
Lung Cancer Mortality and Topography: A Xuanwei Case Study


Abstract
:
1. Introduction
2. Methods
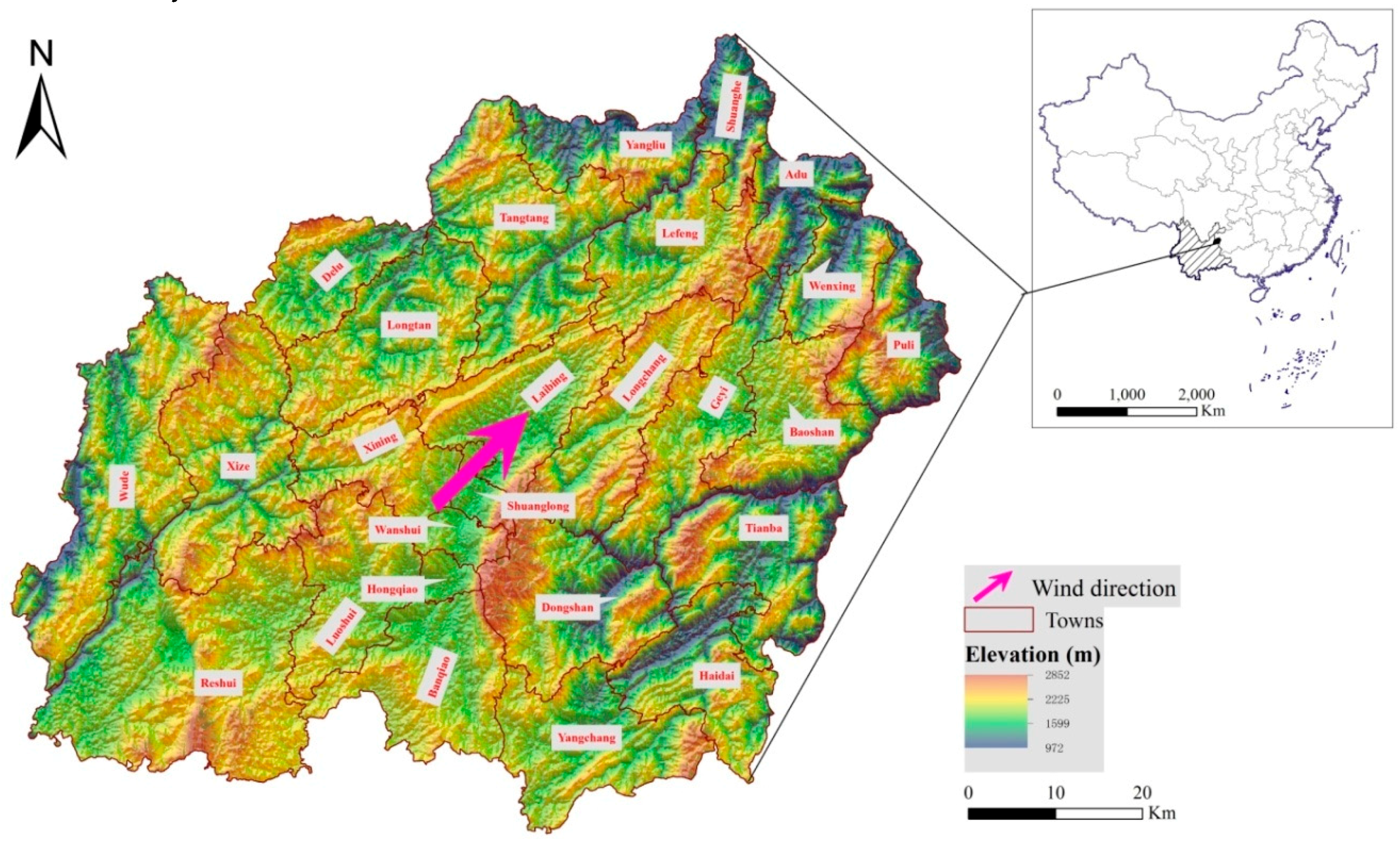
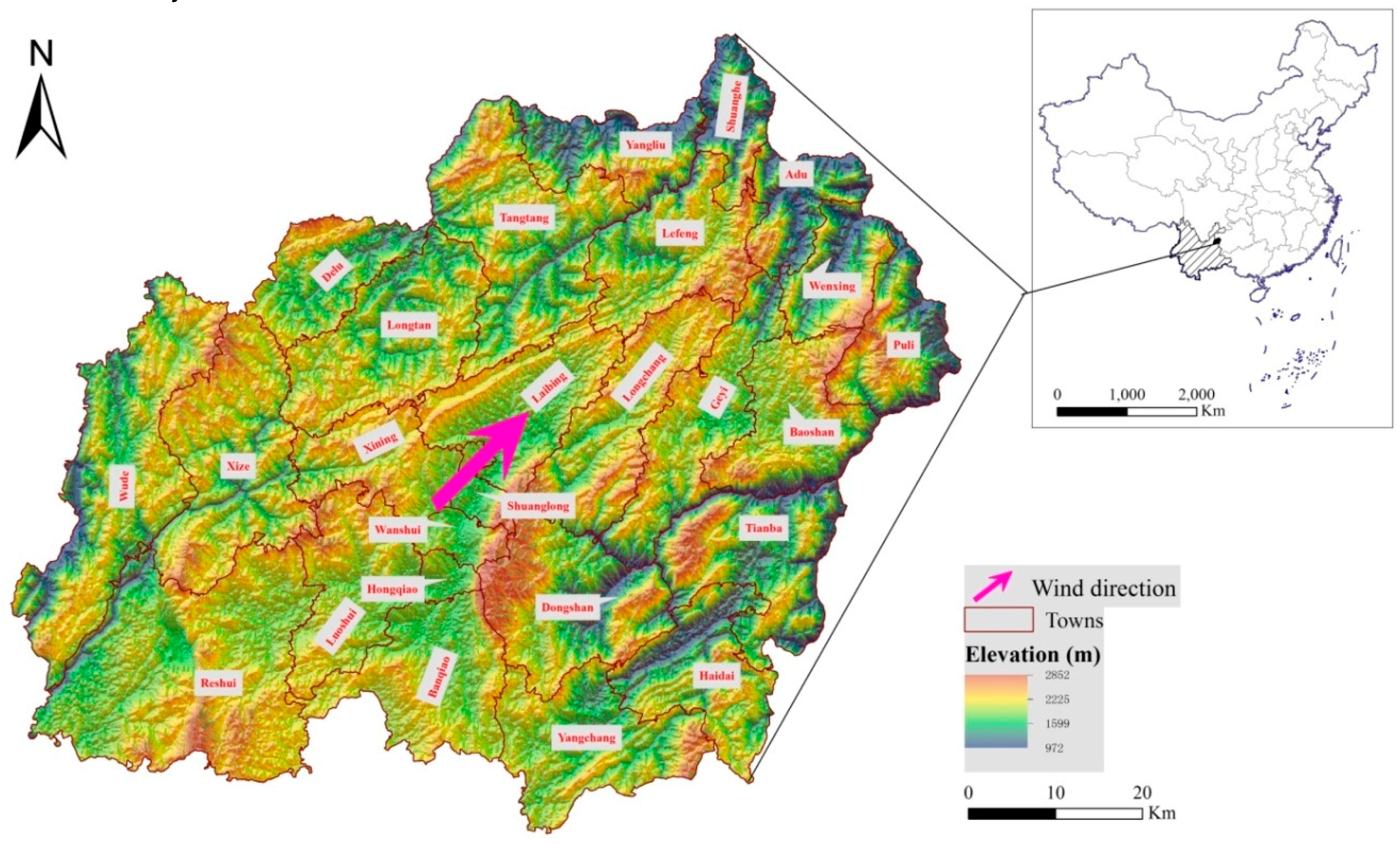
2.1. Study Area
2.2. Data Collection
2.2.1. Topographic Conditions
2.2.2. Lung Cancer Mortality Data
2.2.3. Statistical Analysis
2.3. Spatial Analysis
2.3.1. Spatial Autocorrelation
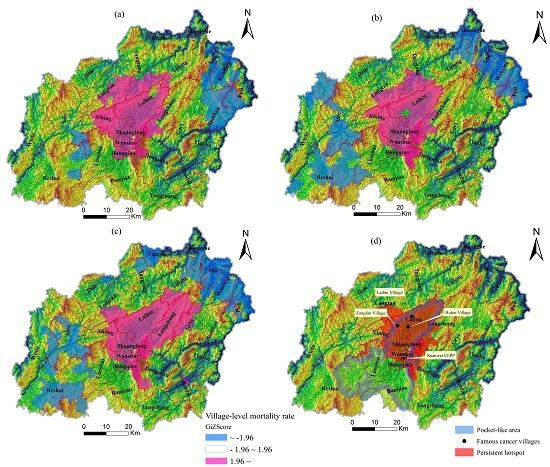
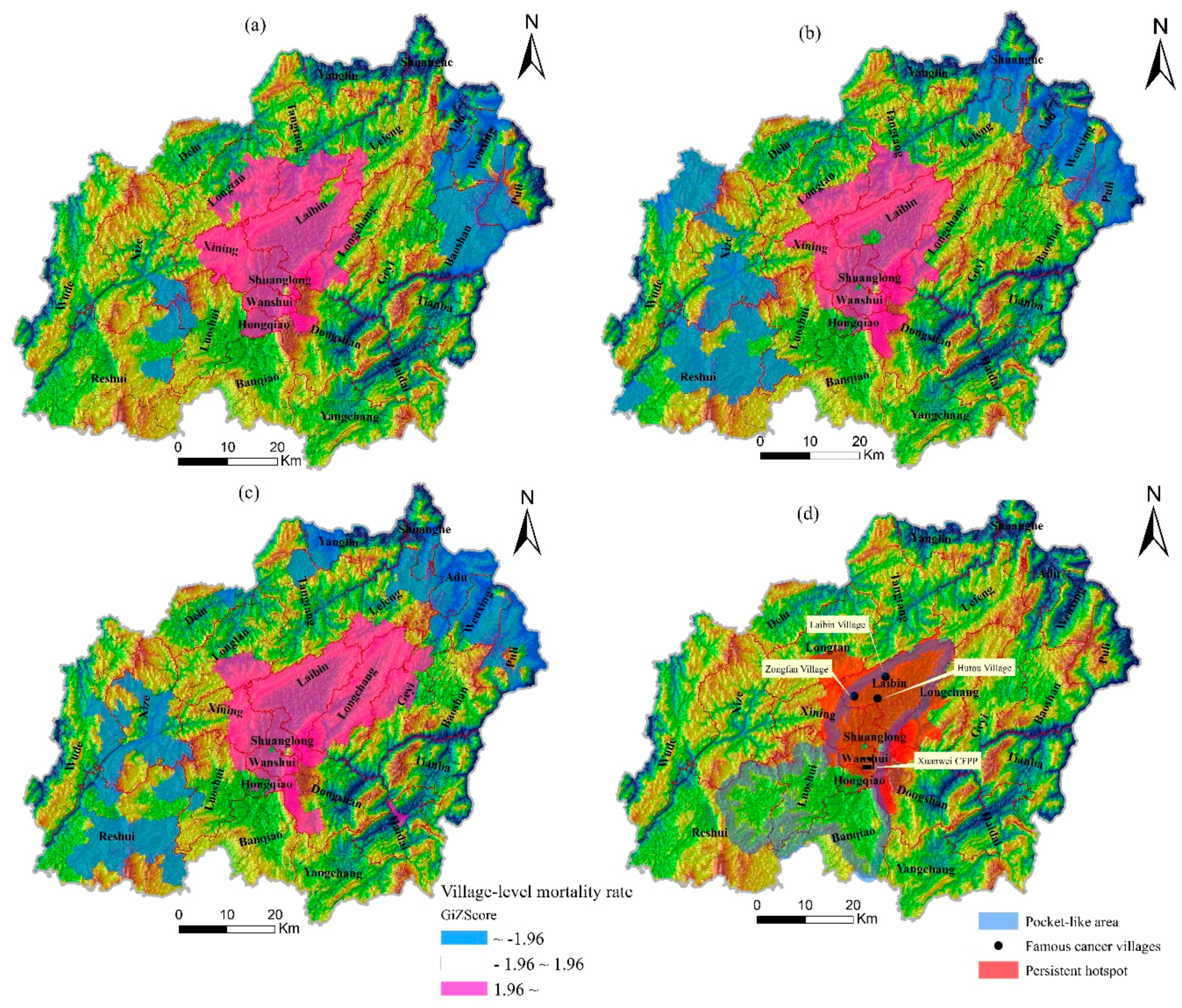
2.3.2. Hotspot Analysis
3. Results
3.1. Descriptive Statistics
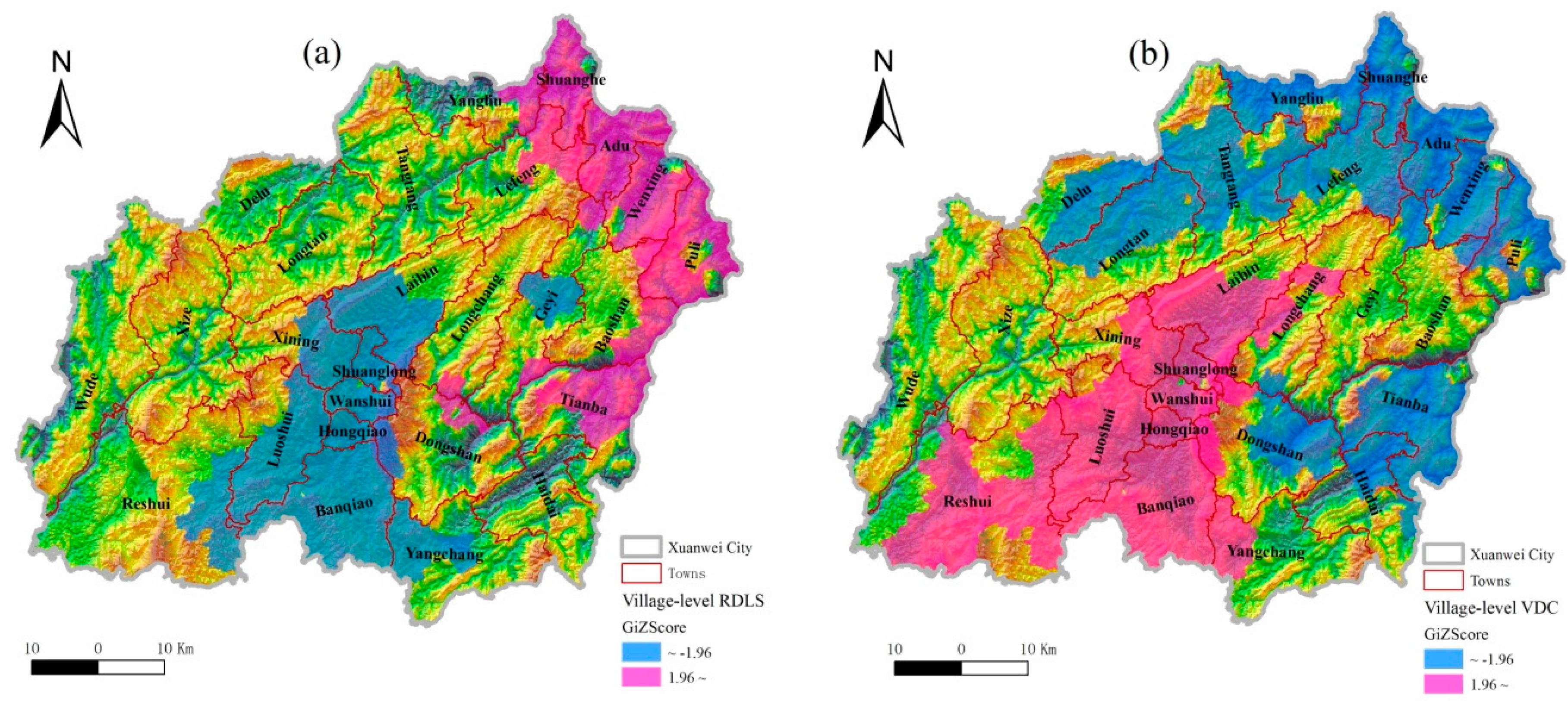
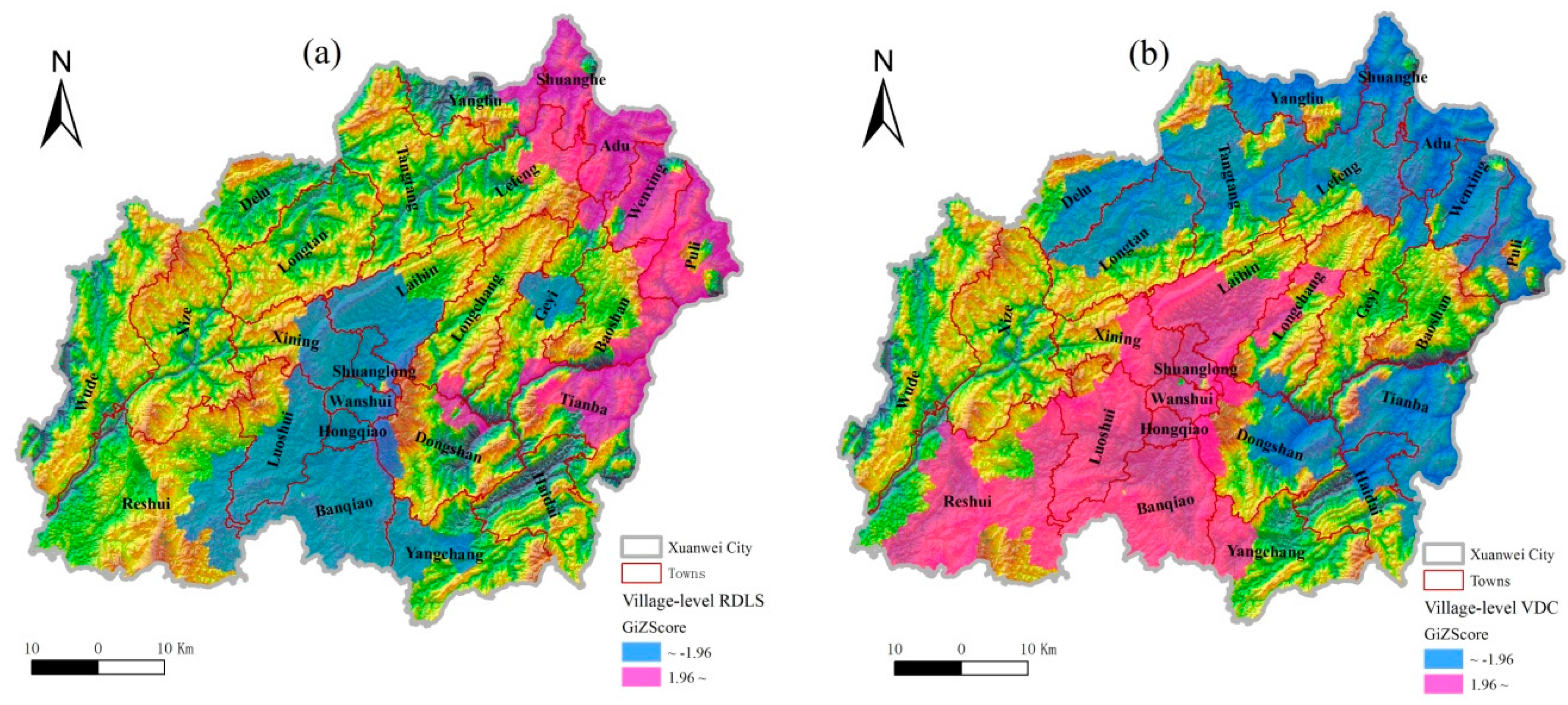
3.2. Topographic Characteristics
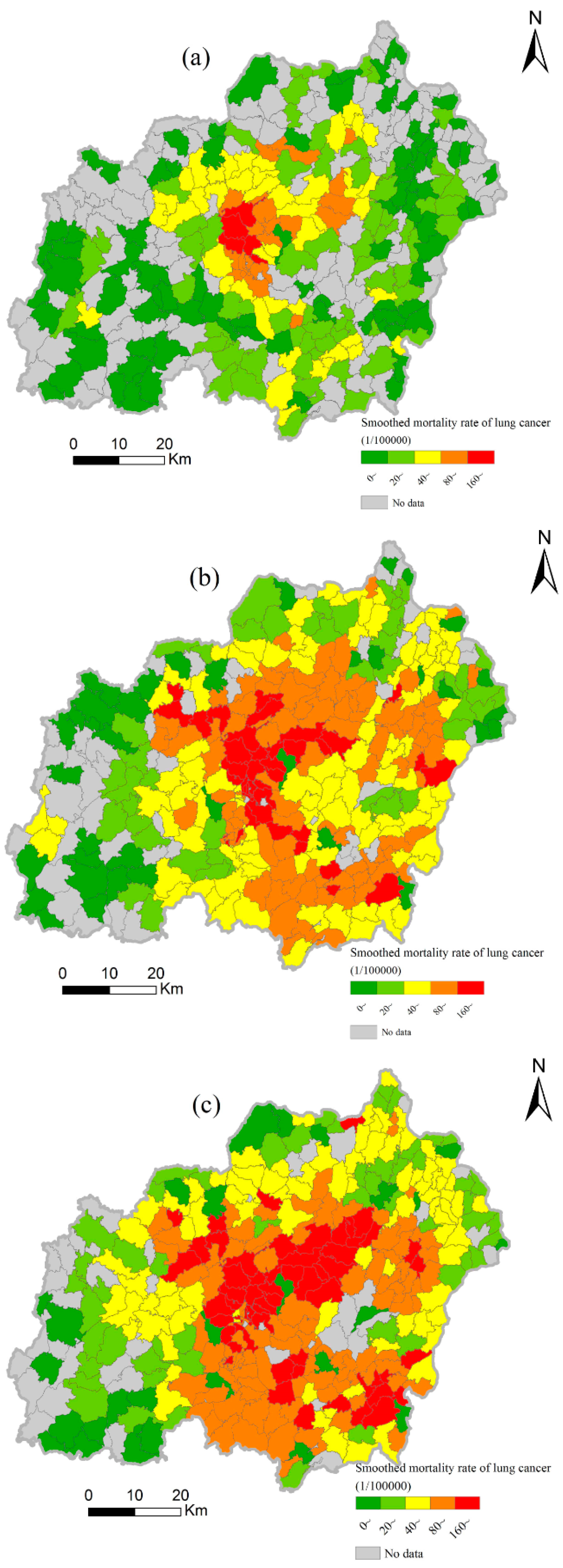
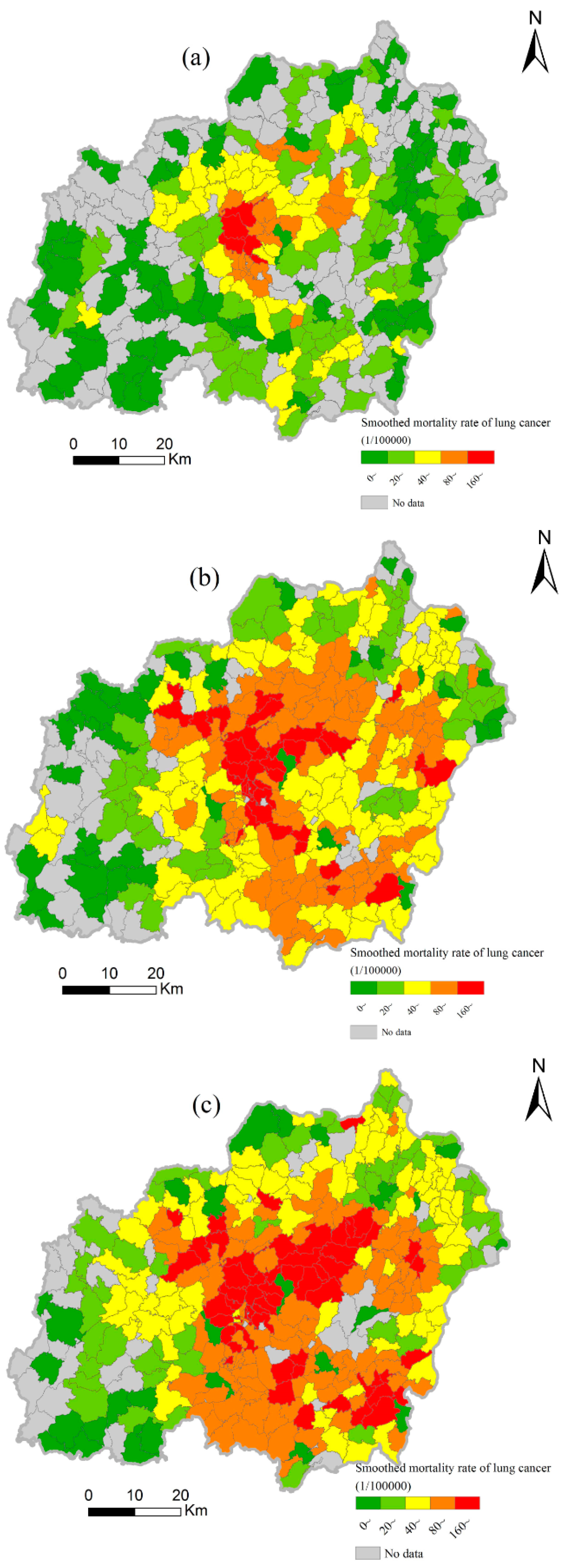
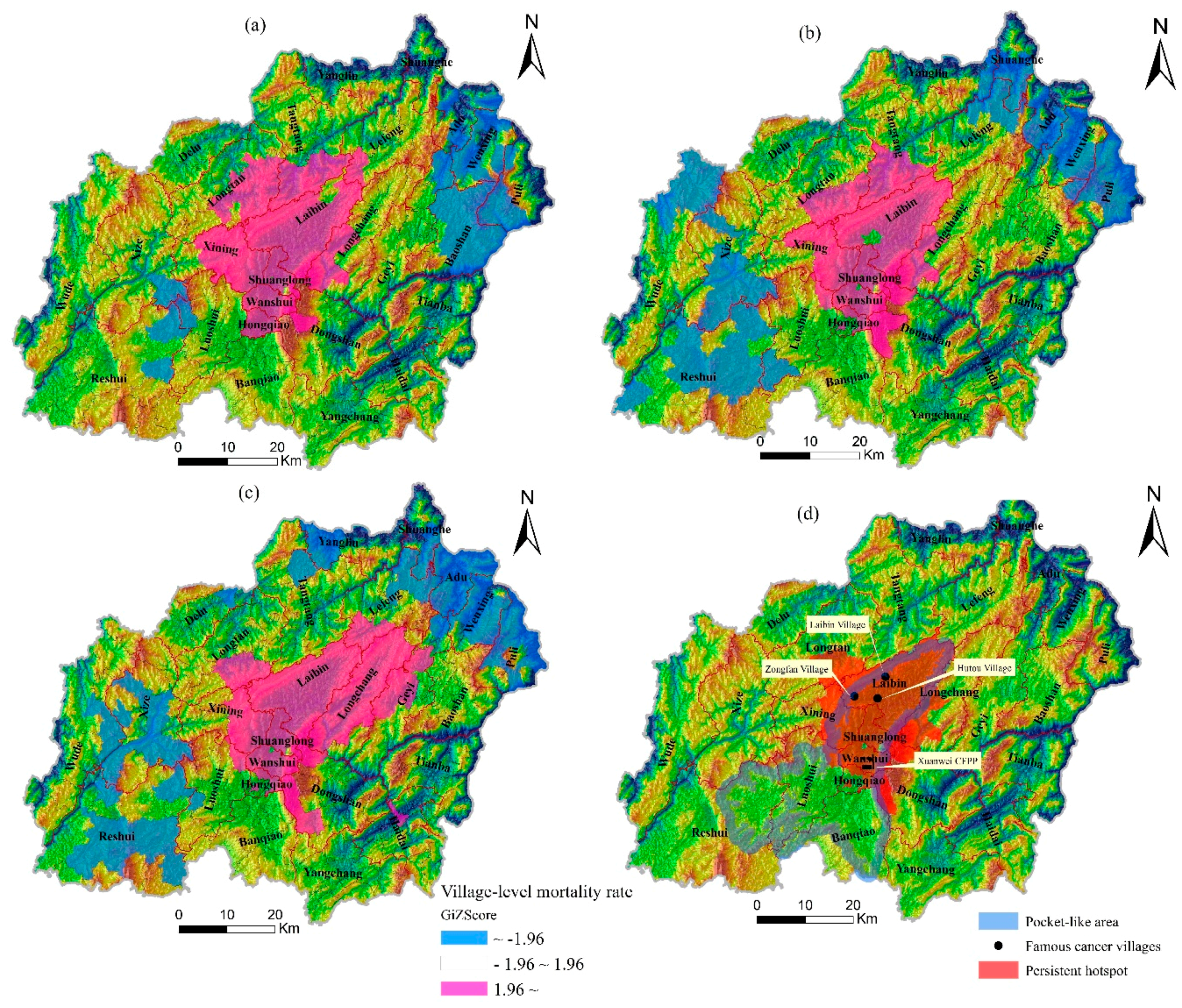
3.3. Spatiotemporal Variations of Lung Cancer Mortality
3.4. Relationship Between Lung Cancer and Topography
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Shao, L.; Hu, Y.; Wang, J.; Hou, C.; Yang, Y.; Wu, M. Particle-induced oxidative damage of indoor PM10 from coal burning homes in the lung cancer area of Xuanwei, China. Atmos Environ. 2013, 77, 959–967. [Google Scholar] [CrossRef]
- Mumford, J.L.; He, X.Z.; Chapman, R.S.; Cao, S.R.; Harris, D.B.; Li, X.M.; Xian, Y.L.; Jiang, W.Z.; Xu, C.W.; Chuang, J.C.; et al. Lung cancer and indoor air pollution in Xuanwei, China. Science 1987, 235, 217–220. [Google Scholar] [CrossRef] [PubMed]
