
Melanoma in the Italian Population and Regional Environmental Influences: A National Retrospective Survey on 2001–2008 Hospitalization Records

 ,
,
Abstract
:1. Introduction
2. Experimental Section
Methods
3. Results and Discussion

{kind=link}
{kind=link}
{kind=link}
| Age Group | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 |
|---|---|---|---|---|---|---|---|---|
| 20 to 30 years old | 334 | 278 | 242 | 329 | 271 | 297 | 301 | 286 |
| 31 to 40 years old | 600 | 614 | 549 | 623 | 659 | 673 | 728 | 729 |
| 41 to 50 years old | 714 | 644 | 598 | 681 | 748 | 843 | 844 | 898 |
| 51 to 60 years old | 872 | 817 | 783 | 857 | 858 | 930 | 942 | 964 |
| 61 to 70 years old | 979 | 963 | 968 | 940 | 1.007 | 1.074 | 1.197 | 1.209 |
| 71 to 80 years old | 954 | 847 | 865 | 844 | 895 | 1.030 | 1.024 | 1.141 |
| ≥81 years old | 393 | 418 | 416 | 433 | 473 | 477 | 581 | 596 |
| TOTAL | 4.846 | 4.581 | 4.421 | 4.707 | 4.911 | 5.324 | 5.617 | 5.823 |
| Age Group | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 |
|---|---|---|---|---|---|---|---|---|
| 20 to 30 years old | 3.92 | 3.35 | 2.96 | 4.08 | 3.46 | 3.89 | 4.00 | 3.83 |
| 31 to 40 years old | 6.56 | 6.63 | 5.83 | 6.53 | 6.93 | 7.10 | 7.71 | 7.78 |
| 41 to 50 years old | 9.39 | 8.18 | 7.38 | 8.15 | 8.69 | 9.54 | 9.29 | 9.66 |
| 51 to 60 years old | 12.26 | 11.42 | 10.81 | 11.68 | 11.51 | 12.20 | 12.36 | 12.61 |
| 61 to 70 years old | 15.16 | 14.87 | 14.91 | 14.48 | 15.59 | 16.72 | 18.22 | 18.09 |
| 71 to 80 years old | 19.56 | 17.09 | 17.31 | 16.75 | 17.62 | 20.01 | 19.76 | 21.80 |
| ≥81 years old | 18.33 | 18.55 | 17.58 | 17.34 | 15.72 | 17.49 | 20.47 | 20.23 |
| TOTAL | 10.56 | 9.90 | 9.44 | 9.95 | 10.24 | 11.12 | 11.64 | 11.97 |
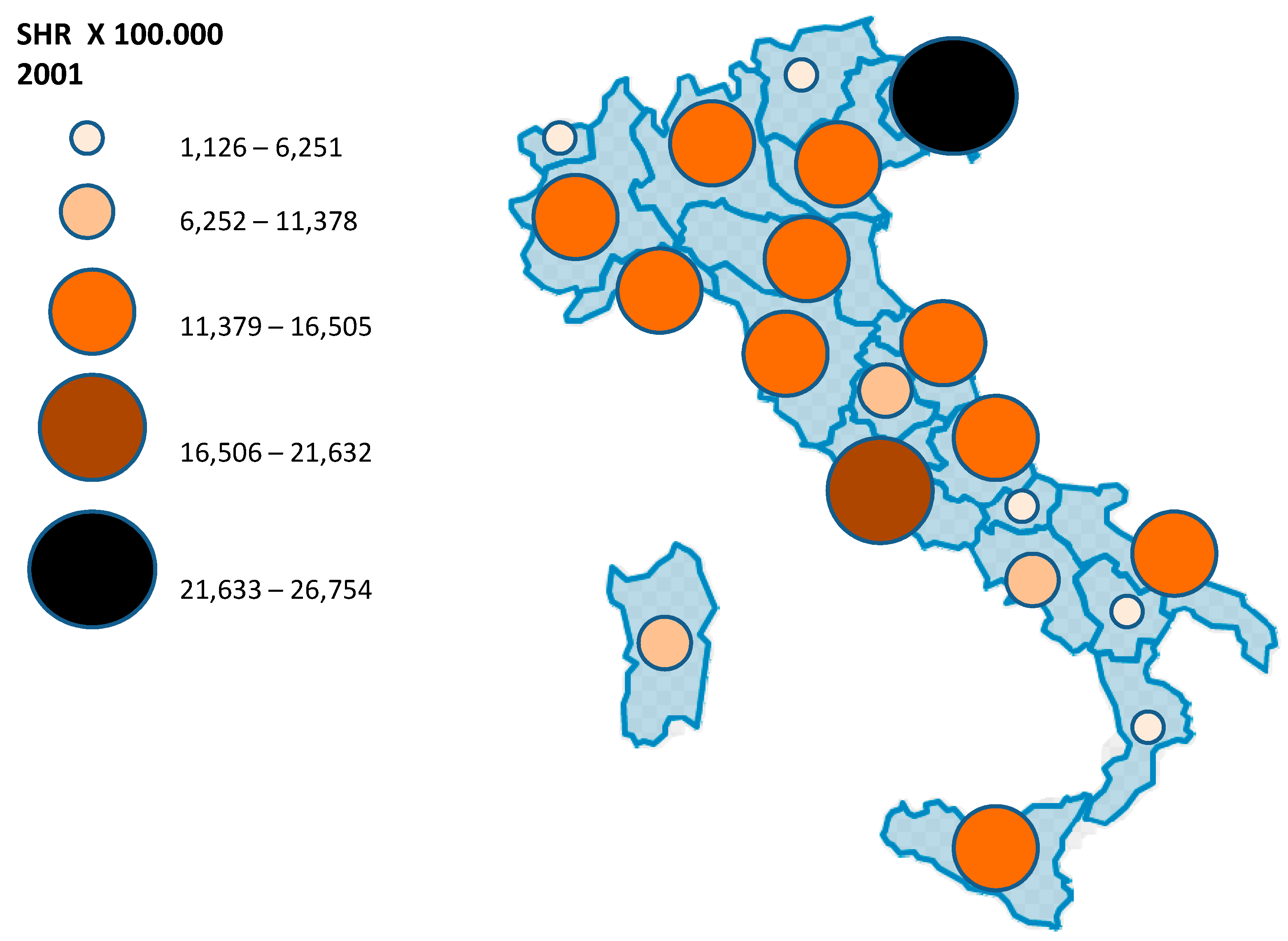
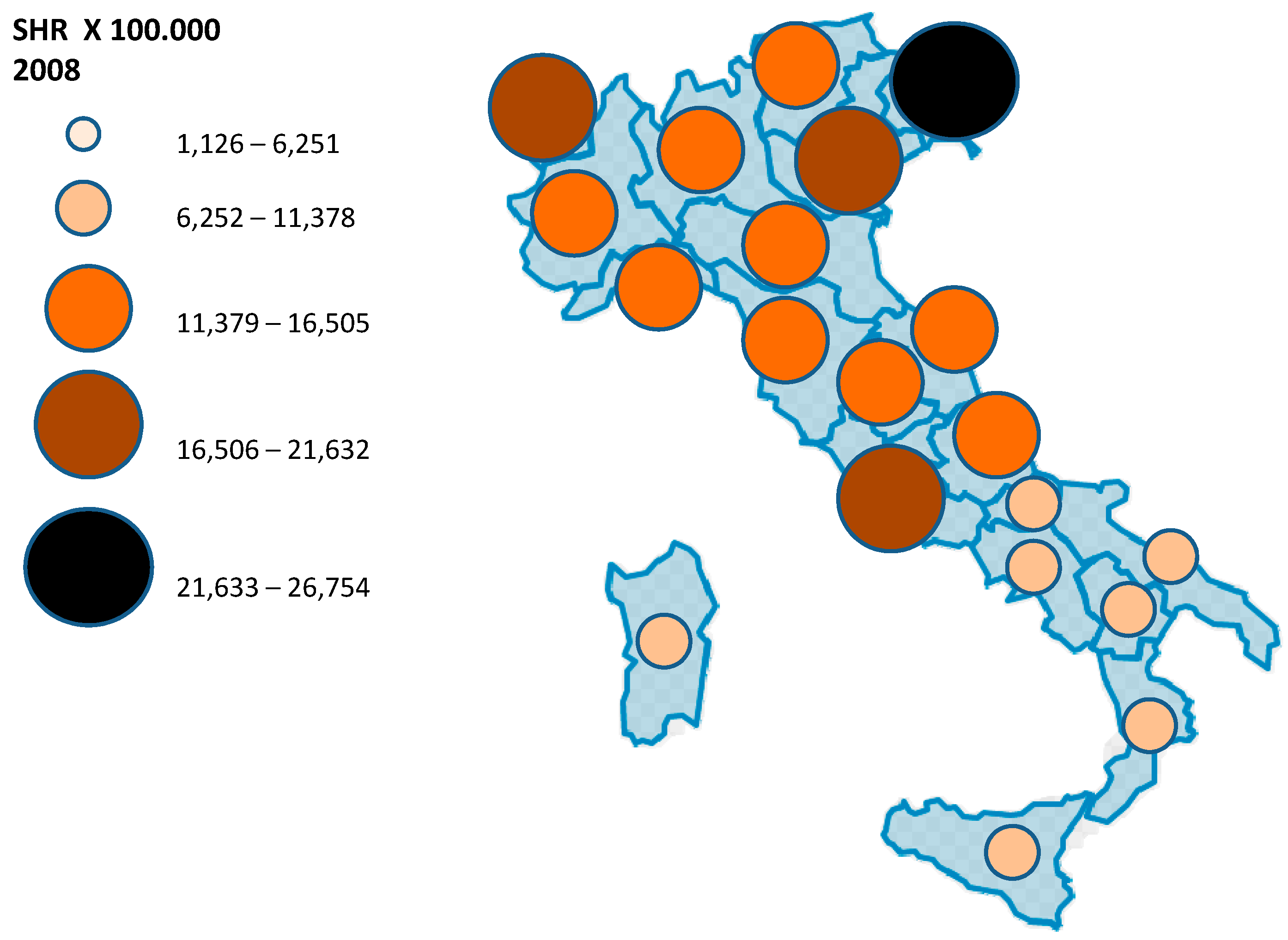
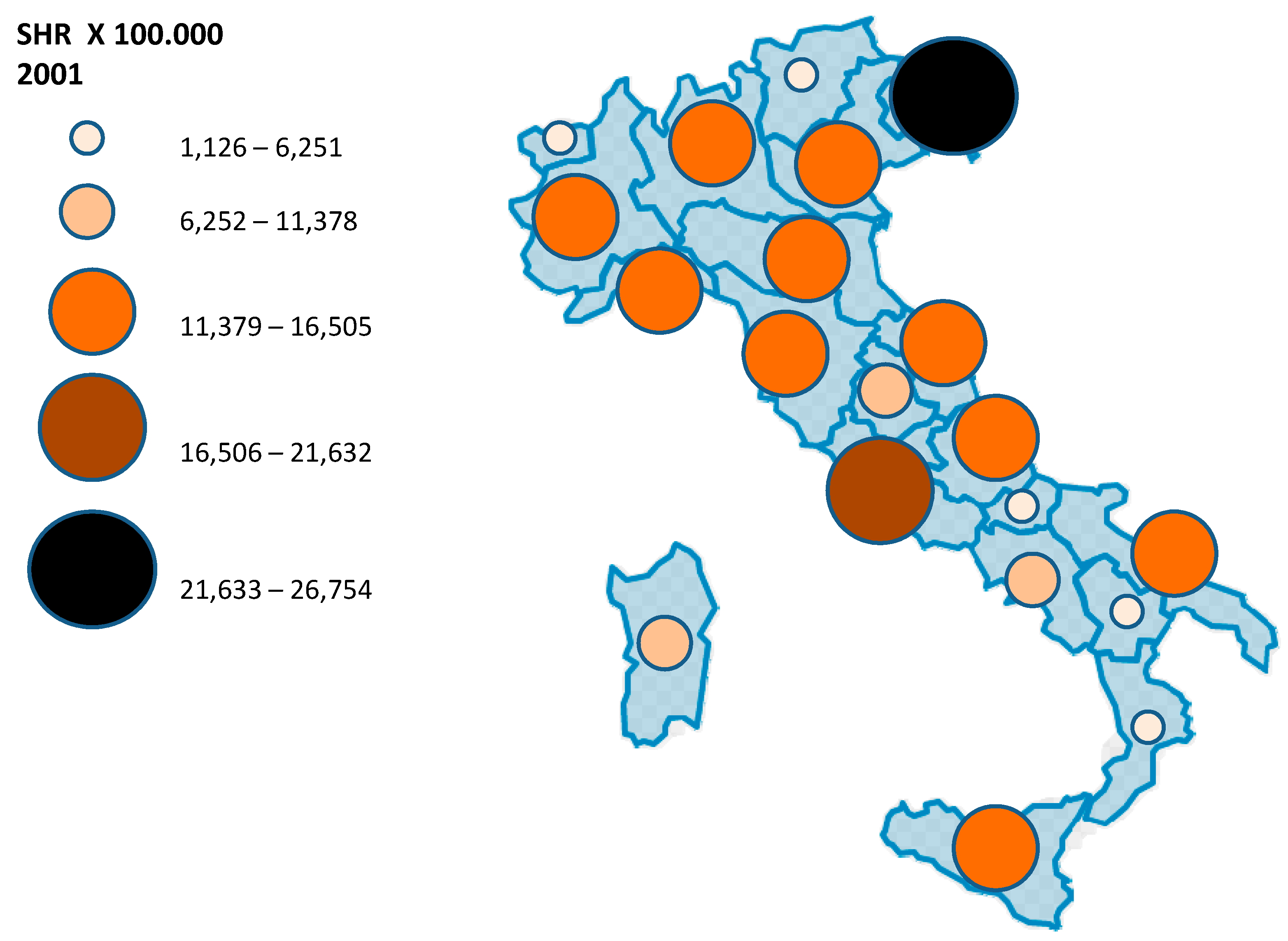
| Region | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | SHR | N | SHR | N | SHR | N | SHR | N | SHR | N | SHR | N | SHR | N | SHR | |
| Piemonte | 385 | 12,164 | 419 | 13,172 | 385 | 11,982 | 415 | 12,767 | 471 | 14,441 | 432 | 13,271 | 457 | 13,914 | 489 | 14,819 |
| Val d'Aosta | − | NA * | − | NA * | 12 | 13,235 | 8 | 8,772 | 7 | 7,588 | 11 | 11,909 | 8 | 8,598 | 17 | 18,220 |
| Lombardia | 814 | 12,202 | 832 | 12,359 | 853 | 12,482 | 808 | 11,668 | 876 | 12,542 | 953 | 13,612 | 983 | 13,912 | 876 | 12,303 |
| Trentino | 40 | 6,041 | 55 | 8,199 | 45 | 6,621 | 71 | 10,313 | 78 | 11,179 | 59 | 8,406 | 87 | 12,217 | 92 | 12,790 |
| Veneto | 432 | 12,971 | 464 | 13,782 | 418 | 12,246 | 434 | 12,593 | 408 | 11,719 | 536 | 15,374 | 582 | 16,487 | 643 | 18,056 |
