
Eating Behaviours of Preadolescent Children over Time: Stability, Continuity and the Moderating Role of Perceived Parental Feeding Practices


Abstract
:1. Introduction
2. Experimental Section
2.1. Participants
2.2. Procedure and Measures
2.2.1. Eating Patten Inventory for Children (EPIC)
2.2.2. Kids’ Child Feeding Questionnaire (KCFQ)
2.3. Statistical Analyses
3. Results and Discussion
3.1. Descriptive Statistics and Gender Differences
3.2. Stability of Perceived Parental Feeding Practices between T1 and T2
3.3. Continuity of Perceived Parental Feeding Practices over 12 Months
3.4. Moderation Analyses
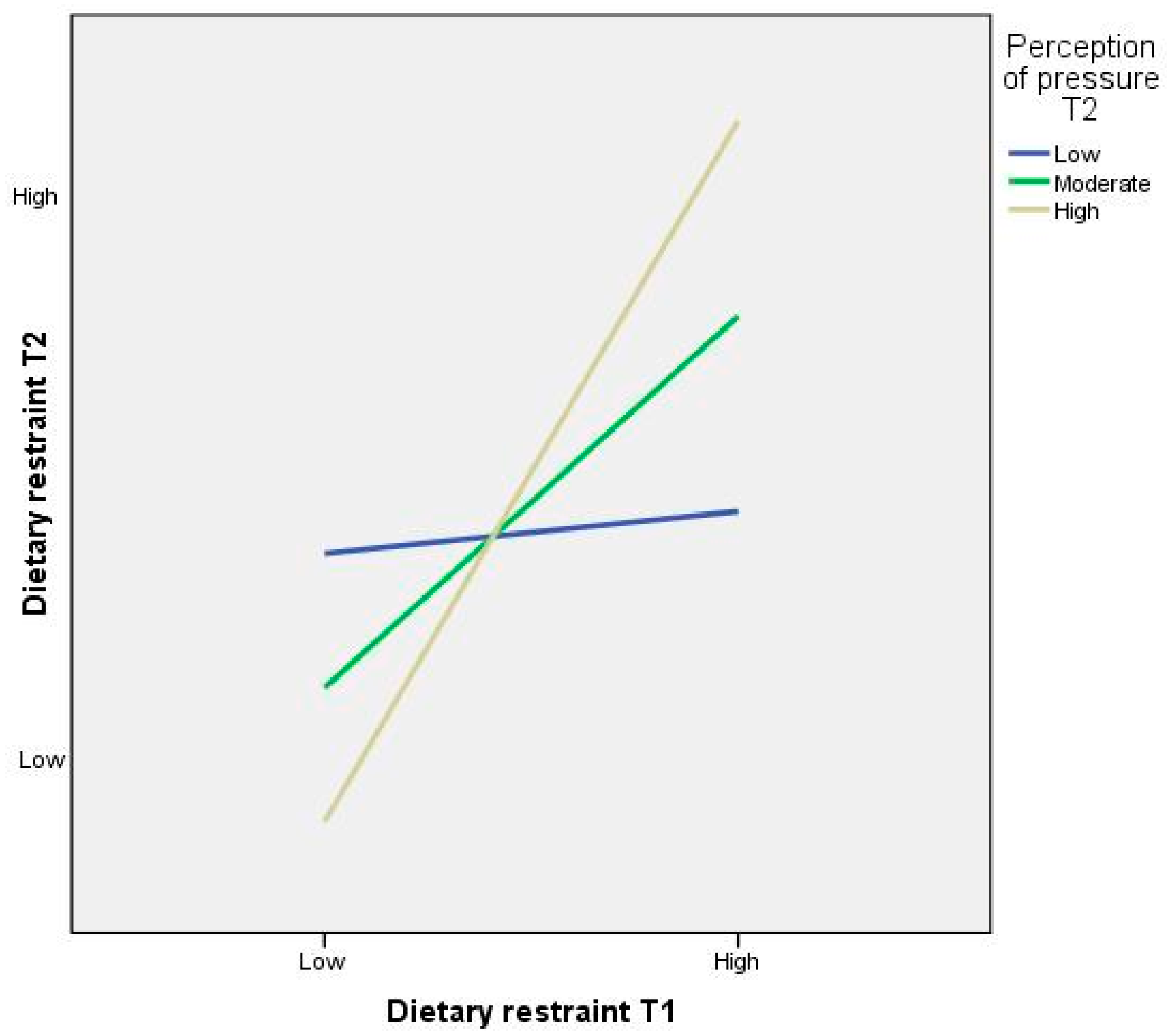
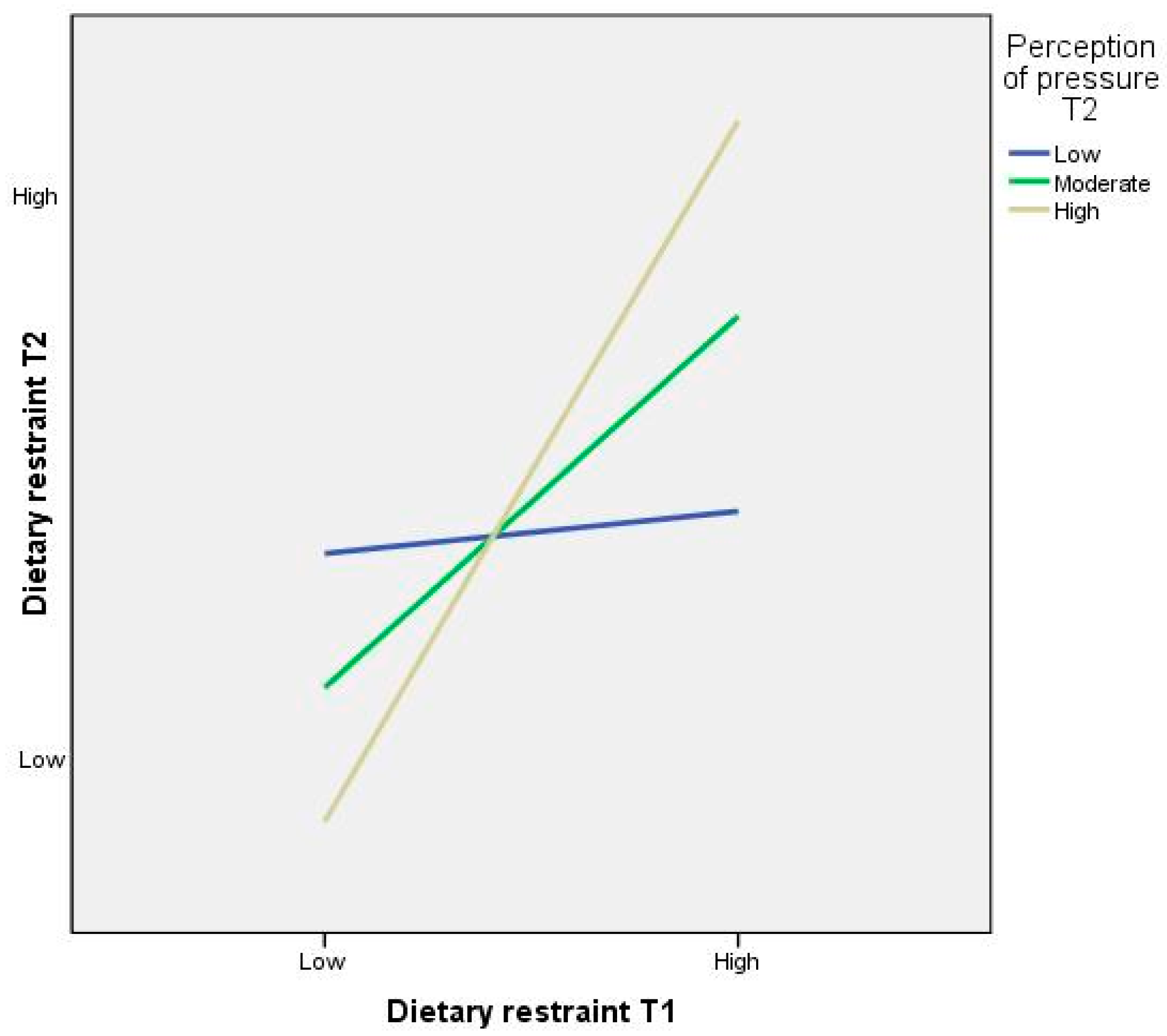
3.4.1. The Moderating Role of Perceived Pressure to Eat on the Stability of Eating Behaviours between T1 and T2
Pressure to eat at T2 as a Moderator of Dietary Restraint between T1 and T2
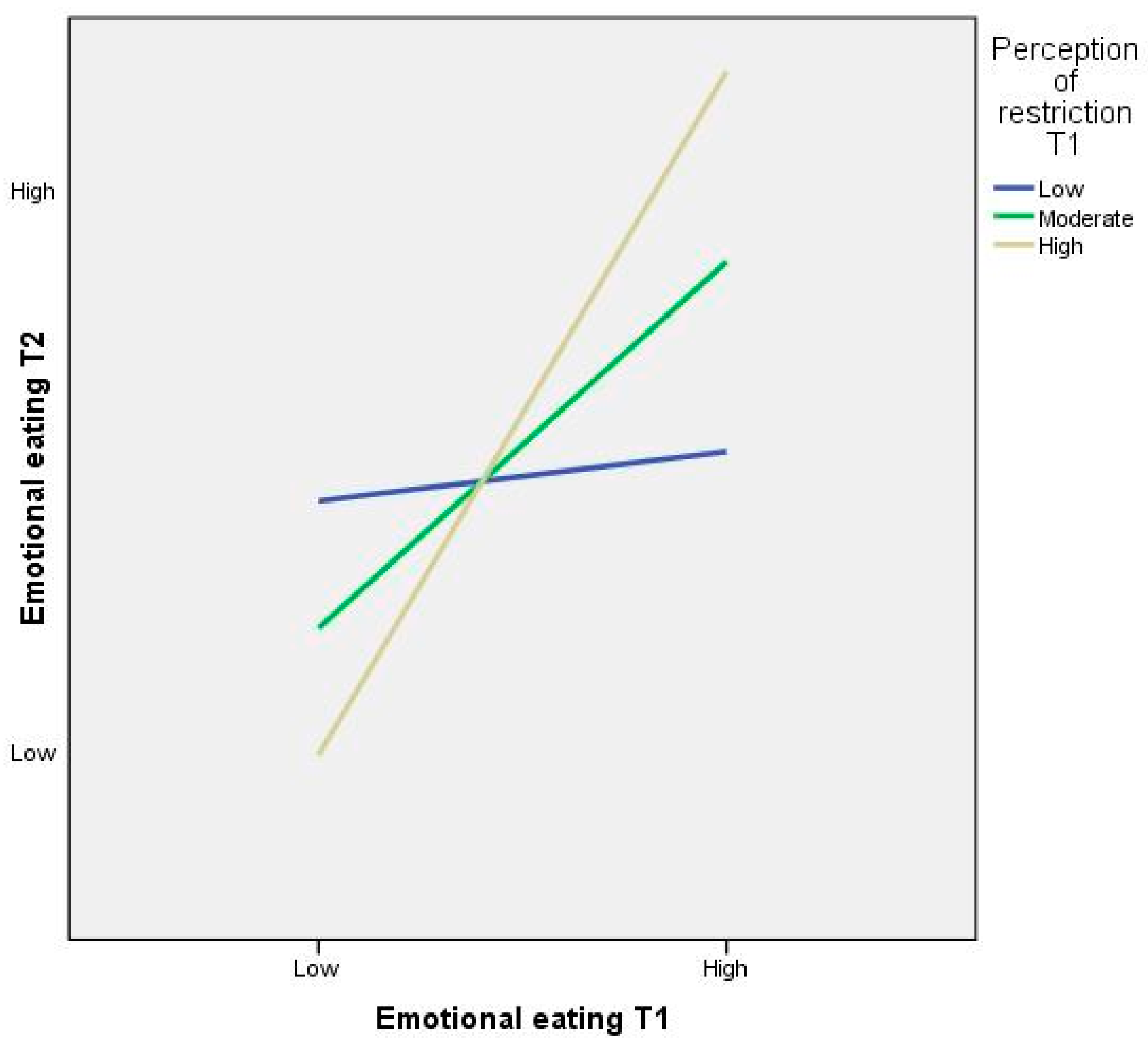
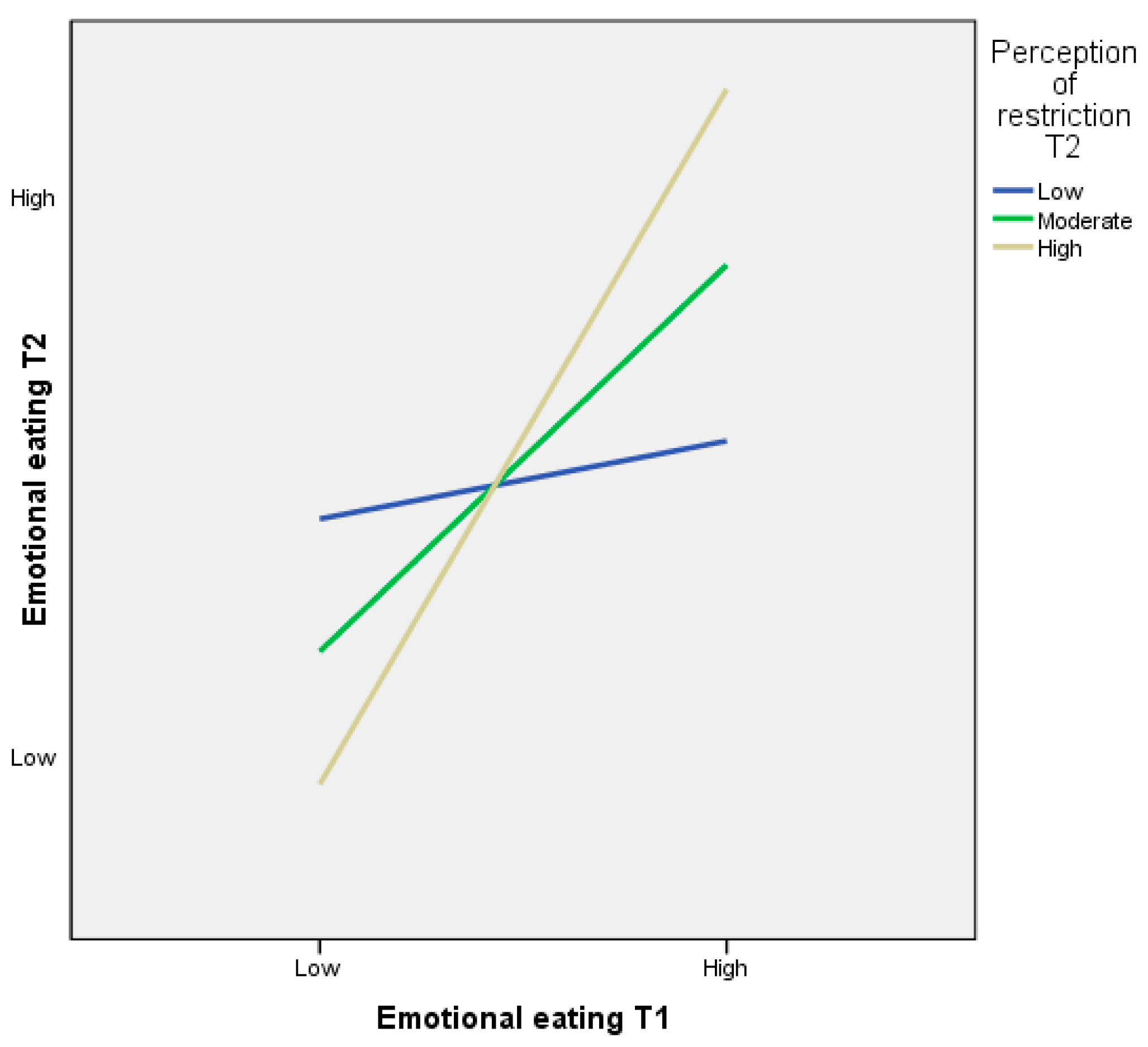
3.4.2. The Moderating Role of Perceived Restriction on the Stability of Eating Behaviours between T1 and T2
Restriction at T1 as a Moderator of Emotional Eating between T1 and T2
Restriction at T2 as a Moderator of Emotional Eating between T1 and T2
3.5. Discussion of Study Findings
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Faith, M.S.; Scanlon, K.S.; Birch, L.; Francis, L.A.; Sherry, B. Parent-child feeding strategies and their relationships to child eating and weight status. Obes. Res. 2004, 12, 1711–1722. [Google Scholar] [CrossRef] [PubMed]
