
Are Non-Pharmacological Interventions Effective in Reducing Drug Use and Criminality? A Systematic and Meta-Analytical Review with an Economic Appraisal of These Interventions

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy for Identification of Studies
2.2. Criteria for Inclusion and Exclusion of Studies
2.2.1. Selection Criteria
2.2.2. Study Design
2.2.3. Selection of Participants
2.2.4. Intervention Type
2.2.5. Outcomes Measures
2.2.6. Excluded Studies
2.2.7. Screening and Coding Process
2.2.8. Quality Assessment
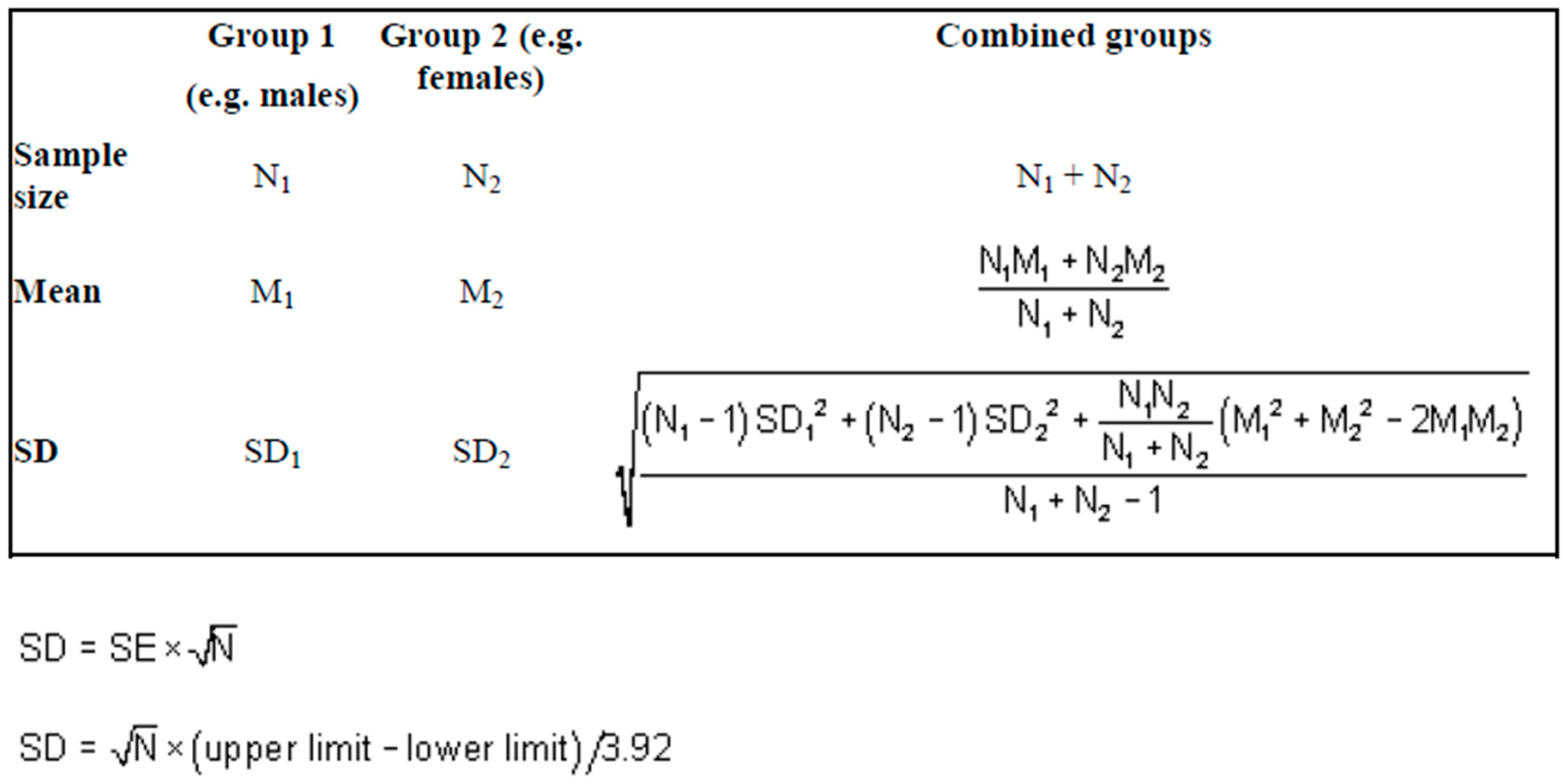
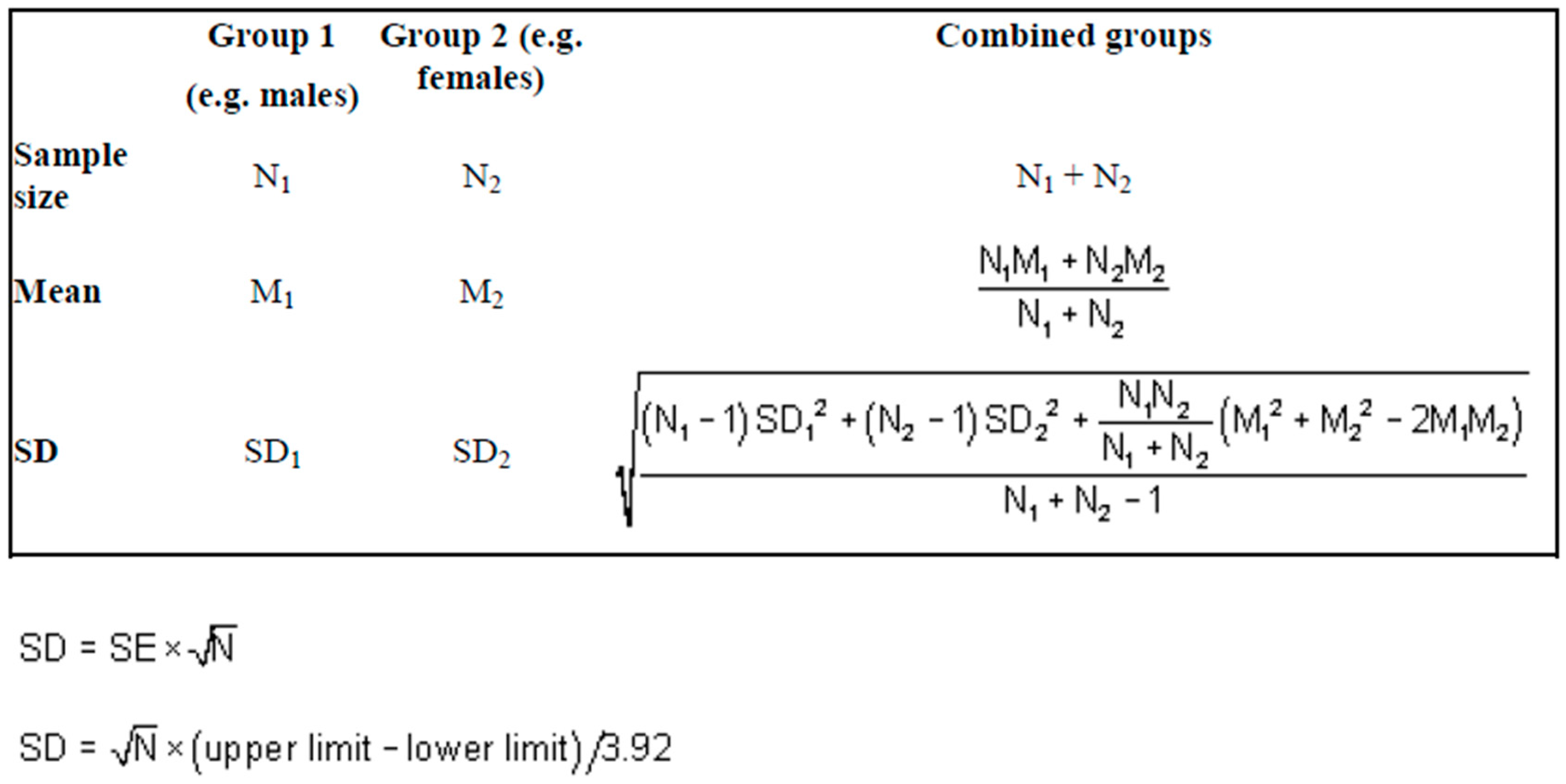
2.2.9. Statistical Methods
2.2.10. Economic Appraisal
3. Results
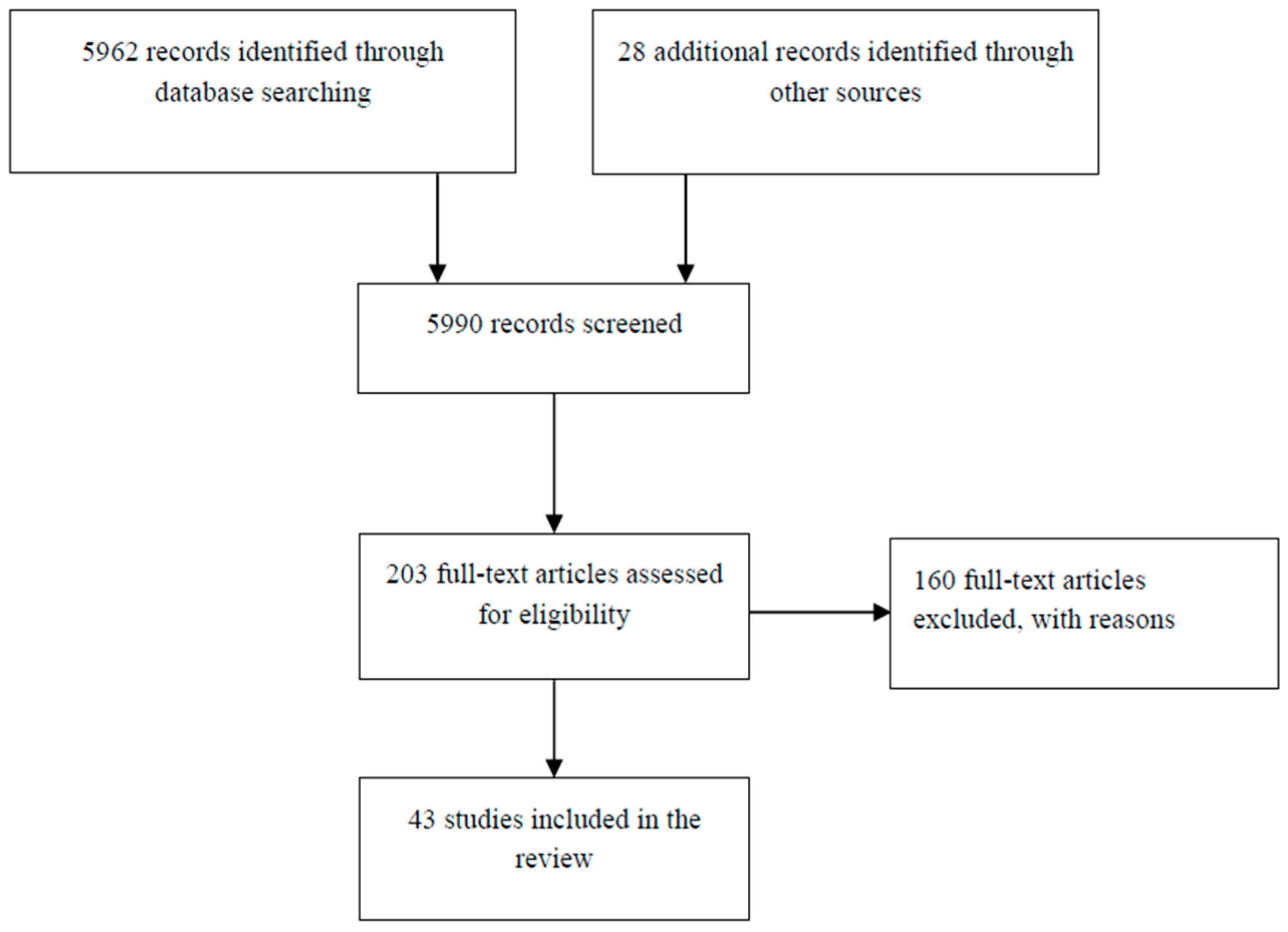
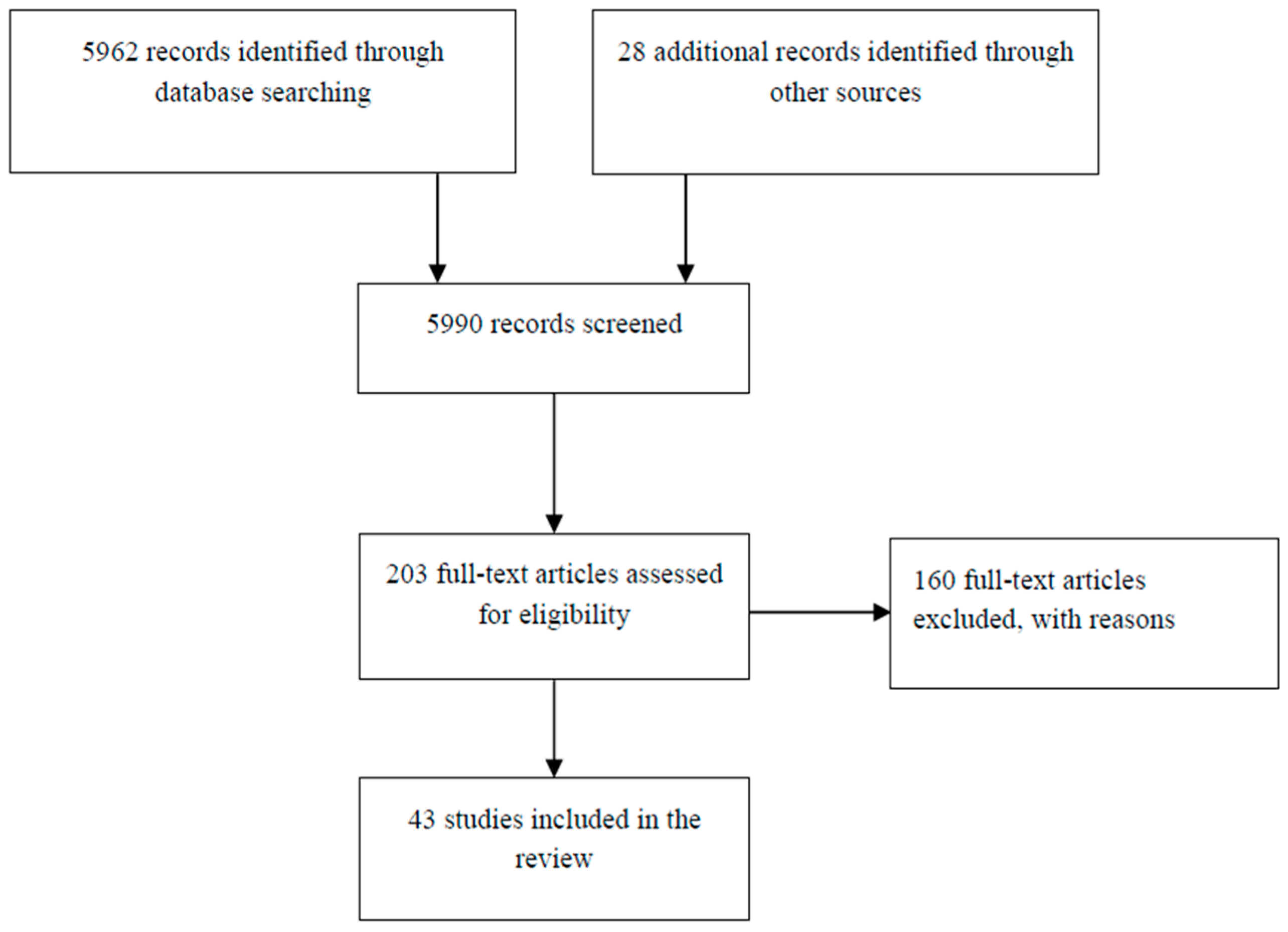
3.1. Search Findings
3.2. Overview of Studies
3.2.1. Meta Analyses
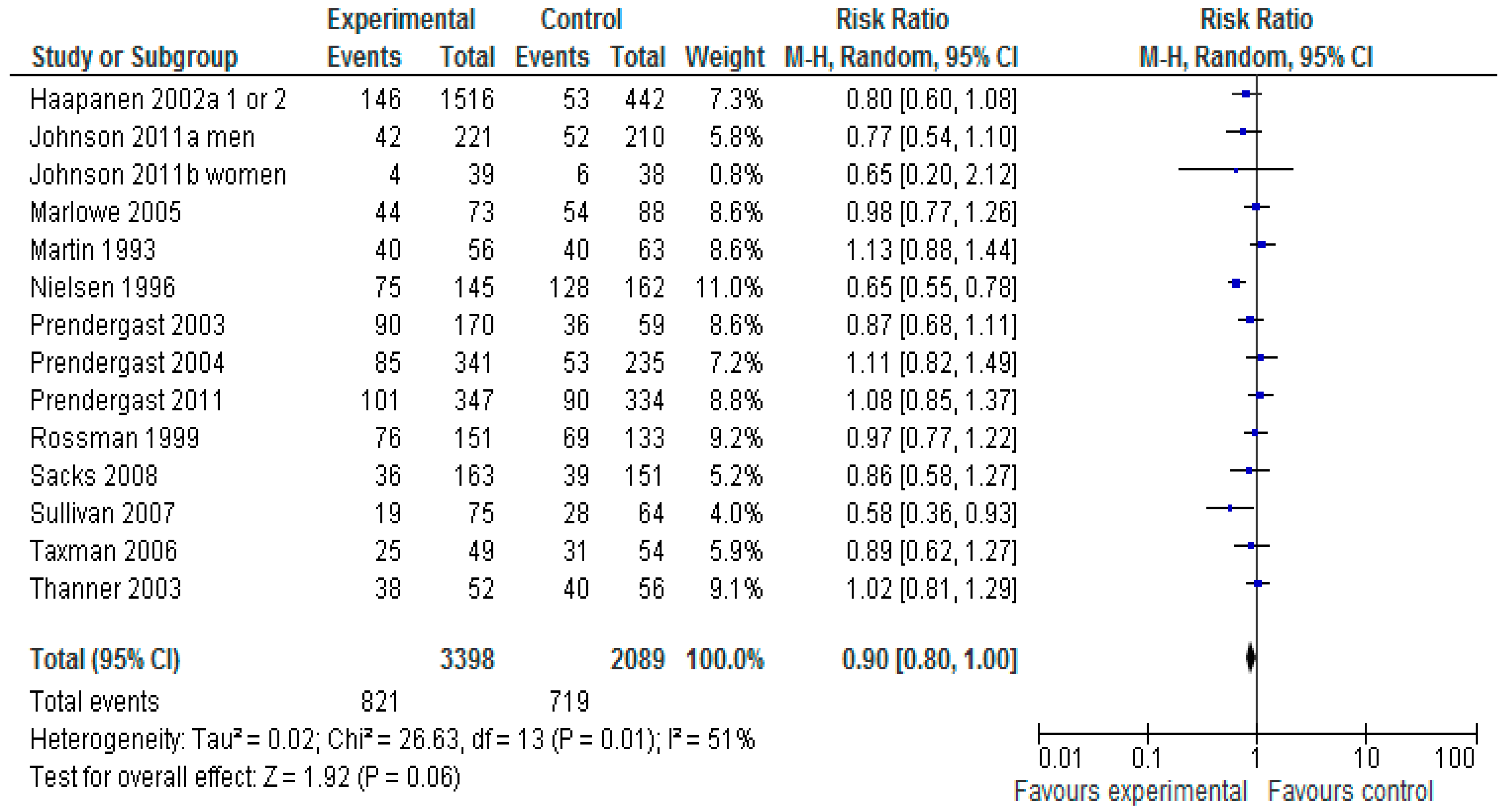
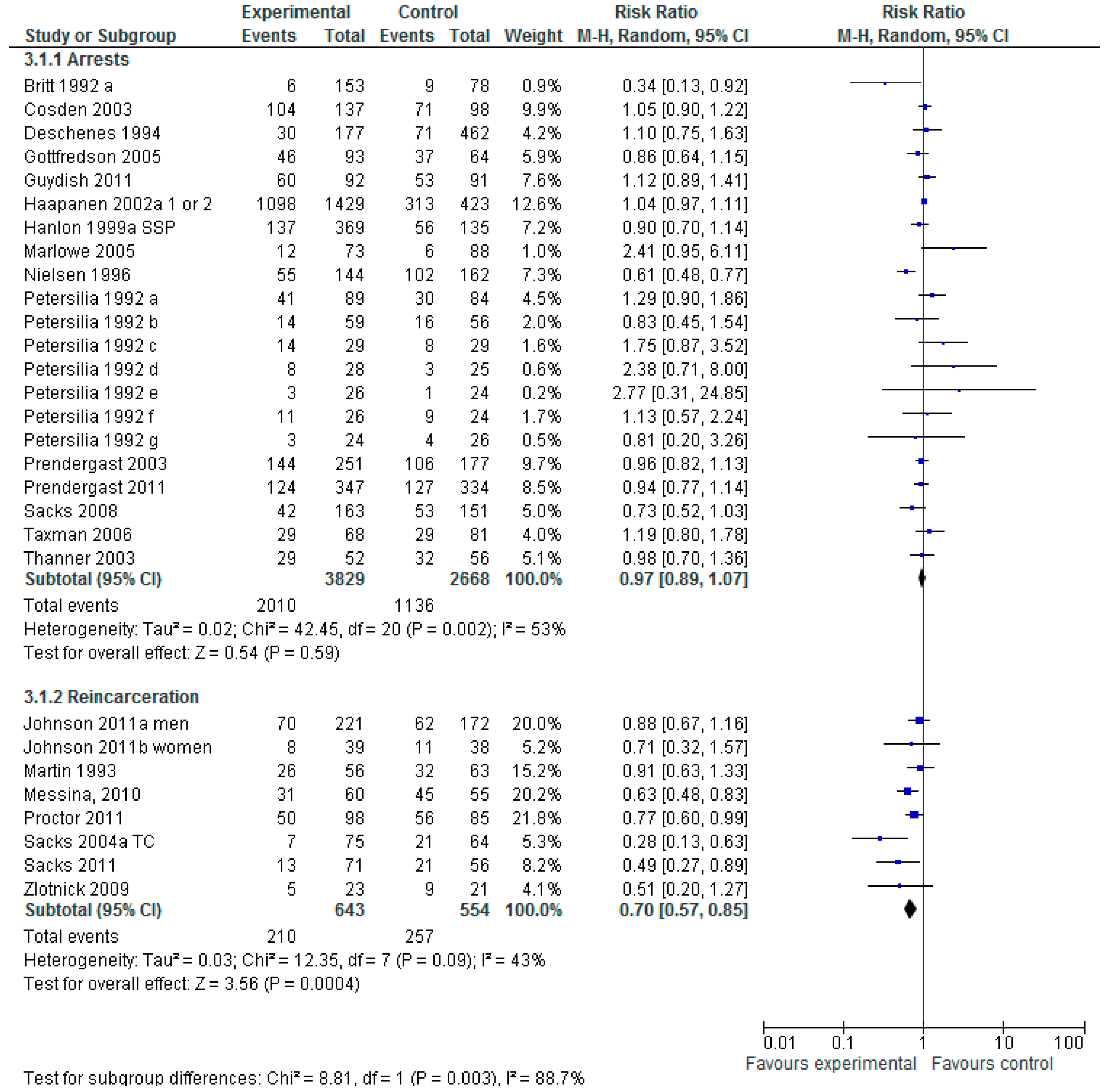
