
Understanding Health Information Seeking from an Actor-Centric Perspective

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
Methods
2. The Changing Health Knowledge Economy
2.1. Changes in the Complex Health Knowledge Economy
2.2. Changes in the Use of ICT to Access These Providers
2.3. Changes in the Health Knowledge Economy and Information Seeking
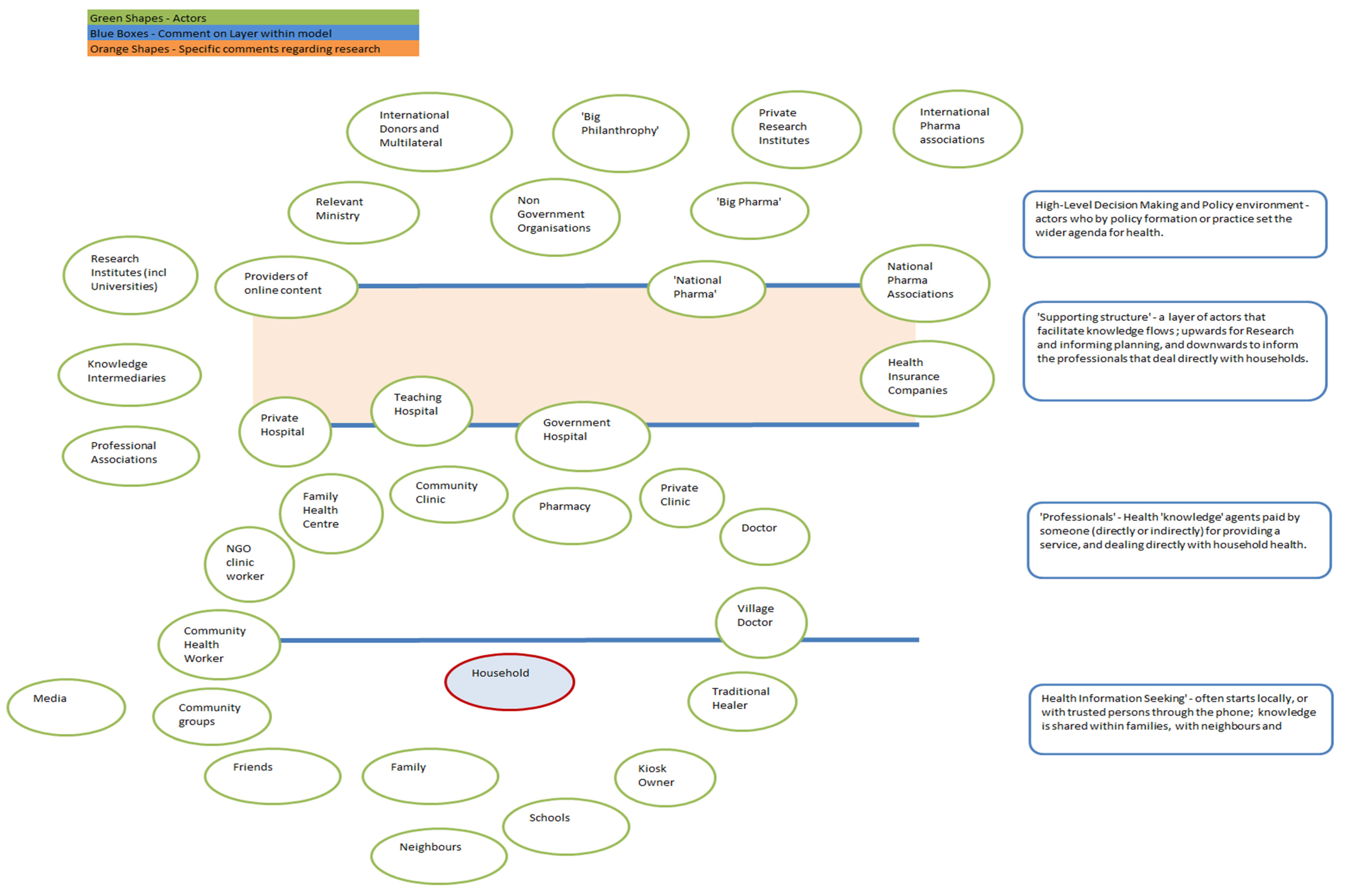