| Friuli | 190 | 21,140 | 162 | 17,904 | 126 | 13,860 | 184 | 20,184 | 164 | 17,887 | 196 | 21,464 | 236 | 25,667 | 247 | 26,754 |
| Liguria | 185 | 15,290 | 190 | 15,685 | 146 | 12,022 | 158 | 12,919 | 145 | 11,720 | 155 | 12,623 | 177 | 14,418 | 187 | 15,230 |
| Emilia | 376 | 12,425 | 330 | 10,786 | 315 | 10,195 | 397 | 12,686 | 387 | 12,261 | 406 | 12,837 | 394 | 12,335 | 455 | 14,092 |
| Toscana | 388 | 14,686 | 334 | 12,544 | 260 | 9,642 | 270 | 9,948 | 281 | 10,305 | 359 | 13,150 | 392 | 14,231 | 371 | 13,395 |
| Umbria | 53 | 8,612 | 54 | 8,650 | 42 | 6,630 | 43 | 6,703 | 62 | 9,560 | 69 | 10,599 | 55 | 8,346 | 76 | 11,445 |
| Marche | 128 | 11,781 | 139 | 12,624 | 134 | 12,023 | 135 | 12,007 | 126 | 11,142 | 171 | 15,085 | 166 | 14,486 | 167 | 14,452 |
| Lazio | 648 | 17,422 | 639 | 17,040 | 705 | 18,584 | 700 | 18,228 | 799 | 20,637 | 799 | 19,956 | 800 | 19,752 | 822 | 20,073 |
| Abruzzo | 102 | 11,182 | 89 | 9,620 | 82 | 8,757 | 104 | 10,982 | 107 | 11,207 | 109 | 11,375 | 87 | 8,969 | 114 | 11,644 |
| Molise | 11 | 4,790 | 20 | 8,637 | 15 | 6,430 | 17 | 7,281 | 20 | 8,554 | 20 | 8,567 | 22 | 9,370 | 17 | 7,209 |
| Campania | 281 | 7,555 | 244 | 6,507 | 267 | 7,038 | 301 | 7,838 | 308 | 7,955 | 325 | 8,117 | 402 | 9,925 | 418 | 10,207 |
| Puglia | 322 | 11,644 | 248 | 8,899 | 227 | 8,071 | 252 | 8,879 | 265 | 9,302 | 264 | 9,254 | 322 | 11,235 | 325 | 11,286 |
| Basilicata | 24 | 5,743 | 19 | 4,529 | 15 | 3,557 | 30 | 7,089 | 26 | 6,135 | 27 | 6,393 | 22 | 5,193 | 37 | 8,710 |
| Calabria | 80 | 5,813 | 58 | 4,187 | 56 | 4,010 | 62 | 4,428 | 66 | 4,695 | 82 | 5,838 | 66 | 4,656 | 93 | 6,517 |
| Sicily | 386 | 11,367 | 281 | 8,225 | 227 | 6,570 | 264 | 7,624 | 249 | 7,150 | 274 | 7,853 | 314 | 8,940 | 290 | 8,229 |
| Sardinia | − | NA * | − | NA * | 91 | 7,636 | 54 | 4,496 | 66 | 5,434 | 77 | 6,310 | 45 | 3,659 | 87 | 7,034 |
| Age Group | Region | 2001 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 |
|---|---|---|---|---|---|---|---|---|---|
| 20–30 | Piemonte | 4,25 | 3,78 | 3,41 | 4,21 | 3,61 | 5,00 | 5,25 | 3,27 |
| 31–40 | Piemonte | 6,30 | 9,83 | 7,41 | 8,11 | 9,27 | 7,27 | 7,45 | 7,72 |
| 41–50 | Piemonte | 9,89 | 11,59 | 10,92 | 10,78 | 10,45 | 9,21 | 10,92 | 10,03 |
| 51–60 | Piemonte | 12,45 | 14,33 | 15,31 | 12,82 | 14,10 | 13,28 | 12,96 | 14,52 |
| 61–70 | Piemonte | 20,15 | 16,48 | 15,50 | 17,51 | 22,69 | 21,37 | 23,02 | 24,18 |
| 71–80 | Piemonte | 20,09 | 23,94 | 19,51 | 25,84 | 29,52 | 25,60 | 28,17 | 28,83 |
| >80 | Piemonte | 11,01 | 42,32 | 34,64 | 40,43 | 49,46 | 41,85 | 41,23 | 47,76 |
| 20–30 | Val d’Aosta | NA * | NA * | 7,77 | 0,00 | 0,00 | 0,00 | 0,00 | 17,44 |
| 31–40 | Val d’Aosta | NA * | 0,00 | 0,00 | 5,25 | 5,28 | 5,36 | 10,83 | 5,55 |