3.2.2. Does Any Type of Non-Pharmacological Treatment for Drug Using Offenders Reduce Criminal Activity?
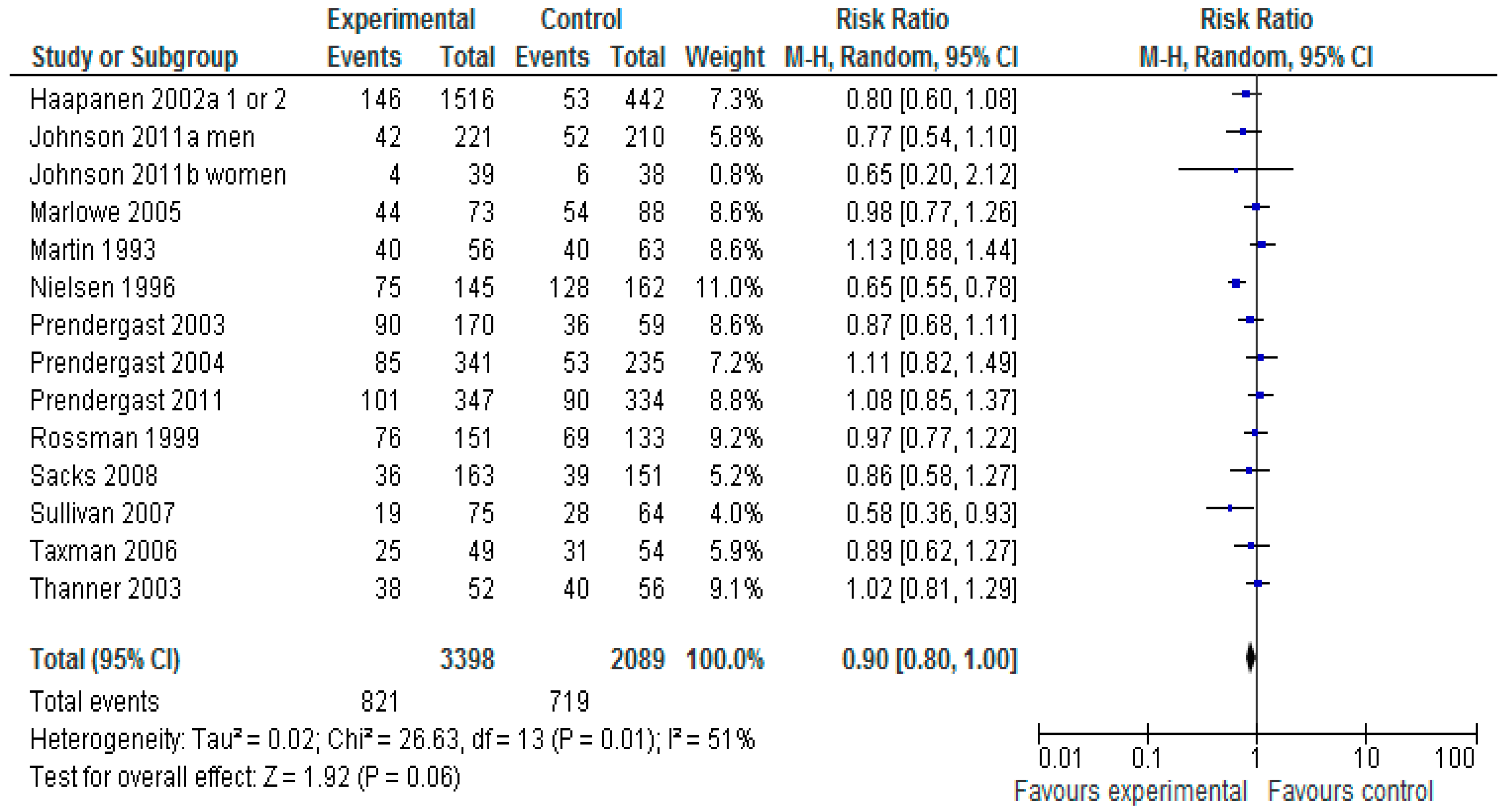
3.2.3. Does Any Non-Pharmacological Treatment for Drug Using Offenders Reduce Drug Use?
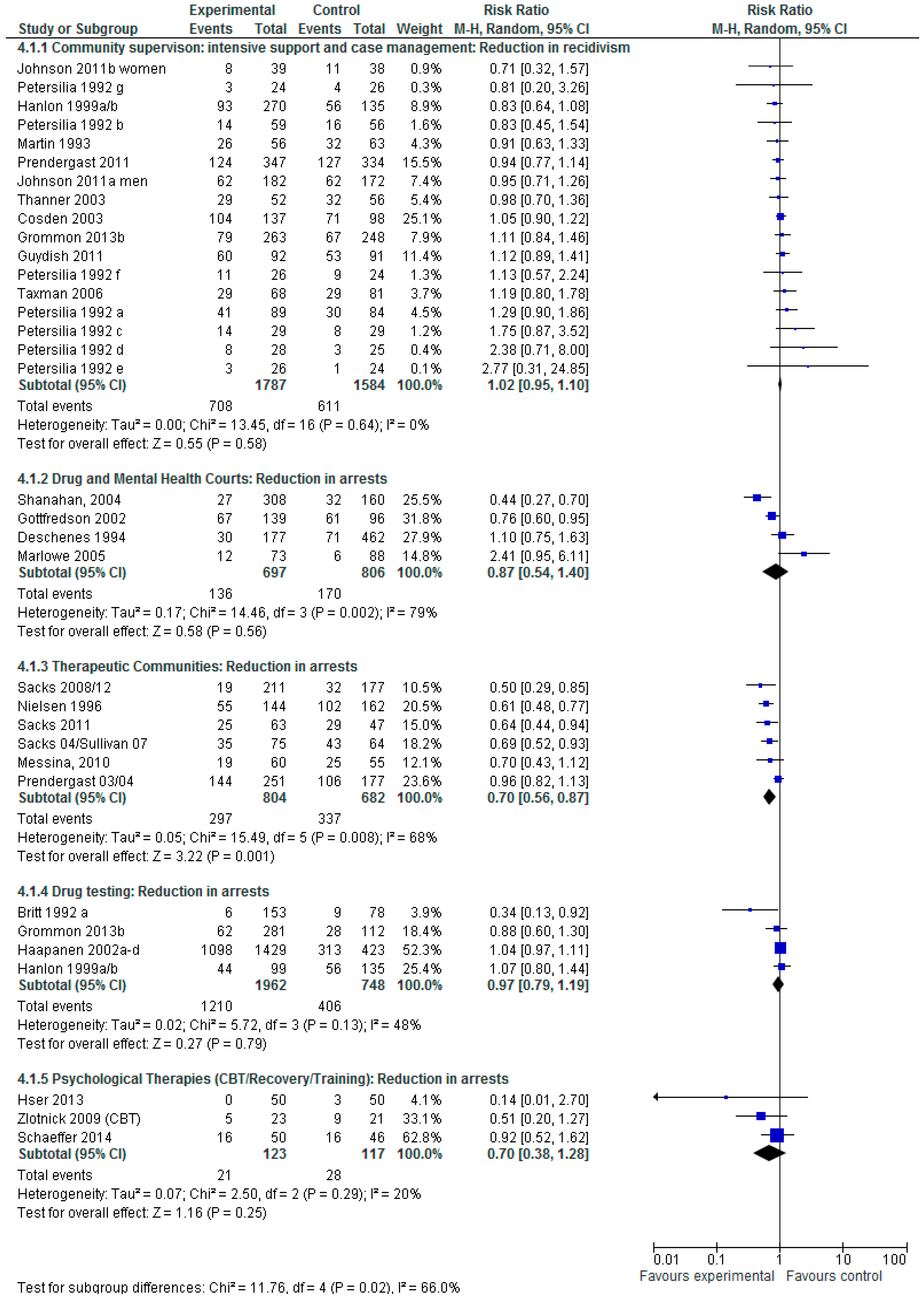
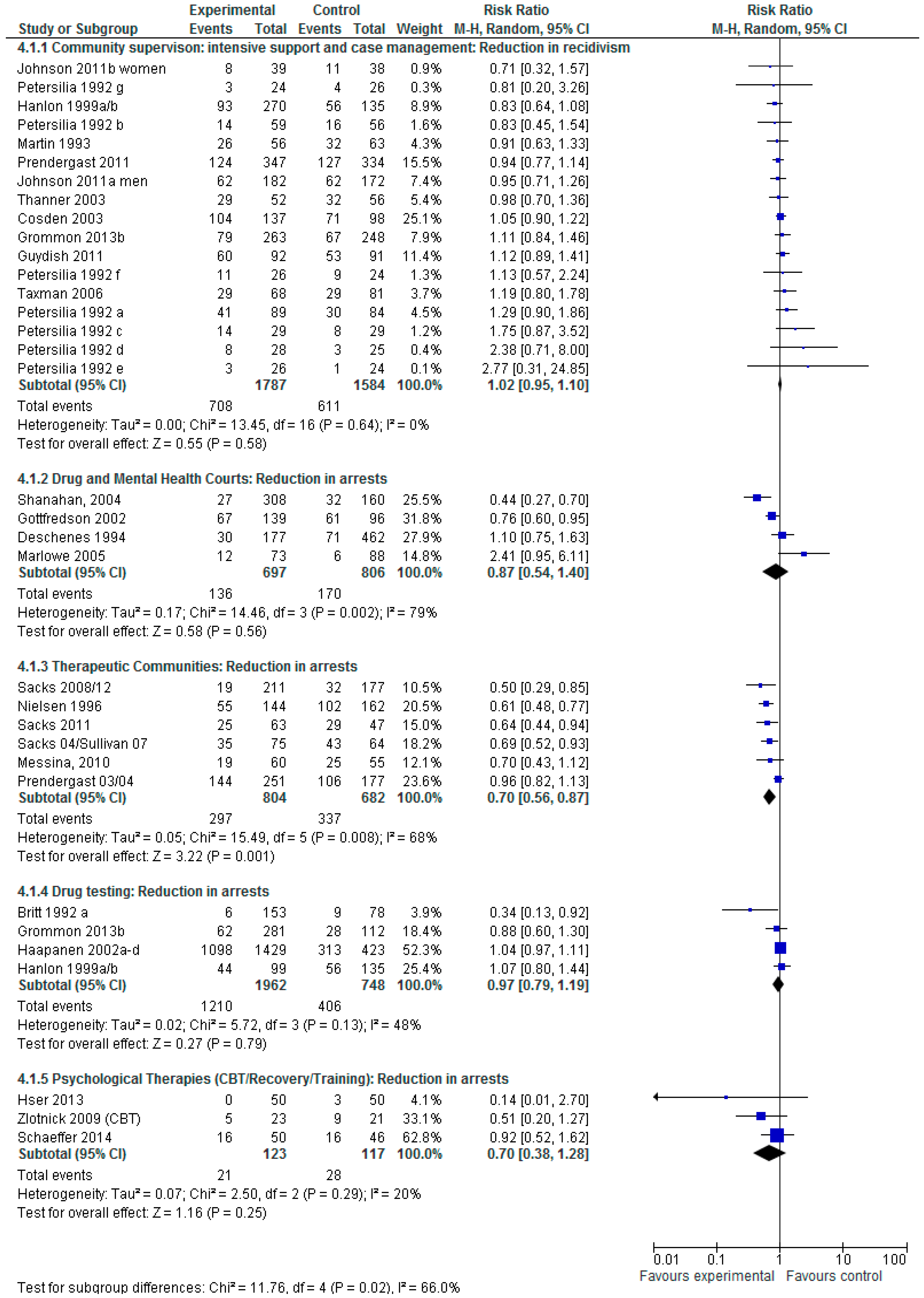
3.2.4. Does Intervention Type Have an Impact on Subsequent Criminal Activity?
3.2.5. Quality Assessment
4. Economic Appraisal
5. Discussion
6. Limitations
7. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Brooke, D.; Taylor, C.; Gunn, J.; Maden, A. Point Prevalence of Mental Disorder in Un-convicted Male Prisoners in England and Wales. Br. Med. J. 1996, 313, 1524–1527. [Google Scholar] [CrossRef]
- Fazel, S.; Bains, P.; Doll, H. Substance abuse and dependence in prisoners: A systematic review. Addiction 2005, 101, 181–191. [Google Scholar] [CrossRef] [PubMed]