3. Developing an Actor-Centric Approach
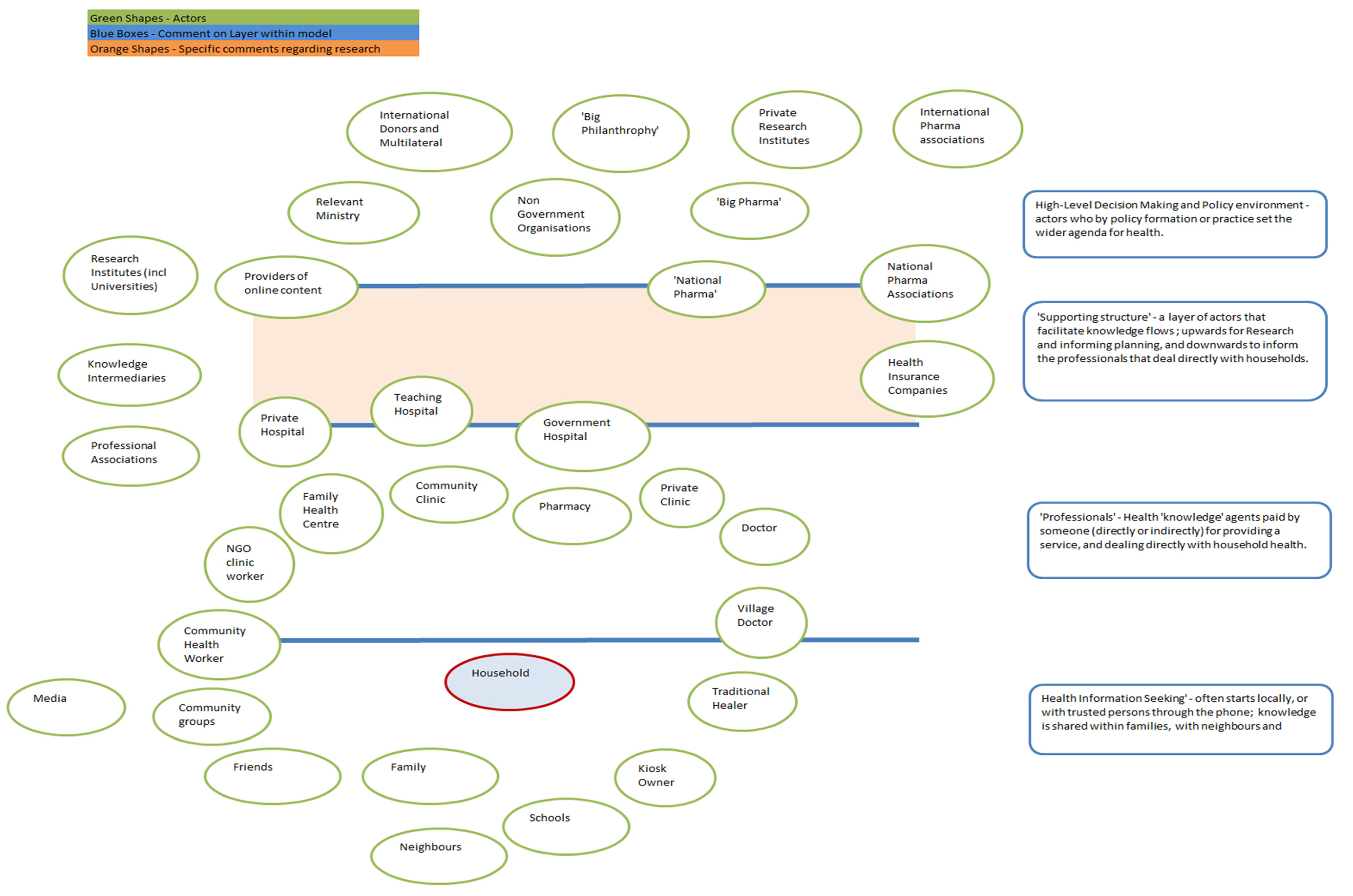
- High-level decision-making and policy environment (including government and political private sector actors)
- Supporting Structure of actors that facilitate knowledge flows
- Professional health knowledge agents
- Person-to-person engagement and trusted support.
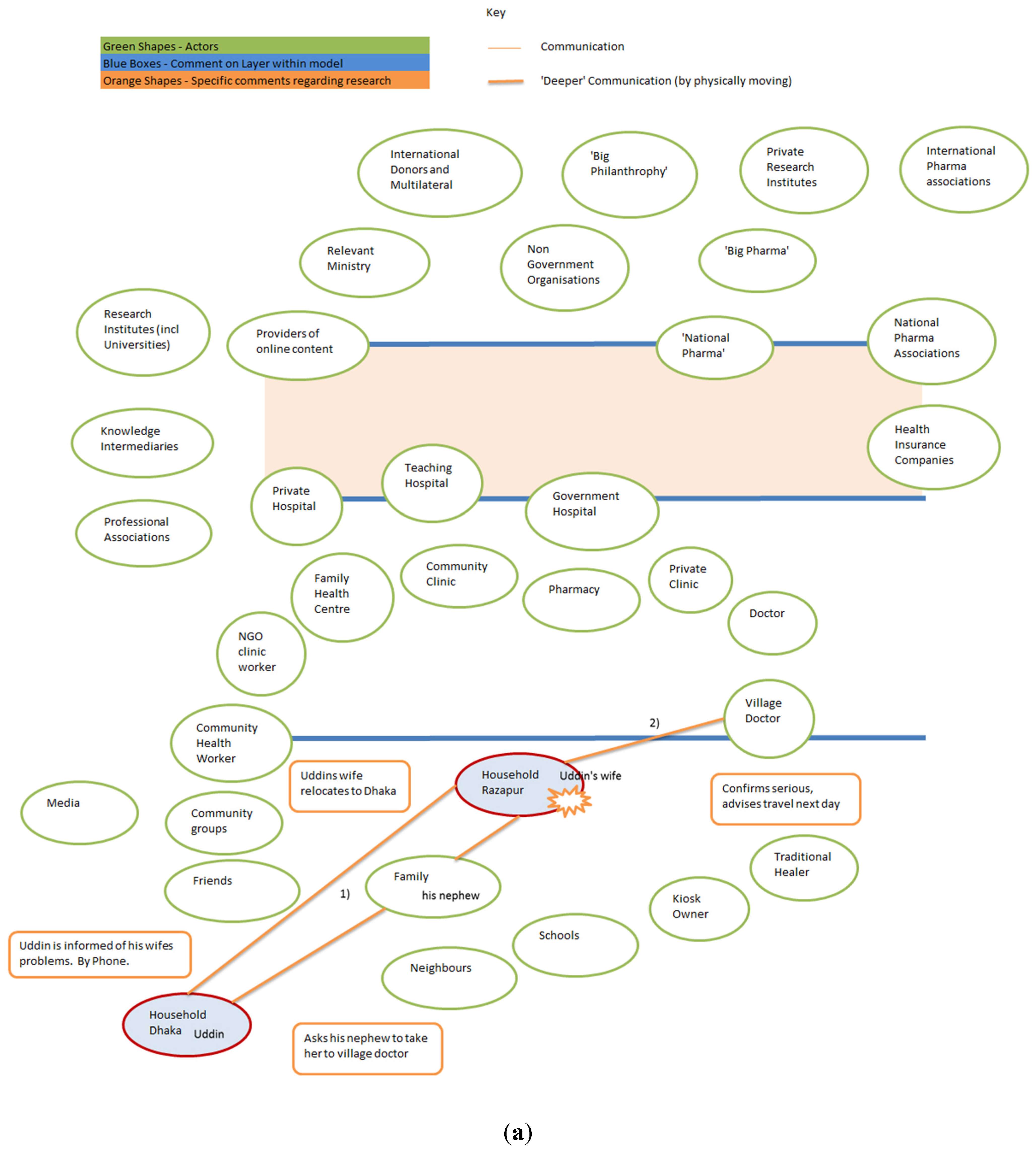