- Lv, J.; Xu, R.; Wu, G.; Zhang, Q.; Li, Y.; Wang, P.; Liao, C.; Liu, J.; Jiang, G.; Wei, F. Indoor and outdoor air pollution of polycyclic aromatic hydrocarbons (pahs) in Xuanwei and Fuyuan, China. J. Environ. Monit. 2009, 11, 1368–1374. [Google Scholar] [CrossRef] [PubMed]
- Lan, Q.; Chapman, R.S.; Schreinemachers, D.M.; Tian, L.; He, X. Household stove improvement and risk of lung cancer in Xuanwei, China. J. Natl. Cancer Inst. 2002, 94, 826–835. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.; Chapman, R.S.; Hu, W.; He, X.; Hosgood, H.D.; Liu, L.Z.; Lai, H.; Chen, W.; Silverman, D.T.; Vermeulen, R.; et al. Smoky coal, tobacco smoking, and lung cancer risk in Xuanwei, China. Lung Cancer 2014, 84, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Shao, Y.; Yu, X.; Zhou, G. The epidemic status and risk factors of lung cancer in Xuanwei city, Yunnan province, China. Front. Med. 2012, 6, 388–394. [Google Scholar] [CrossRef] [PubMed]
- People’ Republic of China, Ministry of Health. The Third Retrospective Sampling Survey Report of Causes of Death; Peking Union Medical College Press: Beijing, China, 2012. [Google Scholar]
- Chen, G.; Sun, X.; Ren, H.; Wan, X.; Huang, H.; Ma, X.; Ning, B.; Zou, X.; Hu, W.; Yang, G. The mortality patterns of lung cancer between 1990 and 2013 in Xuanwei, China. Lung Cancer 2015, 90, 155–160. [Google Scholar] [CrossRef] [PubMed]
