
Patterns of Psychiatric Outpatient Practice in Taiwan: A Nationwide Survey


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Study Population
2.3. Statistical Analysis
3. Results
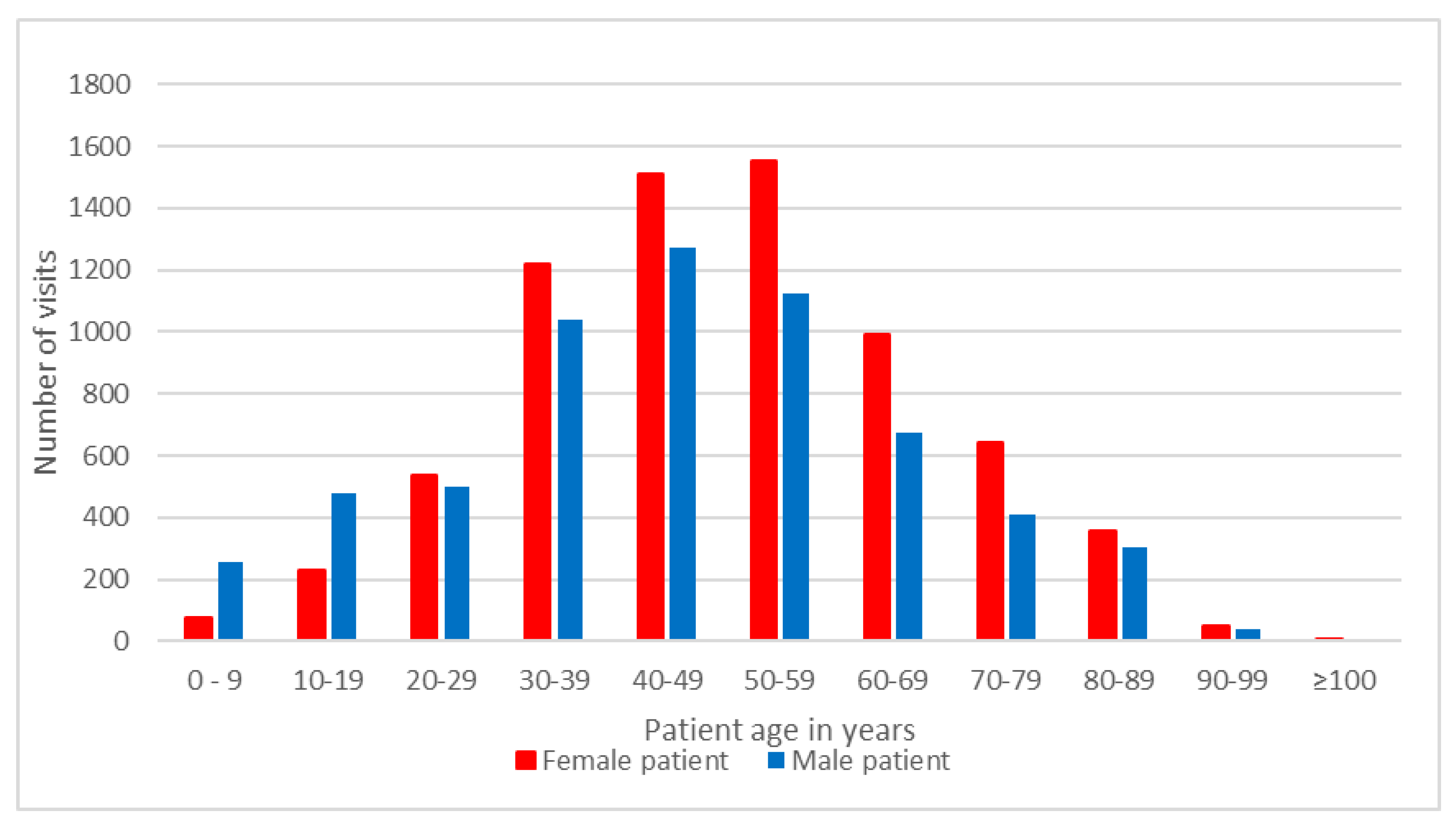
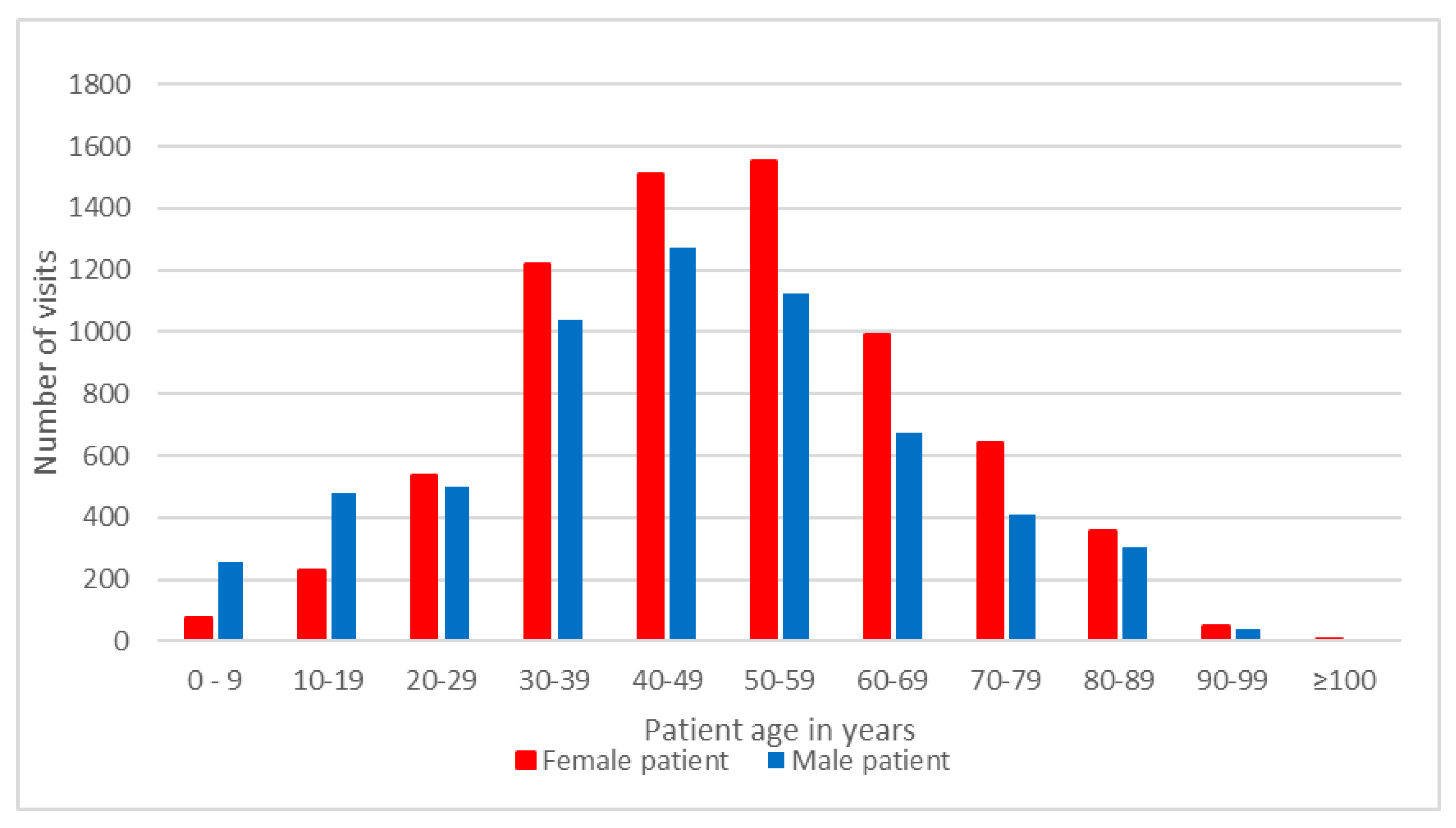
3.1. The Demographics of Psychiatric Outpatients
3.2. Distribution of Outpatient Visits by Patient’s Diagnosis
3.3. Distribution of Outpatient Visits by Pharmacological and Nonpharmacological Treatments
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Hermann, R.C.; Yang, D.; Ettner, S.L.; Marcus, S.C.; Yoon, C.; Abraham, M. Prescription of antipsychotic drugs by office-based physicians in the United States, 1989–1997. Psychiatr. Serv. 2002, 53, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Chien, I.C.; Bih, S.H.; Chou, Y.J.; Lin, C.H.; Lee, W.G.; Chou, P. Trends in the use of psychotropic drugs in Taiwan: A population-based national health insurance study, 1997–2004. Psychiatr. Serv. 2007, 58, 554–557. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.S.; Shau, W.Y.; Chan, H.Y.; Lee, Y.C.; Lai, Y.J.; Lai, M.S. Utilization of antidepressants in Taiwan: A nationwide population-based survey from 2000 to 2009. Pharmacoepidemiol. Drug Saf. 2012, 21, 980–988. [Google Scholar] [CrossRef] [PubMed]
- Hazlett, S.B.; McCarthy, M.L.; Londner, M.S.; Onyike, C.U. Epidemiology of adult psychiatric visits to U.S. emergency departments. Acad. Emerg. Med. 2004, 11, 193–195. [Google Scholar] [CrossRef] [PubMed]
- Larkin, G.L.; Claassen, C.A.; Emond, J.A. Trends in U.S. emergency department visits for mental health conditions, 1992 to 2001. Psychiatr. Serv. 2005, 56, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Kunen, S.; Prejean, C.; Gladney, B. Disposition of emergency department patients with psychiatric comorbidity: Results from the 2004 National Hospital Ambulatory Medical Care Survey. Emerg. Med. J. 2006, 23, 274–275. [Google Scholar] [CrossRef] [PubMed]
- Sankaranarayanan, J.; Puumala, S.E. Epidemiology and characteristics of emergency departments visits by U.S. adults with psychiatric disorder and antipsychotic mention from 2000 to 2004. Curr. Med. Res. Opin. 2007, 23, 1375–1385. [Google Scholar] [CrossRef] [PubMed]
- CDC Morbidity and Mortality Weekly Report—Mental Illness Surveillance among Adults in the United States. Available online: http://www.cdc.gov/mmwr/preview/mmwrhtml/su6003a1.htm (accessed on 6 July 2016).