- Scaglioni, S.; Salvioni, M.; Galimberti, C. Influence of parental attitudes in the development of eating behaviour. Br. J. Nutr. 2008, 99, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Wardle, J.; Carnell, S. Parental feeding practices and children’s weight. Acta Paediatr. 2007, 96, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Patrick, H.; Nicklas, T.A. A review of family and social determinants of children’s eating patterns and diet quality. J. Am. Coll. Nutr. 2005, 24, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Fulkerson, J.A.; Neumark-Sztainer, D.; Story, M. Adolescent and parent views of family meals. J. Am. Diet. Assoc. 2006, 106, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Savage, J.S.; Fisher, J.O.; Birch, L.L. Parental influence on eating behaviour: Conception to adolescence. J. Law Med. Ethics 2007, 35, 22–34. [Google Scholar] [CrossRef] [PubMed]
- Walsh, A.; Nelson, R. The links between diet and health: An exploratory study of adolescents in Northern Ireland using foodmaps. Int. J. Consum. Stud. 2010, 34, 190–195. [Google Scholar] [CrossRef]
- White, H.; Haycraft, E.; Meyer, C. Family mealtimes and eating psychopathology: The role of anxiety and depression among adolescent girls and boys. Appetite 2014, 75, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Farrow, C.; Blissett, J. Controlling feeding practices: Cause or consequence of early child weight? Pediatrics 2008, 121, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Gregory, J.E.; Paxton, S.J.; Brozovic, A.M. Maternal feeding practices, child eating behaviour and body mass index in preschool-aged children: A prospective analysis. