
A Conceptual Framework for the Assessment of Cumulative Exposure to Air Pollution at a Fine Spatial Scale

 ,
,
Abstract
:1. Introduction
The Purpose of This Paper
- (i)
- We present an overview of exposure assessment in the exploration of long-term effects in epidemiological studies.
- (ii)
- We propose a conceptual framework for the retrospective assessment of air pollution, including two components:
- (1)
- retrospective reconstitution of NO2 concentrations at a fine spatial scale (NO2 has been chosen as the index pollutant because its spatial variability is higher than in many other air pollutants); and
- (2)
- a novel approach to assigning time-relevant exposure estimates at the census block level, using all available data on residential mobility throughout the 10-to 20-year period prior to that for which the health events are to be detected.
- (iii)
- We propose an application of this framework using French data to illustrate preliminary results and to describe the feasibility of the different steps of our framework.
- (iv)
- We discuss the need for this conceptual framework, and its subsequent value.
2. Retrospective Air Pollution Assessment: An Overview
2.1. Retrospective Reconstitution of Ambient Air Concentrations and Exposure Assignment
2.2. Retrospective Reconstitution of Cumulative Exposure Levels
3. A Conceptual Framework for Retrospective Assessment of Air Pollution
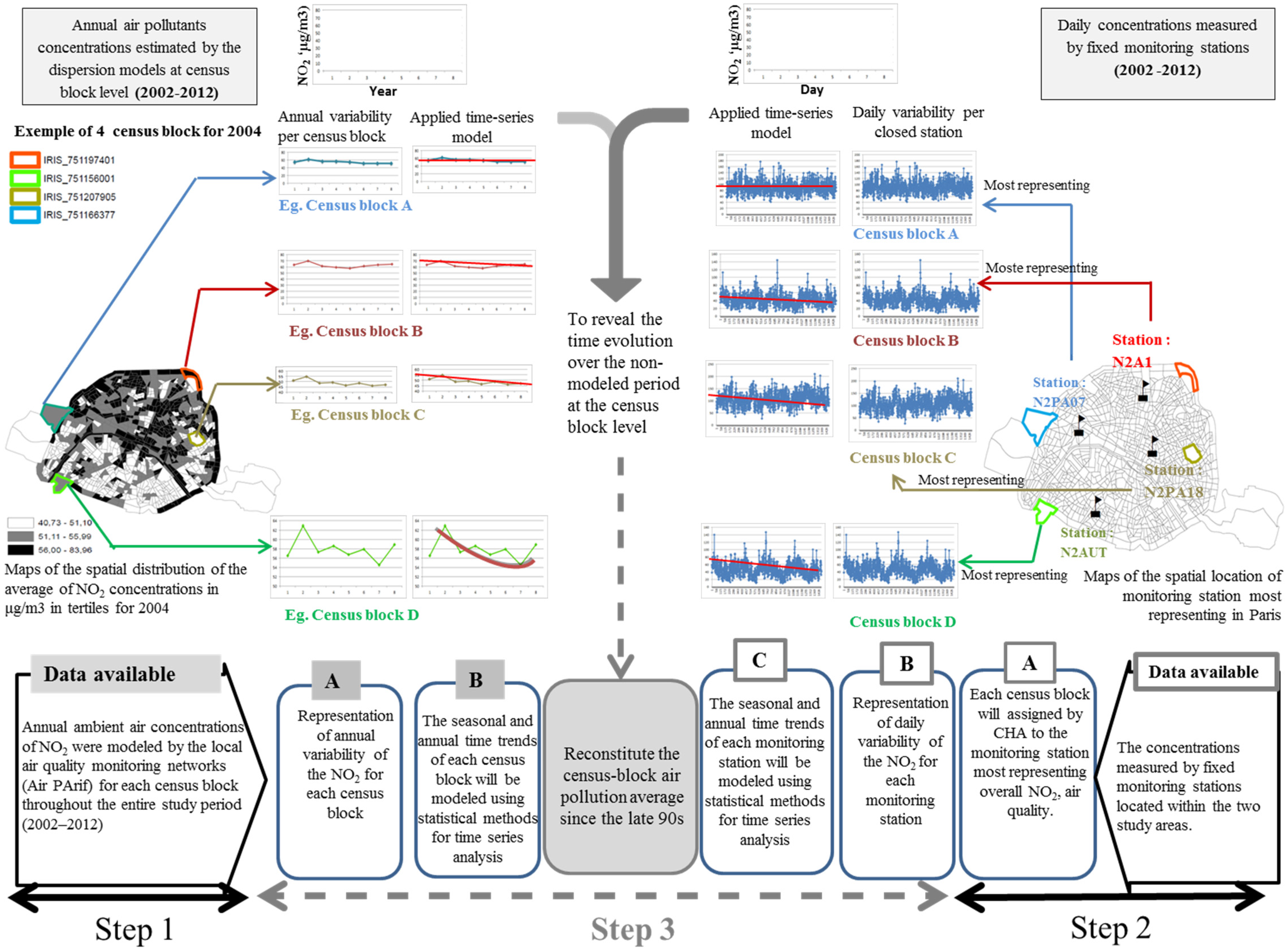
3.1. Retrospective Modeling of Pollutant Concentrations at a Fine Spatial Scale
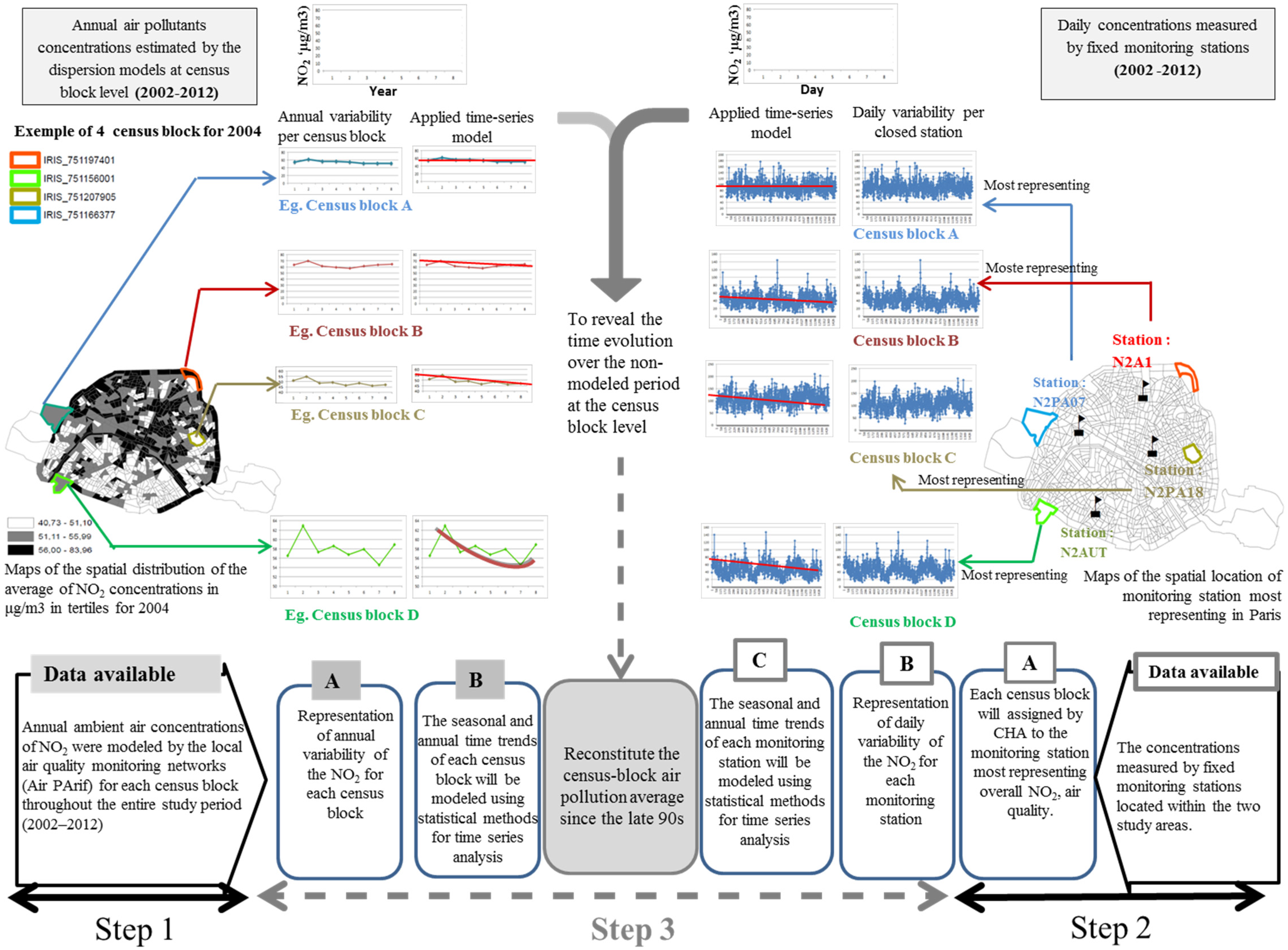
3.1.1. Step1: Modeling the Annual Averages of NO2 Concentrations between 2002 and 2012 at the Census Block Level
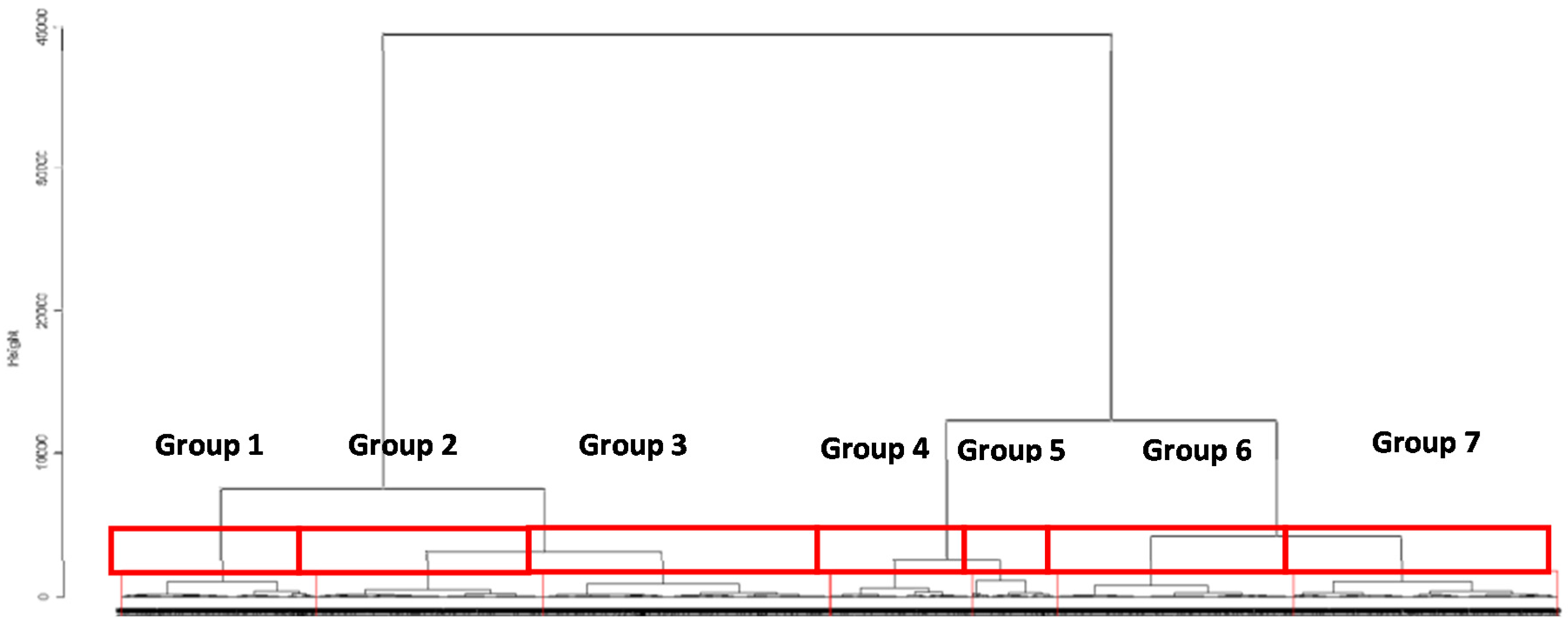
3.1.2. Step 2: Assessing the Spatial Area Representative of the Air Quality Monitoring Stations
3.1.3. Step 3: Reconstitution of the Retrospective Annual Averages Prior to 2002 at the Census Block Level
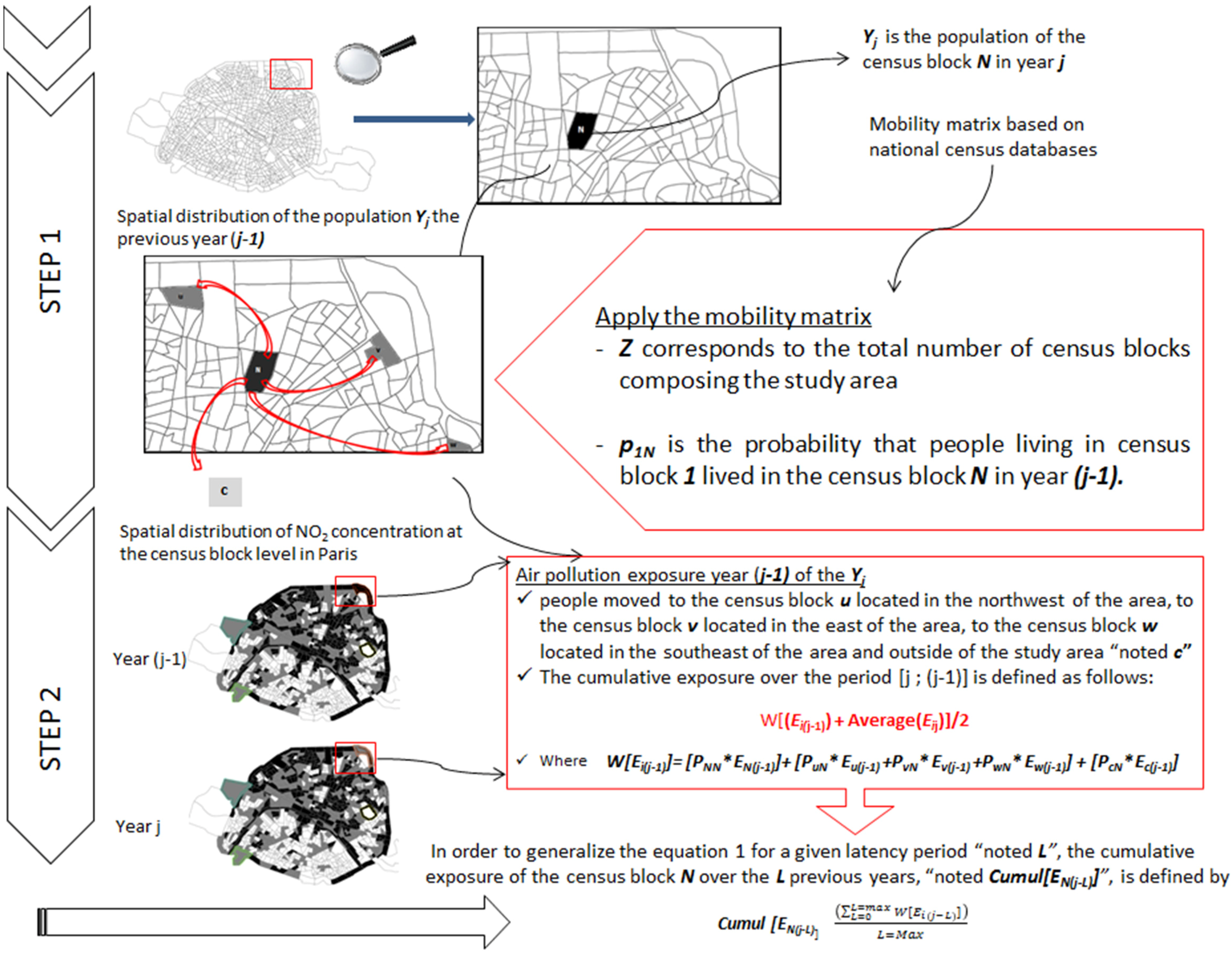
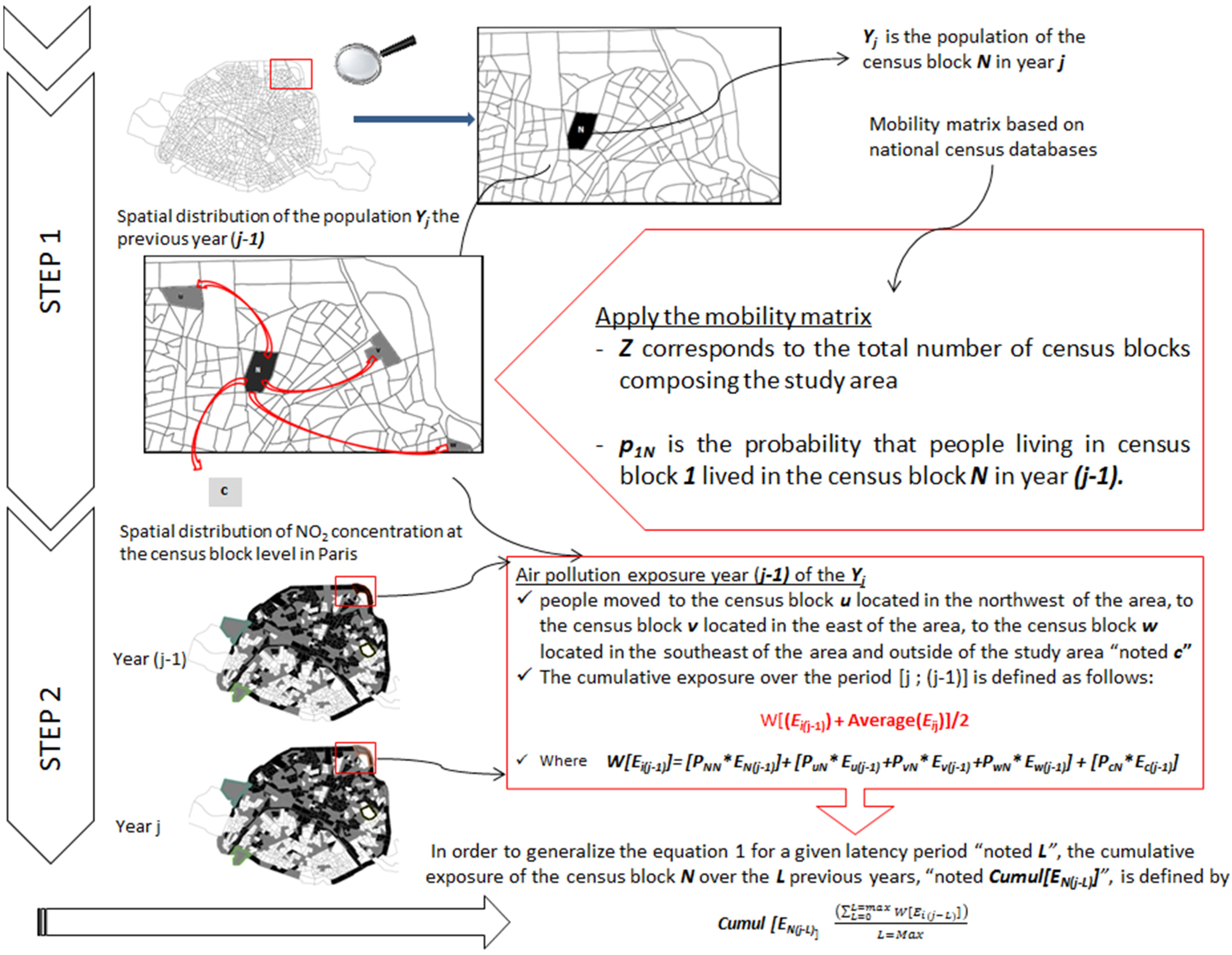
3.2. Assessment of Cumulative Exposure Accounting for Residential Mobility
- First, we retrieve the information from the national census that describes the proportion of the residents of each census block that lived in another census block in the past.
- Second, we derive a population cumulative exposure estimate by weighting the average ambient air levels of the various census blocks according to the population that resided in other census blocks (or cities) in the past.
Theoretical Model
- — Let N denote the census block with an average exposure level ENj in the year j.
- — Let us define U, V and W census blocks comprising the study area with the corresponding average exposure level Euj, Evj and Ewj, estimated in the year j.
- — Let C denote the area outside the study area with Ecj, the corresponding average exposure level estimated in the year j.
- [PNN* EN(j-1)] characterizes the sedentary population; pNN is the probability that the population residing in census block N already lived in the same census block N in year (j-1);
- [PuN*Eu(j-1) + PvN*Ev(j-1) + PwN*Ew(j-1)] characterizes the intra-area movement of the population;
- ○
- puN pvN and pwN are probabilities that the population residing in census block N lived, respectively, in the census block U, V or W in year (j-1) and
- ○
- Eu(j-1), Ev(j-1) and Ew(j-1) are, respectively, the average exposure level of census block U, V or W in year (j-1)
- [PcN*Ec(j-1)] characterizes the population movement outside the study area;pCN is the probability that the population residing in census block N lived in location C (municipality or department or region) in year (j-1)
- ○
- Ec(j-1) is the average exposure level of the location C in year (j-1) extracted from the meta-analysis of French studies conducted at the municipal and regional scales (e.g., Bentayeb et al., 2014).