- He, X.Z.; Chen, W.; Liu, Z.Y.; Chapman, R.S. An epidemiological study of lung cancer in xuan wei county, china: Current progress. Case-control study on lung cancer and cooking fuel. Environ. Health Perspect 1991, 94, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Hosgood, H.D.; Chapman, R.; Shen, M.; Blair, A.; Chen, E.; Zheng, T.; Lee, K.M.; He, X.; Lan, Q. Portable stove use is associated with lower lung cancer mortality risk in lifetime smoky coal users. Brit. J. Cancer 2008, 99, 1934–1939. [Google Scholar] [CrossRef] [PubMed]
- Lan, Q.; He, X.; Shen, M.; Tian, L.; Liu, L.Z.; Lai, H.; Chen, W.; Berndt, S.I.; Hosgood, H.D.; Lee, K.M.; et al. Variation in lung cancer risk by smoky coal subtype in Xuanwei, China. Int. J. Cancer 2008, 123, 2164–2169. [Google Scholar] [CrossRef] [PubMed]
- Barone-Adesi, F.; Chapman, R.S.; Silverman, D.T.; He, X.; Hu, W.; Vermeulen, R.; Ning, B.; Fraumeni, J.F., Jr.; Rothman, N.; Lan, Q. Risk of lung cancer associated with domestic use of coal in Xuanwei, China: Retrospective cohort study. BMJ 2012, 345, e5414. [Google Scholar] [CrossRef] [PubMed]
- Downward, G.S.; Hu, W.; Large, D.; Veld, H.; Xu, J.; Reiss, B.; Wu, G.; Wei, F.; Chapman, R.S.; Rothman, N.; et al. Heterogeneity in coal composition and implications for lung cancer risk in Xuanwei and Fuyuan counties, China. Environ. Int. 2014, 68, 94–104. [Google Scholar] [CrossRef] [PubMed]