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 55. [Google Scholar] [CrossRef] [PubMed]
- Haycraft, E.; Goodwin, H.; Meyer, C. Adolescents’ level of eating psychopathology is related to perceptions of their parents’ current feeding practices. J. Adolesc. Health 2014, 54, 204–208. [Google Scholar] [CrossRef] [PubMed]
- Birch, L.L.; Fisher, J.O. Mothers’ child-feeding practices influence daughters’ eating and weight. Am. J. Clin. Nutr. 2000, 71, 1054–1061. [Google Scholar] [PubMed]
- Carper, J.L.; Fisher, J.O.; Birch, L.L. Young girls’ emerging dietary restraint and disinhibition are related to parental control in child feeding. Appetite 2000, 35, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Birch, L.L.; Fisher, J.O.; Grimm-Thomas, K.; Markey, C.N.; Sawyer, R.; Johnson, S.L. Confirmatory factor analysis of the Child Feeding Questionnaire: A measure of parental attitudes, beliefs and practices about child feeding and obesity proneness. Appetite 2001, 36, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Galloway, A.T.; Fiorito, L.; Lee, Y.; Birch, L.L. Parental pressure, dietary patterns, and weight status among girls who are “picky eaters”. J. Am. Diet. Assoc. 2005, 105, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Francis, L.A.; Hofer, S.M.; Birch, L.L. Predictors of maternal child-feeding style: Maternal and child characteristics. Appetite 2001, 37, 231–243. [Google Scholar] [CrossRef] [PubMed]