- Gerstein, D.R.; Harwood, H.J. Treating Drug Problems: A Study of the Evolution, Effectiveness, and Financing of Public and Private Drug Treatment Systems; National Academy Press: Washington, DC, USA, 1990. [Google Scholar]
- Gunn, J.; Maden, A.; Swinton, M. Treatment Needs of Prisoners with Psychiatric Disorders. Br. Med. J. 1991, 303, 338–341. [Google Scholar] [CrossRef]
- Lo, C.C.; Stephens, R.C. Drugs and prisoners: Treatment needs on entering prison. Am. J. Drug Alcohol Abuse 2000, 26, 229–245. [Google Scholar] [CrossRef] [PubMed]
- Mason, D.; Birmingham, L.; Grubin, D. Substance use in remand prisoners: A consecutive case study. Br. Med. J. 1997, 315, 18–21. [Google Scholar] [CrossRef]
- Greenfeld, L.A.; Snell, T.L. Women Offenders; U.S. Department of Justice, Office of Justice Programs, Bureau of Justice Statistics: Washington, DC, USA, 1999.
- Staton-Tindall, M.; Garner, B.R.; Morey, J.T.; Leukefeld, C.; Krietemeyer, J.; Saum, C.A.; Oser, C.B. Gender Differences in Treatment Engagement Among a Sample of Incarcerated Substance Abusers. Crim. Justice Behav. 2007, 34, 1143–1156. [Google Scholar] [CrossRef]