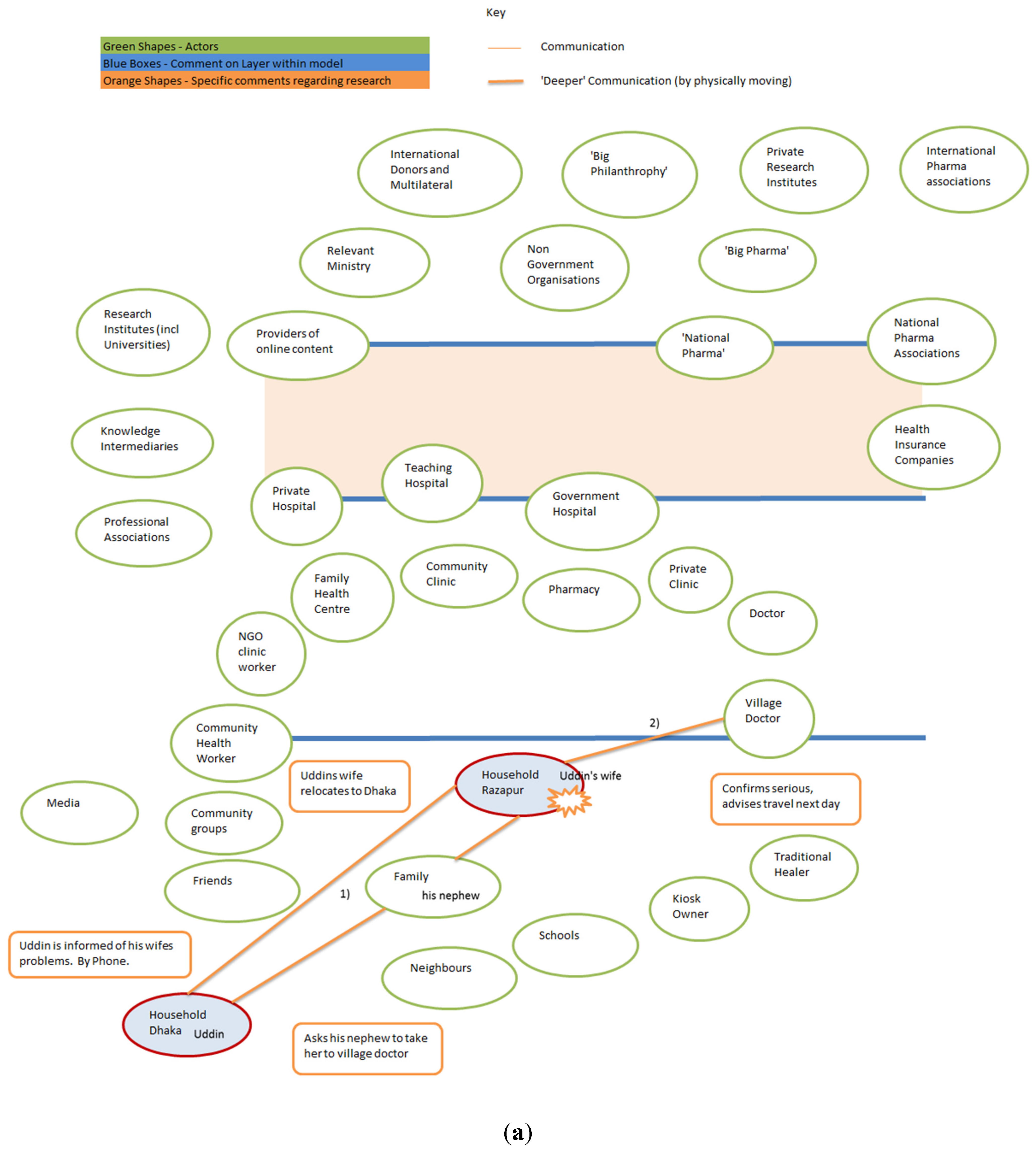
4. Mapping a Bangladesh Case Study

- (1)
- Uddin was not at home and he asked his nephew to bring her to Dhaka to ensure that she received treatment.
- (2)
- They took her to the village doctor, an informal health provider in the village, for treatment and reported to Uddin that her condition was serious and that they would only travel the following morning (see Figure 3a).