| 41–50 | Val d’Aosta | NA * | NA * | 6,22 | 6,04 | 17,35 | 5,62 | 10,87 | 10,60 |
| 51–60 | Val d’Aosta | NA * | 0,00 | 34,70 | 0,00 | 0,00 | 13,24 | 13,21 | 33,08 |
| 61–70 | Val d’Aosta | NA * | 0,00 | 15,35 | 15,28 | 7,62 | 38,35 | 7,58 | 37,61 |
| 71–80 | Val d’Aosta | NA * | NA * | 30,34 | 39,94 | 0,00 | 39,42 | 19,71 | 39,11 |
| >80 | Val d’Aosta | NA * | NA * | 19,42 | 73,80 | 17,84 | 17,31 | 16,55 | 31,78 |
| 20–30 | Lombardia | 3,78 | 3,75 | 3,34 | 5,11 | 3,62 | 4,38 | 5,44 | 3,41 |
| 31–40 | Lombardia | 7,08 | 8,31 | 7,72 | 7,75 | 6,87 | 7,94 | 8,54 | 7,31 |
| 41–50 | Lombardia | 11,21 | 9,73 | 9,29 | 8,87 | 10,54 | 10,72 | 10,21 | 10,19 |
| 51–60 | Lombardia | 12,50 | 13,63 | 11,62 | 13,03 | 14,83 | 16,06 | 15,65 | 13,16 |
| 61–70 | Lombardia | 16,91 | 18,12 | 18,77 | 17,37 | 18,90 | 21,39 | 21,39 | 19,38 |
| 71–80 | Lombardia | 25,12 | 26,53 | 28,36 | 22,90 | 28,11 | 26,46 | 27,45 | 26,78 |
| >80 | Lombardia | 23,89 | 47,63 | 58,20 | 39,77 | 43,95 | 44,64 | 41,81 | 39,00 |
| 20–30 | Trentino | 0,00 | 1,85 | 0,94 | 8,59 | 6,79 | 3,91 | 3,91 | 3,91 |
| 31–40 | Trentino | 2,75 | 6,06 | 4,03 | 5,38 | 4,75 | 4,81 | 6,25 | 4,24 |
| 41–50 | Trentino | 3,44 | 7,47 | 4,80 | 3,84 | 12,53 | 4,97 | 6,87 | 12,02 |
| 51–60 | Trentino | 4,86 | 8,75 | 9,65 | 10,47 | 11,11 | 12,98 | 18,30 | 17,10 |
| 61–70 | Trentino | 15,22 | 10,26 | 11,11 | 19,57 | 19,31 | 18,27 | 15,59 | 18,42 |
| 71–80 | Trentino | 17,50 | 21,85 | 13,12 | 21,89 | 27,61 | 17,37 | 23,06 | 25,65 |
| >80 | Trentino | 6,16 | 34,75 | 21,68 | 27,99 | 31,40 | 11,53 | 39,87 | 38,42 |
| 20–30 | Veneto | 6,20 | 3,78 | 6,38 | 5,74 | 5,11 | 6,32 | 6,59 | 5,80 |
| 31–40 | Veneto | 8,07 | 9,88 | 8,48 | 8,33 | 8,76 | 11,20 | 11,25 | 13,91 |
| 41–50 | Veneto | 11,74 | 10,69 | 8,65 | 9,77 | 9,56 | 13,66 | 14,76 | 15,44 |
| 51–60 | Veneto | 16,28 | 19,54 | 15,65 | 15,14 | 13,85 | 16,34 | 17,70 | 19,91 |
| 61–70 | Veneto | 17,00 | 23,60 | 18,82 | 16,96 | 15,83 | 25,00 | 24,68 | 27,05 |
| 71–80 | Veneto | 24,62 | 20,42 | 26,57 | 20,55 | 17,60 | 29,00 | 31,62 | 30,36 |
| >80 | Veneto | 14,22 | 32,92 | 37,61 | 34,09 | 29,27 | 39,32 | 40,83 | 42,22 |
| 20–30 | Friuli V. G. | 8,25 | 8,67 | 3,28 | 17,16 | 4,43 | 8,25 | 11,22 | 10,47 |
| 31–40 | Friuli V. G. | 13,85 | 11,35 | 10,10 | 12,95 | 11,93 | 12,09 | 16,30 | 20,73 |
| 41–50 | Friuli V. G. | 18,64 | 14,14 | 11,15 | 22,25 | 18,45 | 19,73 | 16,82 | 19,75 |
| 51–60 | Friuli V. G. | 27,28 | 24,66 | 13,35 | 20,04 | 19,06 | 24,22 | 27,84 | 29,42 |
| 61–70 | Friuli V. G. | 29,99 | 24,15 | 20,87 | 24,91 | 26,83 | 29,24 | 40,32 | 36,50 |
| 71–80 | Friuli V. G. | 34,11 | 28,60 | 23,17 | 24,30 | 37,09 | 36,02 | 60,00 | 46,50 |
