
A Preliminary Assessment of the Role of Ambient Nitric Oxide Exposure in Hospitalization with Respiratory Syncytial Virus Bronchiolitis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Health Data
2.2. NO Concentration Data
2.3. Climate Data
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| RSV | Respiratory syncytial virus |
| NO | Nitrogen Oxide |
| OR | Odds ratio |
References
- Gibson, G.J.; Loddenkemper, R.; Sibille, Y.; Lundback, B. The European Lung White Book: Respiratory Health and Disease in Europe; European Respiratory Society: Lausanne, Switzerland, 2013. [Google Scholar]
- Everard, M.L. Respiratory syncytial virus bronchiolitis and pneumonia. In Pediatric Respiratory Medicine; Taussig, L.M., Ed.; Mosby, Elsevier Health Sciences: St. Louis, MO, USA, 2008; pp. 491–499. [Google Scholar]
- Hall, C.B.; Simoes, E.A.; Anderson, L.J. Clinical and epidemiologic features of respiratory syncytial virus. Curr. Top. Microbiol. Immunol. 2013, 372, 39–57. [Google Scholar] [PubMed]
- Nair, H.; Nokes, D.J.; Gessner, B.D.; Dherani, M.; Madhi, S.A.; Singleton, R.J.; O’Brien, K.L.; Roca, A.; Wright, P.F.; Bruce, N.; et al. Global burden of acute lower respiratory infections due to respiratory syncytial virus in young children: A systematic review and meta-analysis. Lancet 2010, 375, 1545–1555. [Google Scholar] [CrossRef]
- Health Protection Agency. (Archived Content) HPA—Weekly Laboratory Reports of Respiratory Syncytial Virus; Health Protection Agency: London, UK, 2013.
- Simoes, E.A.F. Environmental and demographic risk factors for respiratory syncytial virus lower respiratory tract disease. J. Pediatr. 2003, 143 (Suppl. 5), 118–126. [Google Scholar] [CrossRef]
- Meerhoff, T.J.; Paget, J.W.; Kimpen, J.L.; Schellevis, F. Variation of respiratory syncytial virus and the relation with meteorological factors in different winter seasons. Pediatr. Infect. Dis. J. 2009, 28, 860–866. [Google Scholar] [CrossRef] [PubMed]
- Hervas, D.; Reina, J.; Hervas, J.A. Meteorologic conditions and respiratory syncytial virus activity. Pediatr. Infect. Dis. J. 2012, 31, e176–e181. [Google Scholar] [CrossRef] [PubMed]
- Ohuma, E.O.; Okiro, E.A.; Ochola, R.; Sande, C.J.; Cane, P.A.; Medley, G.F.; Bottomley, C.; Nokes, D.J. The natural history of respiratory syncytial virus in a birth cohort: The influence of age and previous infection on reinfection and disease. Am. J. Epidemiol. 2012, 176, 794–802. [Google Scholar] [CrossRef] [PubMed]
- Clarke, S.K.R.; Gardner, P.S.; Poole, P.M.; Simpson, H.; Tobin, J.O.H. Respiratory syncytial virus infection: admissions to hospital in industrial, urban, and rural areas. Report to the Medical Research Council Subcommittee on Respiratory Syncytial Virus Vaccines. Br. Med. J. 1978, 2, 796–798. [Google Scholar]
- Brandenburg, A.H.; Jeannet, P.Y.; v Steensel-Moll, H.A.; Ott, A.; Rothbarth, P.H.; Wunderli, W.; Suter, S.; Neijens, H.J.; Osterhaus, A.D.; Siegrist, C.A. Local variability in respiratory syncytial virus disease severity. Arch. Dis. Child. 1997, 77, 410–414. [Google Scholar] [CrossRef] [PubMed]
- Vandini, S.; Corvaglia, L.; Alessandroni, R.; Aquilano, G.; Marsico, C.; Spinelli, M.; Lanari, M.; Faldella, G. Respiratory syncytial virus infection in infants and correlation with meteorological factors and air pollutants. Ital. J. Pediatr. 2013, 39, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Segala, C.; Poizeau, D.; Mesbah, M.; Willems, S.; Maidenberg, M. Winter air pollution and infant bronchiolitis in Paris. Environ. Res. 2008, 106, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Karr, C.; Lumley, T.; Schreuder, A.; Davis, R.; Larson, T.; Ritz, B.; Kaufman, J. Effects of subchronic and chronic exposure to ambient air pollutants on infant bronchiolitis. Am. J. Epidemiol. 2007, 165, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Karr, C.J.; Rudra, C.B.; Miller, K.A.; Gould, T.R.; Larson, T.; Sathyanarayana, S.; Koenig, J.Q. Infant exposure to fine particulate matter and traffic and risk of hospitalization for RSV bronchiolitis in a region with lower ambient air pollution. Environ. Res. 2009, 109, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Derwent, R.G.; Middleton, D.R.; Field, R.A.; Goldstone, M.E.; Lester, J.N.; Perry, R. Analysis and interpretation of air quality data from an urban roadside location in Central London over the period from July 1991 to July 1992. Atmos. Environ. 1995, 29, 923–946. [Google Scholar] [CrossRef]
