Effects of Weather and Heliophysical Conditions on Emergency Ambulance Calls for Elevated Arterial Blood Pressure

Abstract
:1. Introduction
2. Experimental Section
2.1. Study Setting and Population
2.2. Weather and Space Weather Data
2.3. Data Analysis
3. Results and Discussion
3.1. Results
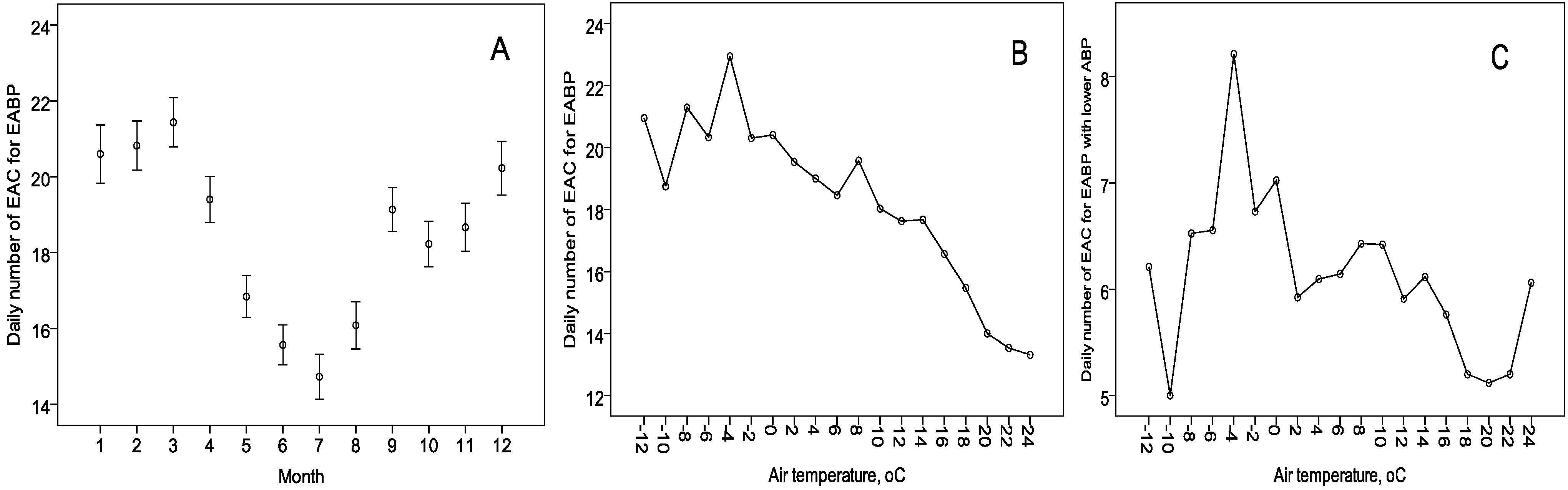
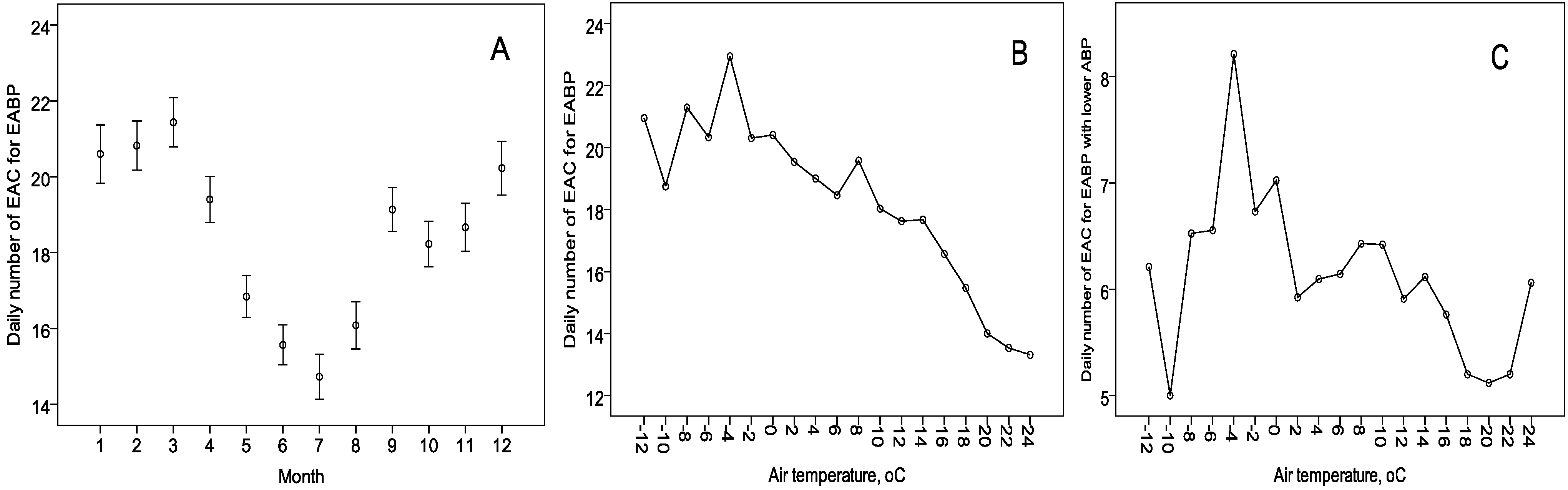
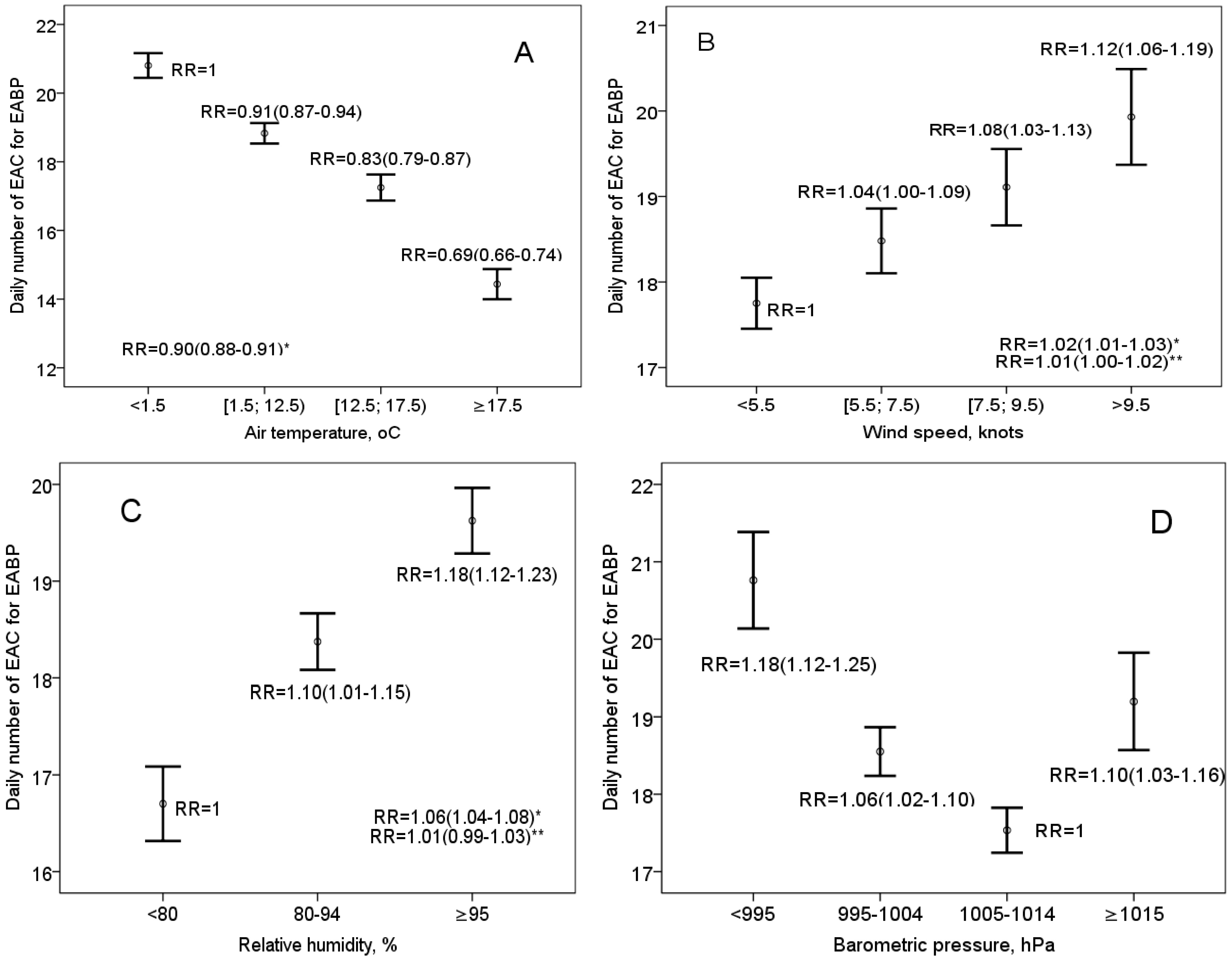
3.1.1. The Effect of Air Temperature, Seasonality, and Day of the Week

{kind=link}
{kind=link}
{kind=link}
| Age | Male | Female | All | |||
|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |
| <30years | 202 | 7.0 | 98 | 0.9 | 300 | 2.2 |
| 30–39 years | 232 | 8.0 | 209 | 2.0 | 441 | 3.3 |
| 40–49 years | 365 | 12.6 | 687 | 6.5 | 1052 | 7.8 |
| 50–59 years | 532 | 18.3 | 1420 | 13.4 | 1952 | 14.5 |
| 60–69 years | 581 | 20.0 | 2366 | 22.4 | 2947 | 21.9 |
| 70–79 years | 645 | 22.2 | 3222 | 30.5 | 3867 | 28.7 |
| 80–89 years | 300 | 10.3 | 2336 | 22.1 | 2636 | 19.6 |
| ≥90 years | 43 | 1.5 | 238 | 2.3 | 281 | 2.1 |
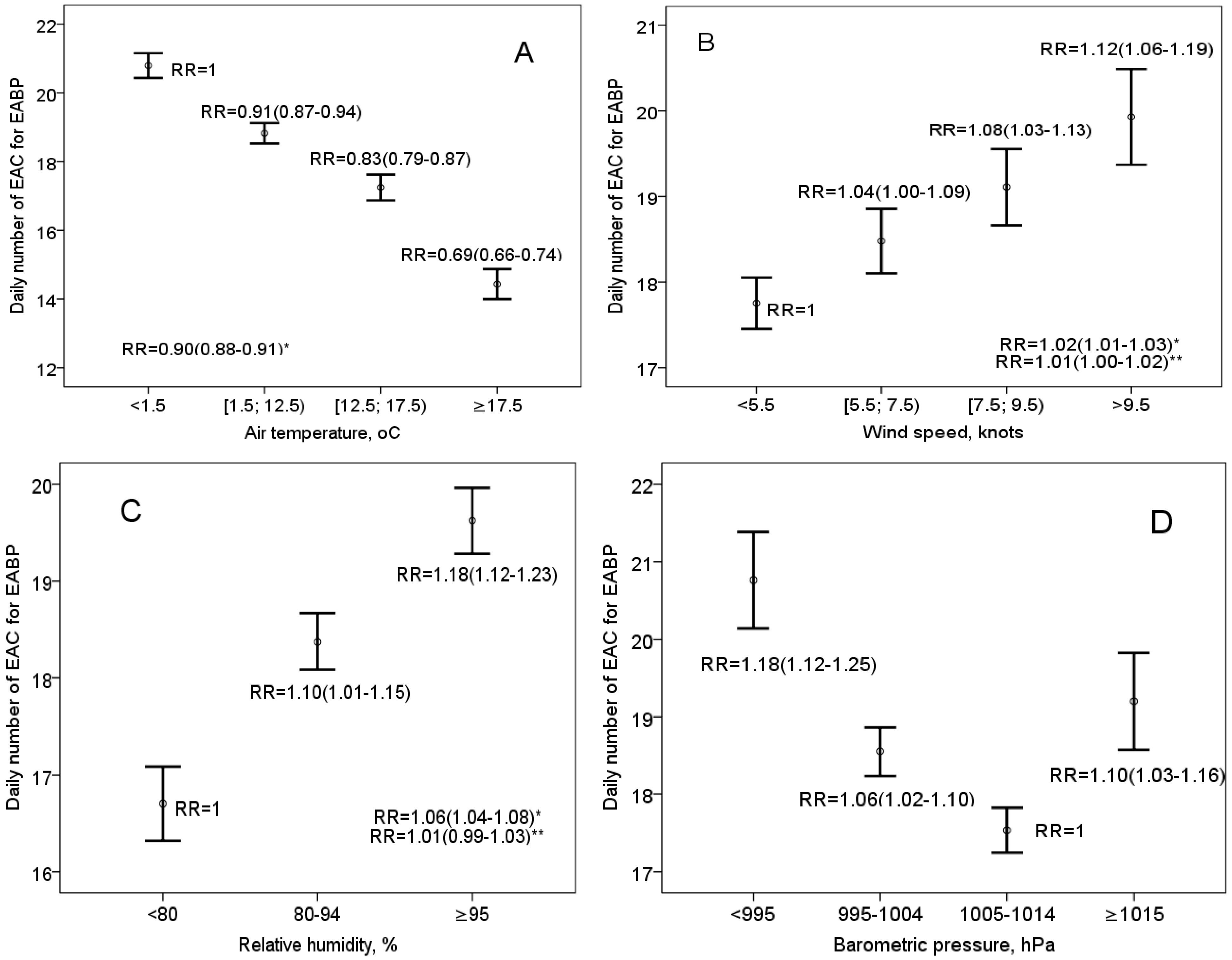
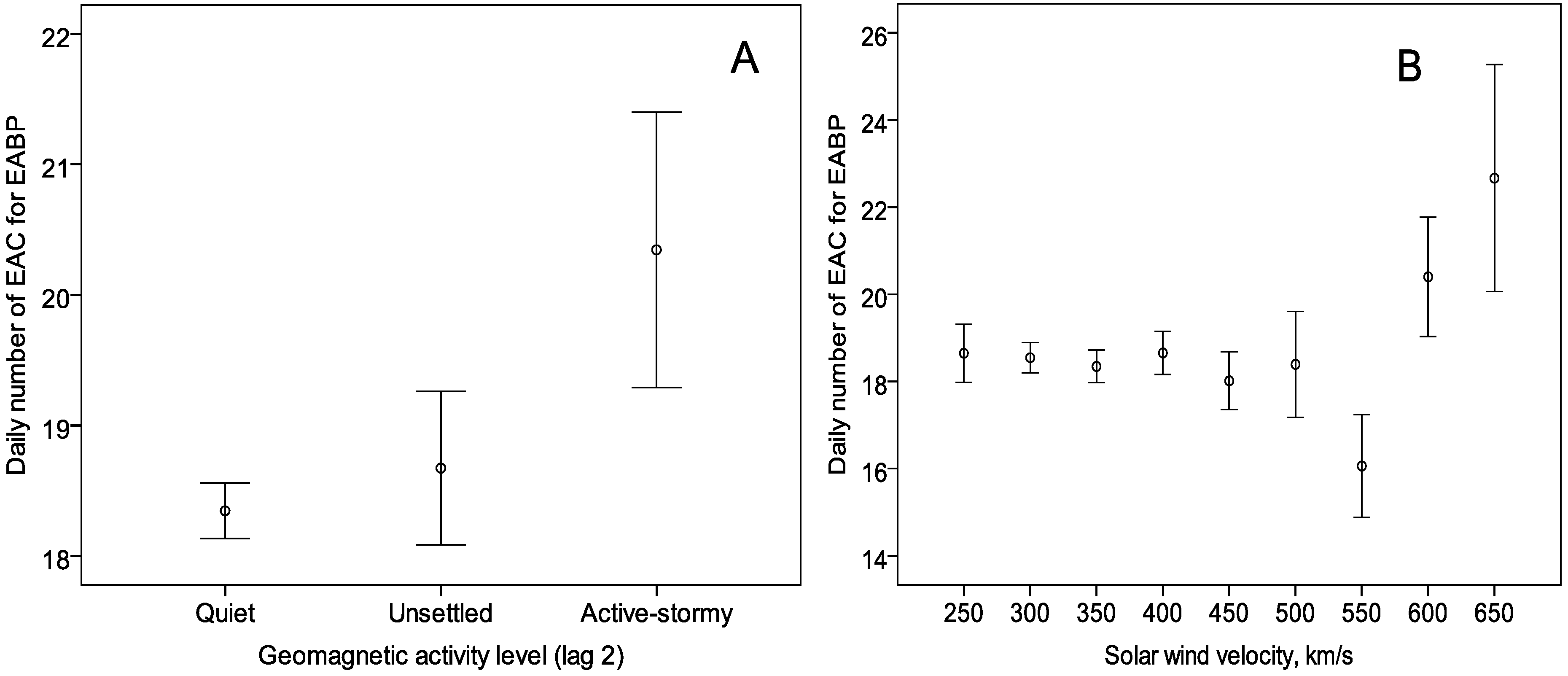
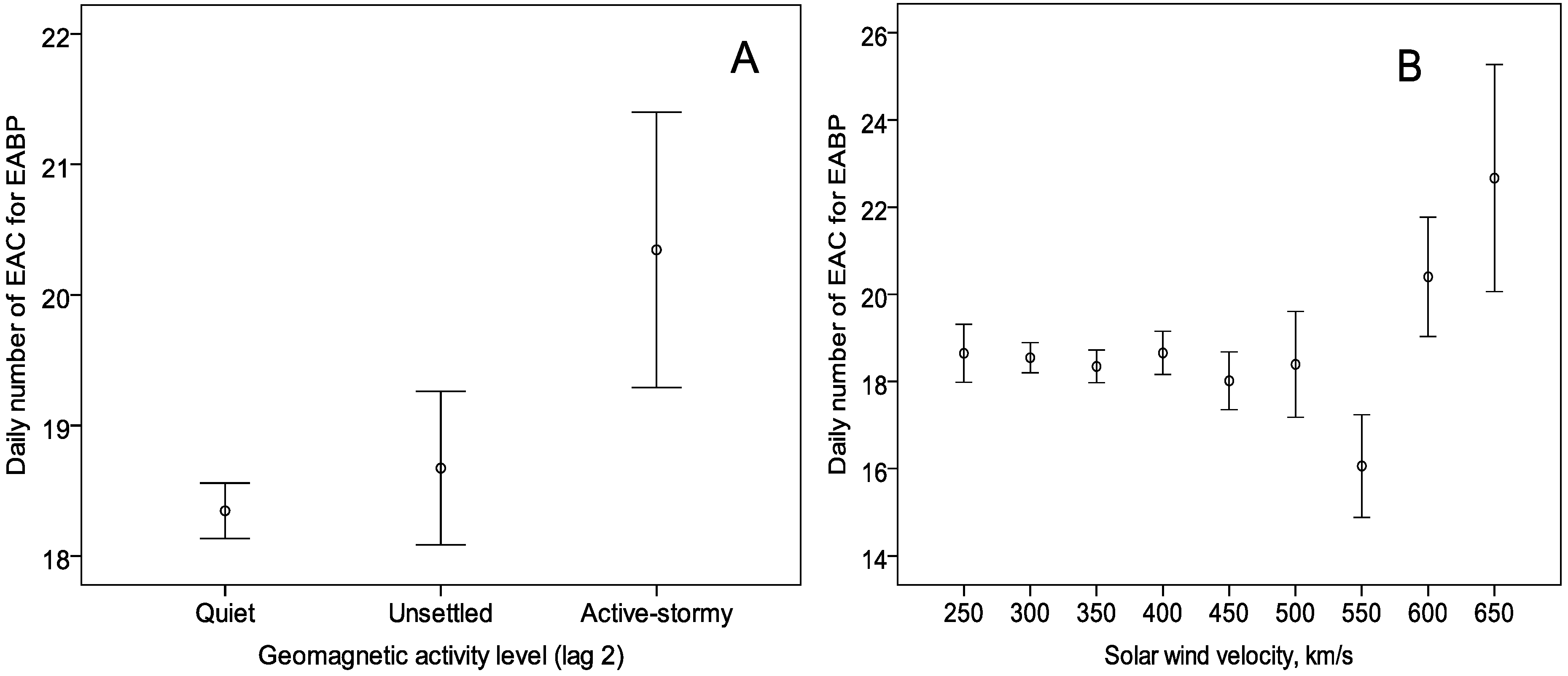
3.1.2. The Effect of Barometric Pressure, Relative Humidity, Wind Speed, and Heliophysical Conditions
| Group | T a | Day length b | BP c (lag2) | WS d WS † | RH e RH † | Helio †† | ||
|---|---|---|---|---|---|---|---|---|