- Taxman, F.S. Supervision—Exploring the dimensions of effectiveness. Fed. Probat. 2002, 66, 14–27. [Google Scholar]
- Byford, S.; Barrett, B.; Metrebian, B.; Groshkova, N.; Cary, T.; Charles, M.; Lintzeris, V.; Strang, N. Cost-effectiveness of injectable opioid treatment vs. oral methadone for chronic heroin addiction. Br. J. Psychiatry 2013, 203, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Austin, C.; McClelland, R. Case management in the human services. Reflections of public policy. J. Case Manag. 1996, 6, 119–126. [Google Scholar]
- Partridge, S. Examining Case Management Models for Community Sentences; Home Office: London, UK, 2004. [Google Scholar]
- Marlowe, D.B.; Elwork, A.; Festinger, D.S.; McLellan, A.T. Drug policy by popular referendum: This too shall pass. J. Subst. Abuse Treat. 2003, 25, 213–221. [Google Scholar] [CrossRef]
- Hall, E.A.; Prendergast, M.L.; Roll, J.M.; Warda, U.S. Reinforcing abstinence and treatment participation among offenders in a drug diversion program: Are vouchers effective? Crim. Justice Behav. 2009, 36, 935–953. [Google Scholar] [CrossRef] [PubMed]
- Petersilia, J.; Turner, S.; Deschenes, E.P. Smat sentencing: The emergence of immediate sanctions. In Intensive Supervision Programs for Drug Offenders; Byrne, J.M., Lurigio, A.J., Eds.; Sage Publications Inc.: Newbury Park, CA, USA, 1992; pp. 18–37. [Google Scholar]
- Prendergast, M.L.; Hall, E.A.; Roll, J.; Warda, U.S. Use of vouchers to reinforce abstinence and positive behaviors among clients in a drug court treatment program. Subst. Abuse Treat. 2008, 35, 125–136. [Google Scholar]
- The Treatment and Supervision of Drug Dependent Offenders. Available online: www.ukdpc.org.uk/reports.shtml (accessed on 3 June 2015).