- Bhatt, J.M.; Everard, M.L. Do environmental pollutants influence the onset of respiratory syncytial virus epidemics or disease severity? Paediatr. Respir. Rev. 2004, 5, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.; Morton, I.; Hobson, L.; Evans, G.S.; Everard, M.L. Differentiation and immune function of human dendritic cells following infection by respiratory syncytial virus. Clin. Exp. Immunol. 2006, 143, 513–522. [Google Scholar] [CrossRef] [PubMed]
- Hobson, L.; Everard, M.L. Persistent of respiratory syncytial virus in human dendritic cells and influence of nitric oxide. Clin. Exp. Immunol. 2008, 151, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Rivera-Toledo, E.; Gomez, B. Respiratory syncytial virus persistence in macrophages alters the profile of cellular gene expression. Viruses 2012, 4, 3270–3280. [Google Scholar] [CrossRef] [PubMed]
- Ugonna, K.; Ugonna, K.; Bingle, C.D.; Plant, K.; Wilson, K.; Everard, M.L. Macrophages are required for dendritic cell uptake of respiratory syncytial virus from an infected epithelium. PLoS ONE 2014, 9, e91855. [Google Scholar] [CrossRef] [PubMed]
- Song, W.; Liu, G.; Bosworth, C.A.; Walker, J.R.; Megaw, G.A.; Lazrak, A.; Abraham, E.; Sullender, W.M.; Matalon, S. Respiratory syncytial virus inhibits lung epithelial Na+ channels by up-regulating inducible nitric-oxide synthase. J. Biol. Chem. 2009, 284, 7294–7306. [Google Scholar] [CrossRef] [PubMed]
- Stark, J.M.; Khan, A.M.; Chiappetta, C.L.; Xue, H.; Alcorn, J.L.; Colasurdo, G.N. Immune and functional role of nitric oxide in a mouse model of respiratory syncytial virus infection. J. Infect. Dis. 2005, 191, 387–395. [Google Scholar] [CrossRef] [PubMed]
- Sow, F.B.; Gallup, J.M.; Krishnan, S.; Patera, A.C.; Suzich, J.; Ackermann, M.R. Respiratory syncytial virus infection is associated with an altered innate immunity and a heightened pro-inflammatory response in the lungs of preterm lambs. Respir. Res. 2011, 12, 106. [Google Scholar] [CrossRef] [PubMed]
- Mgbemena, V.; Segovia, J.; Chang, T.H.; Bose, S. KLF6 and iNOS regulates apoptosis during respiratory syncytial virus infection. Cell. Immunol. 2013, 283, 1–7. [Google Scholar] [CrossRef] [PubMed]
- DEFRA. Air Quality Expert Group. Nitrogen Dioxide in the United Kingdom; Department for Environment, Food and Rural Affairs: London, UK, 2004.
- UK Meteorological Office. MIDAS Land Surface Stations Data (1853-Current), (Internet). NCAS British Atmospheric Data Centre, 2006. Available online: http://badc.nerc.ac.uk/view/badc.nerc.ac.uk__ATOM__dataent_ukmo-midas (accessed on 2 July 2015). [Google Scholar]
- Maclure, M. The case-crossover design: A method for studying transient effects on the risk of acute events. Am. J. Epidemiol. 1991, 133, 144–153. [Google Scholar] [PubMed]
- Lee, J.T.; Schwartz, J. Reanalysis of the effects of air pollution on daily mortality in Seoul, Korea: A case-crossover design. Environ. Health Perspect. 1999, 107, 633–636. [Google Scholar] [CrossRef] [PubMed]
- Jaakkola, J.J. Case-crossover design in air pollution epidemiology. Eur. Respir. J. Suppl. 2003, 40, 81s–85s. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A., III; Muhlestein, J.B.; May, H.T.; Renlund, D.G.; Anderson, J.L.; Horne, B.D. Ischemic heart disease events triggered by short-term exposure to fine particulate air pollution. Circulation 2006, 114, 2443–2448. [Google Scholar] [CrossRef] [PubMed]
- Bhaskaran, K.; Hajat, S.; Armstrong, B.; Haines, A.; Herrett, E.; Wilkinson, P.; Smeeth, L. The effects of hourly differences in air pollution on the risk of myocardial infarction: Case crossover analysis of the MINAP database. BMJ 2011, 343, d5531. [Google Scholar] [CrossRef] [PubMed]
- Breslow, N.E.; Day, N.E.; Schlesselman, J.J. Statistical methods in cancer research. Volume I—The analysis of case-control studies. J. Occup. Environ. Med. 1982, 24, 255–257. [Google Scholar]
- Armstrong, B.G.; Gasparrini, A.; Tobias, A. Conditional Poisson models: A flexible alternative to conditional logistic case cross-over analysis. BMC Med. Res. Methodol. 2014, 14, 122. [Google Scholar] [CrossRef] [PubMed]
- Braga, A.L.; Zanobetti, A.; Schwartz, J. The effect of weather on respiratory and cardiovascular deaths in 12 U.S. cities. Environ. Health Perspect. 2002, 110, 859–863. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, B. Models for the relationship between ambient temperature and daily mortality. Epidemiology 2006, 17, 624–631. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2012; ISBN 3-900051-07-0. Available online: http://www.R-project.org (accessed on 16 October 2012).