- Feng, Z.; Tang, Y.; Yang, Y.; Zhang, D. The relief degree of land surface in china and its correlation with population distribution. Acta Geograph. Sin. 2007, 62, 1073–1082. (In Chinese) [Google Scholar]
- Chen, G.; Huang, H.; Ma, X.; Ning, B.; Ren, H.; Wan, X.; Zou, X.; Yang, G. Investigation on under-reported deaths in Xuanwei Yunnan province, during 2011–2013. Chin. J. Prev. Med. 2015, 49, 541–545. (In Chinese) [Google Scholar]
- Walter, S.D. Assessing spatial patterns in disease rates. Stat. Med. 1993, 12, 1885–1894. [Google Scholar] [CrossRef] [PubMed]
- Antunes, J.L.; Biazevic, M.G.; de Araujo, M.E.; Tomita, N.E.; Chinellato, L.E.; Narvai, P.C. Trends and spatial distribution of oral cancer mortality in Sao Paulo, Brazil, 1980–1998. Oral Oncol. 2001, 37, 345–350. [Google Scholar] [CrossRef]
- Schafer, T.; Pritzkuleit, R.; Jeszenszky, C.; Malzahn, J.; Maier, W.; Gunther, K.P.; Niethard, F. Trends and geographical variation of primary hip and knee joint replacement in Germany. Osteoarthr. Cartil. 2013, 21, 279–288. [Google Scholar] [CrossRef] [PubMed]
- Anselin, L.; Getis, A. Spatial statistical analysis and geographic information systems. Ann. Reg. Sci. 1992, 26, 19–33. [Google Scholar] [CrossRef]
- Burra, T.; Jerrett, M.; Burnett, R.T.; Anderson, M. Conceptual and practical issues in the detection of local disease clusters: A study of mortality in Hamilton, Ontario. Geogr. Demography J. 2002, 46, 160–171. [Google Scholar] [CrossRef]
