
Waist Circumferences of Chilean Students: Comparison of the CDC-2012 Standard and Proposed Percentile Curves

Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Procedures
2.3. Statistical Analysis
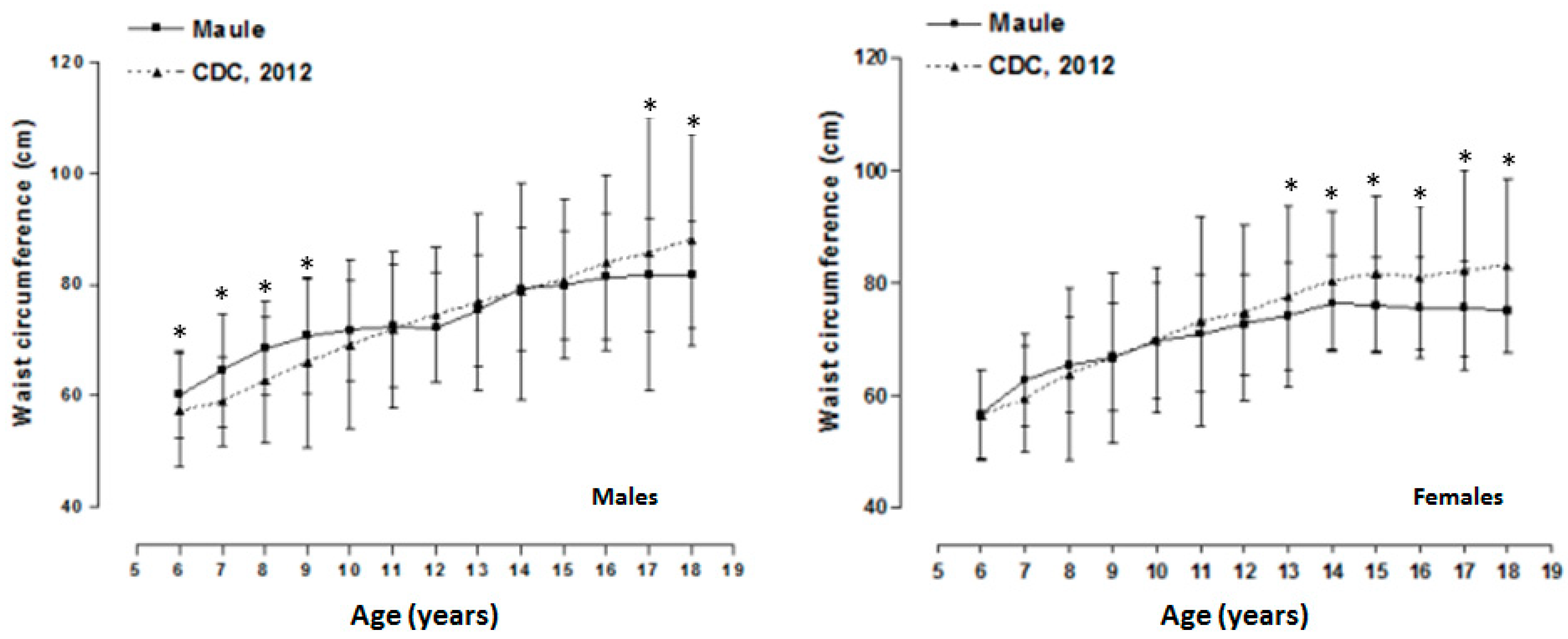
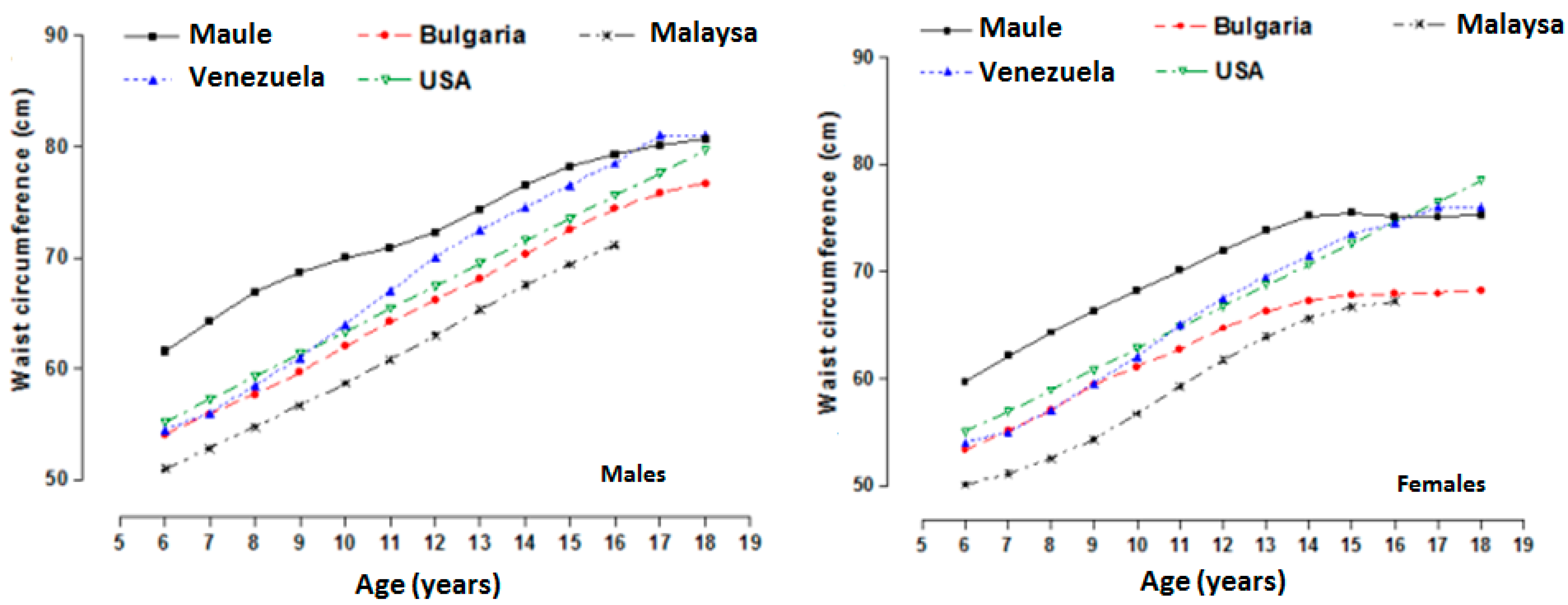
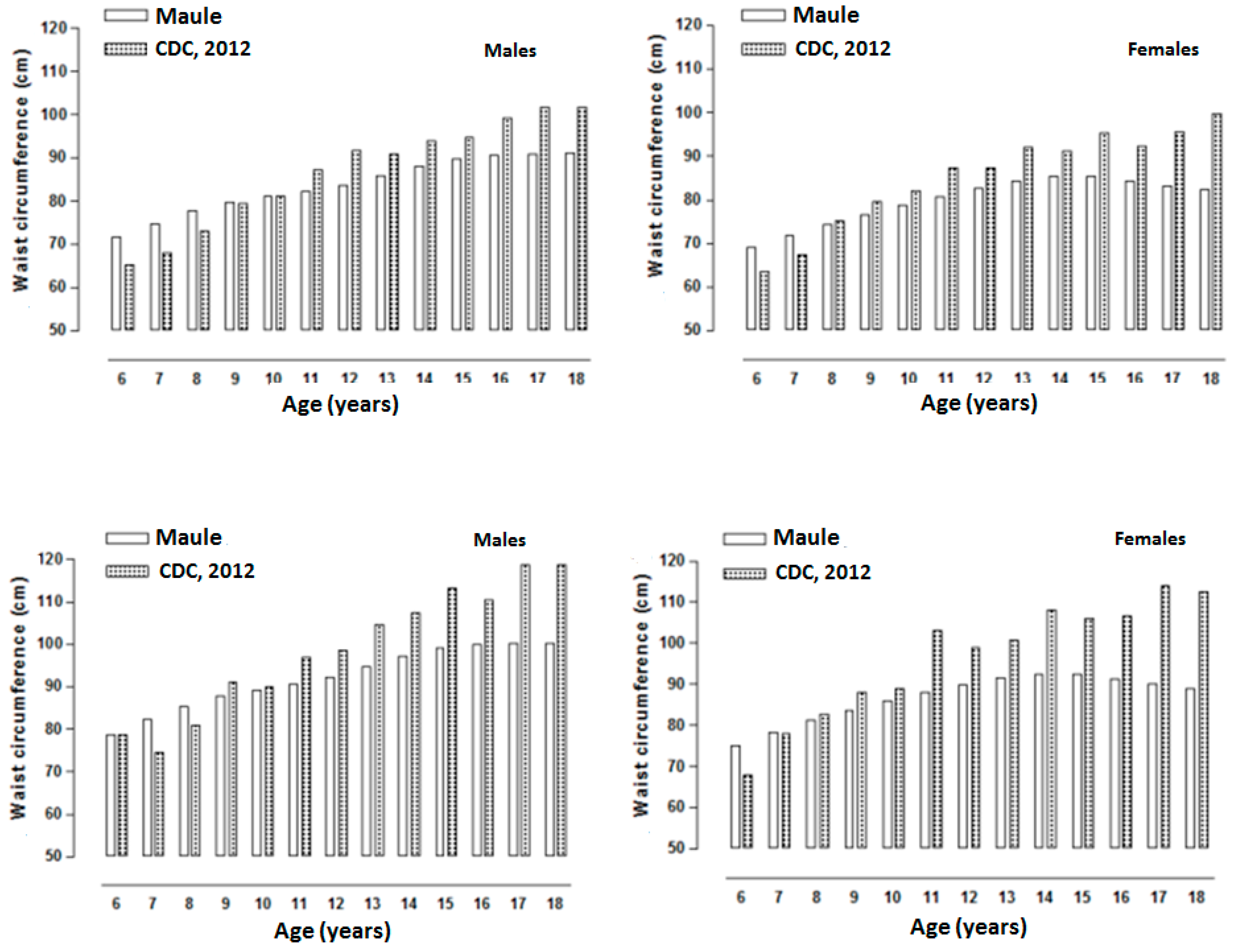
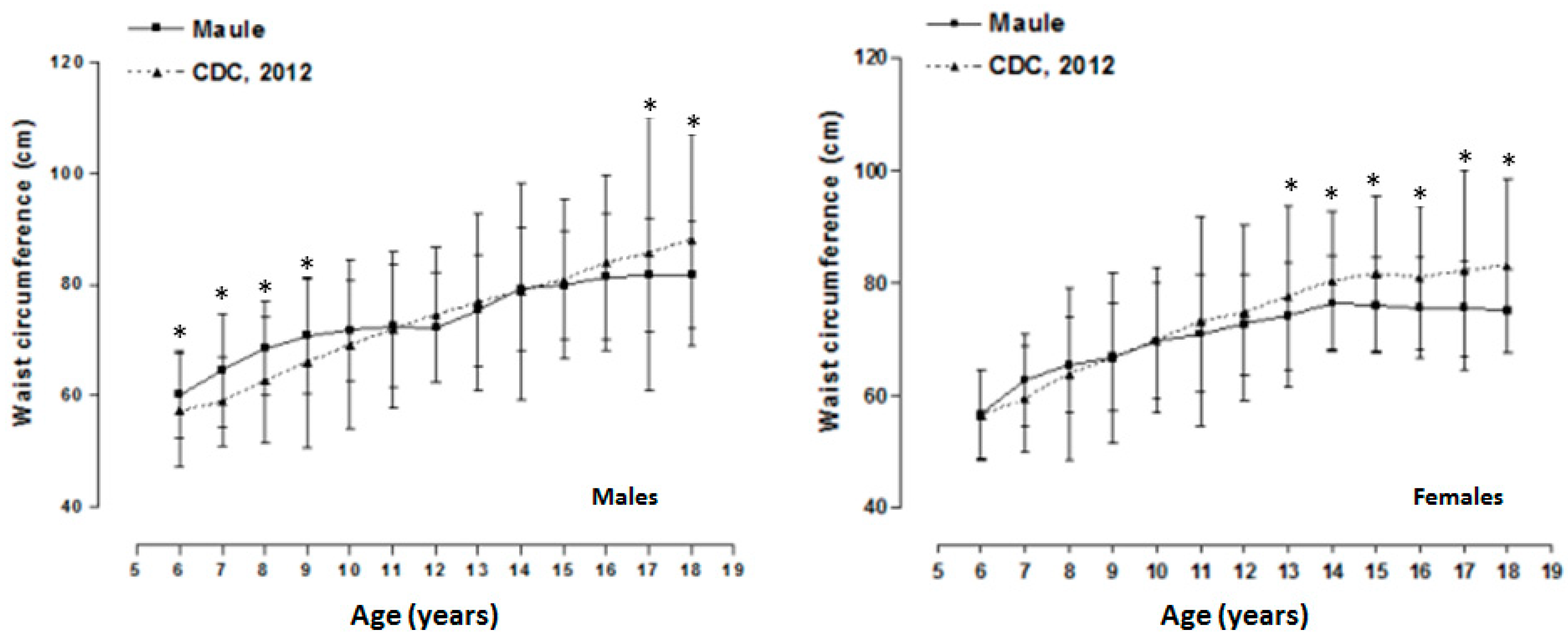
3. Results

{kind=link}
{kind=link}
{kind=link}
| Age (years) | n | Weight (kg) | Height (cm) | Waist Circumference (cm) | BMI (kg/m2) | ||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||
| Males | |||||||||
| 6 | 78 | 26.8 | 7.0 | 123.5 | 6.1 | 60.2 | 7.8 | 17.4 | 3.5 |
| 7 | 73 | 30.1 | 7.5 | 126.7 | 7.3 | 64.6 | 10.2 | 18.6 | 3.8 |
| 8 | 95 | 36.4 | 8.0 | 133.1 | 6.8 | 68.5 | 8.4 | 20.1 | 3.2 |
| 9 | 107 | 38.0 | 8.8 | 136,1 | 9.4 | 70.8 | 10.3 | 19.9 | 3.6 |
| 10 | 108 | 42.0 | 9.1 | 132.7 | 14.8 | 71.7 | 9.0 | 20.5 | 3.3 |
| 11 | 136 | 48.4 | 10.9 | 144.2 | 17.8 | 72.5 | 11.0 | 21.4 | 3.6 |
| 12 | 193 | 52.3 | 10.5 | 156.7 | 11.0 | 72.3 | 9.9 | 21.4 | 3 |
| 13 | 284 | 57.1 | 11.3 | 161.5 | 8.7 | 75.4 | 10.0 | 21.9 | 3.4 |
| 14 | 284 | 63.2 | 13.7 | 167.5 | 7.2 | 79.2 | 11.0 | 22.5 | 4.2 |
| 15 | 260 | 65.0 | 12.0 | 169.5 | 12.6 | 79.9 | 9.7 | 22.5 | 3.5 |
| 16 | 205 | 68.7 | 13.6 | 171.3 | 6.0 | 81.4 | 11.4 | 23.4 | 4.4 |
| 17 | 187 | 70.1 | 12.4 | 172.5 | 5.9 | 81.7 | 10.1 | 23.5 | 3.8 |
| 18 | 82 | 71.9 | 13.6 | 172.3 | 7.4 | 81.7 | 9.6 | 24.2 | 4.2 |
| Females | |||||||||
| 6 | 81 | 26.0 | 5.7 | 123.2 | 7.9 | 56.7 | 7.8 * | 17.1 | 2.9 |
| 7 | 85 | 30.1 | 6.9 | 126.7 | 7.0 | 62.8 | 8.1 * | 18.6 | 2.7 |
| 8 | 90 | 31.8 | 7.2 | 128.5 | 6.1 | 65.4 | 8.5 * | 19.1 | 3.2 |
| 9 | 97 | 36.7 | 9.2 | 137.5 | 8.0 | 66.8 | 9.6 * | 19.3 | 3.8 |
| 10 | 94 | 42.5 | 9.9 | 142.7 | 7.8 | 69.6 | 10.3 | 20.7 | 3.6 |
