
A Concurrent Exposure to Arsenic and Fluoride from Drinking Water in Chihuahua, Mexico

 ,
,
Abstract
:1. Introduction
2. Experimental Section
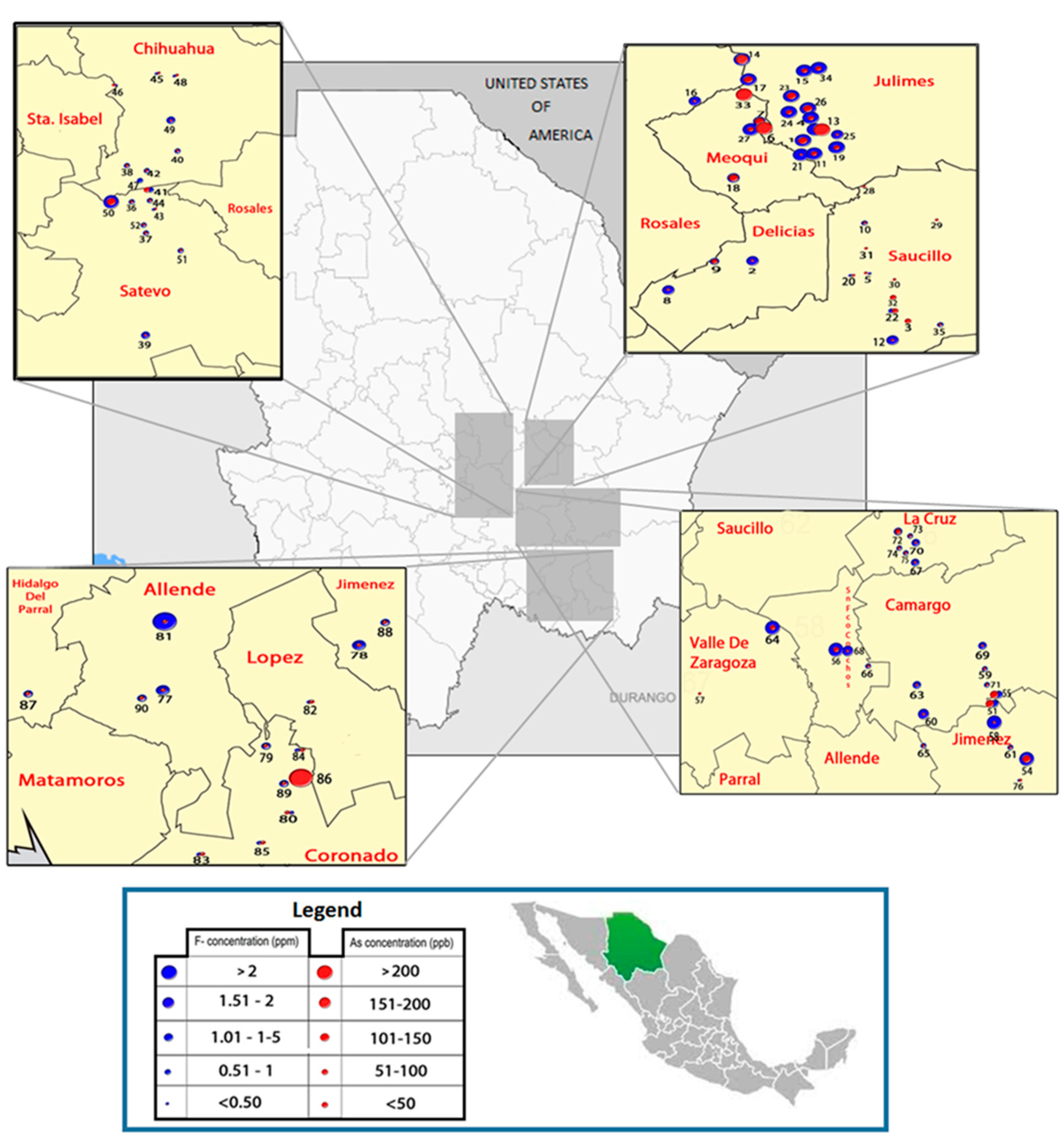
2.1. Study Area
2.2. Study Participants
2.3. Tube Well Water Sample Collection
2.4. Drinking Water and Urine Collection
2.5. Determination of Arsenic and Fluoride Concentrations in Water
2.6. Analysis of Arsenic in Urine
2.7. Analysis of Fluoride-in Urine
2.8. Statistical Analysis
3. Results and Discussion
3.1. Characteristics of the Study Population

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Alls N (%) | Males N (%) | Females N (%) |
|---|---|---|---|
| Age (years) | |||
| 18–90 | 1119 (100%) | 370 (33.1%) | 749 (66.9%) |
| 18–40 | 457 (40.8%) | 118 (10.5%) | 339 (30.3%) |