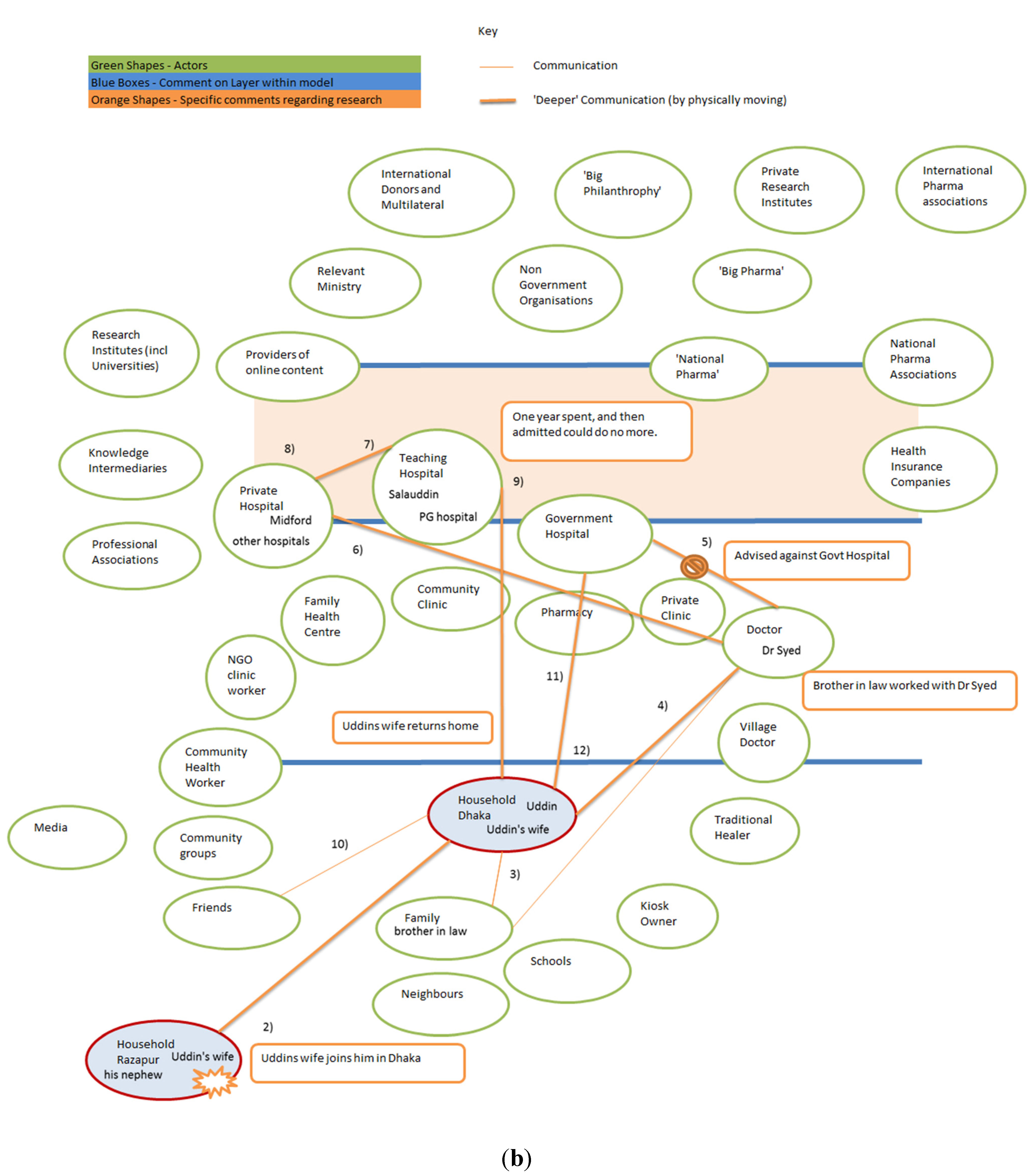
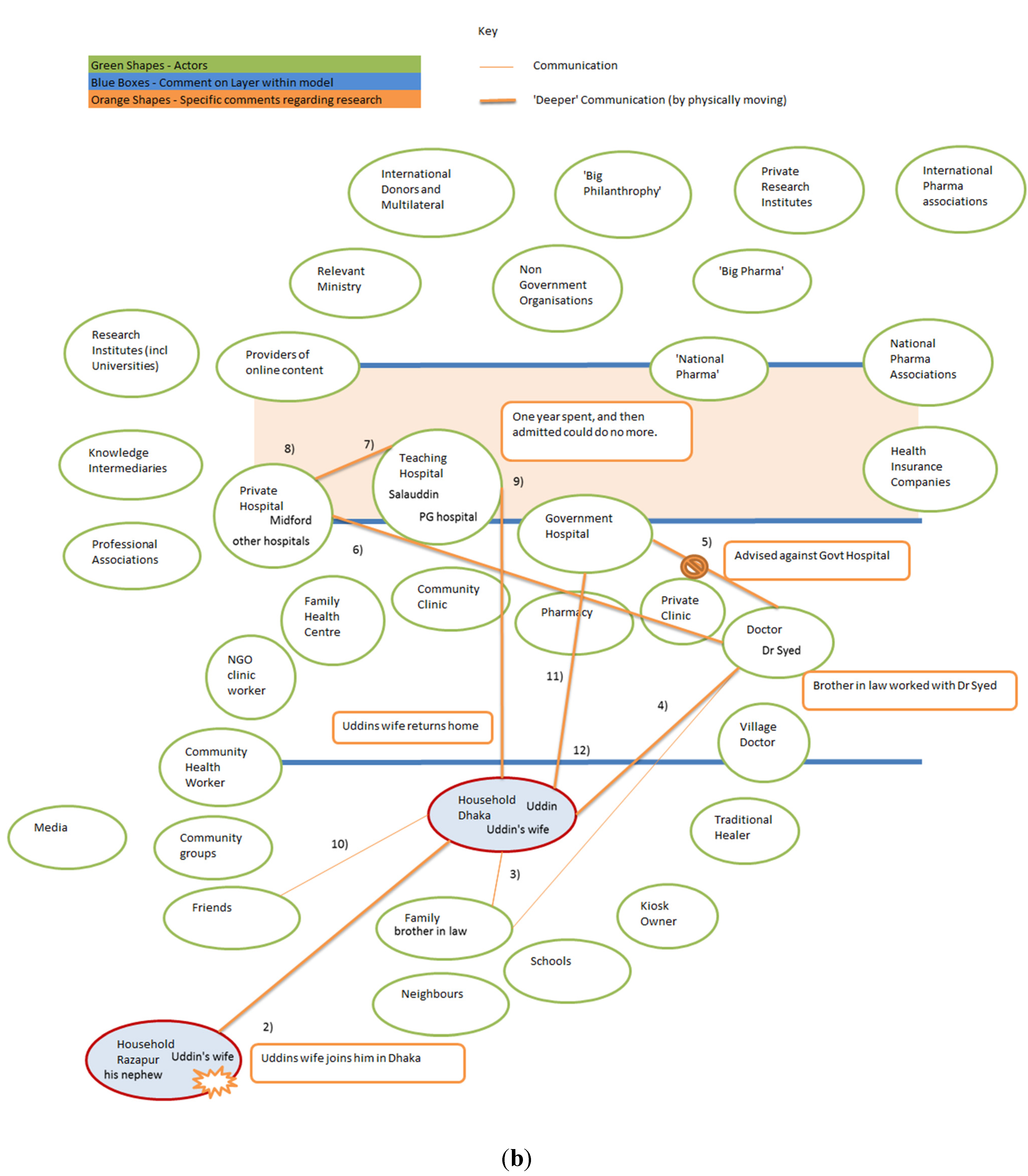
- (3)
- When she arrived in Dhaka (continued in Figure 3b), Uddin consulted with his brother-in-law and
- (4)
- Decided she should visit Dr. Syed in Jatrabari, Dhaka. He chose Dr. Syed because his brother-in-law worked with the doctor. Uddin’s brother in law said: “Dr. Syed will give what will be best”. Dr. Syed informed Uddin that she needed to go to hospital immediately. They discussed whether a government upazila Health Complex or private hospital would be best and
- (5)
- Dr. Syed advised against an upazila health complex because of the long wait for an appointment.