4. An Application Using Data from Paris
4.1. Study Setting
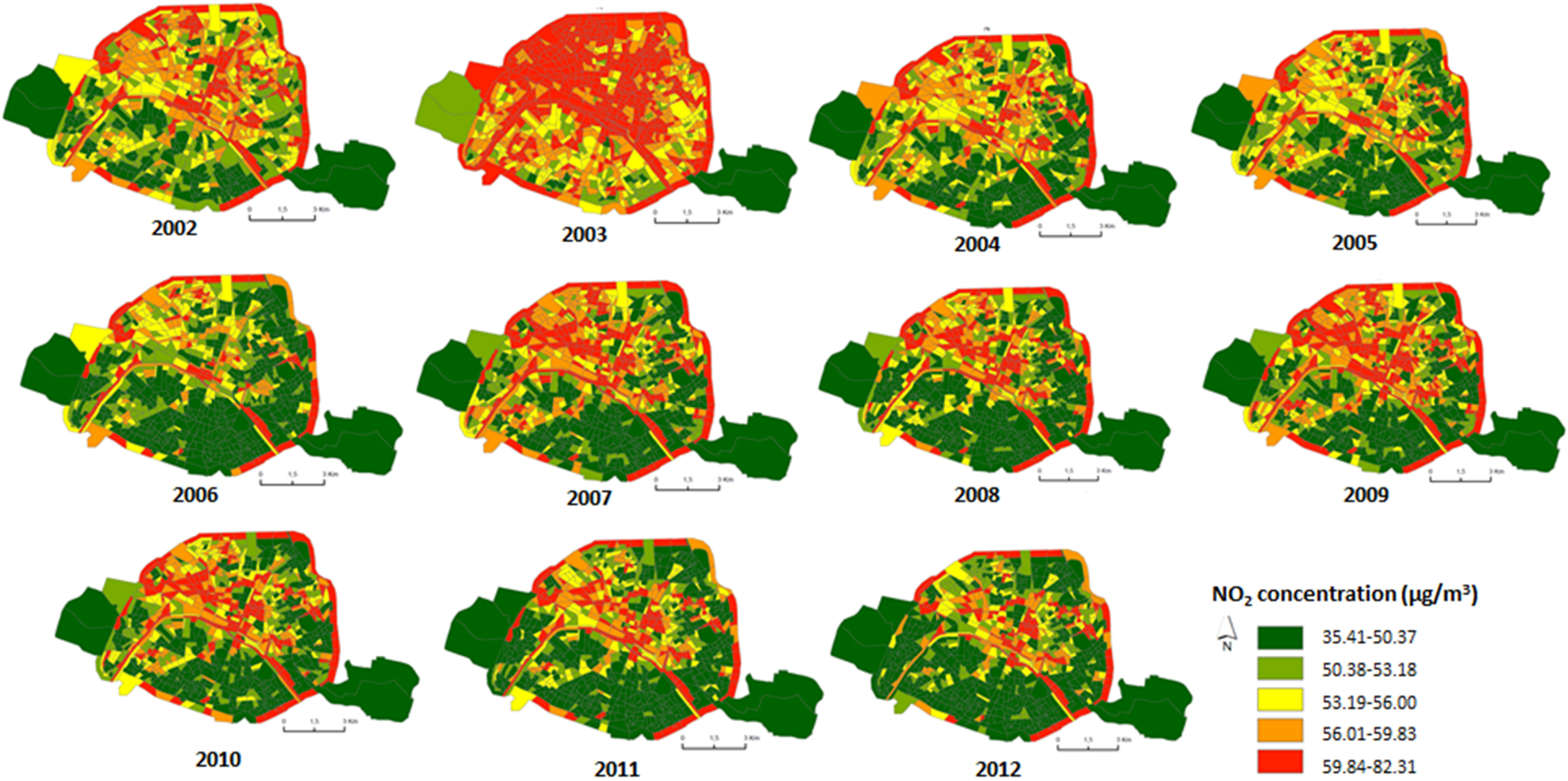
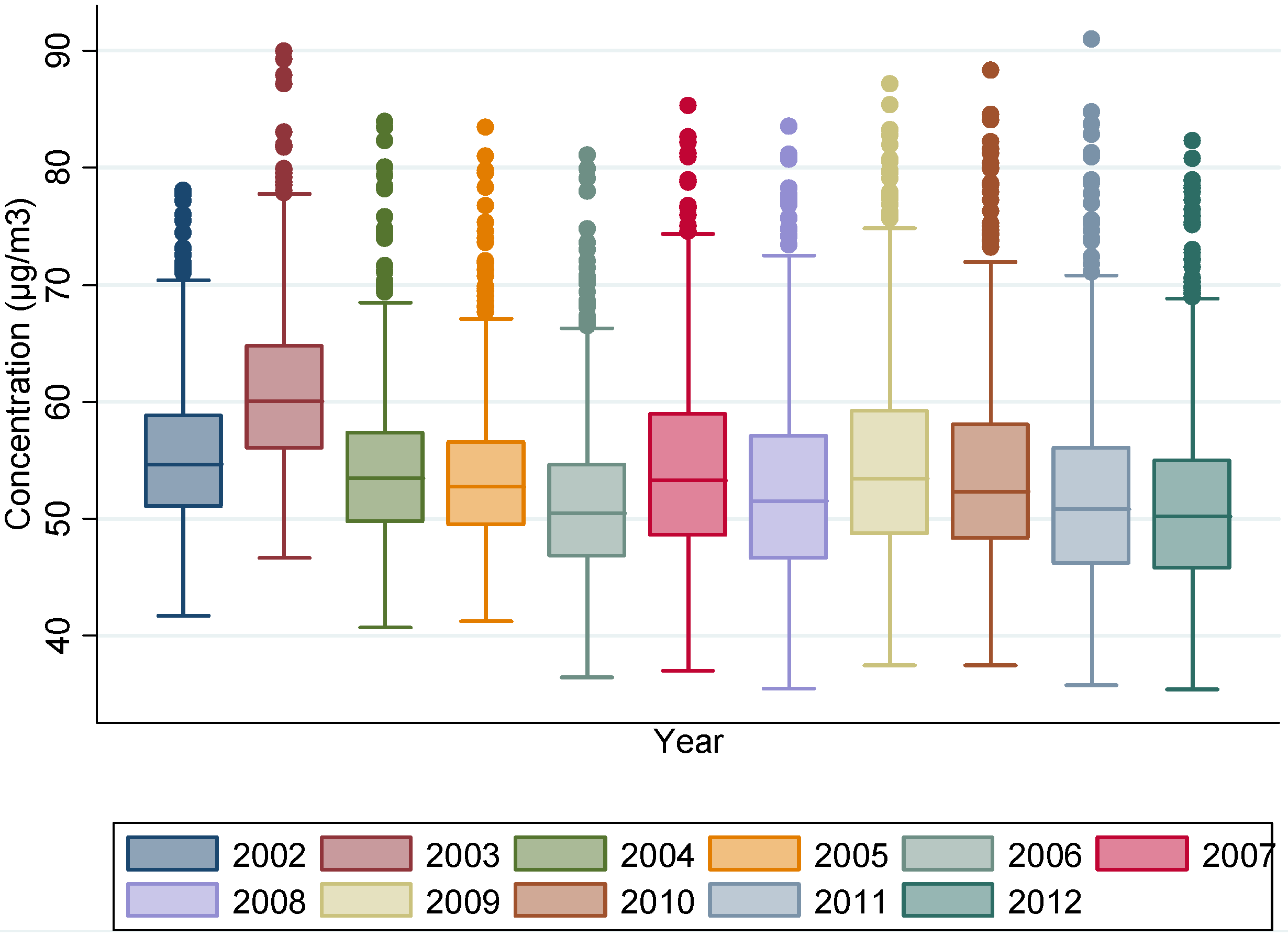
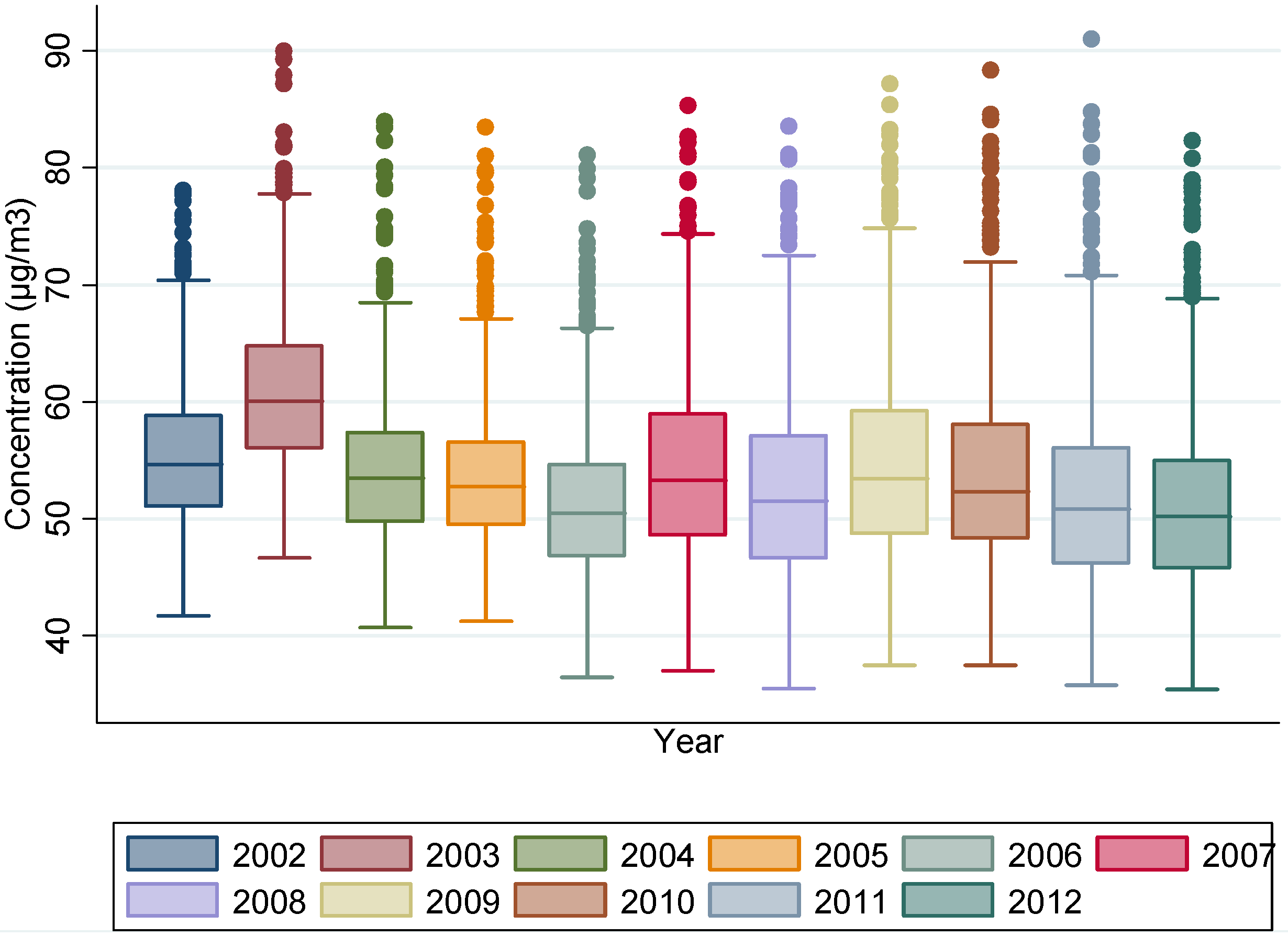
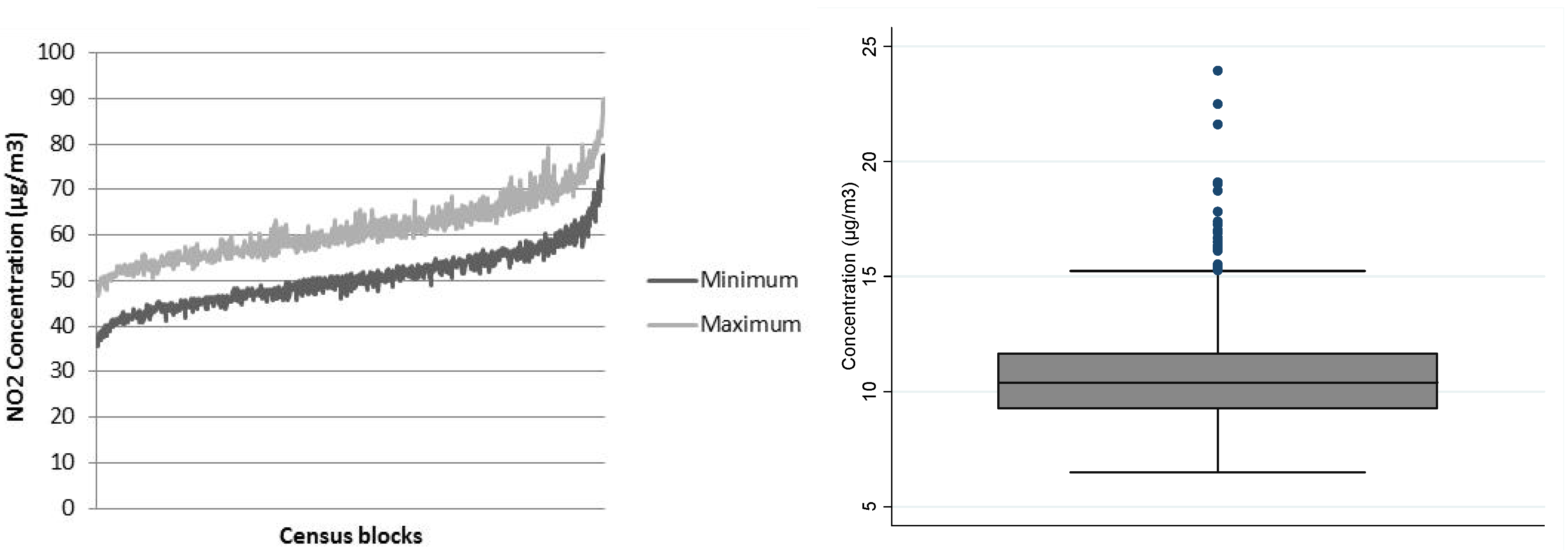
4.2. Step1: Annual NO2 Concentrations between 2002 and 2012 at the Census Block Level
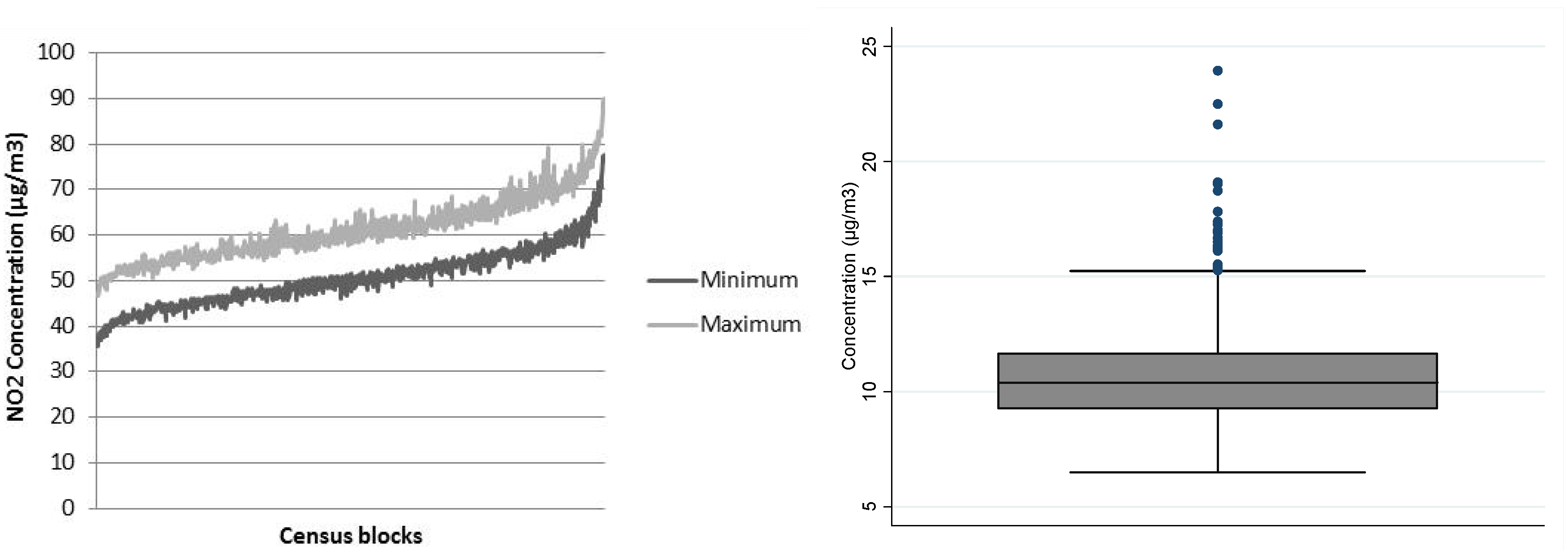
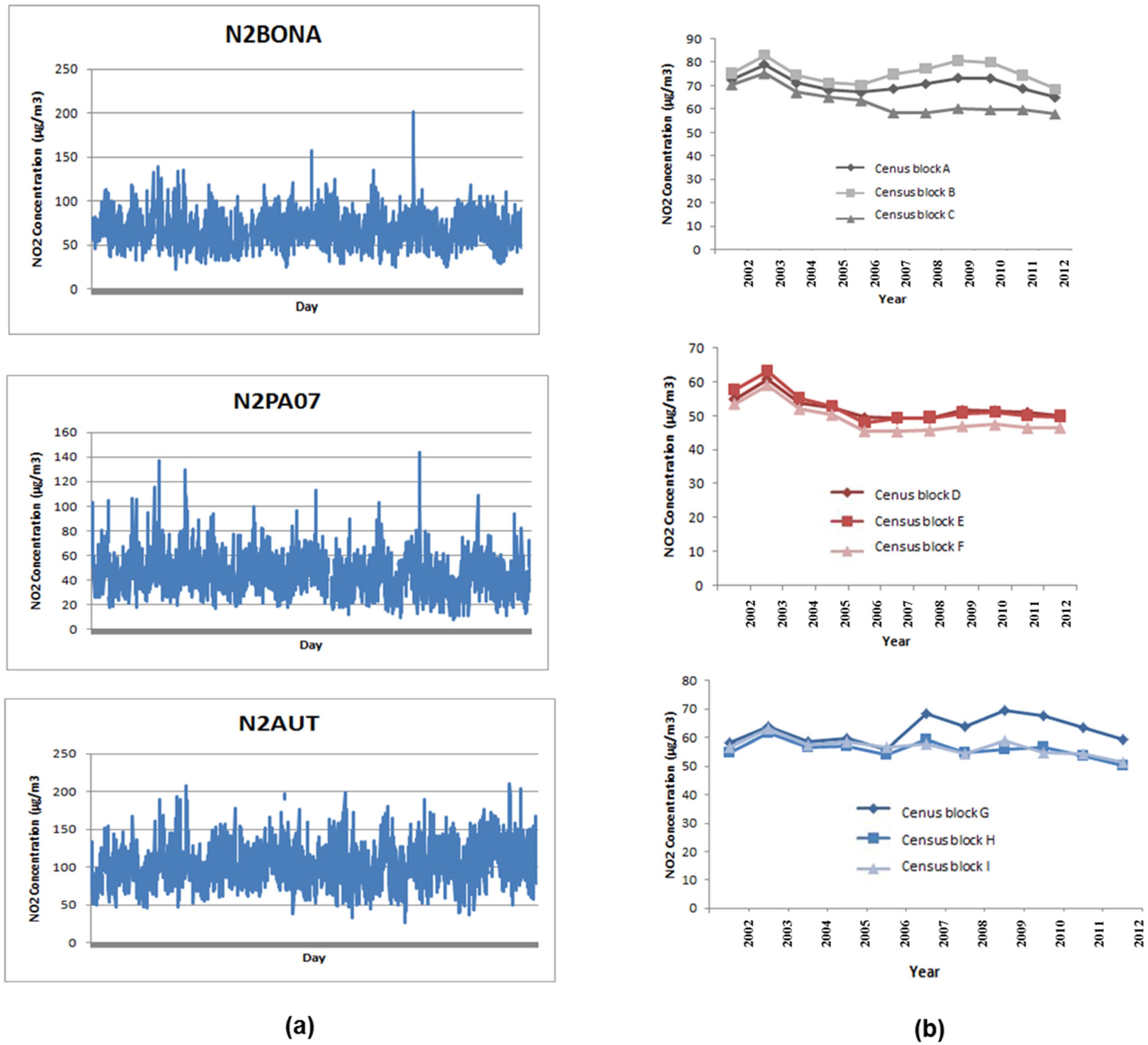
4.3. Step 2: Assessment of the Spatial Representativity of the Air Quality Monitoring Stations
4.4. Step 3. Illustration of Time Trends during the Study Period (2002–2012)
4.5. Estimation of the Cumulative Exposure Accounting for Residential Mobility
5. Discussion and Perspective
6. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- WHO. Ambient (Outdoor) Air Quality and Health. Fact Sheet N°313. Updated March 2014. Available online: http://www.who.int/mediacentre/factsheets/fs313/en/ (accessed on 10 November 2015).
- Hart, J.E.; Garshick, E.; Dockery, D.W.; Smith, T.J.; Ryan, L.; Laden, F. Long-term ambient multipollutant exposures and mortality. Am. J. Respir. Crit. Care Med. 2011, 183, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Lepeule, J.; Laden, F.; Dockery, D.; Schwartz, J. Chronic exposure to fine particles and mortality: An extended follow-up of the Harvard Six Cities study from 1974 to 2009. Environ. Health Perspect. 2012, 120, 965–970. [Google Scholar] [CrossRef] [PubMed]