| All | −23 * | −5 * | −3 * | 2 * | 2 * | 7 * | 12 * | 10 * |
| Men | −16 | −1 | −4 | 0 | −2 | 7 * | 9 * | −4 |
| Women | −26 * | −6 * | −3 * | 3 * | 3 * | 7 * | 13 * | 14* |
| Age ≤ 65 years | −20 | −3 * | −3 * | 3 * | 1 | 11 * | 12 * | 7 * |
| Age > 65 years | −26 * | −6 * | −3 * | 1 | 2 * | 4 * | 12 * | 11 * |
| 3th grade AH | −42 * | −4 * | −4 * | 2 * | 2 * | 7 * | 11 * | 10 * |
| 1–2th grade AH | 19 | −5 * | 0 | 3 * | 1 | 7 * | 13 * | 9 |
3.1.3. The Multivariate Effects of Environmental Variables
3.2. Discussion
| Factors | All patients | Men | Women | Age ≤ 65 years | Age > 65 years | 3th grade AH | 1–2th grade AH |
|---|---|---|---|---|---|---|---|
| Monday–Tuesday | 1.08 (1.041.12) | 1.14 (1.05–1.23) | 1.06 (1.01–1.11) | 1.12 (1.05–1.19) | 1.05 (1.00–1.10) | 1.10 (1.05–1.15) | 1.03 (0.96–1.10) |
| National holiday | 1.33 (1.13–1.56) | 0.98 (0.66–1.47) | 1.41 (1.18–1.68) | 1.19 (0.91–1.56) | 1.40 (1.14–1.70) | 1.47 (1.22–1.77) | 1.03 (0.75–1.42) |
| Other holiday * | 0.80 (0.68–0.93) | 0.66 (0.45–0.95) | 0.84 (0.70–1.00) | 0.86 (0.67–1.09) | 0.75 (0.60–0.92) | 0.77 (0.63–0.94) | 0.83 (0.64–1.09) |
| Helio | 1.12 (1.04–1.21) | 1.16 (1.06–1.26) | 1.09 (0.97–1.23) | 1.14 (1.03–1.25) | 1.12 (1.02–1.23) | 1.13 (0.99–1.28) | |
| T (increase in 10 °C) | 0.97 (0.94–0.99) | 0.91 (0.88–0.95) | 0.98 (0.95–1.01) | 0.98 (0.94–1.03) | 0.96 (0.93–1.00) | 0.94 (0.91–0.97) | 1.03 (0.98–1.08) |