- (6)
- Dr. Syed provided Uddin with the address of a tertiary level government hospital, the Mitford in Dhaka, which offers a free service for the poor, where Uddin’s wife was admitted and had an MRI (Magnetic Resonance Imaging) scan, but where she received no treatment, so
- (7)
- She went to Salauddin private hospital and
- (8)
- Then spent a year at PG Government Tertiary Teaching hospital receiving treatment, until they admitted that they could do no more for her, but Uddin continued to seek treatment for his wife.
- (10)
- While Uddin was in Malaysia, he discussed his wife’s illness with one of his fellow migrants. This migrant told Uddin about “his uncle who is a doctor who lives in Mohakhali” and who worked at the Government specialized cancer hospital. He then talked to his uncle about Uddin’s wife.
- (11)
- Uddin sent a large sum of money to this doctor as an upfront payment, and this ensured treatment and medicine.
- (12)
- After being released from this hospital, Uddin’s wife was better able to feed herself and walk around, but then she developed an ulcer on her leg and subsequent complications. She died before she was able to seek further treatment.
5. What is the Role of ICTs in Health Knowledge Systems?
- The lack of skilled healthcare staff: Yonazi et al. [65] suggest that “eLearning and telemedicine solutions can extend expertise to remote areas and provide otherwise inaccessible care”. This is a key role for the actor centric approach proposed in this paper, and which draws attention to asking who the healthcare workers are, and emphasizes both formal and informal providers. The Bangladesh heath system has community volunteers funded by NGOs, as well as long-standing village doctors. Pharmacists often offer advice. While it is accepted that ICTs could be used to strengthen the skill of healthcare workers, the identification of relevant healthcare workers who require this additional learning is a priority. In addition, as Malone et al. have shown, even in high-income contexts, the quality of access to health care can have a significant impact on online health information seeking with “ease of access” positively influencing information seeking [58]. In contexts such as Bangladesh where access to skilled health care is extremely difficult, the data suggests that online searching is currently not highly valued.
- Health information system inadequacies: “Data collection and surveillance mHealth applications can monitor and track health indicators in real time, providing insight to policymakers on true challenges and providing valuable data enabling health workers to better serve and patients to be more proactive in their own health” [65]. The feedback of data from the field to policy actors has long been recognized as important. But applying an actor centric model forces one to ask: which actors need to supply the data? Will only the formal system provide data, or would it be possible to engage with the informal healthcare workers to provide feedback that might make policy development more evidenced based and potentially more responsive to the needs of the poor? [56]. Village doctors are often, as shown in the above account, a critical entry point into the health system. Experimentation with using mHealth with village doctors in Bangladesh has not, to date, been successful and more work needs to be done for mHealth to offer a useful service to these informal health suppliers.
- Insufficient equipment, medication and other supplies: “Supply Chain Management mHealth applications can decrease stock-out frequency and increase efficacy of and trust in health system” [65]. An actor centric perspective focuses on who is providing drugs and equipment, rather than assuming that these are available only from formal providers. In Bangladesh, the challenge is not just the shortage of drugs and equipment but the attachment of good advice to the provision of drugs and equipment. Data from many emerging economies suggests that fake drugs can be killers, and, in Bangladesh, even a genuine drug taken for an inappropriate illness or in inappropriate dosage is a waste of limited resources and can do more harm than good [37]. In addition, although not explicitly developed in the above account of Uddin’s wife, it is evident that there is substantial scope for patients to receive different and multiple drugs from different providers and to not complete a course of medication.
- Lack of information concerning preventable diseases: “Public health promotion applications can be used to disseminate empowering information in a friendly, personal manner. Engaging without being intrusive” [65]. Our example shows the connectedness of society, and helps visualize the processes of health information seeking through the mapping of information flows. It is not enough to provide information on a Short Message System (SMS) text if no one reads the text. In many resource poor settings, a lack of literacy prevents the reading of a text by a significant portion of the population, and overuse of unsolicited texts has meant that many of those who could read the text no longer bother to. In addition, even though Uddin would have had several possible ways of accessing information through mHealth (phoning a health help line, reading government-sent SMS messages), at no point did he avail himself of these possibilities. An actor centric perspective encourages researchers to explore who talks to who, how they communicate and what kinds of information they are seeking.
- Financial limitations: “Health financing and personal insurance programmes offer increased opportunities for savings, both for patients and healthcare providers” [65]. ICT has opened up financial systems to resource poor communities. Uddin’s story illustrates how less-formalized financial flows compromise an integral part of the health information seeking, and ICTs can facilitate enhanced communication between people, thus aiding individuals in their search for health financing mechanisms, and enable more innovative financial flows between actors.