- Hoek, G.; Krishnan, R.M.; Beelen, R.; Peters, A.; Ostro, B.; Brunekreef, B.; Kaufman, J.D. Long-term air pollution exposure and cardio- respiratory mortality: A review. Environ. Health 2013, 12, 43. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Goldberg, M.S.; Villeneuve, P.J. A systematic review of the relation between long-term exposure to ambient air pollution and chronic diseases. Rev. Environ. Health 2008, 23, 243–297. [Google Scholar] [PubMed]
- Filleul, L.; Rondeau, V.; Vandentorren, S.; Le Moual, N.; Cantagrel, A.; Annesi-Maesano, I.; Charpin, D.; Declercq, C.; Neukirch, F.; Paris, C.; et al. Twenty five year mortality and air pollution: Results from the French PAARC survey. Occup. Environ. Med. 2005, 62, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Bentayeb, M.; Wagner, V.; Stempfelet, M.; Zins, M.; Goldberg, M.; Pascal, M.; Larrieu, S.; Beaudeau, P.; Cassadou, S.; Eilstein, D.; et al. Association between long-term exposure to air pollution and mortality in France: A 25-year follow-up study. Environ. Int. 2015, 85, 5–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nyberg, F.; Gustavsson, P.; Järup, L.; Bellander, T.; Berglind, N.; Jakobsson, R.; Pershagen, G. Urban air pollution and lung cancer in Stockholm. Epidemiology 2000, 11, 487–495. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.D.; Rajagopalan, S.; Pope, C.A.; Brook, J.R.; Bhatnagar, A.; Diez-Roux, A.V.; Holguin, F.; Hong, Y.; Luepker, R.V.; Mittleman, M.A.; et al. American Heart Association Council on Epidemiology and Prevention, Council on the Kidney in Cardiovascular Disease, and Council on Nutrition, Physical Activity and Metabolism Particulate matter air pollution and cardiovascular disease: An update to the scientific statement from the American Heart Association. Circulation 2010, 121, 2331–2378. [Google Scholar] [PubMed]
- Brook, R.D.; Franklin, B.; Cascio, W.; Hong, Y.; Howard, G.; Lipsett, M.; Luepker, R.; Mittleman, M.; Samet, J.; Smith, S.C.; et al. Expert Panel on Population and Prevention Science of the American Heart Association Air pollution and cardiovascular disease: A statement for healthcare professionals from the Expert Panel on Population and Prevention Science of the American Heart Association. Circulation 2004, 109, 2655–2671. [Google Scholar] [PubMed]
- World Health Organization: Outdoor Air Pollution Causes Cancer. Available online: http://www.cancer.org/cancer/news/world-health-organization-outdoor-air-pollution-causes-cancer (accessed on 10 November 2015).