| 11 | 108 | 47.4 | 10.8 | 149.4 | 7.4 | 71.0 | 10.5 | 21 | 3.6 |
| 12 | 128 | 53.2 | 13.0 | 154.5 | 6.4 | 72.6 | 8.9 | 22.3 | 5.6 |
| 13 | 164 | 55.6 | 9.8 | 155.9 | 6.0 | 74.2 | 9.5 | 22.8 | 3.6 |
| 14 | 241 | 57.8 | 9.3 | 157.0 | 6.3 | 76.4 | 8.4 | 23.5 | 3.7 |
| 15 | 204 | 57.6 | 9.9 | 157.4 | 5.1 | 76.0 | 8.5 * | 23.2 | 3.6 |
| 16 | 244 | 59.9 | 10.7 | 159.1 | 5.5 | 75.6 | 8.8 * | 23.6 | 3.8 |
| 17 | 171 | 59.4 | 10.3 | 159.1 | 6.3 | 75.6 | 8.5 * | 23.4 | 3.6 |
| 18 | 93 | 60.1 | 9.6 | 160.1 | 6.0 | 75.6 | 7.5 * | 23.4 | 3.5 |
| Age (years) | L | M | S | P5 | P10 | P15 | P25 | P50 | P75 | P85 | P90 | P95 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Males | ||||||||||||
| 6 | −0.52439 | 6.155.318 | 0.140661 | 49.4 | 51.8 | 53.5 | 56.1 | 61.6 | 67.8 | 71.6 | 74.4 | 78.8 |
| 7 | −0.55103 | 6.434.286 | 0.139546 | 51.8 | 54.3 | 56.0 | 58.7 | 64.3 | 70.9 | 74.8 | 77.7 | 82.2 |
| 8 | −0.58833 | 6.685.606 | 0.138349 | 54.0 | 56.5 | 58.3 | 61.1 | 66.9 | 73.6 | 77.7 | 80.6 | 85.4 |
| 9 | −0.65335 | 6.872.915 | 0.137032 | 55.7 | 58.2 | 60.0 | 62.8 | 68.7 | 75.6 | 79.8 | 82.8 | 87.7 |
| 10 | −0.75198 | 6.997.597 | 0.135455 | 57.0 | 59.4 | 61.3 | 64.1 | 70.0 | 76.9 | 81.2 | 84.3 | 89.3 |
| 11 | −0.87856 | 7.094.686 | 0.1335 | 58.1 | 60.5 | 62.3 | 65.1 | 70.9 | 77.9 | 82.2 | 85.4 | 90.5 |
| 12 | −102.779 | 7.225.754 | 0.130902 | 59.5 | 61.9 | 63.6 | 66.4 | 72.3 | 79.3 | 83.6 | 86.9 | 92.2 |
| 13 | −119.085 | 7.428.609 | 0.127672 | 61.6 | 64.0 | 65.7 | 68.4 | 74.3 | 81.4 | 85.8 | 89.1 | 94.6 |
| 14 | −137.599 | 7.651.446 | 0.123782 | 64.0 | 66.3 | 68.0 | 70.7 | 76.5 | 83.6 | 88.1 | 91.5 | 97.2 |
| 15 | −161.832 | 782.086 | 0.118974 | 66.0 | 68.2 | 69.9 | 72.5 | 78.2 | 85.2 | 89.7 | 93.2 | 99.0 |