- Olfson, M.; Blanco, C.; Wang, S.; Laje, G.; Correll, C.U. National trends in the mental health care of children, adolescents, and adults by office-based physicians. JAMA Psychiatry 2014, 71, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Olfson, M.; Kroenke, K.; Wang, S.; Blanco, C. Trends in office-based mental health care provided by psychiatrists and primary care physicians. J. Clin. Psychiatry 2014, 75, 247–253. [Google Scholar] [CrossRef] [PubMed]
- CDC Nonresponse Bias in Estimates from the 2012 National Ambulatory Medical Care Survey. Available online: http://www.cdc.gov/nchs/data/series/sr_02/sr02_171.pdf (accessed on 6 July 2016).
- Katz, S.J.; Kessler, R.C.; Frank, R.G.; Leaf, P.; Lin, E.; Edlund, M. The use of outpatient mental health services in the United States and Ontario: The impact of mental morbidity and perceived need for care. Am. J. Public Health 1997, 87, 1136–1143. [Google Scholar] [CrossRef] [PubMed]
- Matheson, F.I.; Smith, K.L.; Fazli, G.S.; Moineddin, R.; Dunn, J.R.; Glazier, R.H. Physical health and gender as risk factors for usage of services for mental illness. J. Epidemiol. Community Health 2014, 68, 971–978. [Google Scholar] [CrossRef] [PubMed]
- Kovess-Masfety, V.; Boyd, A.; van de Velde, S.; de Graaf, R.; Vilagut, G.; Haro, J.M.; Florescu, S.; O’Neill, S.; Weinberg, L.; Alonso, J.; EU-WMH investigators. Are there gender differences in service use for mental disorders across countries in the European Union? Results from the EU-World Mental Health survey. J. Epidemiol. Community Health 2014, 68, 649–656. [Google Scholar]
- Seedat, S.; Scott, K.M.; Angermeyer, M.C.; Berglund, P.; Bromet, E.J.; Brugha, T.S.; Demyttenaere, K.; de Girolamo, G.; Haro, J.M.; Jin, R.; et al. Cross-national associations between gender and mental disorders in the World Health Organization World Mental Health Surveys. Arch. Gen. Psychiatry 2009, 66, 785–795. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Chiu, W.T.; Demler, O.; Merikangas, K.R.; Walters, E.E. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 617–627. [Google Scholar] [CrossRef] [PubMed]
- Bertisch, S.M.; Herzig, S.J.; Winkelman, J.W.; Buettner, C. National Use of Prescription Medications for Insomnia: NHANES 1999–2010. Sleep 2014, 29, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Wing, Y.K. Sex differences in insomnia: A meta-analysis. Sleep 2006, 29, 85–93. [Google Scholar] [PubMed]
- Ford, D.E.; Kamerow, D.B. Epidemiologic study of sleep disturbances and psychiatric disorders. An opportunity for prevention? JAMA 1989, 262, 1479–1484. [Google Scholar] [CrossRef] [PubMed]
