
Reliability and Construct Validity of Two Versions of Chalder Fatigue Scale among the General Population in Mainland China

 ,
,
Abstract
:1. Introduction
2. Methods
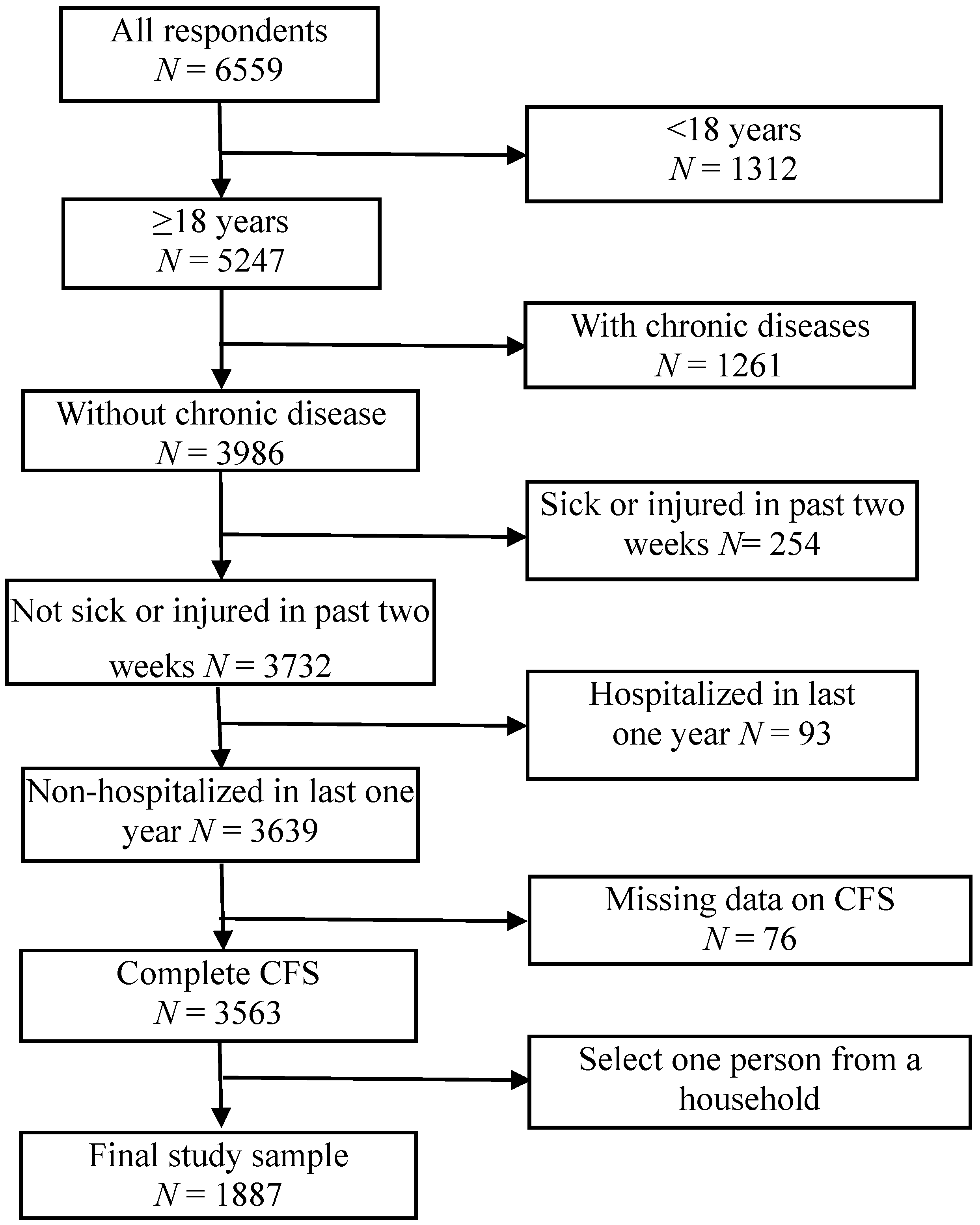
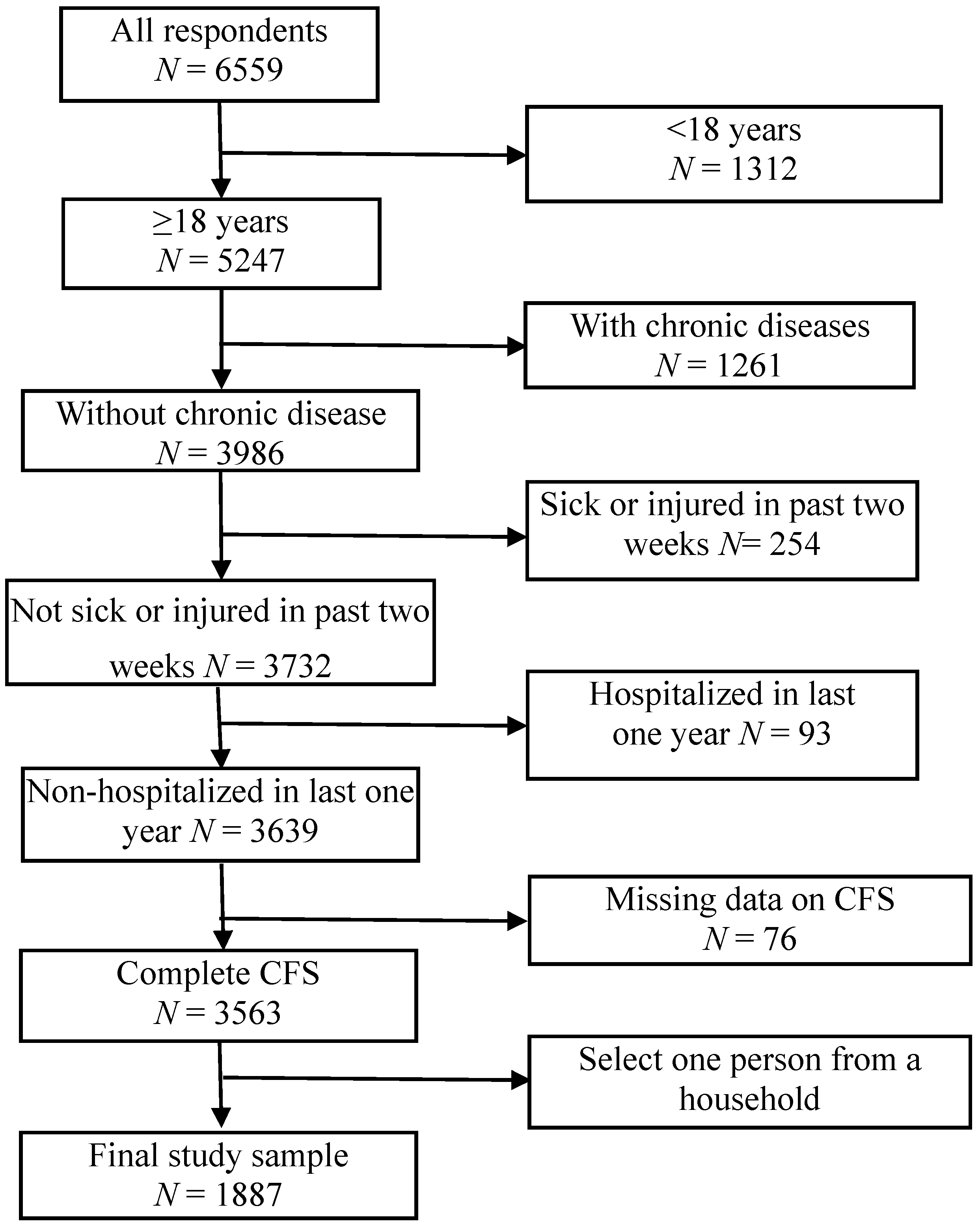
2.1. Sampling and Participants
2.2. Procedures
2.3. Fatigue Measurement

{kind=link}
{kind=link}
| ITEM | Question |
|---|---|
| Item 1 | Do you have problems with tiredness? |
| Item 2 | Do you need to rest more? |
| Item 3 | Do you feel sleepy or drowsy? |
| Item 4 | Do you have problems starting things? |
| Item 5 | Do you start things without difficulty but get weak as you go on? |
| Item 6 | Are you lacking in energy? |
| Item 7 | Do you have less strength in your muscles? |
| Item 8 | Do you feel weak? |
| Item 9 | Do you have difficulty concentrating? |
| Item 10 | Do you think as clearly as usual? |
| Item 11 | Do 6 you make slips of the tongue when speaking? |
| Item 12 | Do you find it more difficult to find the correct word? |
| Item 13 | Is your memory as good as usual? |
| Item 14 | Are you still interested in the things you used to do? |
2.4. Statistical Analysis
2.5. Ethical Approval
3. Results
3.1. Description of the Samples
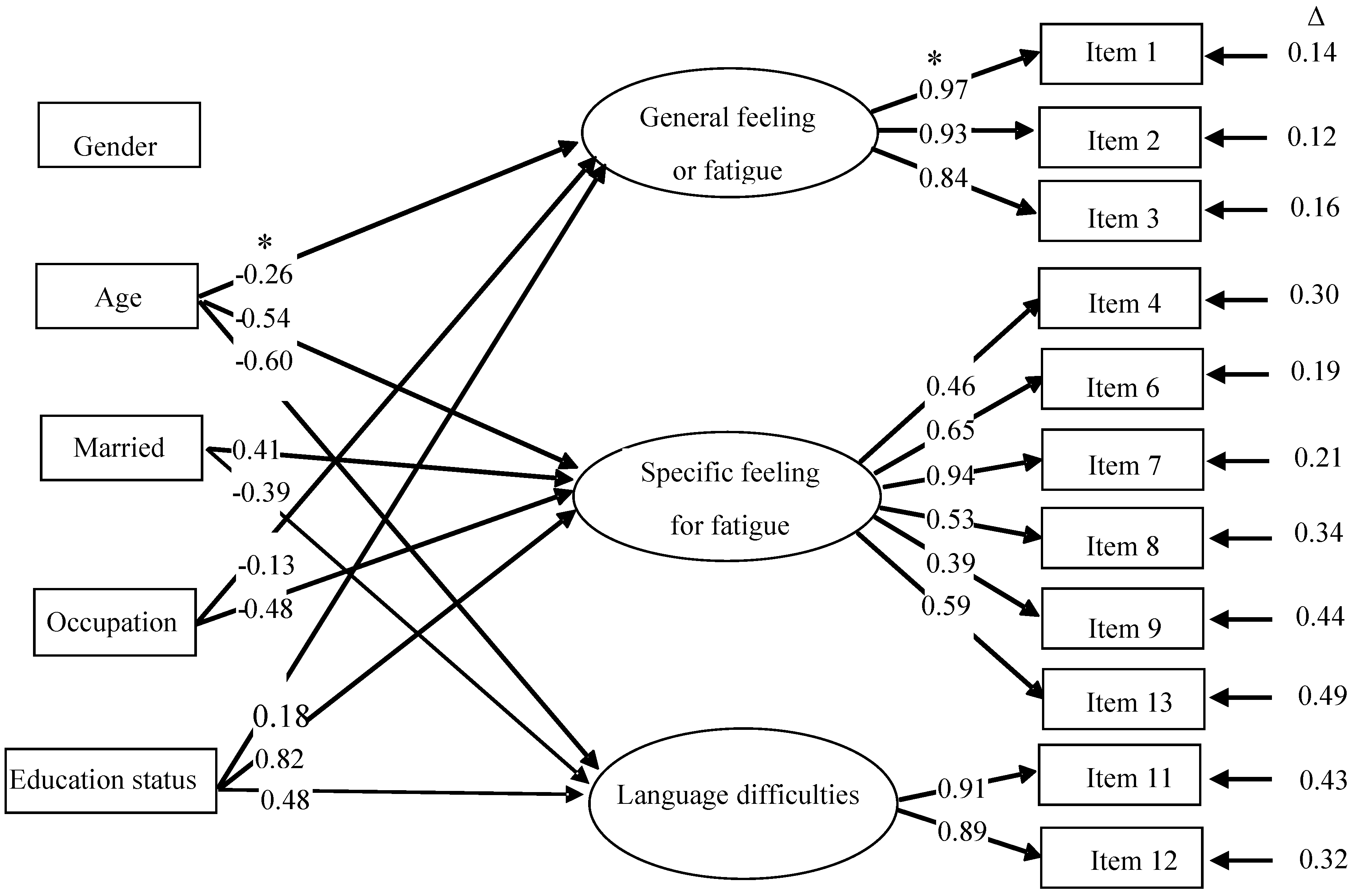
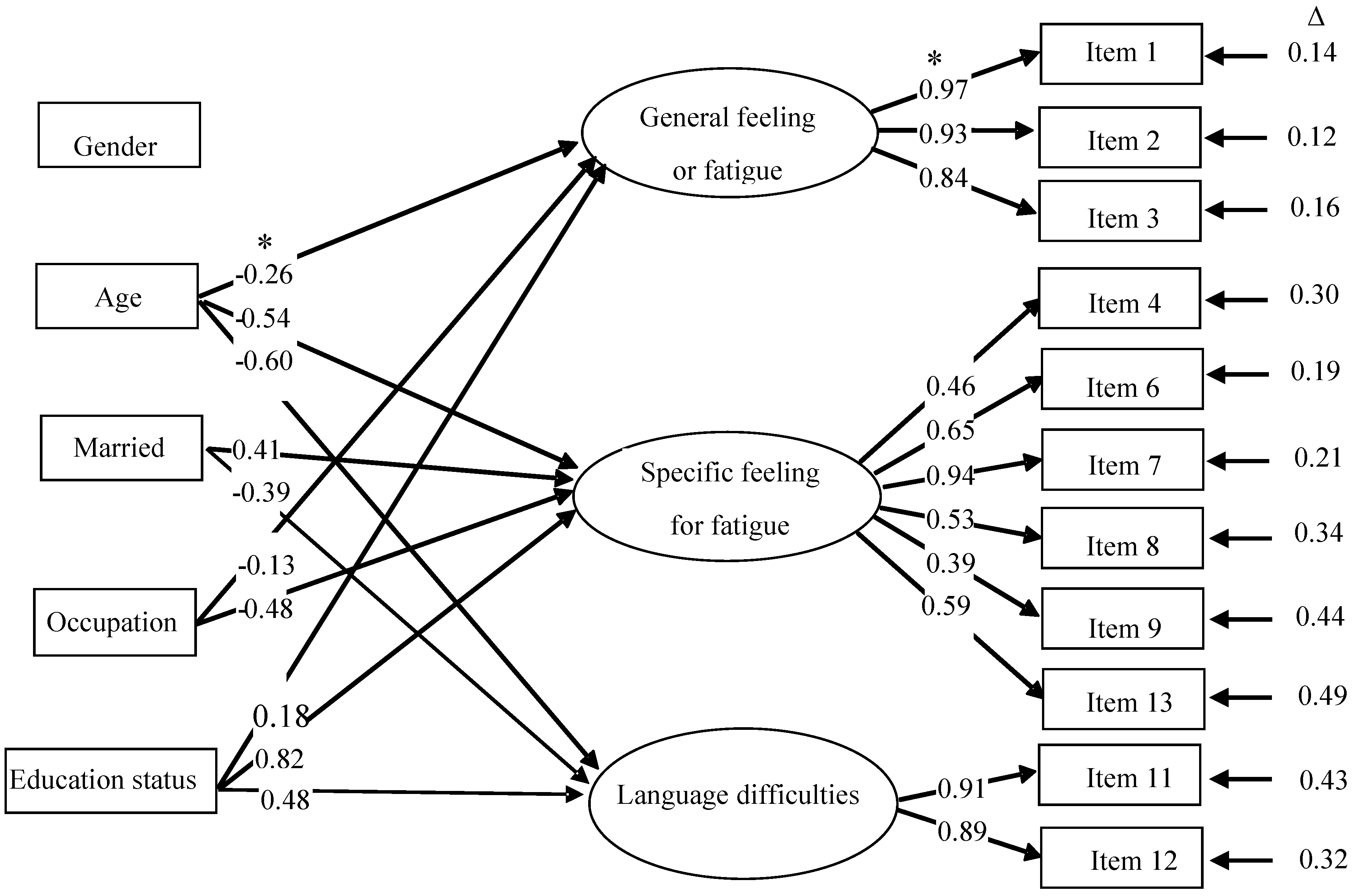
3.2. Construct Validity
| Model | χ2 | df | CFI | TLI | RMSEA (90% CI) | WRMR |
|---|---|---|---|---|---|---|
| 14-version | ||||||
| Original model | 690.392 * | 76 | 0.946 | 0.935 | 0.065 (0.061–0.070) | 2.329 |
| Revised model | 587.572 * | 75 | 0.955 | 0.945 | 0.060 (0.056–0.065) | 2.114 |