- Galloway, A.T.; Fiorito, L.M.; Francis, L.A.; Birch, L.L. “Finish your soup”: Counterproductive effects of pressuring children to eat on intake and affect. Appetite 2006, 46, 318–323. [Google Scholar] [CrossRef] [PubMed]
- Hart, K.H.; Bishop, J.A.; Truby, H. An investigation into school children’s knowledge and awareness of food and nutrition. J. Hum. Nutr. Diet. 2002, 15, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Birch, L.L.; Fisher, J.O.; Davison, K.K. Learning to overeat: Maternal use of restrictive feeding practices promotes girls’ eating in the absence of hunger. Am. J. Clin. Nutr. 2003, 78, 215–220. [Google Scholar] [PubMed]
- Rollins, B.Y.; Loken, E.; Savage, J.S.; Birch, L.L. Effects of restriction on children’s intake differ by child temperament, food reinforcement, and parent’s chronic use of restriction. Appetite 2014, 73, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Van Strien, T.; Bazelier, F.G. Perceived parental control of food intake is related to external, restrained and emotional eating in 7–12-year-old boys and girls. Appetite 2007, 49, 618–625. [Google Scholar] [CrossRef] [PubMed]
- Houldcroft, L.; Farrow, C.; Haycraft, E. Perceptions of parental pressure to eat and eating behaviours in preadolescents: The mediating role of anxiety. Appetite 2014, 80, 61–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pulley, C.; Galloway, A.T.; Webb, R.M.; Payne, L.O. Parental child feeding practices: How do perceptions of mother, father, sibling, and self vary? Appetite 2014, 80, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Cote, L.R.; Bornstein, M.H. Cultural and parenting cognitions in acculturating cultures. 