| >40–50 | 235 (21.0%) | 64 (5.7%) | 171 (15.3%) |
| >50–65 | 281 (25.1%) | 103 (9.2%) | 178 (15.9%) |
| >65 | 146 (13.1%) | 82 (7.3%) | 64 (5.7%) |
| Arsenic in water (µg/L) | |||
| <10 | 187 (16.7%) | 54 (4.8%) | 133 (11.9%) |
| >10–50 | 401 (35.8%) | 137 (12.2%) | 264 (23.6%) |
| >50–100 | 321 (28.7%) | 106 (9.5%) | 215 (19.2%) |
| >100 | 210 (18.8%) | 73 (6.5%) | 137 (12.2%) |
| Fluoride in water (mg/L) | |||
| <0.5 | 184 (16.4%) | 52 (4.6%) | 132 (11.8%) |
| >0.5–1.5 | 471 (42.1%) | 146 (13.1%) | 325 (29.0%) |
| >1.5–3.0 | 222 (19.8%) | 86 (7.7%) | 136 (12.1%) |
| >3.0 | 242 (21.6%) | 86 (7.7%) | 156 (13.9%) |
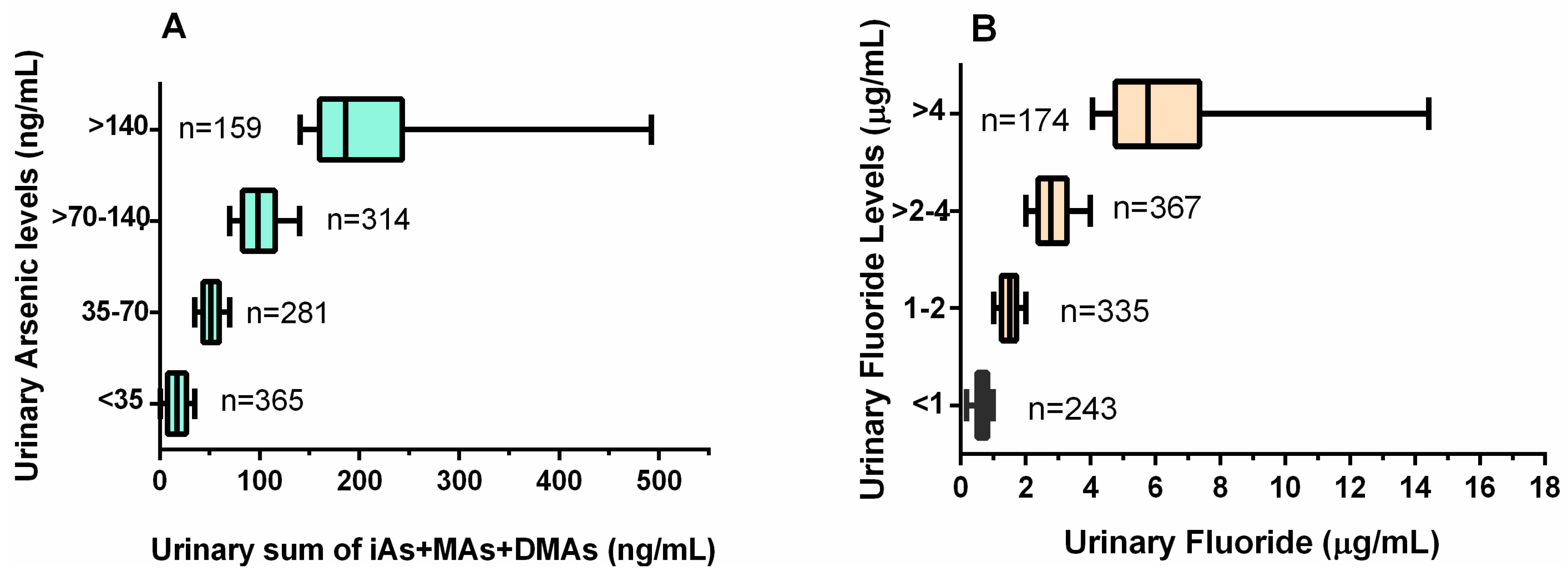
| Urinary Arsenic (ng/mL a) | |||
| <35 | 365 (32.6%) | 92 (8.2%) | 273 (24.4%) |
| 35–70 | 281 (25.1%) | 102 (9.1%) | 179 (16.0% |