| 11-version | ||||||
| Original model | 484.801 * | 43 | 0.950 | 0.936 | 0.074 (0.068–0.080) | 2.378 |
| Revised model | 396.625 * | 42 | 0.960 | 0.948 | 0.067 (0.061–0.073) | 2.116 |
| Model | χ2 | df | CFI | TLI | RMSEA (90% CI) | WRMR |
|---|---|---|---|---|---|---|
| 14-version | ||||||
| Two-factor | 351.972 * | 64 | 0.975 | 0.964 | 0.049 (0.044–0.054) | 1.483 |
| Revised Two-factor | 255.833 * | 63 | 0.983 | 0.975 | 0.040 (0.035–0.045) | 1.249 |
| Three-factor | 208.555 * | 52 | 0.986 | 0.976 | 0.040 (0.034–0.046) | 1.074 |
| 11-version | ||||||
| Two-factor | 129.677 * | 34 | 0.989 | 0.983 | 0.039 (0.032–0.046) | 1.057 |
| Revised Two-factor | 67.444 * | 33 | 0.996 | 0.994 | 0.024 (0.015–0.032) | 0.741 |
| Three-factor | 33.979 | 25 | 0.999 | 0.998 | 0.014 (0.001–0.025) | 0.474 |
| Three-factor + covariates | 142.419 * | 65 | 0.991 | 0.985 | 0.025 (0.020–0.031) | 0.864 |
| Item | Factors | ||
|---|---|---|---|
| General Feeling for Fatigue | Specific Feeling for Fatigue | Language Difficulties | |
| Item 1 | 0.989 * | 0.005 | −0.127 |
| Item 2 | 0.962 * | −0.041 | −0.001 |
| Item 3 | 0.859 * | 0.060 | 0.031 |
| Item 4 | 0.361 * | 0.549 * | 0.002 |
| Item 6 | 0.096 | 0.822 * | 0.016 |
| Item 7 | −0.010 | 0.916 * | −0.061 |
| Item 8 | 0.244 * | 0.446 * | 0.211 * |
| Item 9 | 0.092 | 0.512 * | 0.231 * |
| Item 11 | −0.137 | 0.003 | 0.934 * |
| Item 12 | 0.002 | 0.176 | 0.733 * |
| Item 13 | 0.090 | 0.555 * | −0.166 |
3.3. Internal Consistency
4. Discussion
Strengths and Limitations of Our Study
5. Conclusions
Acknowledgements
Author Contributions