- Katz, D.A.; McHorney, C.A. Clinical correlates of insomnia in patients with chronic illness. Arch. Intern. Med. 1998, 158, 1099–1107. [Google Scholar] [CrossRef] [PubMed]
- McCall, W.V. A psychiatric perspective on insomnia. J. Clin. Psychiatry 2001, 62, 27–32. [Google Scholar]
- Ancoli-Israel, S. The impact and prevalence of chronic insomnia and other sleep disturbances associated with chronic illness. Am. J. Manag. Care 2006, 12, 221–229. [Google Scholar]
- Ohayon, M.M. Epidemiology of insomnia: What we know and what we still need to learn. Sleep Med. Rev. 2002, 6, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.J.; Chen, Y.C.; Chen, C.K.; Chou, W.J.; Chou, M.C. Trends in anxiolytic-hypnotic use and polypharmacy in Taiwan, 2002–2009: A nationwide, population-based survey. Psychiatr. Serv. 2014, 65, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Rickels, K.; Schweizer, E.; Case, W.G.; Greenblatt, D.J. Long-term therapeutic use of benzodiazepines. I. Effects of abrupt discontinuation. Arch. Gen. Psychiatry 1990, 47, 899–907. [Google Scholar] [CrossRef] [PubMed]
- Neutel, C.I. Risk of traffic accident injury after a prescription for a benzodiazepine. Ann. Epidemiol. 1995, 5, 239–244. [Google Scholar] [CrossRef]
- Neutel, C.I.; Perry, S.; Maxwell, C. Medication use and risk of falls. Pharmacoepidemiol. Drug Saf. 2002, 11, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Paterniti, S.; Dufouil, C.; Alperovitch, A. Long-term benzodiazepine use and cognitive decline in the elderly: The Epidemiology of Vascular Aging Study. J. Clin. Psychopharmacol. 2002, 22, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Holm, K.J.; Goa, K.L. Zolpidem: An update of its pharmacology, therapeutic efficacy and tolerability in the treatment of insomnia. Drugs 2000, 59, 865–889. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, F.; Hies, M.; Glaeske, G. Regional variations of private prescriptions for the non-benzodiazepine hypnotics zolpidem and zopiclone in Germany. Pharmacoepidemiol. Drug Saf. 2010, 19, 1071–1077. [Google Scholar] [CrossRef] [PubMed]
- Victorri-Vigneau, C.; Dailly, E.; Veyrac, G.; Jolliet, P. Evidence of zolpidem abuse and dependence: Results of the French Centre for Evaluation and Information on Pharmacodependence (CEIP) network survey. Br. J. Clin. Pharmacol. 2007, 64, 198–209. [Google Scholar] [CrossRef] [PubMed]
- Rudisill, T.M.; Zhu, M.; Kelley, G.A.; Pilkerton, C.; Rudisill, B.R. Medication use and the risk of motor vehicle collisions among licensed drivers: A systematic review. Accid. Anal. Prev. 2016, 96, 255–270. [Google Scholar] [CrossRef] [PubMed]