| >70–140 | 314 (28.0%) | 117 (10.4%) | 197 (17.6%) |
| >140 | 159 (14.2%) | 59 (5.3%) | 100 (8.9%) |
| Urinary Fluoride (µg/mL a) | |||
| <1 | 243 (21.7%) | 42 (3.7%) | 201 (18.0%) |
| 1–2 | 367 (32.8%) | 100 (8.9%) | 267 (23.9%) |
| >2–4 | 335 (29.9%) | 142 (12.7%) | 193 (17.2% |
| >4 | 174 (15.5%) | 86 (7.7%) | 88 (7.8%) |
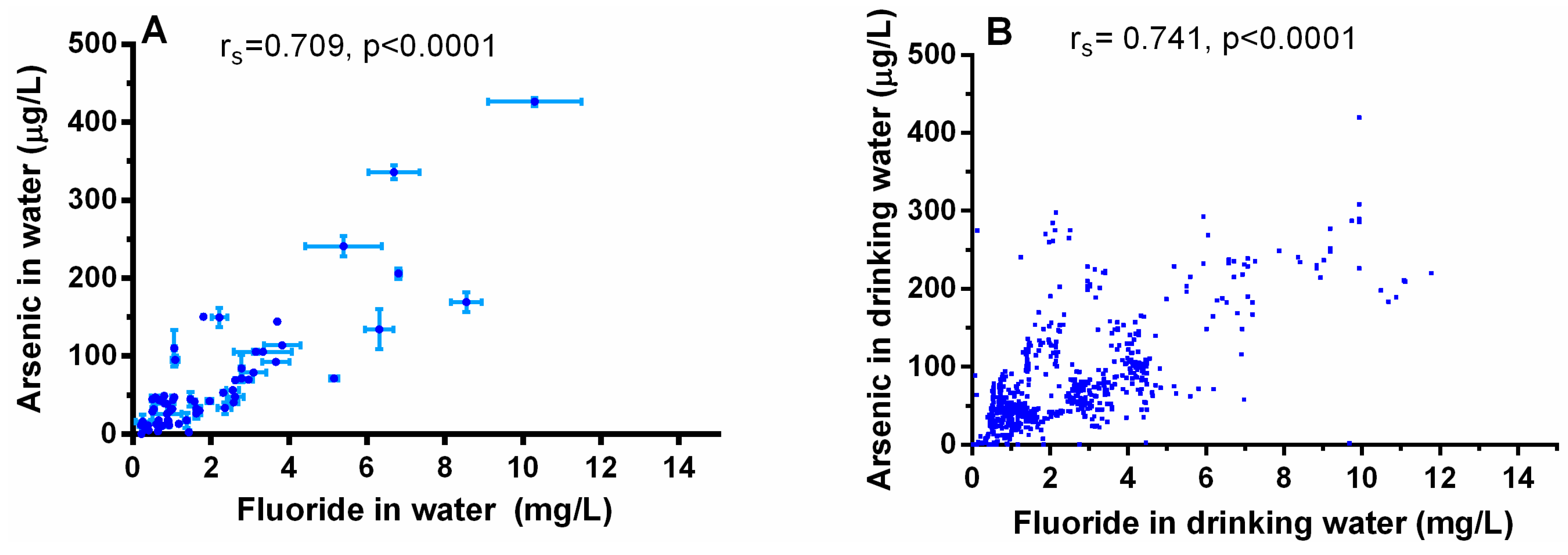
3.2. Co-occurrence of Arsenic and Fluoride in the groundwater
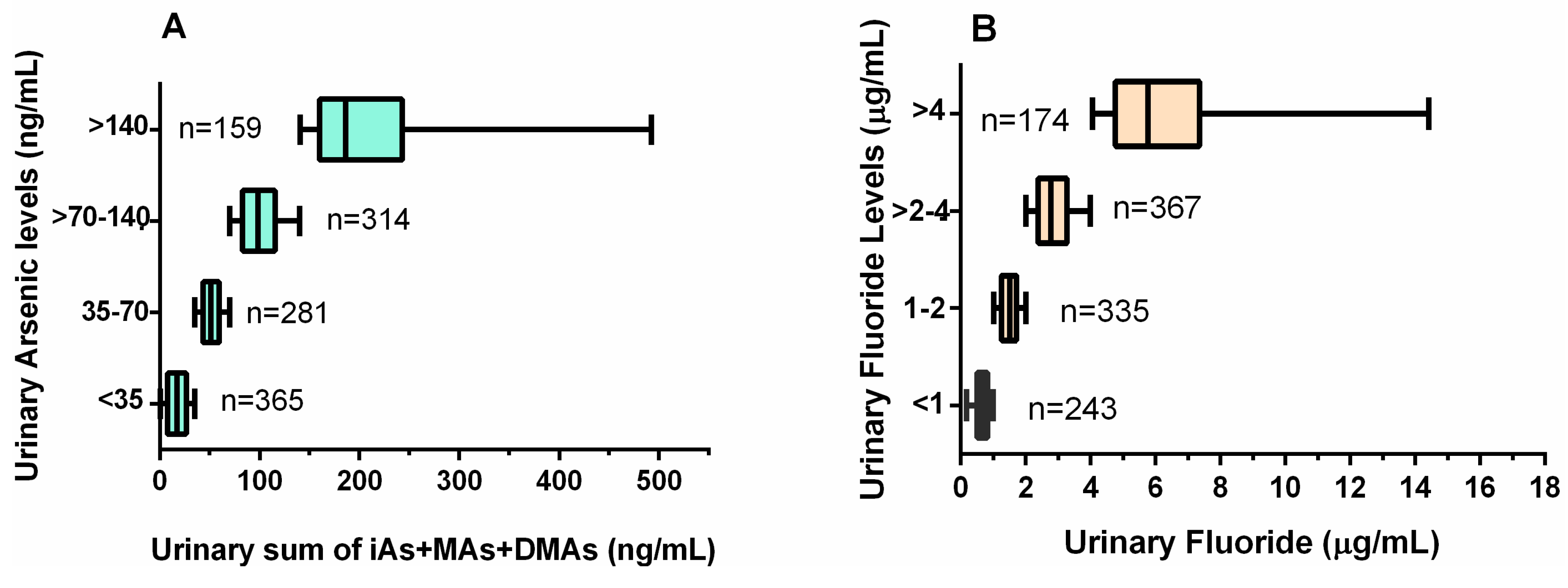
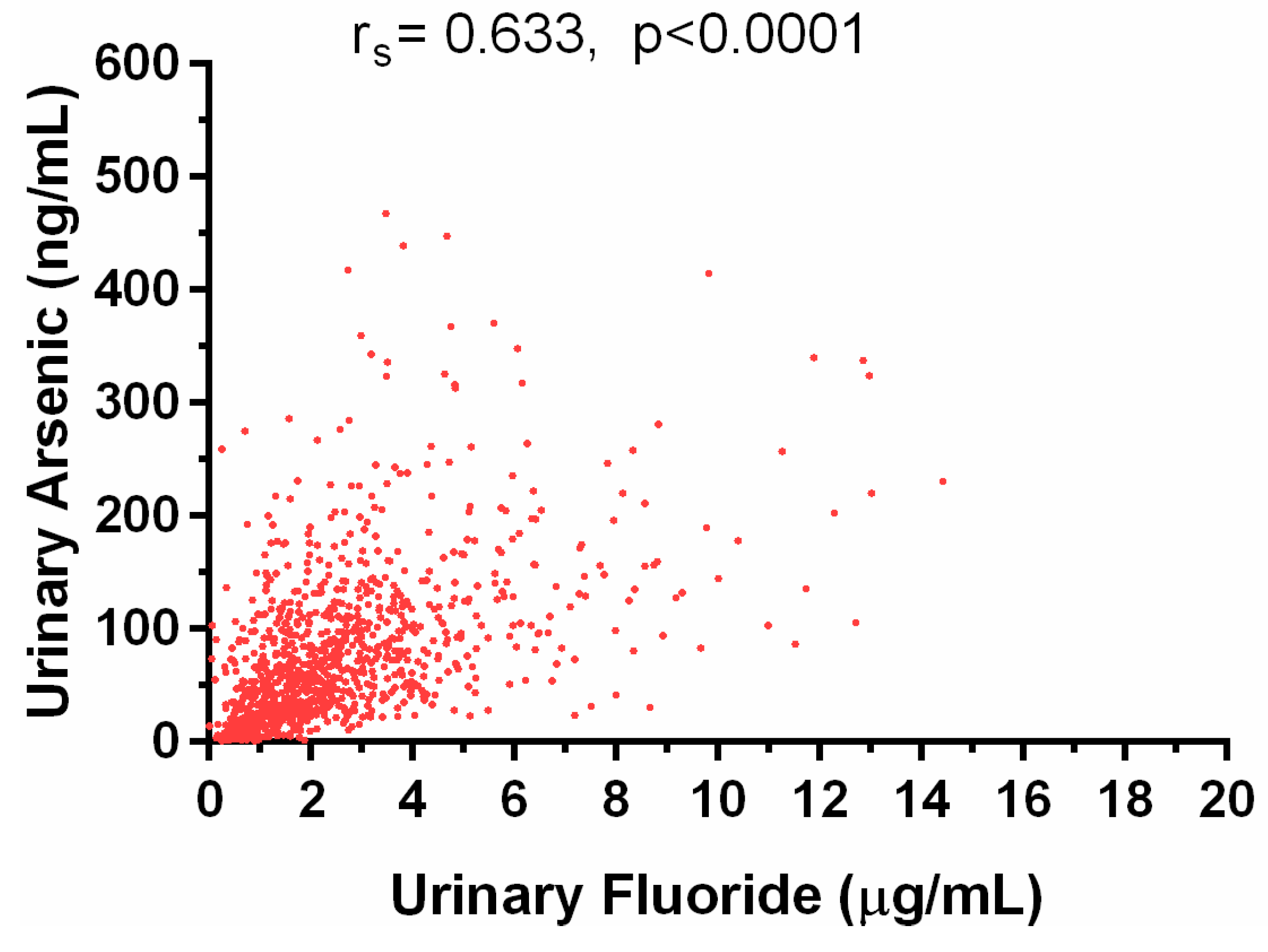
3.3. Co-Occurrence of Arsenic and Fluoride in the Urine
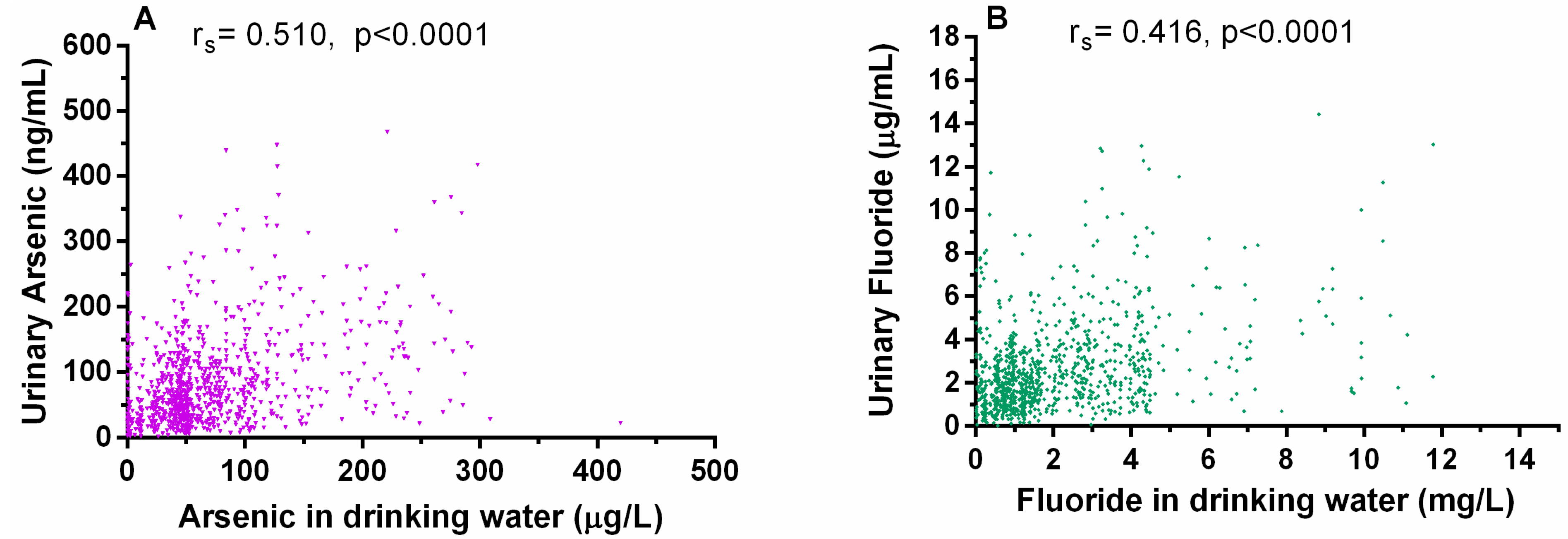
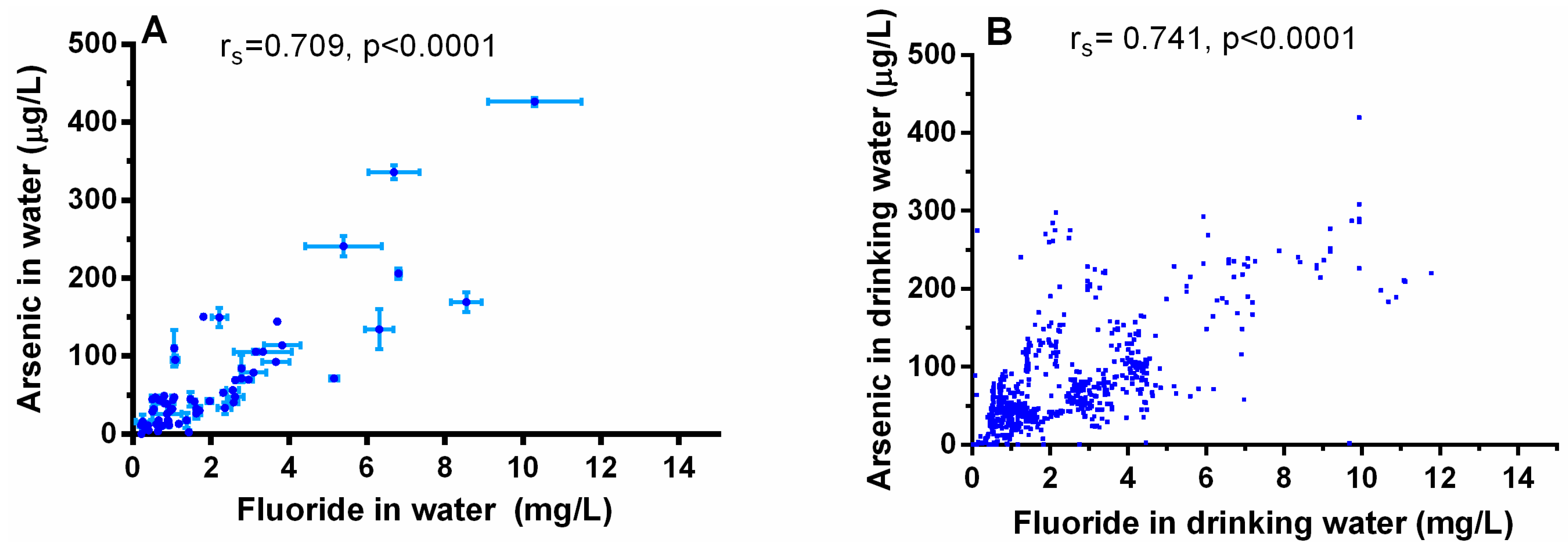
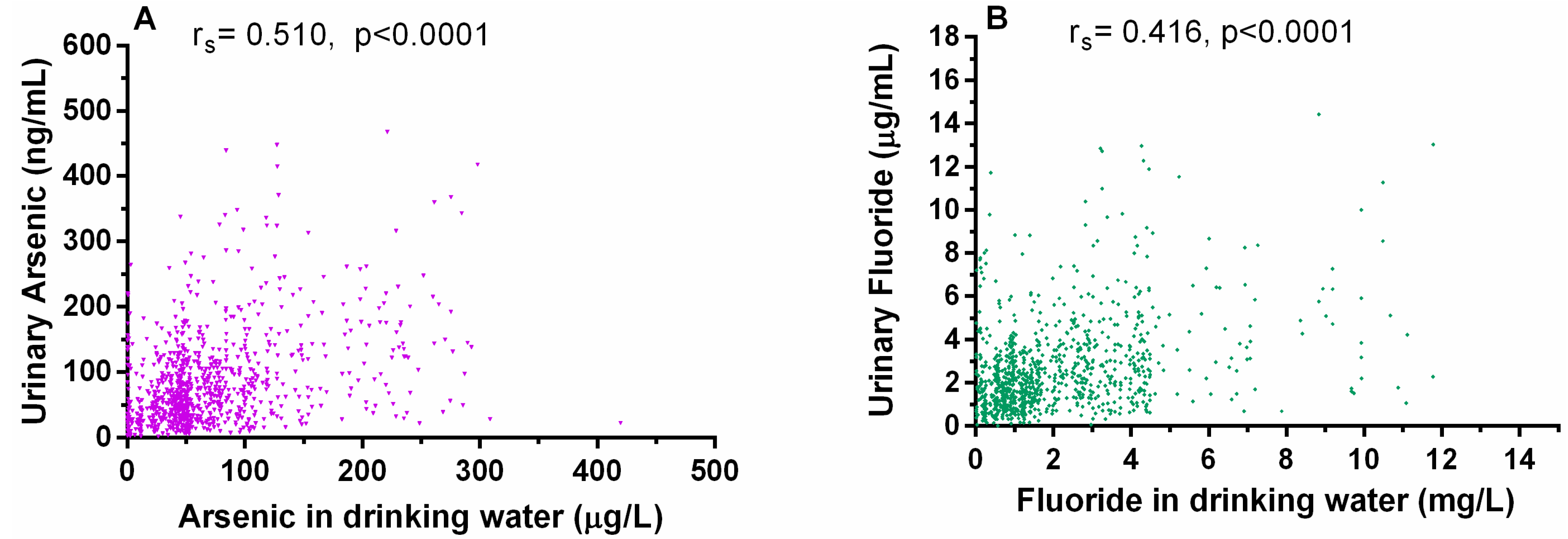
3.4. Relationship between Arsenic and Fluoride Levels in the Water and the Urine