- Mitchell, O.; MacKenzie, D.; Wilson, D. The effectiveness of incarceration-based drug treatment on criminal behavior: A systematic review. Campbell Syst. Rev. 2012, 8, 18. [Google Scholar]
- Mitchell, O.; Wilson, D.; MacKenzie, D.L. The effectiveness of incarceration-based drug treatment on criminal behavior. Campbell Syst. Rev. 2016. [Google Scholar] [CrossRef]
- Mitchell, O.; Wilson, D.; Eggers, A.; MacKenzie, D. Drug Courts’ effects on criminal offending for juveniles and adults. Campbell Syst. Rev. 2012. [Google Scholar] [CrossRef]
- Higgins, S.T.; Roll, J.M.; Wong, C.J.; Tidey, J.W.; Dantona, R. Clinic and laboratory studies on the use. In Motivating Behavior Change among Illicit-Drug Abusers: Research on Contingency Management Interventions; Higgins, S.T., Silverman, K., Eds.; American Psychological Association: Washington, DC, USA, 1990; pp. 25–56. [Google Scholar]
- Lussier, J.P.; Heil, S.H.; Mongeon, J.A.; Badger, G.J.; Higgins, S.T. A meta-analysis of voucher based reinforcement therapy for substance use disorders. Addiction 2006, 101, 192–203. [Google Scholar] [CrossRef] [PubMed]
- Offender Incentives and Behavioural Management Strategies. Available online: http://www.csc-scc.gc.ca/research/005008-0214-01-eng.shtml (accessed on 3 June 2015).
- Silverman, K.; Chutuape, M.A.; Bigelow, G.E.; Stitzer, M.L. Voucher-based reinforcement of attendance by unemployed methadone patients in a job skills training program. Drug Alcohol Depend. 1996, 41, 197–207. [Google Scholar] [CrossRef]
- Lundahl, B.W.; Kunz, C.; Brownell, C.; Tollefson, D.; Burke, B.L. A meta-analysis of motivational interviewing: Twenty-five years of empirical studies. Res. Soc. Work Prac. 2010, 20, 137–160. [Google Scholar] [CrossRef]
- McMurran, M. Motivational Interviewing with offenders. A systematic review. Legal Criminol. Psychol. 2009, 14, 83–100. [Google Scholar] [CrossRef]
- Smedslund, G.; Berg, R.C.; Hammerstrøm, K.T.; Steiro, A.; Leiknes, K.A.; Dahl, H.M.; Karlsen, K. Motivational interviewing for substance abuse. Campbell Syst. Rev. 2011. [Google Scholar] [CrossRef]
- Beck, A.T. Depression: Clinical, Experimental, and Theoretical Aspects; Harper and Row: New York, NY, USA, 1967. [Google Scholar]
- Andrews, D.A.; Zinger, I.; Hoge, R.D.; Bonta, J.; Gendreau, P.; Cullen, F.T. Does correctional treatment work? A clinically relevant and psychologically informed meta-analysis. Criminology 1990, 28, 369–404. [Google Scholar]
- Lipsey, M.; Landenberger, N.A.; Wilson, S.J. Effects of Cognitive-Behavioral Programs for Criminal Offenders: A Systematic Review. Campbell Syst. Rev. 2011, 3, 6. [Google Scholar]
- Lipsey, M.; Wilson, D. Effective intervention for serious juvenile offenders: A synthesis of research. In Serious and Violent Juvenile Offenders: Risk Factors and Successful Intervention; Loeber, R., Farrington, D.P., Eds.; Sage Publications: Thousand Oaks, CA, USA, 1998; pp. 313–345. [Google Scholar]
- Prochaska, J.O.; Velicer, W.F. The transtheoretical model of health behaviour change. Am. J. Health Promot. 1997, 12, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Rollnick, S.; Miller, W.R. What is motivational interviewing? Behav. Cognit. Psychother. 1995, 23, 325–334. [Google Scholar] [CrossRef]
- Frattaroli, J. Experimental disclosure and its moderators: A meta-analysis. Psychol. Bull. 2006, 132, 823–865. [Google Scholar] [CrossRef] [PubMed]
- Camp, S.D.; Daggett, D.M.; Kwon, O.; Klein-Saffran, J. The effect of faith program participation on prison misconduct: The Life Connections Program. J. Crim. Justice 2008, 36, 389–395. [Google Scholar] [CrossRef]
- Weisburd, D. Justifying the use of non-experimental methods and disqualifying the use of randomized controlled trials: Challenging folklore in evaluation research in crime and justice. J. Exp. Criminol. 2010, 6, 209–227. [Google Scholar] [CrossRef]
- Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. Available online: www.cochrane-handbook.org (accessed on 3 June 2015).
- Drummond, M.; O’Brien, B.; Stoddart, G.; Torrance, G. Methods for the Economic Evaluation of Health Care Programmes, 2nd ed.; Oxford University Press: Oxford, New York, NY, USA, 1997. [Google Scholar]
- Wilson, D.B.; Mackenzie, D.L.; Mitchell, F.N. Effects of correctional boot camps on offending. Campbell Syst. Rev. 2003. [Google Scholar] [CrossRef]
- Forsberg, L.G.; Ernst, D.; Sundqvist, K.; Farbring, C.A. Motivational Interviewing delivered by existing prison staff: A randomized controlled study of effectiveness on substance use after release. Subst. Use Misuse 2011, 46, 1477–1485. [Google Scholar] [CrossRef] [PubMed]
- Hser, Y.-I.; Fu, L.; Wu, F.; Du, J.; Zhao, M. Pilot trial of a recovery management intervention for heroin addicts released from compulsory rehabilitation in China. J. Subst. Abuse Treat. 2013, 44, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Lanza, P.V.; Garcia, P.F.; Lamelas, F.R.; Gonzalez-Menendez, A. Acceptance and commitment therapy versus cognitive behavioral therapy in the treatment of substance use disorder with incarcerated women. J. Clin. Psychol. 2014, 70, 644–657. [Google Scholar] [CrossRef] [PubMed]
- Lanza, P.V.; Gonzalez-Menendez, A. Acceptance and Commitment Therapy for drug abuse in incarcerated women. Psicothema 2013, 25, 307–312. [Google Scholar]
- Jones, C.G. Early-phase outcomes from a randomized trial of intensive judicial supervision in an Australian Drug Court. Crim. Justice Behav. 2013, 40, 453–468. [Google Scholar] [CrossRef]
- Britt, I.C.; Gottfredson, M.R.; Goldkamp, J.S. Drug testing and pre-trial misconduct: An experiment on the specific deterrent effects of drug monitoring defendants on pre-trial release. J. Res. Crime Delinq. 1992, 29, 62–78. [Google Scholar] [CrossRef]
- Martin, S.; Scarpitt, S. An intensive case management approach for paroled IV drug users. J. Drug Issues 1993, 23, 43–59. [Google Scholar] [CrossRef]
- Hanlon, T.E.; Bateman, R.W.; O’Grady, K.E. The relative effects of three approaches to the parole supervision of narcotic addicts and cocaine abusers. Prison J. 1999, 79, 163–181. [Google Scholar] [CrossRef]
- Rossman, S.; Sridharan, S.; Gouvis, C.; Buck, J.; Morley, E. Impact of the Opportunity to Succeed (OPTS) aftercare program for substance-abusing felons. In Comprehensive Final Report; Urban Institute: Washington, DC, USA, 1999. [Google Scholar]
- Sacks, J.Y.; Sacks, S.; McKendrick, K.; Banks, S.; Schoeneberger, M.; Hamilton, Z.; Stommel, J.; Shoemaker, J. Prison Therapeutic Community Treatment for Female Offenders: Profiles and Preliminary Findings for Mental Health and Other Variables (Crime, Substance Use and HIV Risk). J. Offend. Rehabil. 2008, 46, 233–261. [Google Scholar] [CrossRef]
- Zlotnick, C.; Johnson, J.; Najavits, L.M. Randomized controlled pilot study of cognitive-behavioral therapy in a sample of incarcerated women with substance use disorder and PTSD. Behav. Ther. 2009, 40, 325–336. [Google Scholar] [CrossRef] [PubMed]