| >80 | Friuli V. G. | 18,95 | 51,86 | 35,82 | 34,30 | 41,91 | 53,13 | 62,28 | 57,04 |
| 20–30 | Liguria | 3,93 | 4,86 | 4,36 | 5,26 | 4,55 | 4,72 | 5,64 | 3,24 |
| 31–40 | Liguria | 9,29 | 8,79 | 6,47 | 5,97 | 5,50 | 8,45 | 8,16 | 5,91 |
| 41–50 | Liguria | 12,32 | 13,07 | 9,13 | 6,86 | 7,93 | 8,62 | 7,08 | 9,12 |
| 51–60 | Liguria | 16,97 | 16,60 | 10,89 | 16,53 | 12,62 | 12,89 | 10,46 | 15,25 |
| 61–70 | Liguria | 17,87 | 22,31 | 19,40 | 15,02 | 19,67 | 18,53 | 26,52 | 18,92 |
| 71–80 | Liguria | 29,10 | 28,82 | 24,02 | 23,33 | 21,05 | 20,50 | 24,65 | 26,34 |
| >80 | Liguria | 19,85 | 40,87 | 35,44 | 36,82 | 26,50 | 33,15 | 27,80 | 48,11 |
| 20–30 | Emilia R. | 5,36 | 3,97 | 3,61 | 6,08 | 4,74 | 4,89 | 5,47 | 4,17 |
| 31–40 | Emilia R. | 7,98 | 6,14 | 5,19 | 8,13 | 7,28 | 9,50 | 6,63 | 6,79 |
| 41–50 | Emilia R. | 9,75 | 9,42 | 7,94 | 10,20 | 10,74 | 10,09 | 11,59 | 9,63 |
| 51–60 | Emilia R. | 14,20 | 11,35 | 11,66 | 13,60 | 12,51 | 11,62 | 10,38 | 13,56 |
| 61-70 | Emilia R. | 16,78 | 15,34 | 14,94 | 15,27 | 17,00 | 18,14 | 16,48 | 23,19 |
| 71–80 | Emilia R. | 19,82 | 17,07 | 15,54 | 22,25 | 20,35 | 21,50 | 20,22 | 31,13 |
| >80 | Emilia R. | 20,07 | 30,72 | 24,89 | 37,51 | 31,68 | 32,06 | 33,53 | 41,01 |
| 20–30 | Toscana | 4,07 | 5,06 | 4,89 | 4,45 | 5,17 | 5,05 | 6,01 | 5,47 |
| 31–40 | Toscana | 6,46 | 8,95 | 5,05 | 6,93 | 8,08 | 6,77 | 9,66 | 7,80 |
| 41–50 | Toscana | 12,97 | 8,74 | 6,88 | 8,19 | 8,12 | 11,33 | 10,57 | 9,17 |
| 51–60 | Toscana | 19,27 | 15,19 | 9,47 | 9,87 | 10,20 | 13,81 | 16,68 | 13,98 |
| 61–70 | Toscana | 18,30 | 15,20 | 15,16 | 14,91 | 12,80 | 18,86 | 19,94 | 17,31 |
| 71–80 | Toscana | 24,94 | 18,23 | 20,69 | 18,12 | 15,49 | 23,25 | 26,61 | 25,20 |
| >80 | Toscana | 27,25 | 36,16 | 30,86 | 26,17 | 28,07 | 33,42 | 33,33 | 36,31 |
| 20–30 | Umbria | 0,00 | 2,17 | 0,00 | 1,11 | 3,36 | 2,29 | 0,00 | 5,72 |
| 31–40 | Umbria | 6,26 | 6,14 | 5,98 | 3,37 | 6,68 | 3,35 | 4,96 | 7,45 |
| 41–50 | Umbria | 6,06 | 6,87 | 5,69 | 5,53 | 2,67 | 12,99 | 7,55 | 12,26 |
| 51–60 | Umbria | 8,29 | 11,25 | 7,09 | 7,96 | 11,68 | 9,73 | 10,66 | 14,59 |
| 61–70 | Umbria | 18,20 | 10,68 | 5,35 | 4,28 | 14,01 | 14,10 | 11,82 | 13,92 |
| 71–80 | Umbria | 12,32 | 15,88 | 7,35 | 13,50 | 20,98 | 17,30 | 14,93 | 18,57 |
| >80 | Umbria | 12,61 | 30,17 | 24,07 | 26,77 | 29,73 | 30,29 | 23,69 | 17,69 |
| 20–30 | Marche | 3,48 | 3,55 | 3,58 | 7,90 | 1,87 | 5,13 | 4,52 | 3,91 |
| 31–40 | Marche | 8,30 | 6,71 | 5,64 | 5,63 | 6,55 | 8,43 | 6,06 | 8,38 |
| 41–50 | Marche | 11,73 | 9,25 | 5,27 | 9,73 | 6,46 | 12,19 | 11,37 | 8,32 |