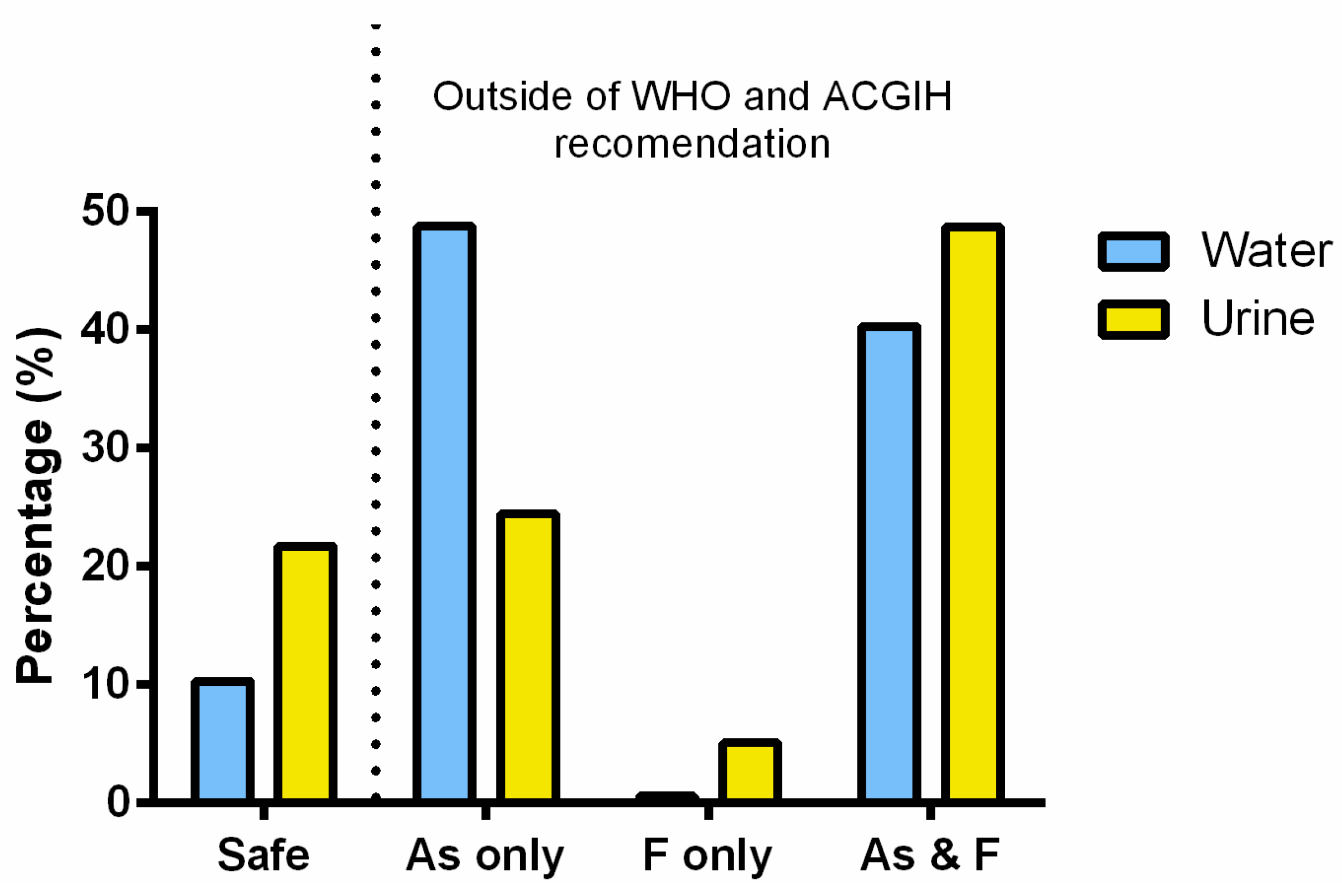
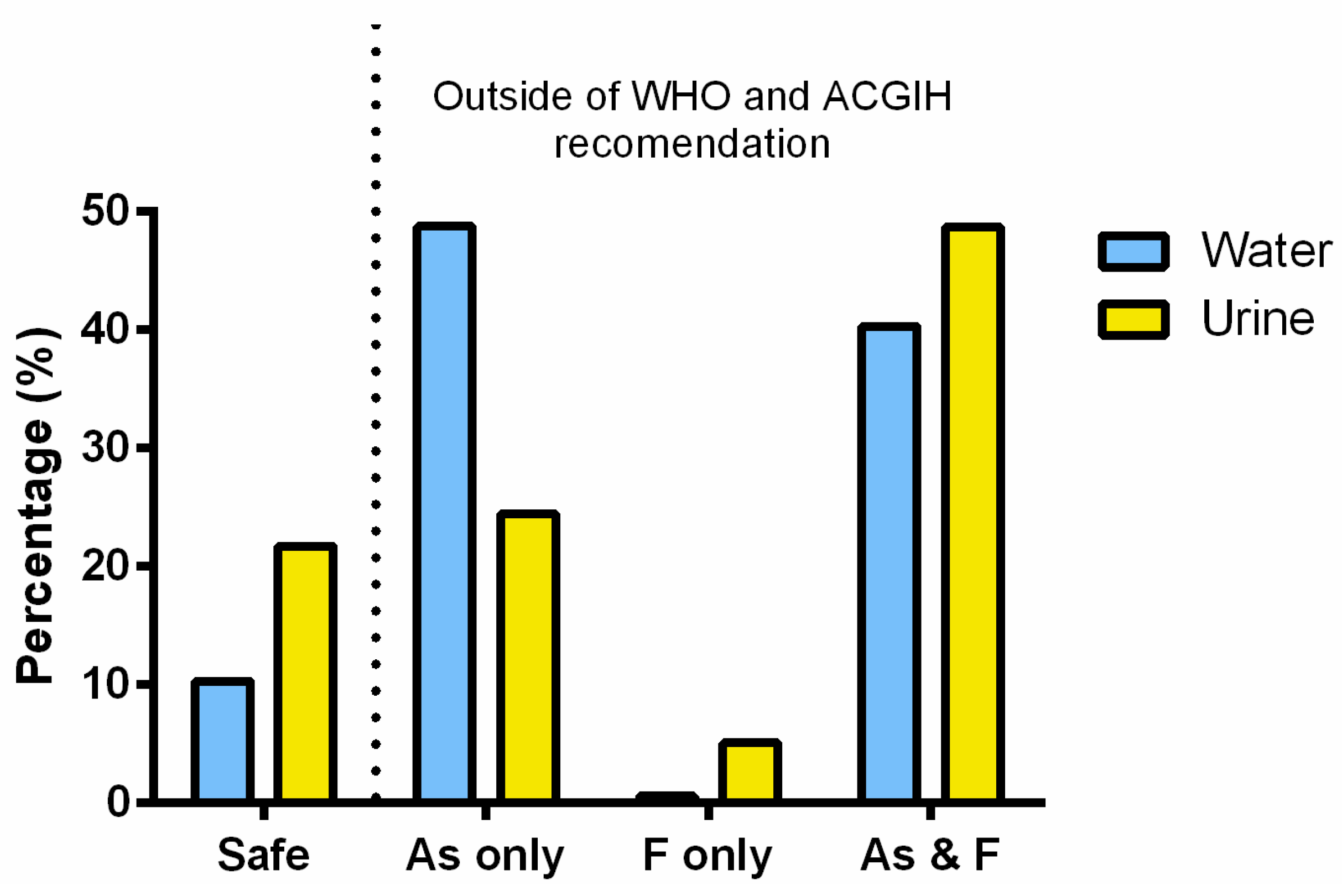
3.5. Risk Associated with the Combined Exposure to Inorganic Arsenic and Fluoride
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Alarcón-Herrera, M.T.; Bundschuh, J.; Nath, B.; Nicolli, H.B.; Gutierrez, M.; Reyes-Gomez, V.M.; Nuñez, D.; Martìn-Dominguez, I.R.; Sracek, O. Co-occurrence of arsenic and fluoride in groundwater of semi-arid regions in Latin America: Genesis, mobility and remediation. J. Hazard. Mater. 2013, 262, 960–969. [Google Scholar] [CrossRef] [PubMed]
- Buchhamer, E.E.; Blanes, P.S.; Osicka, R.M.; Giménez, M.C. Environmental risk assessment of arsenic and fluoride in the Chaco Province, Argentina: Research advances. J. Toxicol. Environ. Health A 2012, 75, 1437–1450. [Google Scholar] [CrossRef] [PubMed]