6. Theory of Planned Behavior
7. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Bloom, G.; Standing, H. Future health systems: Why future, why now? Soc. Sci. Med. 2008, 66, 2067–2075. [Google Scholar] [CrossRef] [PubMed]
- Bloom, G.; Standing, H.; Lloyd, R. Markets, information asymmetry and health care: Towards new social contracts. Soc. Sci. Med. 2008, 66, 2076–2087. [Google Scholar] [CrossRef] [PubMed]
- Bloom, G.; Ainsworth, P. Beyond Scaling Up: Towards Universal Access to Health Services. In STEPS Centre Working Paper 40; STEPS Centre: Brighton, UK, 2010. [Google Scholar]
- Lucas, H. Information and communications technology for future health systems in developing countries. Soc. Sci. Med. 2008, 66, 2122–2132. [Google Scholar] [CrossRef] [PubMed]
- Mayhew, M.; Hansen, P.M.; Peters, D.; Edward, A.; Singh, L.P.; Dwivedi, V.; Mashkoor, A.; Burnham, G. Determinants of skilled birth attendant utilization in Afghanistan where basic health services are provided—A cross-sectional study. Amer. J. Public Health 2008, 98, 1849–1856. [Google Scholar] [CrossRef] [PubMed]
- Tripathi, M. Transforming India into a knowledge economy through information communication technologies—Current developments. Int. Inf. Libr. Rev. 2006, 38, 139–146. [Google Scholar] [CrossRef]
- Leonard, D.; Bloom, G.; Hanson, K.; O’Farrell, J.; Spicer, N. Institutional solutions to the asymmetric information problem in health and development services for the poor. World Dev. 2013, 48, 71–87. [Google Scholar] [CrossRef]
- Bloom, G.; Wolcott, S. Building institutions for health and health systems in contexts of rapid change. Soc. Sci. Med. 2012, 96, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Heeks, R. Where next for ICTs and international development? In ICTs for Development; OECD: Paris, France, 2009; pp. 29–74. [Google Scholar]
- Heeks, R. Do information and communication technologies (ICTs) contribute to development? J. Int. Dev. 2010, 22, 625–640. [Google Scholar] [CrossRef]
- ICT4D: Information and Communication Technology for Development; Cambridge University Press: Cambridge, UK, 2009.
- McNamara, E.K. Enhancing the Livelihoods of the Rural Poor Through ICT: A Knowledge Map, Working Paper 9; Overseas Development Institute: London, UK, 2008. [Google Scholar]
- Hamel, J.Y. ICT4D and the Human Development and Capabilities Approach: The Potentials of Information and Communication Technology; UNDP: New York, NY, USA, 2010. [Google Scholar]
- Smith, M.L.; Spence, R. ICT, Development, and poverty reduction: Five emerging stories. Annenb. Sch. Commun. J. 2010, 6, 11–17. [Google Scholar]
- Mehl, G.; Labrique, A. Prioritizing integrated mHealth strategies for universal health coverage. Science 2014, 345, 1284–1287. [Google Scholar] [CrossRef] [PubMed]
- Leon, N.; Schneider, H. MHealth4CBS in South Africa: A Review of the Role of Mobile Phone Technology for the Monitoring and Evaluation of Community Based Health Services; Medical Research Council and University of Western Cape: Cape Town, South Africa, 2012. [Google Scholar]
- WHO Glossary. 2015. Available online: http://www.who.int/trade/glossary/story021/en/ (accessed on 31 January 2015).
- Batchelor, S.; Scott, N.; Manfre, C. Sustainable Agriculture: A Mobile Landscape; Prince of Wales International Sustainability Unit and Oxfam Great Britain: Reading, United Kingdom, 2014. [Google Scholar]
- Labrique, A.; Vasudevana, L.; Kochi, E.; Fabricant, R.; Mehl, G. mHealth innovations as health system strengthening tools: 12 Common appliances and a visual framework. Glob. Health Sci. Pract. 2013, 1, 160–171. [Google Scholar] [CrossRef] [PubMed]
- Jennings, L.; Gagliardi, L. Influence of mhealth interventions on gender relations in developing countries: A systematic literature review. Int. J. Equity Health 2013, 12. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Evans, T.; Standing, H.; Mahmud, S. Harnessing pluralism for better health in Bangladesh. Lancet 2013, 382, 1746–1755. [Google Scholar] [CrossRef]
- Ahmed, S.M.; Adams, A.M.; Chowdhurya, M.; Bhuiya, A. Gender, socioeconomic development and health-seeking behavior in Bangladesh. Soc. Sci. Med. 2000, 51, 361–371. [Google Scholar] [CrossRef]
- Bangladesh Health Watch. Health Workforce in Bangladesh: Who Constitutes the Health Care System? The State of Health in Bangladesh 2007; BRAC University: Dhaka, Bangladesh, 2008; Available online: http://sph.bracu.ac.bd/images/reports/bhw/2007/Full_Report_2007_Final.pdf (accessed on 10 July 2015).
- Rashid, S.F.; Akram, O.; Standing, H. The sexual and reproductive health care market in Bangladesh: Where do poor women go? Reprod. Health Matters 2011, 19, 21–31. [Google Scholar] [CrossRef]
- Ahmed, S.M.; Petzold, M.; Kabir, Z.N.; Tomson, G. Targeted intervention for the ultra poor in rural Bangladesh: Does it make any difference in their health-seeking behavior? Soc. Sci. Med. 2006, 63, 2899–2911. [Google Scholar] [CrossRef] [PubMed]
- Paul, B.K.; Rumsey, D.J. Utilization of health facilities and trained birth attendants for childbirth in rural Bangladesh: An empirical study. Soc. Sci. Med. 2002, 54, 1755–1765. [Google Scholar] [CrossRef]
- Lane, R. Profile: Mushtaque Chowdhury: Seeking health transition in Bangladesh. Lancet 2013, 382. [Google Scholar] [CrossRef]
- Heller, L.R. Do slums matter? Location and early childhood preventive care choices among urban residents of Bangladesh. Soc. Sci. Med. 2013, 94, 43–55. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.T.H.; Hatt, L.; Islam, M.; Sloan, N.L.; Chowdhury, J.; Schmidt, J.-O.; Hossain, A.; Wang, H. Encouraging maternal health service utilization: An evaluation of the Bangladesh voucher program. Soc. Sci. Med. 2012, 74, 989–996. [Google Scholar] [CrossRef] [PubMed]
- Paul, B.K. National health care “by-passing” in Bangladesh: A comparative study. Soc. Sci. Med. 1999, 49, 679–689. [Google Scholar] [CrossRef]
- Bhardway, S.M.; Paul, B.K. Medical pluralism and infant mortality in a rural area of Bangladesh. Soc. Sci. Med. 1986, 23, 1003–1010. [Google Scholar] [CrossRef]
- Rahman, Z.; Agrawal, A.K. Understanding the role of “process” in value co-creation. In Proceedings of the 3rd Biennial Conference of the Indian Academy of Management (IAM), IIM Ahmedabad, India, 12–14 December 2013.