Conflicts of Interest
References
- Łabuz-Roszak, B.; Kubicka-Bączyk, K.; Pierzchała, K.; Machowska-Majchrzak, A.; Skrzypek, M. Fatigue and its association with sleep disorders, depressive symptoms and anxiety in patients with multiple sclerosis. Neurol. Neurochir. Pol. 2012, 46, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Bower, J.E.; Lamkin, D.M. Inflammation and cancer-related fatigue: Mechanisms, contributing factors, and treatment implications. Brain Behav. Immun. 2013, 30, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.H.; Ai, Q.L. Correlation between fatigue and cognitive impairment and depression in patient with lacunar stroke: A retrospective case series study (Chinese). Int. J. Cerebrovasc. Dis. 2012, 20, 496–500. [Google Scholar]
- Stocchi, F.; Abbruzzese, G.; Ceravolo, R.; Cortelli, P.; D’Amelio, M.; de Pandis, M.F.; Fabbrini, G.; Pacchetti, C.; Pezzoli, G.; Tessitore, A.; et al. Prevalence of fatigue in Parkinson disease and its clinical correlates. Neurology 2014, 83, 215–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waters, F.; Naik, N.; Rock, D. Sleep, fatigue, and functional health in psychotic patients. Schizophr. Res. Treatment 2013. [Google Scholar] [CrossRef] [PubMed]
- Wong, W.S.; Fielding, R. The co-morbidity of chronic pain, insomnia, and fatigue in the general adult population of Hong Kong: Prevalence and associated factors. J. Psychosom. Res. 2012, 73, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Yun, Y.H.; Lee, M.K.; Chun, H.N.; Lee, Y.M.; Park, S.M.; Mendoza, T.R.; Wang, X.S.; Cleeland, C.S. Fatigue in the general Korean population: Application and normative data of the Brief Fatigue Inventory. J. Pain. Symptom. Manag. 