- Chakraborti, D.; Das, B.; Murrill, M.T. Examining India’s groundwater quality management. Environ. Sci. Technol. 2011, 45, 27–33. [Google Scholar] [CrossRef] [PubMed]
- National Research Council (NRC). Fluoride in Drinking-Water; A Scientific Review of EPA’s Standards; NRC: Washington, DC, USA, 2006. [Google Scholar]
- Mahlangu, O.; Mamba, B.; Momba, M. Efficiency of silver impregnated porous pot (SIPP) filters for production of clean potable water. Int. J. Environ. Res. Public Health 2012, 9, 3014–3029. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Bain, R.; Bartram, J.; Gundry, S.; Pedley, S.; Wright, J. Water safety and inequality in access to drinking-water between rich and poor households. Environ. Sci. Technol. 2013, 47, 1222–1230. [Google Scholar] [PubMed]
- World Health Organization. United Nations Synthesis Report on Arsenic in Drinking Water; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- World Health Organization. Guidelines for Drinking-Water Quality, 1st addendum to Vol. 1, Recommendations, 3rd ed.; World Health Organization: Geneva, Switzerland, 2006; p. 595. [Google Scholar]
- U.S. EPA. EPA and HHS Announce New Scientific Assessments and Actions on Fluoride: Agencies Working together to Maintain Benefits of Preventing Tooth Decay while Preventing Excessive Exposure. Available online: http://yosemite.epa.gov/opa/admpress.nsf/bd4379a92ceceeac85257359 00400c27/86964af577c37ab285257811005a8417!OpenDocument (accessed on 20 January 2013).