| 51–60 | Marche | 13,50 | 10,83 | 10,04 | 12,72 | 12,50 | 13,05 | 14,59 | 15,59 |
| 61–70 | Marche | 12,95 | 19,75 | 19,92 | 20,04 | 18,43 | 21,16 | 19,08 | 24,19 |
| 71–80 | Marche | 22,78 | 21,09 | 21,91 | 27,72 | 17,51 | 29,03 | 21,09 | 28,83 |
| >80 | Marche | 14,51 | 48,75 | 45,14 | 34,28 | 31,68 | 46,06 | 41,22 | 34,54 |
| 20–30 | Lazio | 9,46 | 8,68 | 8,42 | 10,93 | 9,68 | 9,49 | 8,20 | 9,66 |
| 31–40 | Lazio | 9,74 | 10,31 | 13,22 | 15,66 | 17,12 | 16,89 | 16,64 | 16,16 |
| 41–50 | Lazio | 14,29 | 16,61 | 13,90 | 15,73 | 19,58 | 17,58 | 16,57 | 17,11 |
| 51–60 | Lazio | 20,02 | 20,07 | 20,68 | 22,91 | 22,04 | 20,93 | 23,72 | 22,01 |
| 61–70 | Lazio | 28,36 | 24,79 | 30,41 | 24,47 | 27,61 | 26,00 | 27,70 | 27,83 |
| 71–80 | Lazio | 27,79 | 29,62 | 34,74 | 26,97 | 30,70 | 37,40 | 31,81 | 37,67 |
| >80 | Lazio | 26,16 | 52,49 | 59,15 | 41,53 | 53,27 | 62,49 | 45,63 | 56,36 |
| 20–30 | Abruzzo | 4,57 | 5,31 | 0,00 | 4,71 | 4,12 | 4,20 | 4,20 | 5,64 |
| 31–40 | Abruzzo | 6,26 | 4,49 | 4,42 | 6,03 | 8,26 | 3,88 | 7,74 | 9,45 |
| 41–50 | Abruzzo | 7,84 | 6,37 | 9,28 | 10,25 | 8,21 | 10,86 | 5,55 | 7,04 |
| 51–60 | Abruzzo | 12,54 | 9,35 | 7,02 | 13,71 | 9,28 | 8,56 | 5,21 | 9,06 |
| 61–70 | Abruzzo | 12,98 | 15,31 | 11,68 | 11,76 | 15,86 | 11,27 | 14,30 | 14,04 |
| 71–80 | Abruzzo | 19,00 | 18,76 | 23,19 | 19,43 | 10,58 | 29,81 | 17,53 | 19,18 |
| >80 | Abruzzo | 31,93 | 41,69 | 41,36 | 39,22 | 27,11 | 50,20 | 19,30 | 42,58 |
| 20–30 | Molise | 0,00 | 5,17 | 2,61 | 8,01 | 2,74 | 2,80 | 5,65 | 0,00 |
| 31–40 | Molise | 9,36 | 13,97 | 6,95 | 2,34 | 4,71 | 4,77 | 9,58 | 4,85 |
| 41–50 | Molise | 10,29 | 5,06 | 4,95 | 9,79 | 12,02 | 7,12 | 4,66 | 11,49 |
| 51–60 | Molise | 3,06 | 2,96 | 2,86 | 2,78 | 8,06 | 5,31 | 15,80 | 5,26 |
| 61–70 | Molise | 5,97 | 12,16 | 12,62 | 13,03 | 3,35 | 6,88 | 10,28 | 3,36 |
| 71–80 | Molise | 0,00 | 13,83 | 13,78 | 17,03 | 10,21 | 13,60 | 13,64 | 6,83 |
| >80 | Molise | 0,00 | 33,56 | 25,50 | 12,24 | 41,44 | 34,29 | 21,93 | 21,02 |
| 20–30 | Campania | 4,17 | 3,00 | 3,03 | 3,24 | 4,75 | 6,86 | 4,46 | 4,47 |
| 31–40 | Campania | 6,10 | 5,67 | 3,81 | 4,42 | 5,71 | 4,10 | 6,83 | 6,84 |
| 41–50 | Campania | 7,30 | 4,98 | 6,15 | 8,22 | 6,71 | 7,24 | 6,90 | 8,68 |
| 51–60 | Campania | 8,99 | 8,10 | 10,01 | 8,84 | 10,22 | 9,15 | 11,78 | 11,01 |
| 61–70 | Campania | 8,02 | 8,14 | 10,38 | 12,61 | 10,07 | 9,27 | 14,29 | 14,97 |
| 71–80 | Campania | 12,61 | 11,29 | 14,50 | 13,61 | 11,69 | 15,10 | 20,83 | 18,50 |
| >80 | Campania | 9,51 | 21,00 | 20,94 | 22,74 | 19,80 | 27,34 | 32,59 | 27,60 |
| 20–30 | Puglia | 3,24 | 3,66 | 3,33 | 3,97 | 3,13 | 2,83 | 5,20 | 6,61 |
| 31–40 | Puglia | 5,03 | 6,61 | 4,62 | 5,15 | 4,63 | 5,55 | 5,74 | 7,23 |