2008, 36, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Chalder, T.; Berelowitz, G.; Pawlikowska, T.; Watts, L.; Wessely, S.; Wright, D.; Wallace, E.P. Development of a fatigue scale. J. Psychosom. Res. 1993, 37, 147–153. [Google Scholar] [CrossRef]
- Morriss, R.K.; Wearden, A.J.; Mullis, R. Exploring the validity of the Chalder Fatigue scale in chronic fatigue syndrome. J. Psychosom. Res. 1998, 45, 411–417. [Google Scholar] [CrossRef]
- Wong, W.S.; Fielding, R. Construct validity of the Chinese version of the Chalder Fatigue Scale in a Chinese community sample. J. Psychosom. Res. 2010, 68, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Fukuda, S.; Mizuno, K.; Imai-Matsumura, K.; Jodoi, T.; Kawatani, J.; Takano, M.; Miike, T.; Tomoda, A.; Watanabe, Y. Reliability and validity of the Japanese version of the Chalder Fatigue Scale among youth in Japan. Psychol. Rep. 2008, 103, 682–690. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.J.; Costa, E.; Menezes, P.R.; Chalder, T.; Bhugra, D.; Wessely, S. Cross-cultural validation of the Chalder fatigue questionnaire in Brazilian primary care. J. Psychosom. Res. 2007, 62, 301–304. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, C.; Riechelmann, R.; Martins, L.C.; Hassan, B.J.; Casa, F.B.; del Giglio, A. Guarana (Paullinia cupana) improves fatigue in breast cancer patients undergoing systemic chemotherapy. J. Altern. Complement. Med. 2011, 17, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Sabes-Figuera, R.; McCrone, P.; Hurley, M.; King, M.; Donaldson, A.N.; Ridsdale, L. Cost-effectiveness of counselling, graded-exercise and usual care for chronic fatigue: Evidence from a randomised trial in primary care. BMC Health Serv. Res. 2012, 12, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Crawley, E.; Collin, S.M.; White, P.D.; Rimes, K.; Sterne, J.A.; May, M.T. Treatment outcome in adults with chronic fatigue syndrome: A prospective study in England based on the CFS/ME National Outcomes Database. QJM 2013, 106, 555–565. [Google Scholar] [CrossRef] [PubMed]
- Knoop, H.; van Kessel, K.; Moss-Morris, R. Which cognitions and behaviours mediate the positive effect of cognitive behavioural therapy on fatigue in patients with multiple sclerosis? Psychol. Med. 2012, 42, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Kocalevent, R.D.; Klapp, B.F.; Albani, C.; Brähler, E. Gender differences in a resources-demands model in the general population. BMC Public Health 2014, 14, 902–909. [Google Scholar] [CrossRef] [PubMed]
- Sun, K.; Wang, H. Relationship between emotional labor and fatigue among nurses working in psychiatric hospital. J. Nur. Sci. 2012, 27, 71–72. [Google Scholar]
- Huang, X.B.; Li, Z.X.; Chen, W.Q.; Wang, M.Y.; Zhang, C.Y. The research of relationship between fatigue degree and quality of life in chronic fatigue syndrome patients. Chin. J. Behav. Med. Sci. 2006, 15, 687–688. [Google Scholar]
- Li, S.L.; Yan, W.J.; Sun, G.X.; Lu, Z.J. Analysis of influencing factors on the fatigue situation of female doctors. Chin. J. Soc. Med. 2009, 26, 366–368. [Google Scholar]