- Wagner, S.E.; Bauer, S.E.; Bayakly, A.R.; Vena, J.E. Prostate cancer incidence and tumor severity in Georgia: Descriptive epidemiology, racial disparity, and geographic trends. Cancer Cause Control 2013, 24, 153–166. [Google Scholar] [CrossRef] [PubMed]
- Getis, A.; Ord, J.K. The analysis of spatial association by use of distance statistics. Geogr. Anal. 1992, 24, 189–206. [Google Scholar] [CrossRef]
- Unwin, D.; Unwin, A. Local indicators of spatial association—Foreword. J. R. Stat. Soc. 1998, 47, 413. [Google Scholar] [CrossRef]
- Anselin, L.; Syabri, I.; Kho, Y. Geoda : An introduction to spatial data analysis. Geogr. Anal. 2005, 38, 5–22. [Google Scholar] [CrossRef]
- Goovaerts, P.; Xiao, H.; Adunlin, G.; Ali, A.; Tan, F.; Gwede, C.K.; Huang, Y. Geographically-weighted regression analysis of percentage oflate-stage prostate cancer diagnosis in Florida. Appl. Geogr. 2015, 62, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Ren, H.; Xu, D.; Shi, X.; Xu, J.; Zhuang, D.; Yang, G. Characterisation of gastric cancer and its relation to environmental factors: A case study in Shenqiu county, China. Int. J. Environ. Health Res. 2015, 26, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Chapman, R.S.; He, X.; Blair, A.E.; Lan, Q. Improvement in household stoves and risk of chronic obstructive pulmonary disease in Xuanwei, China: Retrospective cohort study. BMJ 2005, 331, 1050. [Google Scholar] [CrossRef] [PubMed]