- Bhaskaran, K.; Gasparrini, A.; Hajat, S.; Smeeth, L.; Armstrong, B. Time series regression studies in environmental epidemiology. Int. J. Epidemiol. 2013, 42, 1187–1195. [Google Scholar] [CrossRef] [PubMed]
- European Community (EC). Directive 2008/50/EC of the European Parliament and of the Council of 21 May 2008 on ambient air quality and cleaner air for Europe. Off. J. Eur. Union 2008, L152, 1–44. [Google Scholar]
- Bradley, J.P.; Bacharier, L.B.; Bonfiglio, J.; Schechtman, K.B.; Strunk, R.; Storch, G.; Castro, M. Severity of respiratory syncytial virus bronchiolitis is affected by cigarette smoke exposure and atopy. Pediatrics 2005, 115, e7–e14. [Google Scholar] [PubMed]
- Von Linstow, M.L.; Høgh, M.; Nordbø, S.A.; Eugen-Olsen, J.; Koch, A.; Høgh, B. A community study of clinical traits and risk factors for human metapneumovirus and respiratory syncytial virus infection during the first year of life. Eur. J. Pediatr. 2008, 167, 1125–1133. [Google Scholar] [CrossRef] [PubMed]
- DiFranza, J.R.; Masaquel, A.; Barrett, A.M.; Colosia, A.D.; Mahadevia, P.J. Systematic literature review assessing tobacco smoke exposure as a risk factor for serious respiratory syncytial virus disease among infants and young children. BMC Pediatr. 2012, 12, 81. [Google Scholar] [CrossRef] [PubMed]
- Carbonell-Estrany, X.; Fullarton, J.R.; Gooch, K.L.; Vo, P.G.; Figueras-Aloy, J.; Lanari, M.; Gouyon, J.B.; Liese, J.G. Effects of parental and household smoking on the risk of respiratory syncytial virus (RSV) hospitalization in late-preterm infants and the potential impact of RSV prophylaxis. J. Matern Fetal Neonatal Med. 2013, 26, 926–931. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, M.D.; Mansbach, J.M.; Mowad, E.; Dunn, M.; Clark, S.; Piedra, P.A.; Sullivan, A.F.; Camargo, C.A. Prenatal versus postnatal tobacco smoke exposure and intensive care use in children hospitalized with bronchiolitis. Acad. Pediatr. 2015. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Mean | Median (IQR b) | Minimum | Maximum | Number of Days |
|---|---|---|---|---|---|
| Age (days) | 132.7 (101) | 111 (43–189) | 7 | 573 | 121 |
| Admission count | 1.7 (1.9) | 1 (0–2) | 0 | 9 | 121 |
| Temperature (°C) | 6.3 (3.6) | 6.7 (3.6–9.1) | −2.3 | 13.3 | 121 |
| Relative humidity (%) | 80.3 (11.4) | 81.8 (72–88.5) | 41.8 | 98 | 101 |
| NO (μg/m3) | |||||
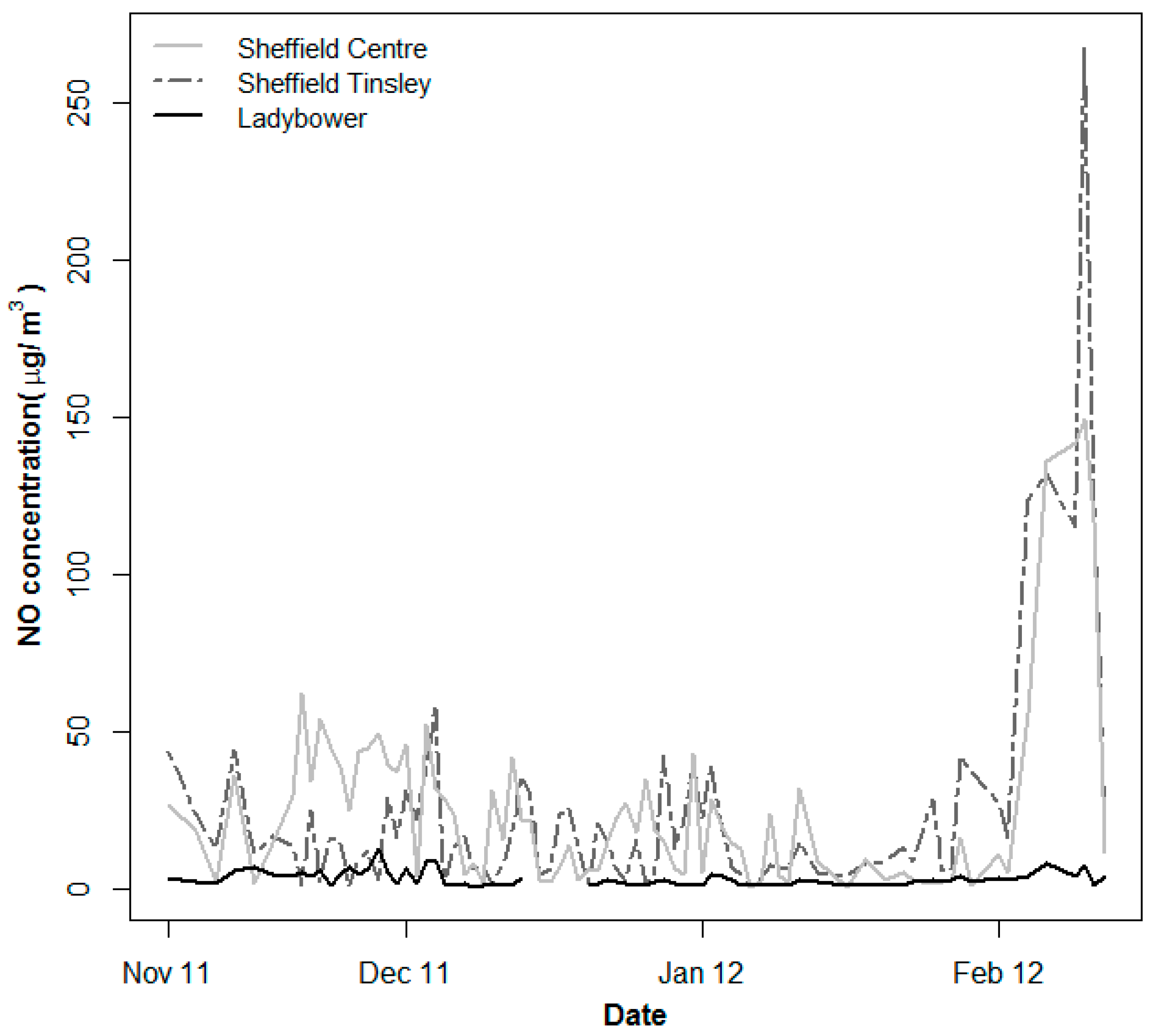
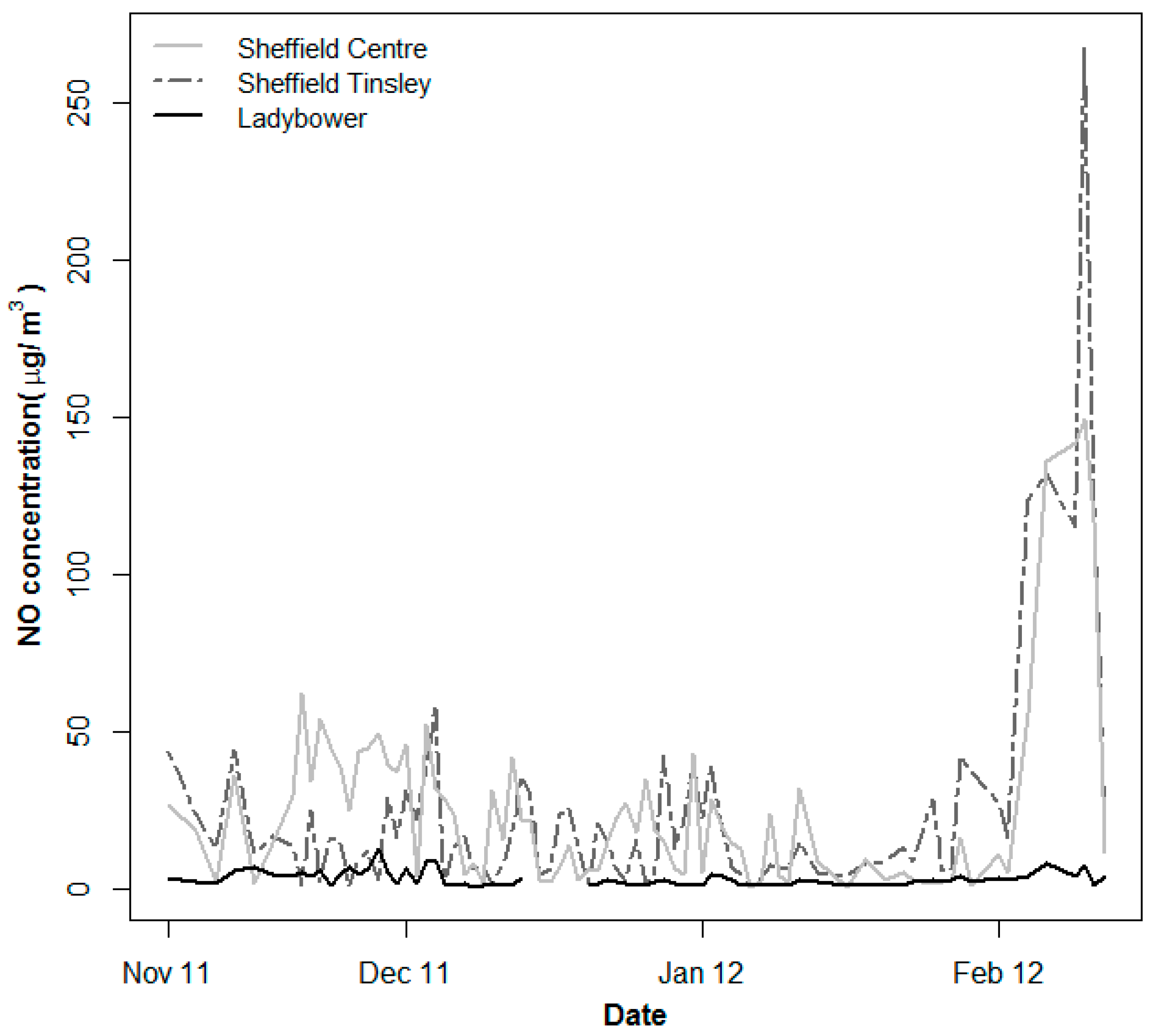