- Zuo, L.J.; Yu, S.Y.; Cao, C.J.; Liu, Z.; Huang, X.Y.; Sun, L.; Hu, Y.; Wang, F.; Chen, Z.J.; Zhang, W. Investigation on fatigue and associated factors in patients with Parkinson disease. Chin. J. Clin. 2012, 6, 7238–7244. [Google Scholar]
- Wang, L.Y.; Guo, X.Y.; Hu, X.M.; Bai, L.X. Study on social factors of chronic fatigue in populations. Chin. Prev. Med. 2008, 9, 726–728. [Google Scholar]
- Fong, T.C.; Chan, J.S.; Chan, C.L.; Ho, R.T.; Ziea, E.T.; Wong, V.C.; Ng, B.F.; Ng, S.M. Psychometric properties of the Chalder Fatigue Scale revisited: An exploratory structural equation modeling approach. Qual. Life Res. 2015, 24, 2273–2278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, W.F.; Huang, L.Y.; Zhou, Z.H.; Li, M.; Gao, Y.Q. Estimation on reliability and validity of Fatigue Scale-14 in patients with chronic hepatitis B. Acta Univ. Tradit. Med. Sin. Pharmacol. Shanghai 2012, 26, 33–36. (In Chinese) [Google Scholar]
- Beauducel, A.; Herzberg, P.Y. On the performance of maximum likelihood vs. means and variance adjusted weighted least squares estimation in CFA. Struct. Eq. Model. 2006, 13, 186–203. [Google Scholar] [CrossRef]
- Wen, Z.L.; Ye, B.J. Estimation of reliability: From the alpha coefficient to internal consistency reliability. Acta Psychologica Sinica 2011, 43, 821–829. (In Chinese) [Google Scholar]
- Nunnally, J.C.; Bernstein, I.H. Psychometric Theory; McGraw-Hill, Inc.: New York, NY, USA, 1994. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria vs. new alternatives. Struct. Eq. Model. 2009, 6, 1–55. [Google Scholar] [CrossRef]