- Shen, M.; Chapman, R.S.; Vermeulen, R.; Tian, L.; Zheng, T.; Chen, B.E.; Engels, E.A.; He, X.; Blair, A.; Lan, Q. Coal use, stove improvement, and adult pneumonia mortality in Xuanwei, China: A retrospective cohort study. Environ. Health Perspect. 2009, 117, 261–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lan, Q.; Chen, W.; Chen, H.; He, X.Z. Risk factors for lung cancer in non-smokers in Xuanwei county of China. Biomed. Environ. Sci. 1993, 6, 112–118. [Google Scholar] [PubMed]
- Bradford, D.F.; Stanley, K.A.; Tallent, N.G.; Sparling, D.W.; Nash, M.S.; Knapp, R.A.; McConnell, L.L.; Massey Simonich, S.L. Temporal and spatial variation of atmospherically deposited organic contaminants at high elevation in yosemite national park, California, USA. Environ. Toxicol. Chem. 2013, 32, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.P.; Yao, T.D.; Cong, Z.Y.; Yan, X.L.; Kang, S.C.; Zhang, Y. Gradient distribution of persistent organic contaminants along northern slope of central-himalayas, China. Sci. Total Envir. 2006, 372, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Foan, L.; Leblond, S.; Thoni, L.; Raynaud, C.; Santamaria, J.M.; Sebilo, M.; Simon, V. Spatial distribution of pah concentrations and stable isotope signatures (delta13c, delta15n) in mosses from three european areas--characterization by multivariate analysis. Environ. Pollut. 