| 16 | −194.069 | 7.933.414 | 0.113281 | 67.6 | 69.8 | 71.4 | 73.9 | 79.3 | 86.2 | 90.6 | 94.1 | 100.0 |
| 17 | −229.912 | 8.010.295 | 0.106921 | 68.9 | 71.1 | 72.4 | 74.9 | 80.1 | 86.7 | 91.0 | 94.4 | 100.3 |
| 18 | −266.586 | 8.068.186 | 0.100333 | 69.8 | 72.2 | 73.1 | 75.8 | 80.7 | 86.9 | 91.1 | 94.4 | 100.3 |
| Females | ||||||||||||
| 6 | 0.11684 | 5.968.906 | 0.14066 | 47.2 | 49.7 | 51.6 | 54.3 | 59.7 | 65.6 | 69.0 | 71.3 | 75.0 |
| 7 | −0.06848 | 6.214.301 | 0.13893 | 49.5 | 52.1 | 53.9 | 56.6 | 62.1 | 68.3 | 71.8 | 74.3 | 78.2 |
| 8 | −0.24588 | 6.434.521 | 0.1372 | 51.6 | 54.2 | 55.9 | 58.7 | 64.3 | 70.7 | 74.4 | 77.0 | 81.2 |
| 9 | −0.39868 | 6.631.717 | 0.1353 | 53.5 | 56.1 | 57.8 | 60.6 | 66.3 | 72.8 | 76.6 | 79.4 | 83.7 |
| 10 | −0.509 | 6.820.444 | 0.13291 | 55.4 | 57.9 | 59.6 | 62.5 | 68.2 | 74.8 | 78.7 | 81.5 | 86.0 |
| 11 | −0.57003 | 7.007.619 | 0.12978 | 57.2 | 59.8 | 61.4 | 64.3 | 70.1 | 76.7 | 80.6 | 83.5 | 88.0 |
| 12 | −0.59462 | 7.198.154 | 0.12588 | 59.2 | 61.7 | 63.3 | 66.3 | 72.0 | 78.5 | 82.5 | 85.3 | 89.8 |
| 13 | −0.63148 | 7.381.331 | 0.12145 | 61.3 | 63.6 | 65.4 | 68.1 | 73.8 | 80.3 | 84.2 | 87.0 | 91.4 |
| 14 | −0.73154 | 7.519.916 | 0.11669 | 63.2 | 65.2 | 67.2 | 69.7 | 75.2 | 81.5 | 85.4 | 88.1 | 92.5 |
| 15 | −0.92937 | 754.787 | 0.11197 | 64.1 | 66.0 | 68.0 | 70.2 | 75.5 | 81.6 | 85.3 | 88.0 | 92.4 |
| 16 | −121.427 | 7.512.015 | 0.10724 | 64.1 | 65.9 | 67.7 | 69.8 | 75.1 | 80.7 | 84.3 | 87.0 | 91.2 |
| 17 | −153.789 | 7.503.616 | 0.10231 | 63.8 | 65.7 | 67.2 | 69.3 | 75.1 | 79.6 | 83.1 | 85.7 | 90.0 |
| 18 | −187.113 | 753.231 | 0.09716 | 63.6 | 65.7 | 66.7 | 69.1 | 75.3 | 78.9 | 82.2 | 84.7 | 88.9 |
4. Discussion
5. Conclusions
Acknowledgements
Author Contributions
Conflicts of Interest
References
