, J.A.; McNeil, B.J. The meaning and use of the area under a receiver operating characteristic (roc) curve. Radiology 1982, 143, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Salo, R.J.; Cliver, D.O. Effect of acid pH, salts, and temperature on the infectivity and physical integrity of enteroviruses. Arch. Virol. 1976, 52, 269–282. [Google Scholar] [CrossRef] [PubMed]
- Solomon, T.; Lewthwaite, P.; Perera, D.; Cardosa, M.J.; McMinn, P.; Ooi, M.H. Virology, epidemiology, pathogenesis, and control of enterovirus 71. Lancet Infect. Disease. 2010, 10, 778–790. [Google Scholar] [CrossRef]
- Luby, S.P.; Agboatwalla, M.; Feikin, D.R.; Painter, J.; Billhimer, W.; Altaf, A.; Hoekstra, R.M. Effect of handwashing on child health: A randomised controlled trial. Lancet 2005, 366, 225–233. [Google Scholar] [CrossRef]
- Washing Hands Frequently, Eating Cooked Food, Drinking Boiled Water, Better Ventilation and Sun Exposure Can Be Effective in Preventing Infectious Disease. Available online: http://www.gov.cn/zxft/ft109/content_958671.htm (accessed on 19 January 2016).
- Chung, P.-W.; Huang, Y.-C.; Chang, L.-Y.; Lin, T.-Y.; Ning, H.-C. Duration of enterovirus shedding in stool. J. Microbiol. Immunol. Infect. 2001, 34, 167–170. [Google Scholar] [PubMed]
- Bible, J.M.; Iturriza-Gomara, M.; Megson, B.; Brown, D.; Pantelidis, P.; Earl, P.; Bendig, J.; Tong, C.W. Molecular epidemiology of human enterovirus 71 in the united kingdom from 1998 to 2006. J. Clin. Microbiol. 2008, 46, 3192–3200. [Google Scholar] [CrossRef] [PubMed]
- Lund, E. Oxidative inactivation of adenovirus. Arch. Virol. 1996, 19, 32–37. [Google Scholar] [CrossRef]
- Hand, Foot and Mouth Disease—Daily Prevention. Available online: http://www.szcdc.net/rdzt/szkbzt/zyzz/201408/t20140807_2542801.htm (accessed on 16 January 2016).
- Benakappa, A.D.; Shivamurthy, P. Beliefs regarding diet during childhood illness. Indian J. Community Med. 2012, 37, 20–24. [Google Scholar] [PubMed]

{kind=link}
| Characteristics | Cases (n = 96) | Controls (n = 126) | p Value |
|---|---|---|---|
| Male | 34 | 58 | 0.88 |
| Age, years (mean ± SD) | 2.92 ± 1.68 | 5.59 ± 1.53 | <0.01 |
| Risk Factor | Case (n = 96) | Control (n = 126) | OR | 95% CI | Adjusted OR | Adjusted 95% CI | |
|---|---|---|---|---|---|---|---|
| Socio-economic factor | |||||||
| Education | School children | 3 | 9 | 0.81 | 0.02–0.34 | 3.31 | 0.43–25.46 |
| Preschool children | 30 | 101 | 0.72 | 0.04–0.14 | 0.85 | 0.27–2.66 | |
| Children raised at home | 62 | 15 | 1 | - | 1 | - | |
| Whether the child is permanent resident or floating population | Permanent resident | 78 | 120 | 0.72 | 0.02–0.32 | 0.18 | 0.03–1.04 |
| Floating population a | 18 | 2 | 1 | - | 1 | - | |
| Any other children in the family | Yes | 49 | 64 | 0.98 | 0.57–1.67 | 1.17 | 0.58-2.36 |
| No | 47 | 60 | 1 | - | 1 | - | |
| Who is the caregiver | Father | 6 | 4 | 3 | 0.20–45.24 | 20.50 | 0.82–514.48 |
| Mother | 51 | 75 | 1.36 | 0.12–15.40 | 3.49 | 0.22–55.47 | |
| Grandparents | 38 | 43 | 1.77 | 0.15–20.27 | 5.03 | 0.31–82.46 | |
| Baby-sitter | 1 | 2 | 1 | - | 1 | - | |
| Clinical factor | |||||||
| Birth weight | - | - | - | 0.80 | 0.51–1.23 | 0.61 | 0.34–1.09 |
| Recent vaccination history | Yes | 41 | 18 | 4.33 | 2.26–8.30 | 1.58 | 0.63–3.95 |
| No | 51 | 97 | 1 | - | 1 | - | |
| Recent history of common cold and diarrhea | Yes | 37 | 46 | 1.06 | 0.61–1.84 | 0.91 | 0.5–1.88 |
| No | 59 | 78 | 1 | - | 1 | - | |