| BP (lag2) (increase in 10 hPa) | 0.97 (0.95–0.99) | 0.95 (0.91–0.99) | 0.97 (0.95–1.00) | 0.96 (0.93–0.99) | 0.96 (0.93–0.98) | ||
| T × T ≥ 17.5) | 0.99 (0.98–0.99) | 0.99 (0.98–0.99) | 0.99 (0.98–0.99) | 0.99 (0.98–0.99) | 0.99 (0.98–0.99) | 0.99 (0.98–1.00) | |
| (Day length–12) × (12.5 ≤ T < 17.5) | 0.96 (0.95–0.98) | 0.95 (0.94–0.97) | 0.97 (0.94–0.99) | 0.96 (0.94–0.98) | 0.97 (0.95–0.99) | 0.95 (0.93–0.98) | |
| (WS ≥ 5.5) × (T < 1.5 or T ≥ 12.5) | 1.08 (1.04–1.12) | 1.08 (1.04–1.13) | 1.09 (1.03–1.15) | 1.06 (1.01–1.12) | 1.05 (1.00–1.10) | 1.12 (1.05–1.20) | |
| (BP < 995) or (BP ≥ 1015) (lag2) | 1.08 (1.00–1.16) | ||||||
| WS ≥ 3.5 | 1.09 (0.98–1.21) | ||||||
| BP < 995 | 1.09 (1.02–1.16) |
3.3. Limitations
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redon, J.; Zanchetti, A.; Bohm, M.; Christiaens, T.; Cifkova, R.; De Backer, G.; Dominiczak, A.; et al. 2013 ESH/ESC Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur. Heart J. 2013, 34, 2159–2219. [Google Scholar] [CrossRef] [PubMed]
- Taddei, S. Blood pressure through aging and menopause. Climateric 2009, 12, 36–40. [Google Scholar] [CrossRef]
- Palatini, P.; Mos, L.; Santonastaso, M.; Saladini, F.; Benetti, E.; Mormino, P.; Bortolazzi, A.; Cozzio, S. Premenopausal women have increased risk of hypertensive target organ damage compared with men of similar age. J. Womens Health (Larchmt) 2011, 20, 1175–1181. [Google Scholar] [CrossRef]