- World Health Organization. Fluorides. In Environmental Health Criteria 227; International Programme on Chemical Safety; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- ATSDR, (Agency for Toxic Substances and Disease Registry). Toxicological Profile for Arsenic; U.S. Department of Health and Human Services, Public Health Service: Atlanta, GA, USA, 2007. [Google Scholar]
- IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Available online: http://monographs.iarc.fr/ENG/Monographs/vol84/mono84.pdf (accessed on 14 February 2015).
- Moon, K.; Guallar, E.; Navas-Acien, A. Arsenic exposure and cardiovascular disease: An updated systematic review. Curr. Atheroscler. Rep. 2012, 14, 542–555. [Google Scholar] [CrossRef] [PubMed]
- Maull, E.A.; Ahsan, H.; Edwards, J.; Longnecker, M.P.; Navas-Acien, A.; Pi, J.; Silbergeld, E.K.; Styblo, M.; Tseng, C.H.; Thayer, K.A.; et al. Evaluation of the association between arsenic and diabetes: A national toxicology program workshop review. Environ. Health Perspect. 2012, 120, 1658–1670. [Google Scholar] [PubMed]
- Tyler, C.R.; Allan, A.M. The effects of arsenic exposure on neurological and cognitive dysfunction in human and rodent studies: A Review. Curr. Environ. Health Rep. 2014, 1, 132–147. [Google Scholar] [CrossRef] [PubMed]
- Barbier, O.; Arreola-Mendoza, L.; Del Razo, L.M. Molecular mechanisms of fluoride toxicity. Chem. Biol. Interact. 2010, 188, 319–333. [Google Scholar] [CrossRef] [PubMed]
- Hughes, M.F. Biomarkers of exposure: A case study with inorganic arsenic. Environ. Health Perspect. 2006, 114, 1790–1796. [Google Scholar] [PubMed]
- Rugg-Gunn, A.J.; Villa, A.E.; Buzalaf, M.R.A. Contemporary biological markers of exposure to fluoride. Buzalaf Mar (ed): Fluoride and the oral environment. Monogr. Oral Sci. 2011, 22, 37–51. [Google Scholar] [PubMed]
- González-Horta, C.; Sánchez-Ramirez, B.; Ballinas-Casarrubias, L.; Ishida-Gutierrez, C.; del Razo, L.M.; García-Vargas, G.; Loomis, D.; Drobná, Z.; Stýblo, M. Chronic exposure to arsenic and prevalence of diabetes in Mexico. In Proceedings of the 4th International Congress on Arsenic in the Environment, Cairns, Australia, 22–27 July 2012; pp. 169–171.
- Currier, J.M.; Ishida, M.C.; González-Horta, C.; Sánchez-Ramírez, B.; Ballinas-Casarrubias, L.; Gutiérrez-Torres, D.S.; Cerón, R.H.; Morales, D.V.; Terrazas, F.A.; del Razo, L.M.; et al. Associations between arsenic species in exfoliated urothelial cells and prevalence of diabetes among residents of Chihuahua, Mexico. Environ. Health Perspect. 2014, 122, 1088–1094. [Google Scholar] [PubMed]
- Vega-Gleason, S. Riesgo Sanitario Ambiental por la Presencia de Arsénico y Fluoruros en los Acuíferos de México. Available online: https://www.colson.edu.mx:4433/Revista/Articulos/e3/8Haro.pdf (accessed on 14 February 2015).
- Del Razo, L.M.; García-Vargas, G.G.; Valenzuela, O.L.; Hernandez-Castellanos, E.; Sánchez-Peña, L.C.; Currier, J.M.; Drobná, Z.; Loomis, D.; Stýblo, M. Exposure to arsenic in drinking water is associated with increased prevalence of diabetes: A cross-sectional study in the Zimapán and Lagunera regions in Mexico. Environ. Health 2011, 10. [Google Scholar] [CrossRef]
- Del Razo, L.M.; Corona, J.C.; García-Vargas, G.; Albores, A.; Cebrián, M.E. Fluoride levels in well-water from a chronic arsenicism area of Northern Mexico. Environ. Poll. 1993, 80, 91–94. [Google Scholar] [CrossRef]
- Hernández-Zavala, A.; Matoušek, T.; Drobná, Z.; Adair, B.M.; Dĕdina, J.; Thomas, D.J.; Stýblo, M. Speciation of arsenic in biological matrices by automated hydride generation-cryotrapping-atomic absorption spectrometry with multiple microflame quartz tubeatomizer (multiatomizer). J. Anal. At. Spectrom. 2008, 23, 342–351. [Google Scholar] [CrossRef] [PubMed]
- Currier, J.M.; Svoboda, M.; Matoušek, T.; Dědina, J.; Stýblo, M. Direct analysis and stability of methylated trivalent arsenic metabolites in cells and tissues. Metallomics 2011, 3, 1347–1354. [Google Scholar] [CrossRef] [PubMed]
- García-Montalvo, E.A.; Reyes-Pérez, H.; del Razo, L.M. Fluoride exposure impairs glucose tolerance via decreased insulin expression and oxidative stress. Toxicology 2009, 263, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Brahman, K.D.; Kazi, T.G.; Afridi, H.I.; Naseem, S.; Arain, S.S.; Wadhwa, S.K.; Shah, F. Simultaneously evaluate the toxic levels of fluoride and arsenic species in underground water of Tharparkar and possible contaminant sources: A multivariate study. Ecotoxicol. Environ. Saf. 2013, 89, 95–107. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.X.; Wang, Z.H.; Cheng, X.T.; Li, J.; Sang, Z.P.; Zhang, X.D.; Han, L.L.; Qiao, X.Y.; Wu, Z.M.; Wang, Z.Q. Arsenic and fluoride exposure in drinking water: Children’s IQ and growth in Shanyin county, Shanxi province, China. Environ. Health Perspect. 2007, 115, 643–647. [Google Scholar] [CrossRef] [PubMed]