- Dockery, D.W.; Pope, C.A.; Xu, X.; Spengler, J.D.; Ware, J.H.; Fay, M.E.; Ferris, B.G.; Speizer, F.E. An association between air pollution and mortality in six U.S. cities. N. Engl. J. Med. 1993, 329, 1753–1759. [Google Scholar] [CrossRef] [PubMed]
- Laden, F.; Schwartz, J.; Speizer, F.E.; Dockery, D.W. Reduction in fine particulate air pollution and mortality: Extended follow-up of the Harvard Six Cities study. Am. J. Respir. Crit. Care Med. 2006, 173, 667–672. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A.; Burnett, R.T.; Thun, M.J.; Calle, E.E.; Krewski, D.; Ito, K.; Thurston, G.D. Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. JAMA 2002, 287, 1132–1141. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A.; Thun, M.J.; Namboodiri, M.M.; Dockery, D.W.; Evans, J.S.; Speizer, F.E.; Heath, C.W. Particulate air pollution as a predictor of mortality in a prospective study of U.S. adults. Am. J. Respir. Crit. Care Med. 1995, 151, 669–674. [Google Scholar] [CrossRef] [PubMed]
- Jerrett, M.; Burnett, R.T.; Ma, R.; Pope, C.A.; Krewski, D.; Newbold, K.B.; Thurston, G.; Shi, Y.; Finkelstein, N.; Calle, E.E.; Thun, M.J. Spatial analysis of air pollution and mortality in Los Angeles. Epidemiology 2005, 16, 727–736. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.A.; Siscovick, D.S.; Sheppard, L.; Shepherd, K.; Sullivan, J.H.; Anderson, G.L.; Kaufman, J.D. Long-term exposure to air pollution and incidence of cardiovascular events in women. N. Engl. J. Med. 2007, 356, 447–458. [Google Scholar] [CrossRef] [PubMed]
- Puett, R.C.; Hart, J.E.; Yanosky, J.D.; Paciorek, C.; Schwartz, J.; Suh, H.; Speizer, F.E.; Laden, F. Chronic fine and coarse particulate exposure, mortality, and coronary heart disease in the Nurses’ Health Study. Environ. Health Perspect. 2009, 117, 1697–1701. [Google Scholar] [CrossRef] [PubMed]
- Zeger, S.L.; Dominici, F.; McDermott, A.; Samet, J.M. Mortality in the Medicare population and chronic exposure to fine particulate air pollution in urban centers (2000–2005). Environ. Health Perspect. 2008, 116, 1614–1619. [Google Scholar] [CrossRef] [PubMed]
- Beelen, R.; Hoek, G.; van den Brandt, P.A.; Goldbohm, R.A.; Fischer, P.; Schouten, L.J.; Jerrett, M.; Hughes, E.; Armstrong, B.; Brunekreef, B. Long-term effects of traffic-related air pollution on mortality in a Dutch cohort (NLCS-AIR study). Environ. Health Perspect. 2008, 116, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Cesaroni, G.; Badaloni, C.; Gariazzo, C.; Stafoggia, M.; Sozzi, R.; Davoli, M.; Forastiere, F. Long-term exposure to urban air pollution and mortality in a cohort of more than a million adults in Rome. Environ. Health Perspect. 2013, 121, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Stafoggia, M.; Cesaroni, G.; Peters, A.; Andersen, Z.J.; Badaloni, C.; Beelen, R.; Caracciolo, B.; Cyrys, J.; de Faire, U.; de Hoogh, K.; Eriksen, K.T.; et al. Long-term exposure to ambient air pollution and incidence of cerebrovascular events: Results from 11 European cohorts within the ESCAPE project. Environ. Health Perspect. 2014, 122, 919–925. [Google Scholar] [CrossRef] [PubMed]
- Hystad, P.; Villeneuve, P.J.; Goldberg, M.S.; Crouse, D.L.; Johnson, K. Exposure to traffic-related air pollution and the risk of developing breast cancer among women in eight Canadian provinces: A case–control study. Environment International 2015, 74, 240–248. [Google Scholar] [CrossRef] [PubMed]
- Lipsett, M.J.; Ostro, B.D.; Reynolds, P.; Goldberg, D.; Hertz, A.; Jerrett, M.; Smith, D.F.; Garcia, C.; Chang, E.T.; Bernstein, L. Long-term exposure to air pollution and cardiorespiratory disease in the California teachers study cohort. Am. J. Respir. Crit. Care Med. 2011, 184, 828–835. [Google Scholar] [CrossRef] [PubMed]
- Zou, B.; Wilson, J.G.; Zhan, F.B.; Zeng, Y. Air pollution exposure assessment methods utilized in epidemiological studies. J. Environ. Monit. 2009, 11, 475–490. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; Yang, C.; Li, J.; Chen, R.; Chen, B.; Gu, D.; Kan, H. Association between long-term exposure to outdoor air pollution and mortality in China: A cohort study. J. Hazard. Mater. 2011, 186, 1594–1600. [Google Scholar] [CrossRef] [PubMed]
- Bentayeb, M.; Stempfelet, M.; Wagner, V.; Zins, M.; Bonenfant, S.; Songeur, C.; Sanchez, O.; Rosso, A.; Brulfert, G.; Rios, I.; Chaxel, E.; et al. Retrospective modeling outdoor air pollution at a fine spatial scale in France, 1989–2008. Atmos. Environ. 2014, 92, 267–279. [Google Scholar] [CrossRef]
- Gehring, U.; Heinrich, J.; Krämer, U.; Grote, V.; Hochadel, M.; Sugiri, D.; Kraft, M.; Rauchfuss, K.; Eberwein, H.G.; Wichmann, H.-E. Long-term exposure to ambient air pollution and cardiopulmonary mortality in women. Epidemiology 2006, 17, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Heinrich, J.; Thiering, E.; Rzehak, P.; Krämer, U.; Hochadel, M.; Rauchfuss, K.M.; Gehring, U.; Wichmann, H.-E. Long-term exposure to NO2 and PM10 and all-cause and cause-specific mortality in a prospective cohort of women. Occup. Environ. Med. 2013, 70, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Ueda, K.; Nagasawa, S.-Y.; Nitta, H.; Miura, K.; Ueshima, H. NIPPON DATA80 Research Group Exposure to particulate matter and long-term risk of cardiovascular mortality in Japan: NIPPON DATA80. J. Atheroscler. Thromb. 2012, 19, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.; Davis, J.; Bina, W.F. Ambient air pollution is associated with the increased incidence of breast cancer in U.S. Int. J. Environ. Health Res. 2012, 22, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Eeftens, M.; Beelen, R.; Fischer, P.; Brunekreef, B.; Meliefste, K.; Hoek, G. Stability of measured and modelled spatial contrasts in NO(2) over time. Occup. Environ. Med. 2011, 68, 765–770. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Henderson, S.B.; Sbihi, H.; Allen, R.W.; Brauer, M. Temporal stability of land use regression models for traffic-related air pollution. Atmospheric Environment 2013, 64, 312–319. [Google Scholar] [CrossRef]
- Zhang, P.; Dong, G.; Sun, B.; Zhang, L.; Chen, X.; Ma, N.; Yu, F.; Guo, H.; Huang, H.; Lee, Y.L.; Tang, N.; Chen, J. Long-term exposure to ambient air pollution and mortality due to cardiovascular disease and cerebrovascular disease in Shenyang, China. PLoS ONE 2011, 6, e20827. [Google Scholar] [CrossRef] [PubMed]
- Crouse, D.L.; Peters, P.A.; van Donkelaar, A.; Goldberg, M.S.; Villeneuve, P.J.; Brion, O.; Khan, S.; Atari, D.O.; Jerrett, M.; Pope, C.A.; et al. Risk of nonaccidental and cardiovascular mortality in relation to long-term exposure to low concentrations of fine particulate matter: A Canadian national-level cohort study. Environ. Health Perspect. 2012, 120, 708–714. [Google Scholar] [CrossRef] [PubMed]
- Hales, S.; Blakely, T.; Woodward, A. Air pollution and mortality in New Zealand: Cohort study. J. Epidemiol. Community Health 2012, 66, 468–473. [Google Scholar] [CrossRef] [PubMed]
- Oudin, A.; Forsberg, B.; Strömgren, M.; Beelen, R.; Modig, L. Impact of residential mobility on exposure assessment in longitudinal air pollution studies: A sensitivity analysis within the ESCAPE project. Sci. World J. 2012, 2012, 125818. [Google Scholar] [CrossRef] [PubMed]
- Clark, N.A.; Demers, P.A.; Karr, C.J.; Koehoorn, M.; Lencar, C.; Tamburic, L.; Brauer, M. Effect of early life exposure to air pollution on development of childhood asthma. Environ. Health Perspect. 2010, 118, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Modig, L.; Torén, K.; Janson, C.; Jarvholm, B.; Forsberg, B. Vehicle exhaust outside the home and onset of asthma among adults. Eur. Respir. J. 2009, 33, 1261–1267. [Google Scholar] [CrossRef] [PubMed]
- Jacquemin, B.; Sunyer, J.; Forsberg, B.; Aguilera, I.; Briggs, D.; García-Esteban, R.; Götschi, T.; Heinrich, J.; Järvholm, B.; Jarvis, D.; et al. Home outdoor NO2 and new onset of self-reported asthma in adults. Epidemiology 2009, 20, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Künzli, N.; Bridevaux, P.-O.; Liu, L.-J.S.; Garcia-Esteban, R.; Schindler, C.; Gerbase, M.W.; Sunyer, J.; Keidel, D.; Rochat, T. Swiss Cohort Study on Air Pollution and Lung Diseases in Adults Traffic-related air pollution correlates with adult-onset asthma among never-smokers. Thorax 2009, 64, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Andersen, Z.J.; Raaschou-Nielsen, O.; Ketzel, M.; Jensen, S.S.; Hvidberg, M.; Loft, S.; Tjønneland, A.; Overvad, K.; Sørensen, M. Diabetes incidence and long-term exposure to air pollution: A cohort study. Diabetes Care 2012, 35, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Gan, W.Q.; Koehoorn, M.; Davies, H.W.; Demers, P.A.; Tamburic, L.; Brauer, M. Long-term exposure to traffic-related air pollution and the risk of coronary heart disease hospitalization and mortality. Environ. Health Perspect. 2011, 119, 501–507. [Google Scholar] [CrossRef] [PubMed]
- AIRPARIF—Air Quality Assessment Network in the Paris Region. Air Quality in the Paris Region 2012. Available online: http://www.airparif.asso.fr/_pdf/publications/bilan-2012-anglais.pdf (accessed on 11 March 2016).