- Geraci, T.S.; Geraci, S.A. Considerations in women with hypertension. South. Med. J. 2013, 106, 434–438. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.D.; Weder, A.B.; Rajagopalan, S. Environmental hypertensionology”. The effects of environmental factors on blood pressure in clinical practice and research. J. Clin. Hypertens. (Greenwich). 2011, 13, 836–842. [Google Scholar] [CrossRef]
- Brook, R.D.; Rajagopalan, S. Particulate matter air pollution and blood pressure. J. Am. Soc. Hypertens. 2009, 3, 332–350. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.D.; Bard, R.L.; Burnett, R.T.; Shin, H.H.; Vette, A.; Croghan, C.; Phillips, M.; Rodes, C.; Thornburg, J.; Williams, R. Differences in blood pressure and vascular responses associated with ambient fine particulate matter exposures measured at the personal versus community level. Occup. Environ. Med. 2011, 68, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Fuks, K.; Mebus, S.; Hertel, S.; Viehmann, A.; Nonnemacher, M.; Dragano, N.; Möhlenkamp, S.; Jakobs, H.; Kessler, C.; Erbel, R.; Hoffmann, B. Long-term urban particulate air pollution, traffic noise and arterial blood pressure. Environ. Health Perspect. 2011, 119, 1706–1711. [Google Scholar] [CrossRef] [PubMed]
- Barregard, L. Traffic noise and hypertension. Environ. Res. 2011, 111, 186–187. [Google Scholar] [CrossRef] [PubMed]