1. Cultural comparisons and developmental continuity and stability. J. Cross Cult. Psychol. 2003, 34, 323–349. [Google Scholar] [CrossRef]
- Farrow, C.; Blissett, J. Stability and continuity of parentally reported child eating behaviours and feeding practices from 2 to 5 years of age. Appetite 2012, 58, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Webber, L.; Cooke, L.; Hill, C.; Wardle, J. Child adiposity and maternal feeding practices. A longitudinal analysis. Am. J. Clin. Nutr. 2010, 92, 1423–1428. [Google Scholar] [CrossRef] [PubMed]
- Schact, M.; Richter-Appelt, H.; Schulte-Markwort, M.; Hebebrand, J.; Schimmelmann, B.G. Eating pattern inventory for children: A new self-rating questionnaire for preadolescents. J. Clin. Psychol. 2006, 62, 1259–1273. [Google Scholar] [CrossRef] [PubMed]
- Farrow, C.; Haycraft, E.; Meyer, C. Similarities between eating attitudes among friendship groups: The moderating role of child anxiety. J. Pediatr. Psychol. 2011, 36, 1144–1152. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Personal. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Ogden, J.; Reynolds, R.; Smith, A. Expanding the concept of parental control: A role for overt and covert control in children’s snacking behaviour? Appetite 2006, 47, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Fisher, J.O.; Birch, L.L. Eating in the absence of hunger and overweight in girls from 5 to 7 year of age. Am. J. Clin. Nutr. 2002, 76, 226–231. [Google Scholar] [PubMed]