| 41–50 | Puglia | 13,59 | 7,91 | 8,56 | 4,78 | 8,15 | 9,71 | 10,06 | 9,51 |
| 51–60 | Puglia | 15,37 | 8,99 | 9,76 | 11,98 | 10,49 | 13,99 | 11,57 | 10,74 |
| 61–70 | Puglia | 17,66 | 18,49 | 11,55 | 15,10 | 17,59 | 14,69 | 18,56 | 14,78 |
| 71–80 | Puglia | 23,90 | 17,28 | 15,99 | 19,93 | 19,97 | 16,32 | 24,45 | 21,80 |
| >80 | Puglia | 14,37 | 26,10 | 27,56 | 35,05 | 31,01 | 24,46 | 36,58 | 39,98 |
| 20–30 | Basilicata | 0,00 | 0,00 | 1,34 | 2,73 | 2,80 | 1,44 | 4,41 | 3,00 |
| 31–40 | Basilicata | 3,62 | 0,00 | 0,00 | 1,23 | 3,74 | 3,78 | 3,82 | 3,88 |
| 41–50 | Basilicata | 2,79 | 2,73 | 1,33 | 5,25 | 3,86 | 6,37 | 5,02 | 8,66 |
| 51–60 | Basilicata | 12,08 | 5,03 | 4,88 | 4,72 | 6,05 | 8,95 | 4,41 | 10,27 |
| 61–70 | Basilicata | 9,99 | 13,64 | 7,07 | 18,30 | 9,46 | 19,48 | 9,82 | 13,61 |
| 71–80 | Basilicata | 10,50 | 18,67 | 4,12 | 16,11 | 9,95 | 15,83 | 7,93 | 13,77 |
| >80 | Basilicata | 4,90 | 18,39 | 4,34 | 32,68 | 19,86 | 7,56 | 7,19 | 10,23 |
| 20–30 | Calabria | 2,23 | 1,89 | 0,76 | 0,77 | 1,19 | 1,62 | 2,04 | 4,11 |
| 31–40 | Calabria | 3,31 | 2,21 | 2,93 | 3,70 | 6,36 | 3,41 | 4,16 | 5,70 |
| 41–50 | Calabria | 4,17 | 2,86 | 2,80 | 3,56 | 3,11 | 3,08 | 4,55 | 5,23 |
| 51–60 | Calabria | 7,00 | 2,93 | 3,35 | 6,05 | 1,80 | 8,46 | 3,98 | 8,34 |
| 61–70 | Calabria | 5,39 | 5,48 | 5,59 | 3,98 | 4,62 | 6,44 | 5,19 | 5,06 |
| 71–80 | Calabria | 13,10 | 11,49 | 6,67 | 7,89 | 7,17 | 7,74 | 9,00 | 9,59 |
| >80 | Calabria | 18,48 | 30,50 | 20,82 | 17,01 | 21,13 | 26,10 | 12,49 | 17,52 |
| 20–30 | Sicilia | 9,28 | 4,88 | 2,53 | 3,38 | 3,45 | 3,02 | 2,53 | 2,55 |
| 31–40 | Sicilia | 11,57 | 4,88 | 3,52 | 4,57 | 4,14 | 5,37 | 7,48 | 6,34 |
| 41–50 | Sicilia | 9,02 | 6,35 | 4,40 | 5,78 | 5,37 | 6,86 | 5,68 | 7,12 |
| 51–60 | Sicilia | 10,38 | 6,96 | 8,12 | 9,45 | 7,42 | 8,43 | 7,72 | 8,42 |
| 61–70 | Sicilia | 14,19 | 9,67 | 10,67 | 10,82 | 12,47 | 10,20 | 17,79 | 13,54 |
| 71–80 | Sicilia | 16,28 | 15,76 | 14,27 | 13,93 | 13,54 | 16,93 | 21,63 | 15,62 |
| >80 | Sicilia | 11,51 | 37,89 | 26,12 | 27,56 | 25,64 | 28,91 | 27,65 | 21,31 |
| 20–30 | Sardegna | NA * | NA * | 1,40 | 0,48 | 2,00 | 2,07 | 0,53 | 2,19 |
| 31–40 | Sardegna | NA * | NA * | 4,53 | 2,87 | 5,74 | 4,11 | 2,89 | 4,16 |
| 41–50 | Sardegna | NA * | NA * | 5,00 | 4,46 | 2,61 | 5,97 | 4,61 | 4,54 |
| 51–60 | Sardegna | NA * | NA * | 12,15 | 7,24 | 7,04 | 8,41 | 2,93 | 5,80 |
| 61–70 | Sardegna | NA * | NA * | 16,02 | 5,70 | 7,44 | 6,72 | 4,18 | 14,03 |
| 71–80 | Sardegna | NA * | NA * | 15,92 | 7,80 | 10,15 | 6,70 | 4,11 | 17,09 |
| >80 | Sardegna | NA * | NA * | 23,22 | 13,51 | 17,68 | 15,48 | 13,31 | 21,28 |


Discussion