- Moreno, L.A.; Fleta, J.; Mur, L.; Rodriguez, A.; Sarría, A.; Bueno, M. Waist circumference values in Spanish children-gender related differences. Eur. J. Clin. Nutr. 1999, 53, 429–433. [Google Scholar] [CrossRef]
- Galcheva, S.V.; Iotova, V.M.; Yotov, Y.T.; Grozdeva, K.P.; Stratev, V.K.; Tzaneva, V.I. Waist circumference percentile curves for Bulgarian children and adolescents aged 6–18 years. Int. J. Pediatr. Obes. 2009, 4, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Engeland, A.; Bjorge, T.; Sogaard, A.J.; Tverdal, A. Body mass index in adolescence in relation to total mortality: 32-year follow-up of 227,000 Norwegian boys and girls. Am. J. Epidemiol. 2003, 157, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.W.; Jones, I.E.; Williams, S.M.; Aage, T. Evaluation of waist circumference, waist-to-hip ratio, and the conicity index as screening tools for high trunk fat mass, as measured by dual energy X-ray absorptiometry, in children aged 3–19 y. Am. J. Clin. Nutr. 2000, 72, 490–495. [Google Scholar]
- Lee, S.; Bacha, F.; Gungor, N.; Arslanian, S.A. Waist circumference is an independent predictor of insulin resistance in black and white youths. J. Pediatr. 2006, 148, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Wajchenberg, B.L. Subcutaneous and visceral tissue: Their relation to the metabolic syndrome. Endocr. Rev. 2000, 21, 697–738. [Google Scholar] [CrossRef] [PubMed]
- Maffeis, C.; Pietrobelli, A.; Grezzani, A.; Provera, S.; Tatò, L. Waist circumference and cardiovascular risk factors in prepubertal children. Obes. Res. 2001, 9, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Bitsori, M.; Linardakis, M.; Tabakaki, M.; Kafatos, A. Waist circumference as a screening tool for the identification of adolescents with the metabolic syndrome