- Susman, E.J.; Dorn, L.D. Puberty: Its role in development. In Handbook of Adolescent Psychology; Lerner, R.M., Steinberg, L., Eds.; Wiley: New York, NY, USA, 2009; pp. 116–151. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| Variable | Mean (SD) Boys (n = 120) | Mean (SD) Girls (n = 109) | Independent t-Test (t) | p-Value | 95% Confidence Interval |
|---|---|---|---|---|---|
| Dietary restraint T1 | 2.18 (0.80) | 2.16 (0.75) | 0.18 | 0.859 | −0.185–0.221 |
| Dietary restraint T2 | 1.95 (0.75) | 1.87 (0.78) | 0.76 | 0.446 | −0.122–0.276 |
| External eating T1 | 2.38 (0.88) | 2.19 (0.78) | 1.74 | 0.083 | −0.025–0.409 |
| External eating T2 | 2.09 (0.80) | 1.92 (0.77) | 1.76 | 0.079 | −0.021–0.379 |
| Emotional eating T1 | 1.83 (0.77) | 1.79 (0.73) | 0.42 | 0.673 | −0.153–0.237 |
| Emotional eating T2 | 1.65 (0.74) | 1.59 (0.70) | 0.60 | 0.548 | −0.130–0.245 |
| Variable | Mean (SD) Boys (n = 120) | Mean (SD) Girls (n = 109) | Independent Samples t-Test (t) | p-Value | 95% Confidence Interval |
|---|---|---|---|---|---|
| Perceived pressure to eat T1 | 0.98 (0.42) | 0.96 (0.43) | 0.25 | 0.806 | −0.097–0.124 |
| Perceived pressure to eat T2 | 0.90 (0.49) | 0.85 (0.40) | 0.77 | 0.444 | −0.067–0.167 |
| Perceived restriction T1 | 0.90 (0.36) | 0.94 (0.35) | 0.84 | 0.401 | −0.129–0.057 |