- Messina, N.; Grella, C.E.; Cartier, J.; Torres, S. A randomized experimental study of gender-responsive substance abuse treatment for women in prison. J. Subst. Abuse Treat. 2010, 38, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Guydish, J.; Chan, M.; Bostrom, A.; Jessup, M.; Davis, T.; Marsh, C. A Randomized Trial of Probation Case Management for Drug-Involved Women Offenders. Crime Delinq. 2011, 57, 167–198. [Google Scholar] [CrossRef] [PubMed]
- Sacks, S.; Sacks, J.Y.; McKendrick, K.; Banks, S.; Stommel, J. Modified TC for MICA offenders: Crime outcomes. Behav. Sci. Law 2004, 22, 477–501. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, C.J.; McKendrick, K.; Sacks, S.; Banks, S. Modified therapeutic community treatment for offenders with MICA disorders: Substance use outcomes. Am. J. Drug Alcohol Abuse 2007, 33, 823–832. [Google Scholar] [CrossRef] [PubMed]
- Sacks, S.; Chaple, M.; Sacks, J.Y.; McKendrick, K.; Cleland, C.M. Randomized trial of a reentry modified therapeutic community for offenders with co-occurring disorders: Crime outcomes. J. Subst. Abuse Treat. 2011, 42, 247–259. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.K.; Chamberlain, P.; Eddy, J.M.; Smith, D.K.; Chamberlain, P.; Eddy, J.M. Preliminary support for multidimensional treatment foster care in reducing substance use in delinquent boys. J. Child Adolesc. Subst. Abuse 2010, 19, 343–358. [Google Scholar] [CrossRef] [PubMed]
- Stein, L.A.; Lebeau, R.; Colby, S.M.; Barnett, N.P.; Golembeske, C.; Monti, P.M. Motivational interviewing for incarcerated adolescents: Effects of depressive symptoms on reducing alcohol and marijuana use after release. J. Stud. Alcohol Drug. 2011, 72, 497–506. [Google Scholar]
- Grommon, E.; Cox, S.M.; Davidson, W.S.; Bynum, T.S. Alternative models of instant drug testing: Evidence from an experimental trial. J. Exp. Criminol. 2013, 9, 145–168. [Google Scholar] [CrossRef] [Green Version]
- Grommon, E.; Davidson, W.S.; Bynum, T.S. A randomized trial of a multi-modal community-based prisoner re-entry program emphasizing substance abuse treatment. J. Offend. Rehabil. 2013, 52, 287–309. [Google Scholar] [CrossRef] [Green Version]
- Freudenberg, N.; Ramaswamy, M.; Daniels, J.; Crum, M.; Ompad, D.C.; Vlahov, D. Reducing drug use, human immunodeficiency virus risk, and recidivism among young men leaving jail: Evaluation of the REAL MEN re-entry program. J. Adolesc. Health 2010, 47, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Prendergast, M.; Hall, E.A.; Wexler, H.K. Multiple Measures of Outcome in Assessing a Prison-Based Drug Treatment Program. J. Offend. Rehabil. 2003, 37, 65–94. [Google Scholar] [CrossRef]
- Prendergast, M.; Hall, E.A.; Wexler, H.K.; Melnick, G.; Cao, Y. Amity prison-based therapeutic community: 5-year outcomes. Prison J. 2004, 84, 36–60. [Google Scholar] [CrossRef]
- Wexler, H.K.; DeLeon, G.; Thomas, G.; Kressel, D.; Peters, J. The Amity prison TC evaluation—Re incarceration outcomes. Crim. Justice Behav. 1999, 26, 147–167. [Google Scholar] [CrossRef]
- Wexler, H.K.; Melnick, G.; Lowe, L.; Peters, J. Three-Year Reincarceration Outcomes for Amity In-Prison Therapeutic Community and Aftercare in California. Prison J. 1999, 79, 321–336. [Google Scholar] [CrossRef]
- Proctor, S.L.; Hoffmann, N.G.; Allison, S. The Effectiveness of Interactive Journaling in Reducing Recidivism Among Substance-Dependent Jail Inmates. Int. J. Offend. Ther. Comp. Criminol. 2012, 56, 317–332. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, A.L.; Scarpitti, F.R.; Inciardi, J.A. Integrating the therapeutic community and work release for drug-involved offenders: The CREST Program. J. Subst. Abuse Treat. 1996, 13, 349–358. [Google Scholar] [CrossRef]
- Haapanen, R.; Britton, L. Drug testing for youthful offenders on parole: An experimental evaluation. Criminol. Public Policy 2002, 1, 217–244. [Google Scholar] [CrossRef]
- Johnson, J.E.; Zlotnick, C. Pilot study of treatment for major depression among women prisoners with substance use disorder. J. Psychiatr. Res. 2012, 46, 1174–1183. [Google Scholar] [CrossRef] [PubMed]
- Marlowe, D.B.; Festinger, D.S.; Dugosh, K.L.; Arabia, P.L.; Kirby, K.C. An effectiveness trial of contingency management in a felony pre-adjudication drug court. J. Appl. Behav. Anal. 2008, 41, 565–577. [Google Scholar] [CrossRef] [PubMed]
- Deschenes, E.; Greenwood, P. Maricopa-County Drug Court—An innovative program for 1st-time drug offenders on probation. Justice Syst. J. 1994, 17, 99–115. [Google Scholar] [CrossRef]
- Gottfredson, D.C.; Kearley, B.W.; Najaka, S.S.; Rocha, C.M. The Baltimore City Drug Treatment Court: 3-Year Self-Report Outcome Study. Eval. Rev. 2005, 29, 42–64. [Google Scholar] [CrossRef] [PubMed]
- Gottfredson, D.C.; Najaka, S.S.; Kearley, B.W. Effectiveness of drug treatment courts: Evidence from a randomized trial. Criminol. Public Policy 2003, 2, 171–196. [Google Scholar] [CrossRef]
- Gottfredson, D.C.; Najaka, S.S.; Kearley, B.W. Long-term effects of participation in the Baltimore City Drug Treatment Court: Results from an experimental study. J. Exp. Criminol. 2006, 2, 67–98. [Google Scholar] [CrossRef]
- Cosden, M.; Ellens, J.K.; Schnell, J.L.; Yamini-Diouf, Y.; Wolfe, M.M. Evaluation of a mental health treatment court with assertive community treatment. Behav. Sci. Law 2003, 21, 415–427. [Google Scholar] [CrossRef] [PubMed]
- Thanner, M.H.; Taxman, F.S. Responsivity: The value of providing intensive services to high-risk offenders. J. Subst. Abuse Treat. 2003, 24, 137–147. [Google Scholar] [CrossRef]
- Taxman, F.S.; Perdoni, M.L.; Harrison, L.D. Drug treatment services for adult offenders: The state of the state. J. Subst. Abuse Treat. 2007, 32, 239–254. [Google Scholar] [CrossRef] [PubMed]
- Schaeffer, C.M.; Henggeler, S.W.; Ford, J.D.; Mann, M.; Chang, R.; Chapman, J.E. RCT of a promising vocational/employment program for high-risk juvenile offenders. J. Subst. Abuse Treat. 2014, 46, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Prendergast, M.; Frisman, L.; Sacks, J.Y.; Staton-Tindall, M.; Greenwell, L.; Lin, H.-J.; Cartier, J. A multi-site, randomized study of strengths-based case management with substance-abusing parolees. J. Exp. Criminol. 2011, 7, 225–253. [Google Scholar] [CrossRef] [PubMed]
- Henggeler, S.W.; McCart, M.R.; Cunningham, P.B.; Chapman, J.E. Enhancing the effectiveness of juvenile drug courts by integrating evidence-based practices. J. Consult. Clin. Psychol. 2012, 80, 264–275. [Google Scholar] [CrossRef] [PubMed]
- Carroll, K.M.; Nich, C.; Lapaglia, D.M.; Peters, E.N.; Easton, C.J.; Petry, N.M. Combining cognitive behavioral therapy and contingency management to enhance their effects in treating cannabis dependence: Less can be more, more or less. Addiction 2012, 107, 1650–1659. [Google Scholar] [CrossRef] [PubMed]
- Sinha, R.; Easton, C.; Renee-Aubin, L.; Carroll, K.M. Engaging young probation-referred marijuana-abusing individuals in treatment: A pilot trial. Am. J. Addict. 2003, 12, 314–323. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, E.J.; Hunter, S.B.; Miles, J.N.; Ewing, B.A.; Osilla, K.C. A randomized controlled trial of a group motivational interviewing intervention for adolescents with a first time alcohol or drug offense. J. Subst. Abuse Treat. 2013, 45, 400–408. [Google Scholar] [CrossRef] [PubMed]