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Sladden, M.J.; Balch, C.; Barzilai, D.A.; Berg, D.; Freiman, A.; Handiside, T.; Hollis, S.; Lens, M.B.; Thompson, J.F. Surgical excision margins for primary cutaneous Melanoma. Cochrane Database Syst. Rev. 2009. [Google Scholar] [CrossRef] [Green Version]
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [PubMed]
- Pappo, A.S. Melanoma in children and adolescents. Eur. J. Cancer 2003, 39, 2651–2661. [Google Scholar] [CrossRef] [PubMed]
- AIRT Working Group. Italian cancer figures-report 2006: 1. Incidence, mortality and estimates. Epidemiol. Prev. 2006, 30, 8–10. [Google Scholar]
- Pisani, P.; Parkin, D.M.; Bray, F.; Ferlay, J. Estimates of the worldwide mortality from 25 cancers in 1990. Int. J. Cancer 1999, 83, 18–29. [Google Scholar] [CrossRef]
- Bickers, D.R.; Lim, H.W.; Margolis, D.; Weinstock, M.A.; Goodman, C.; Faulkner, E.; Gould, C.; Gemmen, E.; Dall, T. The burden of skin diseases: 2004 a joint project of the American Academy of Dermatology Association and the Society for Investigative Dermatology. J. Amer. Acad. Dermatol. 2006, 55, 490–500. [Google Scholar] [CrossRef] [PubMed]
- AIRT Working Group. Italian cancer figures, report 2009: Cancer trend (1998–2005). Epidemiol. Prev. 2009, 33, 1–168. [Google Scholar]
- Freeman, J.L.; Zhang, D.; Freeman, D.H.; Goodwin, J.S. An approach to identifying incident breast cancer cases using Medicare claims data. J. Clin. Epidemiol. 2000, 53, 605–614. [Google Scholar] [CrossRef]
- Penberthy, L.; McClish, D.; Pugh, A.; Smith, W.; Manning, C.; Retchin, S. Using hospital discharge files to enhance cancer surveillance. Amer. J. Epidemiol. 2003, 158, 27–34. [Google Scholar] [CrossRef]
- Piscitelli, P.; Santoriello, A.; Buonaguro, F.M.; Di Maio, M.; Iolascon, G.; Gimigliano, F.; Marinelli, A.; Distante, A.; Serravezza, G.; Sordi, E.; et al. Incidence of breast cancer in Italy: mastectomies and quadrantectomies performed between 2000 and 2005. J. Exp. Clin. Cancer Res. 2009, 28, 86. [Google Scholar] [CrossRef] [PubMed]
- Piscitelli, P.; Barba, M.; Crespi, M.; Di Maio, M.; Santoriello, A.; D’Aiuto, M.; Fucito, A.; Losco, A.; Pentimalli, F.; Maranta, P.; et al. The burden of breast cancer in Italy: mastectomies and quadrantectomies performed between 2001 and 2008 based on nationwide hospital discharge records. J. Exp. Clin. Cancer Res. 2012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Environment Protection Agency of Piemonte, Healthcare indicators in Piemonte Region. Available online: http://www.arpa.piemonte.it/reporting/indicatori-on_line/qualita-della-vita/salute_dimissioni-ospedaliere (accessed 26 July 2015).