| History of HFMD | Yes | 6 | 22 | 0.31 | 0.12–0.80 | 0.33 | 0.11–1.03 |
| No | - | - | 1 | - | 1 | - | |
| Behavior factor | |||||||
| History of Cold food consumption b | Yes | 24 | 68 | 0.28 | 0.16–0.51 | 0.42 | 0.20–0.88 |
| No | 69 | 55 | 1 | - | 1 | - | |
| Whether he/she has been exposed to populated places | Yes | 58 | 57 | 1.87 | 1.09–3.22 | 1.35 | 0.67–2.74 |
| No | 37 | 68 | 1 | - | 1 | - | |
| Sharing toys with other children | Yes | 73 | 91 | 1.24 | 0.67–2.30 | 1.79 | 0.77–4.17 |
| No | 22 | 34 | 1 | - | 1 | - | |
| History of contact with common cold or diarrhea patients | Yes | 29 | 20 | 2.9 | 1.49–5.67 | 2.10 | 0.87–5.09 |
| No | 47 | 94 | 1 | - | 1 | - | |
| Medical-seeking conditions | Yes | 31 | 35 | 1.28 | 0.72–2.29 | 1.27 | 0.59–2.72 |
| No | 63 | 91 | 1 | - | 1 | - | |
| Recent history of hospital visit (Family members) | Yes | 35 | 39 | 1.28 | 0.73–2.24 | 1.45 | 0.68–3.08 |
| No | 61 | 87 | 1 | - | 1 | - | |
| Hand-washing before meals | Often | 50 | 102 | 0.54 | 0.01–0.44 | 0.41 | 0.19–0.89 |
| Seldom or not | 46 | 24 | 1 | - | 1 | - | |
| Hand-washing after toilet use | Often | 60 | 102 | 0.39 | 0.21–0.72 | 0.79 | 0.35–1.75 |
| Seldom or not | 36 | 24 | 1 | - | 1 | - | |
| Habits of airing out bedding | More than thrice | 27 | 9 | 3.18 | 1.16–8.67 | 3.83 | 1.08–13.58 |
| Thrice | 12 | 14 | 0.91 | 0.33–2.51 | 2.38 | 0.59–9.63 | |
| Twice | 16 | 19 | 0.90 | 0.35–2.28 | 2.90 | 0.78–10.76 | |
| Once | 24 | 66 | 0.39 | 0.17–0.87 | 1.37 | 0.45–4.21 | |
| Less than once | 17 | 18 | 1 | - | 1 | - | |
| Whether there is a dedicated towel for the child | Yes | 90 | 124 | 0.24 | 0.05–1.23 | 0.68 | 0.10–4.79 |
| No | 6 | 2 | 1 | - | 1 | - | |
| Pacifier-using | Yes | 49 | 23 | 4.62 | 2.53–8.46 | 0.78 | 0.32–1.89 |
| No | 47 | 102 | 1 | - | 1 | - | |
| Finger-sucking conditions | Often | 30 | 7 | 10.91 | 4.36–27.26 | 3.02 | 0.89–10.30 |
| Occasionally | 33 | 34 | 2.47 | 1.32–4.62 | 1.24 | 0.56–2.73 | |
| No | 33 | 84 | 1 | - | 1 | - | |
| Risk Factor | p Value | OR | 95% CI | |
|---|---|---|---|---|
| Age | - | 0.00 | 0.44 | 0.34–0.56 |
| History of cold food consumption | Yes | 0.06 | 0.47 | 0.22–1.02 |
| No | - | 1 | - | |
| Hand-washing before meals | Often | 0.01 | 0.30 | 0.13–0.70 |
| Seldom or not | - | 1 | - | |
| Habits of airing out bedding | More than thrice | 0.03 | 4.55 | 1.19–17.37 |
| Thrice | 0.14 | 3.23 | 0.68–15.31 | |
| Twice | 0.11 | 3.10 | 0.78–12.34 | |
| Once | 0.31 | 1.84 | 0.56–6.04 | |
| Less than once | - | 1 | - | |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, D.; Li, Z.; Zhang, W.; Guo, P.; Ma, Z.; Chen, Q.; Du, S.; Peng, J.; Deng, Y.; Hao, Y. Hand-Washing: The Main Strategy for Avoiding Hand, Foot and Mouth Disease. Int. J. Environ. Res. Public Health 2016, 13, 610. https://doi.org/10.3390/ijerph13060610
Zhang D, Li Z, Zhang W, Guo P, Ma Z, Chen Q, Du S, Peng J, Deng Y, Hao Y. Hand-Washing: The Main Strategy for Avoiding Hand, Foot and Mouth Disease. International Journal of Environmental Research and Public Health. 2016; 13(6):610. https://doi.org/10.3390/ijerph13060610
Chicago/Turabian StyleZhang, Dingmei, Zhiyuan Li, Wangjian Zhang, Pi Guo, Zhanzhong Ma, Qian Chen, Shaokun Du, Jing Peng, Yu Deng, and Yuantao Hao. 2016. "Hand-Washing: The Main Strategy for Avoiding Hand, Foot and Mouth Disease" International Journal of Environmental Research and Public Health 13, no. 6: 610. https://doi.org/10.3390/ijerph13060610