| Sheffield Centre | 26.4 (31.7) | 16.6 (5.1–36.8) | 1 | 173.2 | 120 |
| Sheffield Tinsley | 25.8 (35.1) | 15.7 (6.9–28.4) | 1.3 | 267.9 | 121 |
| Ladybower | 3.2 (2.1) | 2.5 (1.6–4.2) | 0.6 | 12.9 | 115 |
| Average | 18.6 (20.7) | 11.8 (7.2–21.1) | 1.3 | 141.8 | 114 |
| Sex (N, %) a | |||||
| Female | 99 (47.6) |
| Metric | Sheffield Centre | Average * | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
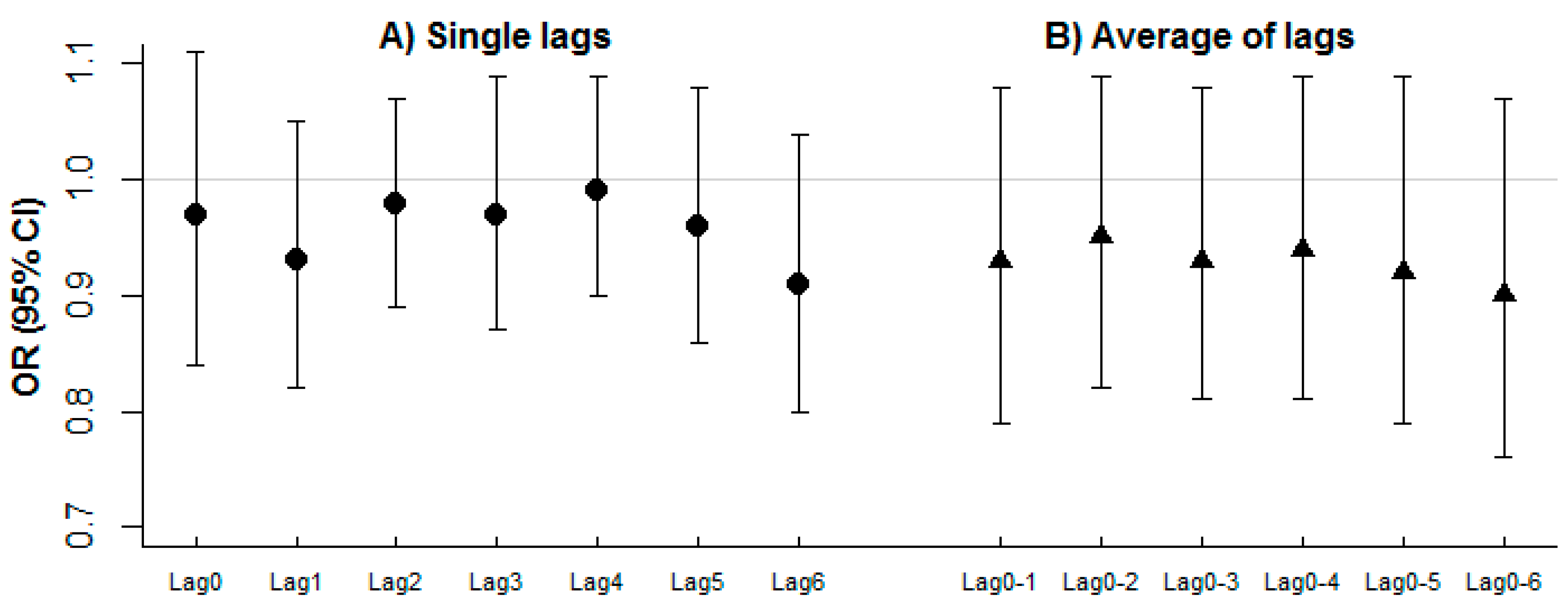
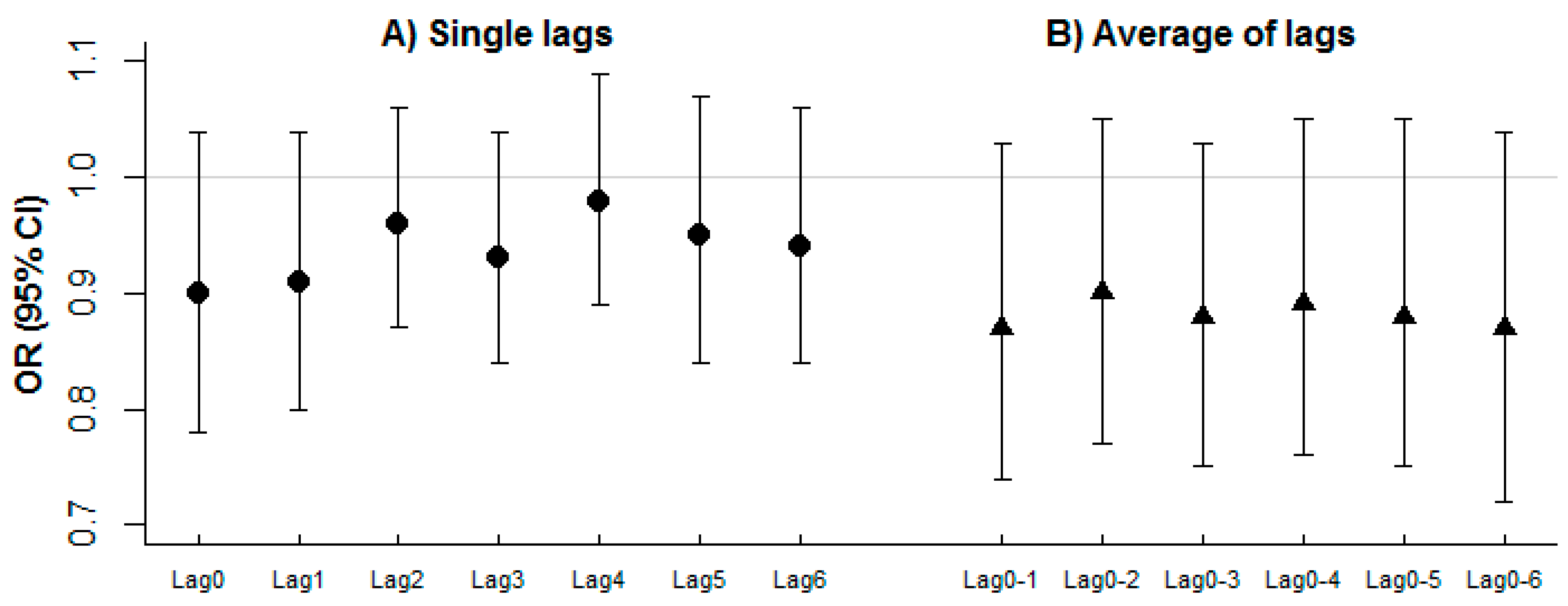
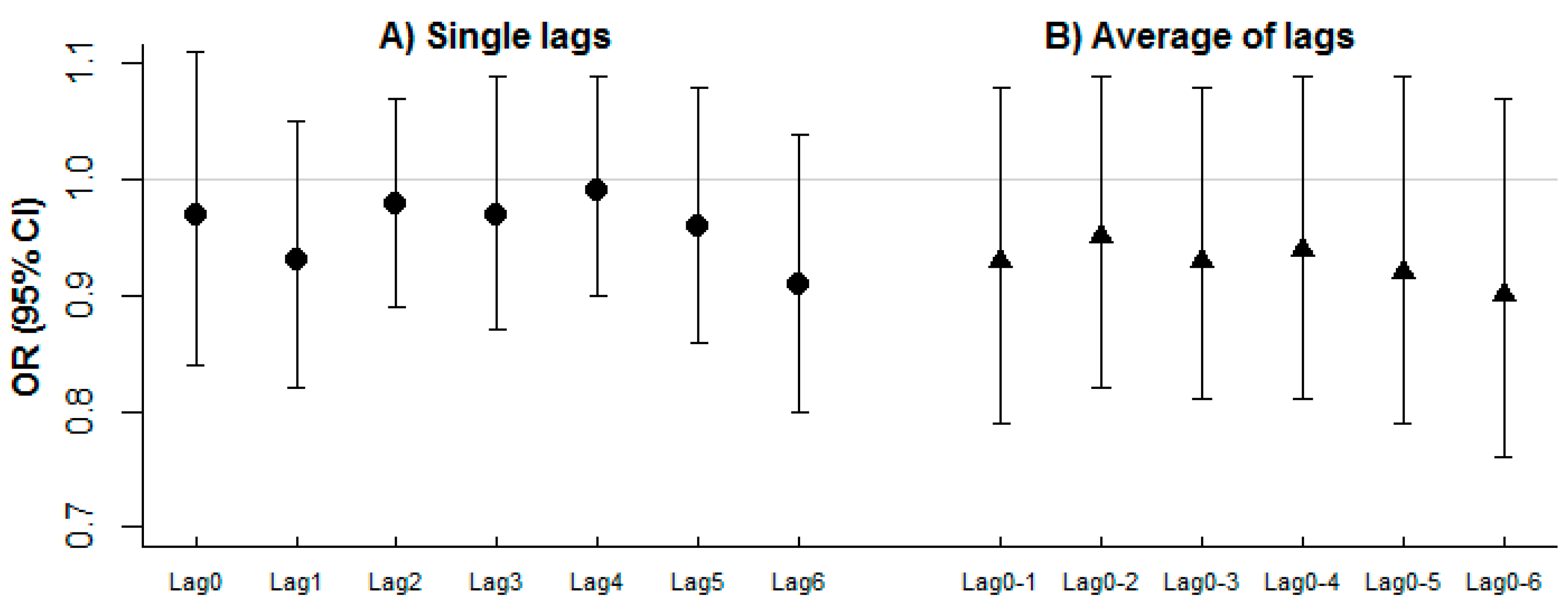
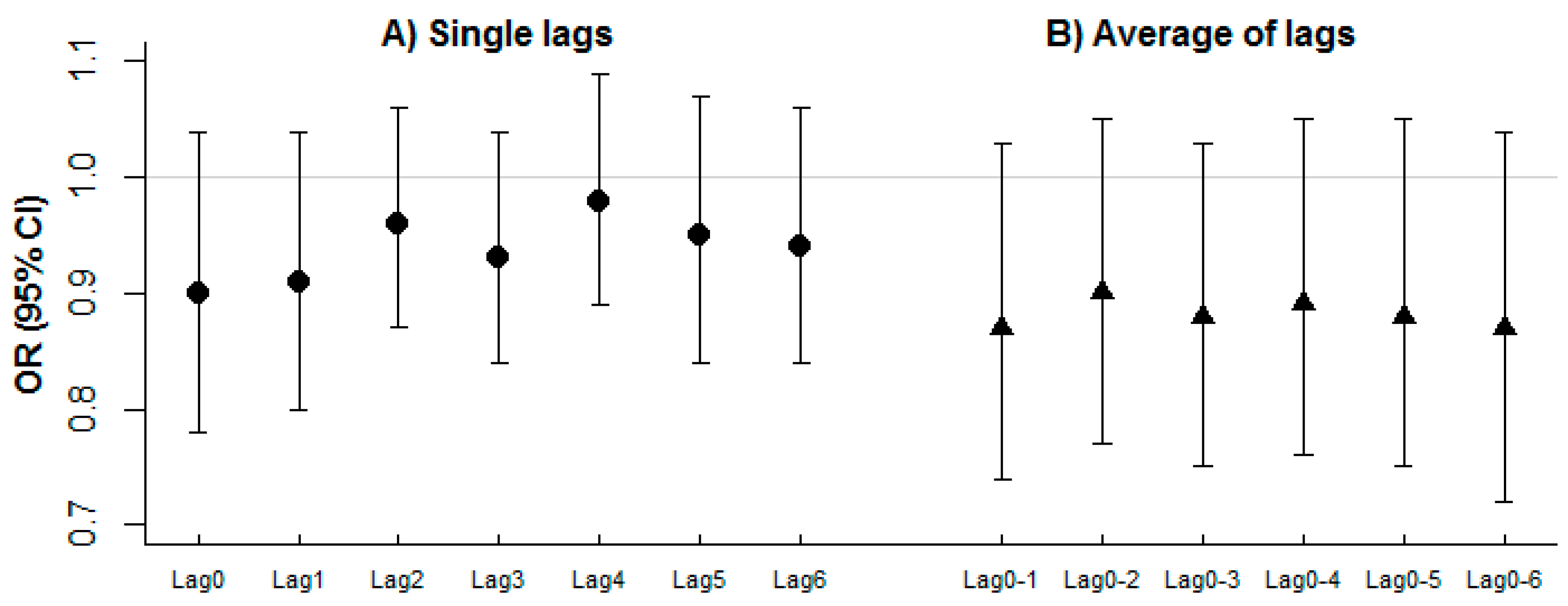
| Lag 0 | 0.94 (0.85, 1.04) | 0.23 | 0.97 (0.84, 1.11) | 0.62 |
| Lag 1 | 0.98 (0.91, 1.05) | 0.57 | 0.93 (0.82, 1.05) | 0.23 |
| Lag 2 | 0.99 (0.92, 1.05) | 0.69 | 0.98 (0.89, 1.07) | 0.59 |
| Lag 3 | 1.01 (0.95, 1.07) | 0.80 | 0.97 (0.87, 1.09) | 0.62 |