- Holterhues, C. Trends in incidence of cutaneous malignant Melanoma in Europe: Analysis of population based cancer registry data. Melanoma Res. 2010. [Google Scholar] [CrossRef]
- Parkin, D.M.; Bray, F.; Ferlay, J.; Pisani, P. Global cancer statistics, 2002. CA Cancer J. Clin. 2005, 55, 74–108. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.M.; Barrett, J.H.; Bishop, D.T.; Armstrong, B.K.; Bataille, V.; Bergman, W.; Berwick, M.; Bracci, P.M.; Elwood, J.M.; Ernstoff, M.S.; et al. Sun exposure and Melanoma risk at different latitudes: a pooled analysis of 5700 cases and 7216 controls. Int. J. Epidemiol. 2009, 38, 814–830. [Google Scholar] [CrossRef] [PubMed]
- Crocetti, E.; Buzzoni, C.; Chiarugi, A.; Nardini, P.; Pimpinelli, N. Relationship between Latitude and Melanoma in Italy. ISRN Oncol. 2012. [Google Scholar] [CrossRef] [PubMed]
- Murali, R.; Desilva, C.; Thompson, J.F.; Scolyer, R.A. Factors predicting recurrence and survival in sentinel lymph node-positive Melanoma patients. Ann. Surg. 2011, 253, 1155–1164. [Google Scholar] [CrossRef] [PubMed]
- De Giorgi, V.; Mavilia, C.; Massi, D.; Gozzini, A.; Aragona, P.; Tanini, A.; Sestini, S.; Paglierani, M.; Boddi, V.; Brandi, M.L.; et al. Estrogen receptor expression in cutaneous Melanoma: A real-time reverse transcriptase-polymerase chain reaction and immunohistochemical study. Arch. Dermatol. 2009, 145, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Balch, C.M.; Gershenwald, J.E.; Soong, S.J.; Thompson, J.F.; Atkins, M.B.; Byrd, D.R.; Buzaid, A.C.; Cochran, A.J.; Coit, D.G.; Ding, S.; et al. Final version of 2009 AJCC Melanoma staging and classification. J. Clin. Oncol. 2009, 27, 6199–6206. [Google Scholar] [CrossRef] [PubMed]
- Korn, E.L.; Liu, P.Y.; Lee, S.J.; Chapman, J.A.; Niedzwiecki, D.; Suman, V.J.; Moon, J.; Sondak, V.K.; Atkins, M.B.; Eisenhauer, E.A.; et al. Meta-analysis of phase II cooperative group trials in metastatic stage IV Melanoma to determine progression-free and overall survival benchmarks for future phase II trials. J. Clin. Oncol. 2008, 26, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Chapman, P.B.; Einhorn, L.H.; Meyers, M.L.; Saxman, S.; Destro, A.N.; Panageas, K.S.; Begg, C.B.; Agarwala, S.S.; Schuchter, L.M.; Ernstoff, M.S.; et al. Phase III multicenter randomized trial of the Dartmouth regimen versus dacarbazine in patients with metastatic Melanoma. J. Clin. Oncol. 1999, 17, 2745–2751. [Google Scholar] [PubMed]
- Middleton, M.R.; Grob, J.J.; Aaronson, N.; Fierlbeck, G.; Tilgen, W.; Seiter, S.; Gore, M.; Aamdal, S.; Cebon, J.; Coates, A.; et al. Randomized phase III study of temozolomide versus dacarbazine in the treatment of patients with advanced metastatic malignant Melanoma. J. Clin. Oncol. 2000, 18, 158–166. [Google Scholar] [PubMed]
- Avril, M.F.; Aamdal, S.; Grob, J.J.; Hauschild, A.; Mohr, P.; Bonerandi, J.J.; Weichenthal, M.; Neuber, K.; Bieber, T.; Gilde, K.; et al. Fotemustine compared with dacarbazine in patients with disseminated malignant Melanoma: A phase III study. J. Clin. Oncol. 2004, 22, 1118–1125. [Google Scholar] [CrossRef] [PubMed]
- Bedikian, A.Y.; Millward, M.; Pehamberger, H.; Conry, R.; Gore, M.; Trefzer, U.; Pavlick, A.C.; DeConti, R.; Hersh, E.M.; Hersey, P.; et al. Bcl-2 antisense (oblimersen sodium) plus dacarbazine in patients with advanced Melanoma: the Oblimersen Melanoma Study Group. J. Clin. Oncol. 2006, 24, 4738–4745. [Google Scholar] [CrossRef] [PubMed]
- Atkins, M.B.; Lotze, M.T.; Dutcher, J.P.; Fisher, R.I.; Weiss, G.; Margolin, K.; Abrams, J.; Sznol, M.; Parkinson, D.; Hawkins, M.; et al. High-dose recombinant interleukin 2 therapy for patients with metastatic Melanoma: Analysis of 270 patients treated between 1985 and 1993. J. Clin. Oncol. 1999, 17, 2105–2116. [Google Scholar] [PubMed]
- Hodi, F.S.; O’Day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C.; et al. Improved survival with ipilimumab in patients with metastatic Melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef] [PubMed]
- Chapman, P.B.; Hauschild, A.; Robert, C.; Haanen, J.B.; Ascierto, P.; Larkin, J.; Dummer, R.; Garbe, C.; Testori, A.; Maio, M.; et al. Improved survival with vemurafenib in Melanoma with BRAF V600E mutation. N. Engl. J. Med. 2011, 364, 2507–2516. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piscitelli, P.; Neglia, C.; Falco, A.; Rivezzi, M.; Agnello, N.; Argentiero, A.; Chitano, G.; Distante, C.; Rosa, G.D.; Vinci, G.; et al. Melanoma in the Italian Population and Regional Environmental Influences: A National Retrospective Survey on 2001–2008 Hospitalization Records. Int. J. Environ. Res. Public Health 2015, 12, 9102-9118. https://doi.org/10.3390/ijerph120809102
Piscitelli P, Neglia C, Falco A, Rivezzi M, Agnello N, Argentiero A, Chitano G, Distante C, Rosa GD, Vinci G, et al. Melanoma in the Italian Population and Regional Environmental Influences: A National Retrospective Survey on 2001–2008 Hospitalization Records. International Journal of Environmental Research and Public Health. 2015; 12(8):9102-9118. https://doi.org/10.3390/ijerph120809102
Chicago/Turabian StylePiscitelli, Prisco, Cosimo Neglia, Andrea Falco, Matteo Rivezzi, Nadia Agnello, Alberto Argentiero, Giovanna Chitano, Chiara Distante, Giulia Della Rosa, Giorgia Vinci, and et al. 2015. "Melanoma in the Italian Population and Regional Environmental Influences: A National Retrospective Survey on 2001–2008 Hospitalization Records" International Journal of Environmental Research and Public Health 12, no. 8: 9102-9118. https://doi.org/10.3390/ijerph120809102