- Booth, J.N.; Behring, M.; Cantor, R.S.; Colantonio, L.D.; Davidson, S.; Donnelly, J.P.; Johnson, E.; Jordan, K.; Singleton, C.; Xie, F.; et al. Zolpidem use and motor vehicle collisions in older drivers. Sleep Med. 2016, 20, 98–102. [Google Scholar] [CrossRef] [PubMed]
- James, S.P.; Mendelson, W.B. The use of trazodone as a hypnotic: A critical review. J. Clin. Psychiatry 2004, 65, 752–755. [Google Scholar] [CrossRef]
- Bossini, L.; Casolaro, I.; Koukouna, D.; Cecchini, F.; Fagiolini, A. Off-label uses of trazodone: A review. Expert Opin. Pharmacother. 2012, 13, 1707–1717. [Google Scholar] [CrossRef] [PubMed]
- Su, T.P.; Chen, T.J.; Hwang, S.J.; Chou, L.F.; Fan, A.P.; Chen, Y.C. Utilization of psychotropic drugs in Taiwan: An overview of outpatient sector in 2000. Zhonghua Yi Xue Za Zhi (Taipei) 2002, 65, 378–391. [Google Scholar] [PubMed]
- Santamaría, B.; Pérez, M.; Montero, D.; Madurga, M.; de Abajo, F.J. Use of antipsychotic agents in Spain through 1985–2000. Eur. Psychiatry 2002, 17, 471–476. [Google Scholar] [CrossRef]
- Bret, P.; Bret, M.C.; Queuille, E. Prescribing patterns of antipsychotics in 13 French psychiatric hospitals. Encephale 2008, 35, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Rojo, L.E.; Gaspar, P.A.; Silva, H.; Risco, L.; Arena, P.; Cubillos-Robles, K.; Jara, B. Metabolic syndrome and obesity among users of second generation antipsychotics: A global challenge for modern psychopharmacology. Pharmacol. Res. 2015, 101, 74–85. [Google Scholar] [CrossRef] [PubMed]
- Mojtabai, R.; Olfson, M. National trends in long-term use of antidepressant medications: Results from the U.S. National Health and Nutrition Examination Survey. J. Clin. Psychiatry 2014, 75, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Wolfsperger, M.; Greil, W.; Rössler, W.; Grohmann, R. Pharmacological treatment of acute mania in psychiatric in-patients between 1994 and 2004. J. Affect. Disord. 2007, 99, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Bowden, C.L. Key treatment studies of lithium in manic-depressive illness: Efficacy and side effects. J. Clin. Psychiatry 1998, 59, 13–19. [Google Scholar]
- Zajecka, J.M.; Weisler, R.; Sachs, G.; Swann, A.C.; Wozniak, P.; Sommerville, K.W. A comparison of the efficacy, safety, and tolerability of divalproex sodium and olanzapine in the treatment of bipolar disorder. J. Clin. Psychiatry 2002, 63, 1148–1155. [Google Scholar] [CrossRef]