2014, 184, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Mast, M.A.; Alvarez, D.A.; Zaugg, S.D. Deposition and accumulation of airborne organic contaminants in yosemite national park, california. Environ. Toxicol. Chem. 2012, 31, 524–533. [Google Scholar] [CrossRef] [PubMed]
- Deng, J.S.; Zhu, S.X.; Zheng, M. The characteristics of wind field within boudary layer of different topography and case analysis on pollution meteorology related to mountain-valley win. Trop. Geogr. 1989, 4, 346–353. (In Chinese) [Google Scholar]
- Zhou, Y.; Levy, J.I.; Evans, J.S.; Hammitt, J.K. The influence of geographic location on population exposure to emissions from power plants throughout China. Environ. Int. 2006, 32, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Zhang, F.; Xu, L.; Chen, J.; Xu, Y. Spatial and temporal distribution of polycyclic aromatic hydrocarbons (pahs) in the atmosphere of Xiamen, China. Sci. Total Environ. 2011, 409, 5318–5327. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Descriptive Statistics | Smoothed Mortality Rate of Lung Cancer (Per 105) | RDLS | VDC | ||||
|---|---|---|---|---|---|---|---|
| 1990–1992 | 2004–2005 | 2011–2013 | 1990–1992 | 2004–2005 | 2011–2013 | 2011–2013 | |
| Mean | 38.97 | 88.18 | 98.75 | 2.87 | 2.89 | 2.88 | 0.40 |
| Range | 264.45 | 470.27 | 458.32 | 2.41 | 2.51 | 2.56 | 1.00 |