- Chowdhury, A.M.R.; Bhuiya, A.; Chowdhury, M.E.; Rasheed, S.; Hussain, Z.; Chen, L.C. The Bangladesh paradox: Exceptional health achievement despite economic poverty. Lancet 2013, 382, 1734–1745. [Google Scholar] [CrossRef]
- Uddin, M.J.; Koehlmoos, T.L.; Ashraf, A.; Saha, N.C.; Hossain, M. Health needs and health-care-seeking behavior of street-dwellers in Dhaka, Bangladesh. Health Policy Plan. 2009, 24, 385–394. [Google Scholar] [CrossRef] [PubMed]
- Amin, R.; Shah, N.M.; Becker, S. Socioeconomic factors differentiating maternal and child health-seeking behavior in rural Bangladesh: A cross-sectional analysis. Int. J. Equity Health. 2010, 9. [Google Scholar] [CrossRef] [PubMed]
- Moran, A.C.; Winch, P.J; Sultana, N; Kalim, N.; Afzal, K.M.; Koblinsky, M.; Arifeen, S.E.; Seraji, M.H.; Mannan, I.; Darmstadt, G.L.; et al. Patterns of maternal care seeking behaviors in rural Bangladesh. Trop. Med. Int. Health 2007, 12, 823–832. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.M.; Haque, R.; Haque, U.; Hossain, A. Knowledge on the transmission, prevention and treatment of malaria among two endemic populations of Bangladesh and their health-seeking behavior. Malar. J. 2009, 8. [Google Scholar] [CrossRef] [PubMed]
- WHO. M-Health: New Horizons for Health through Mobile Technologies. In Global Observatory for eHealth Series; WHO: Geneva, Switzerland, 2011; Volume 3. [Google Scholar]
- Applications of 3G technology: Views of Teachers and Students in Dhaka City. In ICT for Development Working Paper Series: Spearheading ICT4D Knowledge; BIID & ULAB: Dhaka, Bangladesh, 2012; Volume 2, pp. 73–92.
- Union Information and Service Centre: ICT-enabled One Stop e-Service outlet for rural citizens of Bangladesh. In ICT for Development Working Paper Series: Spearheading ICT4D Knowledge; BIID & ULAB: Dhaka, Bangladesh, 2012; Volume 2, pp. 30–42.
- Wilson, T.D. Models in information behavior research. J. Doc. 1999, 55, 249–270. [Google Scholar] [CrossRef]
- Ybarra, M.L.; Suman, M. Help seeking behavior and the Internet: A national survey. Int. J. Med. Inform. 2006, 75, 29–41. [Google Scholar] [CrossRef] [PubMed]
- Case, D.O. Looking for Information: A Survey of Research on Information Seeking, Needs, and Behavior; Academic Press: Burling, MA, USA, 2007. [Google Scholar]
- Johnson, C.A. Choosing people: The role of social capital in information seeking behavior. Sch. Inf. Stud. 2004, 10, Paper 201. [Google Scholar]
- Urqhart, C. Meta-synthesis of research on information seeking behavior. Inf. Res. 2011, 16, 1368–1613. [Google Scholar]
- Ogden, J.; Daniells, E.; Barnett, J. When is choice a good thing? An experimental study of the impact of choice on patient outcomes. Psychol. Health Med. 2009, 14, 34–47. [Google Scholar] [CrossRef] [PubMed]
- Wilson, T.D. Information-seeking behavior and the digital information world. Indexer 2006, 25, 28–31. [Google Scholar]
- Addison, J.; Glover, S.W.; Thornton, C. The impact of information skills training on independent literature searching activity and requests for mediated literature searches. Health Inf. Libr. J. 2010, 27, 191–197. [Google Scholar] [CrossRef] [PubMed]
- McKemey, K.; Scott, N.; Souter, D.; Afullo, T.; Kibombo, R.; Sakyi-Dawson, O. Innovative Demand Models for Telecommunications Services, Innovative Demand for Models for Telecommunications Service; Technical Report, Gamos Ltd.: Reading, UK, 2003. [Google Scholar]
- Scott, N.; Ndiwalana, A.; Sumner, A.; Batchelor, S. Rural Communities and Communication needs (Uganda); Grameen Foundation AppLab, Gamos Ltd.: Reading, UK, 2008. [Google Scholar]
- Stork, S.; Esselaar, S. Towards an African Index: SME e-Access and Usage Across 14 African Countries; Research ICT Africa: Cape Town, South Africa, 2006. [Google Scholar]
- Gillwald, A.; Stork, C. Towards Evidence Based ICT Policy and Regulation: ICT Access and Usage in Africa; Research ICT Africa: Cape Town, South Africa, 2008; Volume 1. [Google Scholar]
- De Silva, H.; Ratnadiwarkara, D.; Zainudeen, A. Social Influence in Mobile Phone Adoption: Evidence from the Bottom of Pyramid in Emerging Asia; SSRN: Rochester, NY, USA, 2009. [Google Scholar]
- Scott, N.; Batchelor, S. Towards Effective e-Governance: The Delivery of Public Services Through Local e-Content; Nokia Siemens Systems: Espoo, Finland, 2009. [Google Scholar]
- Batchelor, S. Changing the Financial Landscape of Africa: An unusual story of evidence-informed innovation, intentional policy influence and private sector engagement. IDS Bull. 2012, 43, 84–90. [Google Scholar] [CrossRef] [Green Version]
- Mahmood, S.S.; Igbal, M.; Hanifi, S.M.A.; Wahed, T.; Bhuiya, A. Are “village doctors” in Bangladesh a curse or a blessing? BMC Int. Health Hum. Rights 2010, 10. [Google Scholar] [CrossRef] [PubMed]
- Katz, J.E. Uses of Internet and Mobile Technology in Health Systems: Organizational and Sociocultural Issues in a Comparative Context; The Network Society and the Knowledge Economy, Portugal in the Global Context: Lisbon, Portugal, 2005. [Google Scholar]