- Osborn, D.P.; Wright, C.A.; Levy, G.; King, M.B.; Deo, R.; Nazareth, I. Relative risk of diabetes, dyslipidaemia, hypertension and the metabolic syndrome in people with severe mental illnesses: Systematic review and metaanalysis. BMC Psychiatry 2008, 8, 84. [Google Scholar] [CrossRef] [PubMed]
- Chien, I.C.; Hsu, J.H.; Lin, C.H.; Bih, S.H.; Chou, Y.J.; Chou, P. Prevalence of diabetes in patients with schizophrenia in Taiwan: A population-based National Health Insurance study. Schizophr. Res. 2009, 111, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.H.; Chang, C.S.; Wei, W.C.; Chang, S.N.; Liao, C.C.; Lane, H.Y.; Sung, F.C. Schizophrenia patients at higher risk of diabetes, hypertension and hyperlipidemia: A population-based study. Schizophr. Res. 2011, 126, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Nehra, V.; Bruce, B.K.; Rath-Harvey, D.M.; Pemberton, J.H.; Camilleri, M. Psychological disorders in patients with evacuation disorders and constipation in a tertiary practice. Am. J. Gastroenterol. 2000, 95, 1755–1758. [Google Scholar] [CrossRef] [PubMed]
- Jessurun, J.G.; van Harten, P.N.; Egberts, T.C.; Pijl, B.J.; Wilting, I.; Tenback, D.E. The effect of psychotropic medications on the occurrence of constipation in hospitalized psychiatric patients. J. Clin. Psychopharmacol. 2013, 33, 587–590. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.S.; Lane, M.; Olfson, M.; Pincus, H.A.; Wells, K.B.; Kessler, R.C. Twelve-month use of mental health services in the United States: Results from the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 629–640. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| ICD9CM | Diagnosis Group | (n = 13,261) | % |
|---|---|---|---|
| 300 | Neurotic disorders | 5714 | 43.1 |
| 296 | Affective psychoses | 3244 | 24.5 |
| 295 | Schizophrenic disorders | 2359 | 17.8 |
| 307 | Special symptoms or syndromes, not elsewhere classified | 2327 | 17.5 |
| 780 | General symptoms | 1299 | 9.8 |
| 311 | Depressive disorder, not elsewhere classified | 813 | 6.1 |
| 564 | Functional digestive disorders, not elsewhere classified | 733 | 5.5 |
| 290 | Senile and presenile organic psychotic conditions | 693 | 5.2 |
| 314 | Hyperkinetic syndrome of childhood | 667 | 5.0 |
| 294 | Other organic psychotic conditions (chronic) | 518 | 3.9 |
| 401 | Essential hypertension | 516 | 3.9 |
| 309 | Adjustment reaction | 431 | 3.3 |
| 333 | Other extrapyramidal disease and abnormal movement disorders | 263 | 2.0 |
| 784 | Symptoms involving head and neck | 238 | 1.8 |
| 250 | Diabetes mellitus | 209 | 1.6 |
| NHI Code | Treatment | (n = 13,261) | % |