| Perceived restriction T2 | 0.90 (0.44) | 0.86 (0.38) | 0.87 | 0.385 | −0.060–0.155 |
| Variable | Rs | p-Value |
|---|---|---|
| Perception of pressure to eat | 0.49 | 0.000 |
| Perception of restriction | 0.37 | 0.000 |
| Variable | T1 Mean (SD) | T2 Mean (SD) | Mean Change (SD) | Paired Samples t-Test (t) | p-Value | 95% Confidence Interval |
|---|---|---|---|---|---|---|
| Perceived pressure to eat | 0.97 (0.42) | 0.92 (0.36) | −0.05 (0.40) | −1.80 | 0.070 | −0.004–0.099 |
| Perceived restriction | 0.88 (0.45) | 0.88 (0.41) | −0.00 (0.48) | −0.02 | 0.982 | −0.064–0.062 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Houldcroft, L.; Farrow, C.; Haycraft, E. Eating Behaviours of Preadolescent Children over Time: Stability, Continuity and the Moderating Role of Perceived Parental Feeding Practices. Int. J. Environ. Res. Public Health 2016, 13, 437. https://doi.org/10.3390/ijerph13040437
Houldcroft L, Farrow C, Haycraft E. Eating Behaviours of Preadolescent Children over Time: Stability, Continuity and the Moderating Role of Perceived Parental Feeding Practices. International Journal of Environmental Research and Public Health. 2016; 13(4):437. https://doi.org/10.3390/ijerph13040437
Chicago/Turabian StyleHouldcroft, Laura, Claire Farrow, and Emma Haycraft. 2016. "Eating Behaviours of Preadolescent Children over Time: Stability, Continuity and the Moderating Role of Perceived Parental Feeding Practices" International Journal of Environmental Research and Public Health 13, no. 4: 437. https://doi.org/10.3390/ijerph13040437