| Lag 4 | 0.99 (0.93, 1.06) | 0.80 | 0.99 (0.9, 1.09) | 0.85 |
| Lag 5 | 1.0 (0.93, 1.08) | 0.97 | 0.96 (0.86, 1.08) | 0.51 |
| Lag 6 | 0.96 (0.88, 1.04) | 0.27 | 0.91 (0.8, 1.04) | 0.16 |
| Lag 0–1 | 0.94 (0.85, 1.04) | 0.27 | 0.93 (0.79, 1.08) | 0.33 |
| Lag 0–2 | 0.95 (0.87, 1.05) | 0.34 | 0.95 (0.82, 1.09) | 0.45 |
| Lag 0–3 | 0.96 (0.87, 1.06) | 0.40 | 0.93 (0.81, 1.08) | 0.36 |
| Lag 0–4 | 0.96 (0.86, 1.06) | 0.39 | 0.94 (0.81, 1.09) | 0.39 |
| Lag 0–5 | 0.96 (0.85, 1.07) | 0.43 | 0.92 (0.79, 1.09) | 0.34 |
| Lag 0–6 | 0.93 (0.82, 1.05) | 0.24 | 0.9 (0.76, 1.07) | 0.24 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohammed, N.I.; Everard, M.L.; Ayres, J.G.; Barker, N.J.; Litchfield, I.J. A Preliminary Assessment of the Role of Ambient Nitric Oxide Exposure in Hospitalization with Respiratory Syncytial Virus Bronchiolitis. Int. J. Environ. Res. Public Health 2016, 13, 578. https://doi.org/10.3390/ijerph13060578
Mohammed NI, Everard ML, Ayres JG, Barker NJ, Litchfield IJ. A Preliminary Assessment of the Role of Ambient Nitric Oxide Exposure in Hospitalization with Respiratory Syncytial Virus Bronchiolitis. International Journal of Environmental Research and Public Health. 2016; 13(6):578. https://doi.org/10.3390/ijerph13060578
Chicago/Turabian StyleMohammed, Nuredin I., Mark L. Everard, Jon G. Ayres, Nicola J. Barker, and Ian J. Litchfield. 2016. "A Preliminary Assessment of the Role of Ambient Nitric Oxide Exposure in Hospitalization with Respiratory Syncytial Virus Bronchiolitis" International Journal of Environmental Research and Public Health 13, no. 6: 578. https://doi.org/10.3390/ijerph13060578