- Barregard, L.; Bonde, E.; Ohrstrom, E. Risk of hypertension from exposure to road traffic noise in a population-based sample. Occup. Environ. Med. 2009, 66, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Chang, T.Y.; Lai, Y.A.; Hsieh, H.H.; Lai, J.S.; Liu, C.S. Effects of environmental noise exposure on ambulatory blood pressure in young adults. Environ. Res. 2009, 109, 900–905. [Google Scholar] [CrossRef] [PubMed]
- Davies, H.W.; Vlaanderen, J.J.; Henderson, S.B.; Brauer, M. Correlation between co-exposures to noise and air pollution from traffic sources. Occup. Environ. Med. 2009, 66, 347–350. [Google Scholar] [CrossRef] [PubMed]
- Halonen, J.I.; Zanobetti, A.; Sparrow, D.; Vokonas, P.S.; Schwartz, J. Relationship between outdoor temperature and blood pressure. Occup. Environ. Med. 2011, 68, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Barnett, A.G.; Sans, S.; Salomaa, V.; Kuulasmaa, K.; Dobson, A.J. The effect of temperature on systolic blood pressure. Blood Press. Monit. 2007, 12, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Lewington, S.; Li, L.; Sherliker, P.; Guo, Y.; Millwood, I.; Bian, Z. Seasonal variation in blood pressure and its relationship with outdoor temperature in 10 diverse regions of China: The China Kadoorie Biobank. J. Hypertens. 2012, 30, 1383–1391. [Google Scholar] [CrossRef] [PubMed]
- Woodhouse, P.R.; Khaw, K-T.; Plummer, M. Seasonal variation of blood pressure and its relationship to ambient temperature in an elderly population. J. Hypertens. 1993, 11, 1267–1274. [Google Scholar] [CrossRef] [PubMed]