- Henggeler, S.W.; Pickrel, S.G.; Brondino, M.J. Multi-systemic treatment of substance-abusing and dependent delinquents: Outcomes, treatment fidelity, and transportability. Ment. Health Serv. Res. 1999, 1, 171–184. [Google Scholar] [CrossRef] [PubMed]
- McCollister, K.E.; French, M.T.; Sheidow, A.J.; Henggeler, S.W.; Halliday-Boykinds, C.A. Estimating the differential costs of criminal activity for juvenile drug court participants: Challenges and recommendations. J. Behav. Health Serv. Res. 2009, 36, 111–126. [Google Scholar] [CrossRef] [PubMed]
- Alemi, F.; Haack, M.; Nemes, S.; Harge, A.; Baghi, H. Impact of online counseling on drug use: A pilot study. Qual. Manag. Health Care 2010, 19, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Carroll, K.M.; Easton, C.J.; Nich, C.; Hunkele, K.A.; Neavins, T.M.; Sinha, R. The use of contingency management and motivational/skills-building therapy to treat young adults with marijuana dependence. J. Consult. Clin. Psychol. 2006, 74, 955–966. [Google Scholar] [CrossRef] [PubMed]
- Marlowe, D.B.; Festinger, D.S.; Dugosh, K.L.; Lee, P.A. Are judicial status hearings a “key component” of drug court? Six and twelve month outcomes. Drug Alcohol Depend. 2005, 79, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Taxman, F.S.; Meridith, T. Risk, need, and responsivity (RNR): It all depends. Crime Delinq. 2006, 52, 28–51. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.E.; Friedmann, P.D.; Green, T.C.; Harrington, M.; Taxman, F.S. Gender and treatment response in substance use treatment-mandated parolees. J. Subst. Abuse Treat. 2011, 40, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Gottfredson, D.C.; Exum, M.L. The Baltimore City drug treatment court: One-year results from a randomized study. J. Res. Crime Delinq. 2002, 39, 337–356. [Google Scholar] [CrossRef]
- Henggeler, S.W.; Halliday-Boykins, C.A.; Cunningham, P.B.; Randall, J.; Shapiro, S.B.; Chapman, J.E. Juvenile drug court: Enhancing outcomes by integrating evidence-based treatments. J. Consult. Clin. Psychol. 2006, 74, 42–54. [Google Scholar] [CrossRef] [PubMed]
- Sacks, J.Y.; McKendrick, K.; Hamilton, Z.K. A randomized clinical trial of a theraputic community treatment for female inmates: outcomes at 6 and 12 months after prison release. J. Addict. Dis. 2012, 31, 258–269. [Google Scholar] [CrossRef] [PubMed]
- Schoenwald, S.K.; Ward, D.M.; Henggeler, S.W.; Pickrel, S.G.; Patel, H. Multi-systemic therapy treatment of substance abusing or dependent adolescent offenders: Costs of reducing incarceration, inpatient, and residential placement. J. Child Family Stud. 1996, 5, 431–444. [Google Scholar] [CrossRef]
- Shanahan, M.; Lancsar, E.; Haas, M.; Lind, B.; Weatherburn, D.; Chen, S. Cost-effectiveness analysis of the New South. Wales adult drug court program. Eval. Rev. 2004, 28, 3–27. [Google Scholar] [CrossRef] [PubMed]
- Chandler, D.W.; Spicer, G. Integrated treatment for jail recidivists with co-occurring psychiatric and substance use disorders. Community Ment. Health J. 2006, 4, 406–425. [Google Scholar] [CrossRef] [PubMed]
- House of Commons and Home Affairs Office. Breaking the Cycle of Drugs: Home Office; The Stationery Office: London, UK, 2012. [Google Scholar]
- Shemilt, I.; Mugford, M.; Vale, L.; Marsh, K.; Donaldson, C.; Drummond, M.F. Evidence synthesis, economics and public policy. Res. Synth. Meth. 2010, 1, 126–135. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Are both Costs (Inputs) and Consequences (Outputs) of the Alternative Examined? | ||||
|---|---|---|---|---|
| Are two or more alternatives compared? | No | No | Yes | |
| Examine consequences only | Examine only costs | |||
| 1B PARTIAL EVALUATION 1B | 2 PARTIAL EVALUATION | |||
| Outcome Description | Cost description | Cost-outcome description | ||
| Yes | 3A PARTIAL EVALUATION 3B | 4 FULL ECONOMIC EVALUATION | ||
| Efficacy effectiveness evaluation (e.g., RCT) | Cost analysis | Cost effectiveness analysis Cost Utility analysis Cost benefit analysis | ||
| Author (Year) | Sample Description | Intervention Summary | Does the Study Describe Resources Use AND/OR Costs for: | Drummond Score | ||||
|---|---|---|---|---|---|---|---|---|
| Interventions | Healthcare | Criminality | Productivity | Other Public Goods | ||||
| Chandler & Spicer (2006) | Jail recidivists with serious mental illness and substance use disorder | Dual Disorder Treatment program | - | √ | √ | - | - | 3B |
| Henggeler (1999) | Young offenders | Community based MST [2] | - | √ | √ | - | √ | 3A |
| Henggeler (2006) | Young offenders | Family and Drug Court with Community Services including MST and enhanced contingency management | - | √ | √ | - | - | 3A |
| Marlowe (2008) | Male adult offenders with no more than two previous convictions and in need of treatment for drug dependence | Drug court and contingency management programme. | √ | √ | √ | - | - | 3A |
| McCollister (2007) | Juveniles offenders meeting the diagnostic criteria for substance abuse | Drug court combined with a number of different therapies. | - | - | √ | √ | - | 3B |
| Petersilia (1992) | Male adult offenders sentenced to community-based supervision | Intensive probation supervision. | - | - | √ | √ | - | 3A |
| Rossman (1999) | Male adults referred to a community-based program. | Opportunity to Succeed Scheme. | √ | √ | √ | √ | √ | 4 |
| Sacks (2004) | Male adult offenders with a serious mental disorder and substance use | Therapeutic Community [1] | √ | √ | √ | √ | - | 3A |
| Schoenwald (1996) | Young offenders | Community based MST [2] | √ | √ | √ | - | - | 4 |
| Shanahan (2004) | Male and female offenders referred to an adult drug court | Drug court | √ | √ | √ | - | - | 4 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perry, A.E.; Woodhouse, R.; Neilson, M.; Martyn St James, M.; Glanville, J.; Hewitt, C.; Trépel, D. Are Non-Pharmacological Interventions Effective in Reducing Drug Use and Criminality? A Systematic and Meta-Analytical Review with an Economic Appraisal of These Interventions. Int. J. Environ. Res. Public Health 2016, 13, 966. https://doi.org/10.3390/ijerph13100966
Perry AE, Woodhouse R, Neilson M, Martyn St James M, Glanville J, Hewitt C, Trépel D. Are Non-Pharmacological Interventions Effective in Reducing Drug Use and Criminality? A Systematic and Meta-Analytical Review with an Economic Appraisal of These Interventions. International Journal of Environmental Research and Public Health. 2016; 13(10):966. https://doi.org/10.3390/ijerph13100966
Chicago/Turabian StylePerry, Amanda E., Rebecca Woodhouse, Matthew Neilson, Marrissa Martyn St James, Julie Glanville, Catherine Hewitt, and Dominic Trépel. 2016. "Are Non-Pharmacological Interventions Effective in Reducing Drug Use and Criminality? A Systematic and Meta-Analytical Review with an Economic Appraisal of These Interventions" International Journal of Environmental Research and Public Health 13, no. 10: 966. https://doi.org/10.3390/ijerph13100966