phenotype. Int. J. Pediatr. Obes. 2009, 4, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Bauer, K.W.; Marcus, M.D.; El Ghormli, L.; Ogden, C.L.; Foster, G.D. Cardio-metabolic risk screening among adolescents: Understanding the utility of body mass index, waist circumference and waist to height ratio. Pediatr. Obes. 2014, 17. [Google Scholar] [CrossRef] [PubMed]
- Avalos, F.C.; Díaz, C.; Martínez, A.; Bancalari, D.R.; Zamorano, R.J.; Harbin, A.F.; Cerda, E.V.; Fernández, F.V.; Cavada, C.G.; Arteaga, R.J.; et al. Waist circumference percentiles in children and adolescents between 6 and 14 years from Santiago, Chile. Endocrinol. Nutr. 2012, 59, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Wei, M.; Gaskill, S.P.; Haffner, S.M.; Stern, M.P. Waist circumference as the best predictor of non-insulin dependent diabetes mellitus (NIDDM) compared to body mass index, waist/hip ratio and other anthropometric measurements in Mexican Americans/a 7-year prospective study. Obes. Res. 1997, 5, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Programa Nacional de Salud Integral de Adolescentes y Jóvenes (PNSIAJ). Orientaciones técnicas para el control de salud integral de adolescentes; Ministerio de Salud: Santiago de Chile, Noviembre 2013. [Google Scholar]
- Kuczmarski, R.J.; Ogden, C.L.; Grummer-Strawn, L.M.; Flegal, K.M.; Guo, S.S.; Wei, R.; Mei, Z.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. CDC growth charts: United States; Department of Health and Human Services: Hyattsville, Maryland, MD, USA, 2000. [Google Scholar]