- Hopstock, L.A.; Barnett, A.G.; Bønaa, K.H.; Mannsverk, J.; Njølstad, I.; Wilsgaard, T. Seasonal variation in cardiovascular disease risk factors in a subarctic population: The Tromsø Study 1979–2008. J. Epidemiol. Community Health 2013, 67, 113–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Modesti, P.A.; Morabito, M.; Massetti, L.; Rapi, S.; Orlandini, S.; Mancia, G.; Gensini, G.F.; Parati, G. Seasonal blood pressure changes: An independent relationship with temperature and daylight hours. Hypertension 2013, 61, 908–914. [Google Scholar] [CrossRef] [PubMed]
- Ghione, S.; Mezzasalma, L.; Del Seppia, C.; Papi, F. Do geomagnetic disturbances of solar origin affect arterial blood pressure? J. Hum. Hypertension 1998, 12, 749–754. [Google Scholar] [CrossRef]
- Dimitrova, S.; Stoilova, I. Planetary geomagnetic indices, human physiology and subjective complaints. J. Balkan. Geophys. Soc. 2003, 6, 37–45. [Google Scholar]
- Charach, G.; Shochat, M.; Argov, O.; Weintraub, M.; Charach, L. Seasonal changes in blood pressure: Cardiac and cerebrovascular morbidity and mortality. World J. Hypertens. 2013, 3, 1–8. [Google Scholar] [CrossRef]