| Standard Deviation | 40.57 | 78.10 | 86.10 | 0.46 | 0.51 | 0.51 | 0.34 |
| Parameters of Spatial Features | Smoothed Mortality Rate of Lung Cancer (Per 105) | RDLS | VDC | ||
|---|---|---|---|---|---|
| 1990–1992 | 2004–2005 | 2011–2013 | 2011–2013 | 2011–2013 | |
| Moran’s I | 0.71 | 0.62 | 0.49 | 0.90 | 0.91 |
| Z Score | 31.46 | 27.02 | 20.44 | 37.15 | 44.72 |
| p-value | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 |
| Variables | 1990–1992 | 2004–2005 | 2011–2013 |
|---|---|---|---|
| RDLS | −0.34 ‡ | −0.36 ‡ | −0.37 ‡ |
| VDC | / | / | 0.33 ‡ |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ren, H.; Cao, W.; Chen, G.; Yang, J.; Liu, L.; Wan, X.; Yang, G. Lung Cancer Mortality and Topography: A Xuanwei Case Study. Int. J. Environ. Res. Public Health 2016, 13, 473. https://doi.org/10.3390/ijerph13050473
Ren H, Cao W, Chen G, Yang J, Liu L, Wan X, Yang G. Lung Cancer Mortality and Topography: A Xuanwei Case Study. International Journal of Environmental Research and Public Health. 2016; 13(5):473. https://doi.org/10.3390/ijerph13050473
Chicago/Turabian StyleRen, Hongyan, Wei Cao, Gongbo Chen, Junxing Yang, Liqun Liu, Xia Wan, and Gonghuan Yang. 2016. "Lung Cancer Mortality and Topography: A Xuanwei Case Study" International Journal of Environmental Research and Public Health 13, no. 5: 473. https://doi.org/10.3390/ijerph13050473