- Fernández, J.R.; Redden, D.T.; Pietrobelli, A.; Allison, D.B. Waist circumference percentiles in nationally representative samples of African-American, European-American, and Mexican-American children and adolescents. J. Pediatr. 2004, 145, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Fryar, C.D.; Gu, Q.; Ogden, C.L. Anthropometric reference data for children and adults: United States, 2007–2010. Vital Health Stat. 2012, 11, 1–48. [Google Scholar]
- Programa de las Naciones Unidas para el Desarrollo (PNUD). Informe Sobre Desarrollo Humano 2010; Edición del vigésimo aniversario: Nueva York, NY, Estados Unidos, 2010. [Google Scholar]
- Ross, W.D.; Marfell-Jones, M.J. Kinanthropometry. In Physiological Testing of Elite Athlete; MacDougall, J.D., Wenger, H.A., Geeny, H.J., Eds.; Human Kinetics: London, NY, USA, 1991; pp. 223–308. [Google Scholar]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ. 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [PubMed]
- LMS Chartmaker. Available online: http://www.healthforallchildren.co.uk (accessed on 11 March 2012).
- Poh, B.K.; Jannah, A.N.; Chong, L.K.; Ruzita, A.T.; Ismail, M.N.; Mccarthy, D. Waist circumference percentile curves for Malaysian children and adolescents aged 6.0–16.9 years. Int. J. Pediatr. Obes. 2011, 6, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Vargas, M.E.; Souki, A.; Ruiz, G.; García, D.; Mengual, E.; González, C.C.; Chavez, M.; González, L. Percentiles de circunferencia de cintura en niños y adolescentes del municipio Maracaibo del Estado Zulia, Venezuela. An. Venez. Nutr. 2011, 24, 13–20. [Google Scholar]
- Hatipoglu, N.; Ozturk, A.; Mazicioglu, M.; Kurtoglu, S.; Seyhan, S.; Lokoglu, F. Waist circumference percentiles for 7- to 17-year-old Turkish children and adolescents. Eur. J. Pediatr. 2008, 167, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Thornton, J.C.; Bari, S.; Williamson, B.; Gallagher, D.; Heymsfield, S.B.; Horlick, M.; Kotler, D.; Laferrere, B.; Mayer, L.; Pi-Sunyer, F.X.; Pierson, R.N. Comparisons of waist circumferences measured at 4 sites. Am. J. Clin. Nutr. 2003, 77, 379–384. [Google Scholar] [PubMed]