- Iwabu, A.; Konishi, K.; Tokutake, H.; Yamane, S.; Ohnishi, H.; Tominaga, Y.; Kusachi, S. Inverse correlation between seasonal changes in home blood pressure and atmospheric temperature in treated-hypertensive patients. Clin. Exp. Hypertens. 2010, 32, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Basu, R.; Pearson, D.; Malig, B.; Broadwin, R.; Green, R. The effect of high ambient temperature on emergency room visits. Epidemiology 2012, 23, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Dedele, A.; Miskinyte, A. Estimation of inter-seasonal differences in NO2 concentrations using a dispersion ADMS-Urban model and measurements. Air Qual. Atmos. Health 2014. [CrossRef]
- Yakerson, N. On the correlation between wind speed, coarse aerosol concentration and the electric state in the ground atmospheric layer in semi-arid areas. Sci. Total Environ. 2002, 293, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Israelsson, S.; Tammet, H. Variation of fair weather atmospheric elecricity at Marsta Observatory, Sweden, 1993–1998. J. Atmos. Sol. Terr. Phys. 2001, 63, 1693–1703. [Google Scholar] [CrossRef]
- Pressinger, M.A. Mental processes and disorders: A neurobehavioral perspective in human biometeorology. Experentia 1987, 43, 39–48. [Google Scholar] [CrossRef]
- Cherry, N. Actual or Potential Effects of Elf and Rf/Mw Radiation on Enhancing Violence and Homicide, and Accelerating Aging of Human, Animal or Plant Cells. Available online: http://researcharchive.lincoln.ac.nz/bitstream/10182/4006/1/90_s8_EMR_and_Aging_and_violence.pdf (accessed on 30 August 2002).