- Carruthers, D.J.; Edmunds, H.A.; Lester, A.E.; McHugh, C.A.; Singles, R.J. Use and validation of ADMS-Urban in contrasting urban and industrial locations. Int. J. Environ. Pollut. 2000, 14, 364–374. [Google Scholar] [CrossRef]
- Deguen, S.; Petit, C.; Delbarre, A.; Kihal, W.; Padilla, C.; Benmarhnia, T.; Lapostolle, A.; Chauvin, P.; Zmirou-Navier, D. Neighbourhood Characteristics and Long-Term Air Pollution Levels Modify the Association between the Short-Term Nitrogen Dioxide Concentrations and All-Cause Mortality in Paris. PLoS ONE 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonne, C.; Wilkinson, P. Long-term exposure to air pollution is associated with survival following acute coronary syndrome. Eur. Heart J. 2013, 34, 1306–1311. [Google Scholar] [CrossRef] [PubMed]
- Huss, A.; Spoerri, A.; Egger, M.; Röösli, M. ; Swiss National Cohort Study Group Aircraft noise, air pollution, and mortality from myocardial infarction. Epidemiology 2010, 21, 829–836. [Google Scholar] [CrossRef] [PubMed]
- Padilla, C.M.; Kihal-Talantikite, W.; Vieira, V.M.; Rossello, P.; Le Nir, G.; Zmirou-Navier, D.; Deguen, S. Air quality and social deprivation in four French metropolitan areas—A localized spatio-temporal environmental inequality analysis. Environ. Res. 2014, 134, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Padilla, C.M.; Deguen, S.; Lalloue, B.; Blanchard, O.; Beaugard, C.; Troude, F.; Navier, D.Z.; Vieira, V.M. Cluster analysis of social and environment inequalities of infant mortality. A spatial study in small areas revealed by local disease mapping in France. Sci. Total Environ. 2013, 454–455, 433–441. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Statistical Indicators | Year | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | |
| Mean * | 55.34 | 60.96 | 54.22 | 53.52 | 51.14 | 54.25 | 52.59 | 54.60 | 53.70 | 52.01 | 51.17 |
| Standard Deviation | 5.96 | 6.63 | 6.20 | 5.82 | 6.23 | 7.72 | 7.86 | 8.07 | 7.79 | 7.93 | 7.48 |
| Median * | 54.63 | 60.02 | 53.52 | 52.74 | 50.45 | 53.27 | 51.54 | 53.43 | 52.31 | 50.82 | 50.19 |
| Minimum * | 41.75 | 46.68 | 40.73 | 41.23 | 36.43 | 37.01 | 35.50 | 37.50 | 37.50 | 35.75 | 35.41 |
| Maximum * | 78.03 | 89.93 | 83.96 | 83.43 | 81.05 | 85.31 | 83.53 | 87.14 | 88.33 | 90.98 | 82.31 |
| Type of Monitoring Station | Name of Station | Mean * | EC | Total of Census Block |
|---|---|---|---|---|
| Urban | N2PA06 | 38.51 | 13.81 | 1 |
| Urban | N2PA07 | 41.35 | 14.57 | 316 |
| Urban | N2PA12 | 46.83 | 12.26 | 33 |
| Urban | N2PA13 | 40.75 | 12.05 | 1 |
| Urban | N2PA18 | 45.64 | 17.49 | 283 |
| Traffic | N2A1(AutA1) | 90.22 | 18.07 | 21 |
| Traffic | N2BONA | 66.38 | 11.476 | 69 |
| Traffic | N2AUT (BPAUT) | 100.39 | 24.70 | 29 |
| Traffic | N2BASC | 91.63 | 19.09 | 45 |
| Arrondissement | Degree of Mobility (%) | Cumulative Exposure without Residential Mobility * | Cumulative Exposure with Residential Mobility * | Relative Difference * |
|---|---|---|---|---|
| Arrondissement 15 | 19.0 | 44.23 | 38.64 | 5.59 |
| Arrondissement 17 | 18.5 | 49.91 | 44.00 | 5.91 |
| Arrondissement 14 | 18.4 | 42.17 | 37.75 | 4.42 |
| Arrondissement 11 | 18.4 | 45.74 | 41.14 | 4.60 |
| Arrondissement 10 | 18.3 | 48.15 | 43.76 | 4.39 |
| Arrondissement 9 | 17.1 | 46.99 | 43.32 | 3.66 |
| Arrondissement 16 | 17.0 | 46.10 | 40.81 | 5.29 |
| Arrondissement 18 | 16.5 | 47.56 | 42.89 | 4.67 |
| Arrondissement 5 | 16.2 | 44.60 | 40.66 | 3.94 |
| Arrondissement 2 | 15.8 | 46.64 | 43.51 | 3.13 |
| Arrondissement 3 | 15.6 | 49.10 | 45.55 | 3.55 |
| Arrondissement 8 | 15.4 | 48.00 | 44.46 | 3.54 |
| Arrondissement 7 | 15.4 | 44.60 | 40.42 | 4.18 |
| Arrondissement 12 | 15.3 | 46.09 | 42.30 | 3.78 |
| Arrondissement 13 | 14.6 | 41.07 | 37.94 | 3.13 |
| Arrondissement 20 | 14.1 | 45.51 | 42.46 | 3.05 |
| Arrondissement 6 | 13.1 | 45.84 | 42.07 | 3.77 |
| Arrondissement 4 | 12.7 | 49.17 | 45.67 | 3.50 |
| Arrondissement 19 | 12.6 | 45.91 | 43.20 | 2.71 |
| Arrondissement 1 | 8.8 | 50.46 | 47.34 | 3.11 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wahida, K.-T.; Padilla, C.M.; Denis, Z.-N.; Olivier, B.; Géraldine, L.N.; Philippe, Q.; Séverine, D. A Conceptual Framework for the Assessment of Cumulative Exposure to Air Pollution at a Fine Spatial Scale. Int. J. Environ. Res. Public Health 2016, 13, 319. https://doi.org/10.3390/ijerph13030319
Wahida K-T, Padilla CM, Denis Z-N, Olivier B, Géraldine LN, Philippe Q, Séverine D. A Conceptual Framework for the Assessment of Cumulative Exposure to Air Pollution at a Fine Spatial Scale. International Journal of Environmental Research and Public Health. 2016; 13(3):319. https://doi.org/10.3390/ijerph13030319
Chicago/Turabian StyleWahida, Kihal-Talantikite, Cindy M. Padilla, Zmirou-Navier Denis, Blanchard Olivier, Le Nir Géraldine, Quenel Philippe, and Deguen Séverine. 2016. "A Conceptual Framework for the Assessment of Cumulative Exposure to Air Pollution at a Fine Spatial Scale" International Journal of Environmental Research and Public Health 13, no. 3: 319. https://doi.org/10.3390/ijerph13030319