- Zanetti Passos, M.A.; de Pádua Cintra, I.; de Moraes Ferrari, G.L.; de Almeida, E.C.; Fisberg, M. Percentiles of body circumferences and cutoff points regarding the obesity of adolescents from são paulo-brazil. Ann. Pediatr. Child Health 2014, 2, 1018. [Google Scholar]
- Ostrowska-Nawarycz, L.; Krzyz, A.; Stawinska-Witoszynska, B.; Krzywinska-Wiewiorowska, M.; Szilagyi-Pagowska, I.; Kowalska, M.; Krzych, L.; Nawarycz, T. Percentile distributions of waist circumference for 7–19-year-old Polish children and adolescents. Obes. Rev. 2010, 11, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Goran, M.I.; Nagy, T.R.; Treuth, M.S. Visceral fat in white and African American prepubertal children. Am. J. Clin. Nutr. 1997, 65, 1703–1708. [Google Scholar] [PubMed]
- Sardinha, L.B.; Santos, R.; Vale, S.; Coelhoe Silva, M.J.; Raimundo, A.M.; Moreira, H.; Baptista, F.; Mota, J. Waist circumference percentiles for Portuguese children and adolescents aged 10 to 18 years. Eur. J. Pediatr. 2012, 171, 499–505. [Google Scholar] [CrossRef] [PubMed]
- Kuczmarski, R.J.; Ogden, C.L.; Guo, S.S.; Grummer-Strawn, L.M.; Flegal, K.M.; Mei, Z.; Wei, R.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. 2000 CDC Growth Charts for the United States: methods and development. Vital Health Stat. 2002, 11, 1–190. [Google Scholar]
- Kułaga, Z.; Litwin, M.; Tkaczyk, M.; Palczewska, I.; Zaja˛czkowska, M.; Zwolinska, D.; Krynicki, T.; Wasilewska, A.; Moczulska, A.; Morawiec-Knysak, A.; et al. Polish 2010 growth references for school-aged children and adolescents. Eur. J. Pediatr. 2011, 170, 599–609. [Google Scholar] [CrossRef] [PubMed]