- Giertz, H.W. Extremely low frequency electromagnetic energy in the air. J. Atmos. Sol. Terr. Phys. 2010, 72, 767–773. [Google Scholar] [CrossRef]
- Kolesnik, S.A.; Pikalov, M.V.; Solovev, S.A.; Chukin, V.V. Physical principles of forescasting the characteristics of the ELF environmental electromagnetic background noise from the meteorological factors. Russ. Phys. J. 2008, 51, 980–985. [Google Scholar] [CrossRef]
- Morabito, M.; Crisci, A.; Orlandini, S.; Maracchi, G.; Gensini, G.F.; Modesti, P.A. A synoptic approach to weather conditions discloses a relationship with ambulatory blood pressure in hypertensives. Am. J. Hypertens. 2008, 21, 748–752. [Google Scholar] [CrossRef] [PubMed]
- Wong, H.T.; Lai, P.C. Weather inference and daily demand for emergency ambulance services. Emer. Med. J. 2012, 29, 60–64. [Google Scholar] [CrossRef]
- Danet, S.; Richard, F.; Montaye, M.; Beauchant, S.; Lemaire, B.; Graux, C.; Cottel, D.; Marécaux, N.; Amouyel, P. Unhealthy effects of atmospheric temperature and pressure on the occurrence of myocardial infarction and coronary deaths. A 10-year survey: The Lille-World Health Organization MONICA project (Monitoring trends and determinants in cardiovascular disease). Circulation 1999, 100, E1–E7. [Google Scholar] [CrossRef] [PubMed]
- Weinbacher, M.; Martina, B.; Bart, T.; Drewe, J.; Gasser, P.; Gyr, K. Blood pressure and atmospheric pressure. Ann. N. Y. Acad. Sci. 1996, 738, 335–336. [Google Scholar] [CrossRef]
- Dimitrova, S.; Stoilova, I.; Cholakov, I. Influence of local geomagnetic storms on arterial blood pressure. Bioelectromagnetics 2004, 25, 408–414. [Google Scholar] [CrossRef]
- Narkiewicz, K.; Phillips, B.G.; Kato, M.; Hering, D.; Bieniaszewski, L.; Somers, V.K. Gender-selective interaction between aging, blood pressure, and sympathetic nerve activity. Hypertension 2005, 45, 522–525. [Google Scholar] [CrossRef] [PubMed]
- Carter, J.R.; Fu, Q.; Minson, C.T.; Joyner, M.J. Ovarian cycle and sympathoexcitation in premenopausal women. Hypertension 2013, 61, 395–399. [Google Scholar] [CrossRef] [PubMed]
- Xue, B.; Zhang, Z.; Beltz, T.G.; Johnson, R.F.; Guo, F.; Hay, M.; Johnson, A.K. Estrogen receptor-β in the paraventricular nucleus and rostroventrolateral medulla plays an essential protective role in aldosterone/salt-induced hypertension in female rats. Hypertension 2013, 61, 1255–1262. [Google Scholar] [CrossRef] [PubMed]
- Hart, E.C.; Charkoudian, N.; Wallin, B.G.; Curry, T.B.; Eisenach, J.H.; Joyner, M.J. Sex differences in sympathetic neural-hemodynamic balance: Implications for human blood pressure regulation. Hypertension 2009, 53, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Krause, D.N.; Doolen, S.; Duckles, S.P. Ovariectomy eliminates sex differences in rat tail artery response to adrenergic nerve stimulation. Am. J. Physiol. 1997, 272, H1819–H1825. [Google Scholar]
- Denton, K.M.; Hilliard, L.M.; Tare, M. Sex-related differences in hypertension: Seek and ye shall find. Hypertension 2013, 62, 674–677. [Google Scholar] [CrossRef] [PubMed]
- Hong, Y.C.; Kim, H.; Oh, S.Y.; Lim, Y.H.; Kim, S.Y. Association of cold ambient temperature and cardiovascular markers. Sci. Total Environ. 2012, 435, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.S.; Thomas, A.; Evans, R.S.; Welch, S.J.; Haug, P.J.; Snow, G.L. Forecasting daily patient volumes in the emergency department. Acad. Emerg. Med. 2008, 15, 159–170. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Heng, B.H.; Seow, Y.T.; Seow, E. Forecasting daily attendances at an emergency department to aid resource planning. BMC Emerg. Med. 2009, 9. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vencloviene, J.; Babarskiene, R.M.; Dobozinskas, P.; Sakalyte, G.; Lopatiene, K.; Mikelionis, N. Effects of Weather and Heliophysical Conditions on Emergency Ambulance Calls for Elevated Arterial Blood Pressure. Int. J. Environ. Res. Public Health 2015, 12, 2622-2638. https://doi.org/10.3390/ijerph120302622
Vencloviene J, Babarskiene RM, Dobozinskas P, Sakalyte G, Lopatiene K, Mikelionis N. Effects of Weather and Heliophysical Conditions on Emergency Ambulance Calls for Elevated Arterial Blood Pressure. International Journal of Environmental Research and Public Health. 2015; 12(3):2622-2638. https://doi.org/10.3390/ijerph120302622
Chicago/Turabian StyleVencloviene, Jone, Ruta M. Babarskiene, Paulius Dobozinskas, Gintare Sakalyte, Kristina Lopatiene, and Nerijus Mikelionis. 2015. "Effects of Weather and Heliophysical Conditions on Emergency Ambulance Calls for Elevated Arterial Blood Pressure" International Journal of Environmental Research and Public Health 12, no. 3: 2622-2638. https://doi.org/10.3390/ijerph120302622