|---|---|---|---|
| 45010C | Supportive individual psychotherapy | 2117 | 16.0 |
| 45087C | Re-educative individual psychotherapy-adult | 1578 | 11.9 |
| 45088C | Re-educative individual psychotherapy: 6–15 years old | 127 | 1.0 |
| 45100C | Behavior modification assessment | 49 | 0.4 |
| 45013C | Intensive individual psychotherapy-adult | 34 | 0.3 |
| 45016C | Supportive group psychotherapy | 33 | 0.2 |
| 45094C | Re-educative group psychotherapy | 24 | 0.2 |
| 45022C | Activity therapy (day) | 24 | 0.2 |
| 45043C | Biofeedback therapy | 14 | 0.1 |
| 45089C | Re-educative individual psychotherapy-under 6 years old | 12 | 0.1 |
| 45095C | Special Occupational therapy | 10 | 0.1 |
| 45090C | Intensive individual psychotherapy: 6–15 years old | 7 | 0.1 |
| ATC Code | Drug Classification | n = 13,261 | % |
|---|---|---|---|
| N05C | Hypnotics and sedatives | 6850 | 51.7 |
| N06A | Antidepressants | 6461 | 48.7 |
| N05B | Anxiolytics | 5181 | 39.1 |
| N05A | Antipsychotics | 4869 | 36.7 |
| N03A | Antiepileptics | 3076 | 23.2 |
| C07A | Beta blocking agents | 1443 | 10.9 |
| N04A | Anticholinergic agents | 1410 | 10.6 |
| A06A | Laxatives | 812 | 6.1 |
| N06B | Pscyhostimulants | 671 | 5.1 |
| N06C | Psycholeptics and psychoanaleptics in combination | 578 | 4.4 |
| ATC Code | Drug Classification | n = 13,261 | % |
|---|---|---|---|
| N05CF02 | Zolpidem | 2998 | 22.6 |
| N03AE01 | Clonazepam | 2312 | 17.4 |
| N05BA12 | Alprazolam | 2222 | 16.8 |
| N05BA06 | Lorazepam | 1894 | 14.3 |
| N06AX05 | Trazodone | 1675 | 12.6 |
| N05CD04 | Estazolam | 1583 | 11.9 |
| N05AH04 | Quetiapine | 1352 | 10.2 |
| C07AA05 | Propranolol | 1331 | 10.0 |
| N05CD03 | Flunitrazepam | 1,102 | 8.3 |
| N06AB10 | Escitalopram | 1,089 | 8.2 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dai, Y.-X.; Chen, M.-H.; Chen, T.-J.; Lin, M.-H. Patterns of Psychiatric Outpatient Practice in Taiwan: A Nationwide Survey. Int. J. Environ. Res. Public Health 2016, 13, 955. https://doi.org/10.3390/ijerph13100955
Dai Y-X, Chen M-H, Chen T-J, Lin M-H. Patterns of Psychiatric Outpatient Practice in Taiwan: A Nationwide Survey. International Journal of Environmental Research and Public Health. 2016; 13(10):955. https://doi.org/10.3390/ijerph13100955
Chicago/Turabian StyleDai, Ying-Xiu, Mu-Hong Chen, Tzeng-Ji Chen, and Ming-Hwai Lin. 2016. "Patterns of Psychiatric Outpatient Practice in Taiwan: A Nationwide Survey" International Journal of Environmental Research and Public Health 13, no. 10: 955. https://doi.org/10.3390/ijerph13100955