- Brannsether, B.; Roelants, M.; Bjerknes, R.; Júlíusson, P.B. Waist circumference and waist-to-height ratio in Norwegian children 4–18 years of age: Reference values and cut-off levels. Acta. Paediatr. 2011, 100, 1576–1582. [Google Scholar] [CrossRef] [PubMed]
- Moreno, L.A.; Pineda, I.; Rodriguez, G.; Fleta, J.; Sarria, A.; Bueno, M. Waist circumference for the screening of the metabolic syndrome in children. Acta. Paediatr. 2002, 91, 1307–1312. [Google Scholar] [CrossRef] [PubMed]
- Katzmarzyk, P.T. Waist circumference percentiles for Canadian youth 11–18 y of age. Eur. J. Clin. Nutr. 2004, 58, 1011–1015. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez-Campos, R.; Andruske, C.L.; Hespanhol, J.; Torres, J.S.; Arruda, M.; Luarte-Rocha, C.; Cossio-Bolaños, M.A. Waist Circumferences of Chilean Students: Comparison of the CDC-2012 Standard and Proposed Percentile Curves. Int. J. Environ. Res. Public Health 2015, 12, 7712-7724. https://doi.org/10.3390/ijerph120707712
Gómez-Campos R, Andruske CL, Hespanhol J, Torres JS, Arruda M, Luarte-Rocha C, Cossio-Bolaños MA. Waist Circumferences of Chilean Students: Comparison of the CDC-2012 Standard and Proposed Percentile Curves. International Journal of Environmental Research and Public Health. 2015; 12(7):7712-7724. https://doi.org/10.3390/ijerph120707712
Chicago/Turabian StyleGómez-Campos, Rossana, Cinthya Lee Andruske, Jefferson Hespanhol, Jose Sulla Torres, Miguel Arruda, Cristian Luarte-Rocha, and Marco Antonio Cossio-Bolaños. 2015. "Waist Circumferences of Chilean Students: Comparison of the CDC-2012 Standard and Proposed Percentile Curves" International Journal of Environmental Research and Public Health 12, no. 7: 7712-7724. https://doi.org/10.3390/ijerph120707712