- Malone, M.; While, A.; Roberts, J. Parental health information seeking and re-exploration of the “digital divide”. Prim. Health Care Res. Dev. 2014, 15, 202–212. [Google Scholar] [CrossRef] [PubMed]
- Hertzum, M.; Andersen, H.H.K.; Andersen, V.; Hansen, C.B. Trust in information sources: Seeking information from people, documents, and virtual agents. Interact. Comput. 2002, 14, 575–599. [Google Scholar] [CrossRef]
- Heath, T.; Motta, E. The Hoonoh Ontology for describing Trust Relationships in Information Seeking. In Proceedings of the 7th International Semantic Web Conference, Karlsruhe, Germany; 2008; pp. 2–10. [Google Scholar]
- Lucas, H. A Review of ICT Innovations by Private Sector Providers in Developing Countries. In Health Markets in Developing Countries; Bloom, G., Kanjilal, B., Lucas, H., Peters, D., Eds.; Earthscan: Abingdon, UK, 2012. [Google Scholar]
- Higgins, O.; Sixsmith, J.; Barry, M.M.; Domegan, C. Literature Review on Health Information Seeking Behaviour on the Web: A Health Consumer and Health Professional Perspective; ECDC: Stockholm, Sweden, 2011. [Google Scholar]
- Mintzes, B. Advertising of prescription-only medicines to the public: Does evidence benefit counterbalance harm? Annu. Rev. Public Health 2012, 33, 259–277. [Google Scholar] [CrossRef] [PubMed]
- Boakye, K.; Scott, N.; Smyth, C. Mobiles for Development: A Global Research Study Commissioned by UNICEF; UNICEF: New York, NY, USA, 2010. [Google Scholar]
- Yonazi, E.; Kelly, T.; Halewood, N.; Blackman, C. The Transformational Use of Information and Communication Technologies in Africa; World Bank: Washington, DC, USA, 2012. [Google Scholar]
- Hellström, J. The Innovative Use of Mobile Applications in East Africa; SIDA: Stockholm, Sweden, 2010. [Google Scholar]
- Mechael, P.; Searle, S. Barriers and Gaps Affecting mHealth in Low and Middle Income Countries : Policy White Paper; Center for Global Health and Economic Development Earth Institute, Columbia University: New York, NY, USA, 2010. [Google Scholar]
- Ajzen, I.; Fishbein, M. Understanding Attitudes and Predicting Social Behavior. Englewood Cliffs; Prentice-Hall: Upper Saddle River, NJ, USA, 1980. [Google Scholar]
- Ajzen, I. The theory of planned behavior. Organ. Behave. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Ajzen, I. Constructing a theory of planned behavior questionnaire. (Unpublished manuscript).
- Francis, J.J.; Eccles, M.P.; Johnson, M; Walker, A.E.; Grimshaw, J.M.; Foy, R.; Kaner, E.F.S.; Smith, L.; Bonetti, D. Constructing Questionnaires Based on the Theory of Planned Behavior: A Manual for Health Services Researchers; Centre for Health Services Research, University of Newcastle upon Tyne: Newcastle upon Tyne, UK, 2004; pp. 2–12. [Google Scholar]
- Madden, T.J.; Ellen, P.S.; Ajzen, I. A comparison of the theory of planned behavior and the theory of reasoned action. Personal. Soc. Psychol. Bull. 1992, 18, 3–9. [Google Scholar] [CrossRef]
- Jullisson, E.A.; Karlsson, N.; Garling, T. Weighing the past and the future in decision making. Eur. J. Cogn. Psychol. 2005, 17, 561–575. [Google Scholar] [CrossRef]
- Sagi, A.; Friedland, N. The cost of richness: The effect of the size and diversity of decision sets on post-decision regret. J. Personal. Soc. Psychol. 2007, 93, 515–524. [Google Scholar] [CrossRef] [PubMed]
- Stanovich, K.E.; West, R.F. On the relative independence of thinking biases and cognitive ability. J. Personal. Soc. Psychol. 2008, 94, 672–695. [Google Scholar] [CrossRef] [PubMed]
- De Bruin, W.B.; Parker, A.M.; Fischhoff, B. Individual differences in adult decision-making competence. J. Personal. Soc. Psychol. 2007, 92, 938–956. [Google Scholar] [CrossRef] [PubMed]
- Acevedo, M.; Krueger, J.I. Two egocentric sources of the decision to vote: The voter’s illusion and the belief in personal relevance. Polit. Psychol. 2004, 25, 115–134. [Google Scholar] [CrossRef]
- Dietrich, C. Decision making: factors that influence decision making, heuristics used, and decision outcomes. Stud. Pulse 2010, 2, 1–3. [Google Scholar]
- Buhi, E.R.; Daley, E.M.; Fuhrmann, H.J.; Smith, S.A. An observational study of how young people search for online sexual health information. J. Amer. Coll. Health 2009, 58, 101–111. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Batchelor, S.; Waldman, L.; Bloom, G.; Rasheed, S.; Scott, N.; Ahmed, T.; Khan, N.U.Z.; Sharmin, T. Understanding Health Information Seeking from an Actor-Centric Perspective. Int. J. Environ. Res. Public Health 2015, 12, 8103-8124. https://doi.org/10.3390/ijerph120708103
Batchelor S, Waldman L, Bloom G, Rasheed S, Scott N, Ahmed T, Khan NUZ, Sharmin T. Understanding Health Information Seeking from an Actor-Centric Perspective. International Journal of Environmental Research and Public Health. 2015; 12(7):8103-8124. https://doi.org/10.3390/ijerph120708103
Chicago/Turabian StyleBatchelor, Simon, Linda Waldman, Gerry Bloom, Sabrina Rasheed, Nigel Scott, Tanvir Ahmed, Nazib Uz Zaman Khan, and Tamanna Sharmin. 2015. "Understanding Health Information Seeking from an Actor-Centric Perspective" International Journal of Environmental Research and Public Health 12, no. 7: 8103-8124. https://doi.org/10.3390/ijerph120708103