- Yu, C.-Y.; Muthén, B. Evaluation of the Model Fit Indices for Latent Variable Models with Categorical and Continuous Outcomes. In Proceedings of the Annual Meeting of the American Educational Research Association, New Orleans, LA, USA, 1–5 April 2002.
- Meade, A.W.; Johnson, E.C.; Braddy, P.W. Power and sensitivity of alternative fit indices in tests of measurement invariance. J. Appl. Psychol. 2008, 93, 568–592. [Google Scholar] [CrossRef] [PubMed]
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jing, M.-J.; Lin, W.-Q.; Wang, Q.; Wang, J.-J.; Tang, J.; Jiang, E.-S.; Lei, Y.-X.; Wang, P.-X. Reliability and Construct Validity of Two Versions of Chalder Fatigue Scale among the General Population in Mainland China. Int. J. Environ. Res. Public Health 2016, 13, 147. https://doi.org/10.3390/ijerph13010147
Jing M-J, Lin W-Q, Wang Q, Wang J-J, Tang J, Jiang E-S, Lei Y-X, Wang P-X. Reliability and Construct Validity of Two Versions of Chalder Fatigue Scale among the General Population in Mainland China. International Journal of Environmental Research and Public Health. 2016; 13(1):147. https://doi.org/10.3390/ijerph13010147
Chicago/Turabian StyleJing, Meng-Juan, Wei-Quan Lin, Qiang Wang, Jia-Ji Wang, Jie Tang, En-She Jiang, Yi-Xiong Lei, and Pei-Xi Wang. 2016. "Reliability and Construct Validity of Two Versions of Chalder Fatigue Scale among the General Population in Mainland China" International Journal of Environmental Research and Public Health 13, no. 1: 147. https://doi.org/10.3390/ijerph13010147