- Reyes-Gómez, V.M.; Alarcón-Herrera, M.T.; Gutiérrez, M.; Núñez-López, D. Fluoride and arsenic in an Alluvial Aquifer System in Chihuahua, Mexico: Contaminant levels, potential sources, and co-occurrence. Water Air Soil Poll. 2013, 224. [Google Scholar] [CrossRef]
- Reyes-Gómez, V.M.; Alarcón-Herrera, M.T.; Gutiérrez, M.; Núñez-López, D. Arsenic and fluoride variations in groundwater of an endorheic basin undergoing land-use changes. Arch. Environ. Contam. Toxicol. 2015, 68, 292–304. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Wang, Y.; Ma, T.; Gan, Y. Speciation and enrichment of arsenic in strongly reducing shallow aquifers at western Hetao Plain, northern China. Environ. Geol. 2009, 56, 1467–1477. [Google Scholar] [CrossRef]
- Scanlona, B.R.; Nicota, J.P.; Reedya, R.C.; Kurtzmana, D.; Mukherjeea, A.; Nordstromb, D.K. Elevated naturally occurring arsenic in a semiarid oxidizing system, Southern High Plains aquifer, Texas, USA. Appl. Geochem. 2009, 24, 2061–2071. [Google Scholar] [CrossRef]
- American Conference of Governmental Industrial Hygienists. Arsenic and soluble Inorganic compounds: BEI®. Available online: http://www.wiley-vch.de/books/info/mak/pdf/MAK_partII_vol4_Arsenic.pdf (accessed on 14 February 2015).
- American Conference of Governmental Industrial Hygienists (ACGIH). Fluorides: BEI®, 7th ed.; ACGIH: Cincinnati, OH, USA, 2012. [Google Scholar]
- Del Razo, L.M.; Garcia-Vargas, G.G.; Garcia-Salcedo, J.; Sanmiguel, M.F.; Rivera, M.; Hernandez, M.C.; Cebrian, M.E. Arsenic levels in cooked food and assessment of adult dietary intake of arsenic in the Region Lagunera, Mexico. Food Chem. Toxicol. 2002, 40, 1423–1431. [Google Scholar] [CrossRef] [PubMed]
- Halder, D.; Bhowmick, S.; Biswas, A.; Chatterjee, D.; Nriagu, J.; Guha Mazumder, D.N.; Šlejkovec, Z.; Jacks, G.; Bhattacharya, P. Risk of arsenic exposure from drinking water and dietary components: Implications for risk management in rural Bengal. Environ. Sci. Technol. 2013, 47, 1120–1127. [Google Scholar] [CrossRef] [PubMed]
- Grimaldo, M.; Borja-Aburto, V.H.; Ramírez, A.L.; Ponce, M.; Rosas, M.; Díaz-Barriga, F. Endemic fluorosis in San Luis Potosi, Mexico. I. Identification of risk factors associated with human exposure to fluoride. Environ. Res. 1995, 68, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Murakami, T.; Narita, N.; Shibata, T.; Nakagaki, H.; Koga, H.; Nishimuta, M. Influence of beverage and food consumption on fluoride intake in Japanese children aged 3–5 years. Caries Res 2009, 43, 382–386. [Google Scholar] [CrossRef] [PubMed]
- Word Health Organization (WHO). Evaluation of Certain Food Additives and Contaminants; 33rd Report of the Join FAO/WHO Expert Committee on Food additives; Technical Report Series 776; WHO: Geneva, Switzerland, 1989. [Google Scholar]
- Rodríguez-Dozal, S.; Alarcón Herrera, M.T.; Cifuentes, E.; Barraza, A.; Loyola-Rodríguez, J.P.; Sanin, L.H. Dental fluorosis in rural communities of Chihuahua, Mexico. Fluoride 2005, 38, 125–132. [Google Scholar]
- Zheng, Y.; Wu, J.; Ng, J.C.; Wang, G.; Lian, W. The absorption and excretion of fluoride and arsenic in humans. Toxicol. Lett. 2002, 133, 77–82. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-Horta, C.; Ballinas-Casarrubias, L.; Sánchez-Ramírez, B.; Ishida, M.C.; Barrera-Hernández, A.; Gutiérrez-Torres, D.; Zacarias, O.L.; Saunders, R.J.; Drobná, Z.; Mendez, M.A.; et al. A Concurrent Exposure to Arsenic and Fluoride from Drinking Water in Chihuahua, Mexico. Int. J. Environ. Res. Public Health 2015, 12, 4587-4601. https://doi.org/10.3390/ijerph120504587
González-Horta C, Ballinas-Casarrubias L, Sánchez-Ramírez B, Ishida MC, Barrera-Hernández A, Gutiérrez-Torres D, Zacarias OL, Saunders RJ, Drobná Z, Mendez MA, et al. A Concurrent Exposure to Arsenic and Fluoride from Drinking Water in Chihuahua, Mexico. International Journal of Environmental Research and Public Health. 2015; 12(5):4587-4601. https://doi.org/10.3390/ijerph120504587
Chicago/Turabian StyleGonzález-Horta, Carmen, Lourdes Ballinas-Casarrubias, Blanca Sánchez-Ramírez, María C. Ishida, Angel Barrera-Hernández, Daniela Gutiérrez-Torres, Olga L. Zacarias, R. Jesse Saunders, Zuzana Drobná, Michelle A. Mendez, and et al. 2015. "A Concurrent Exposure to Arsenic and Fluoride from Drinking Water in Chihuahua, Mexico" International Journal of Environmental Research and Public Health 12, no. 5: 4587-4601. https://doi.org/10.3390/ijerph120504587