
Spatial Pattern Detection of Tuberculosis: A Case Study of Si Sa Ket Province, Thailand

Abstract
:1. Introduction
2. Materials and Methods
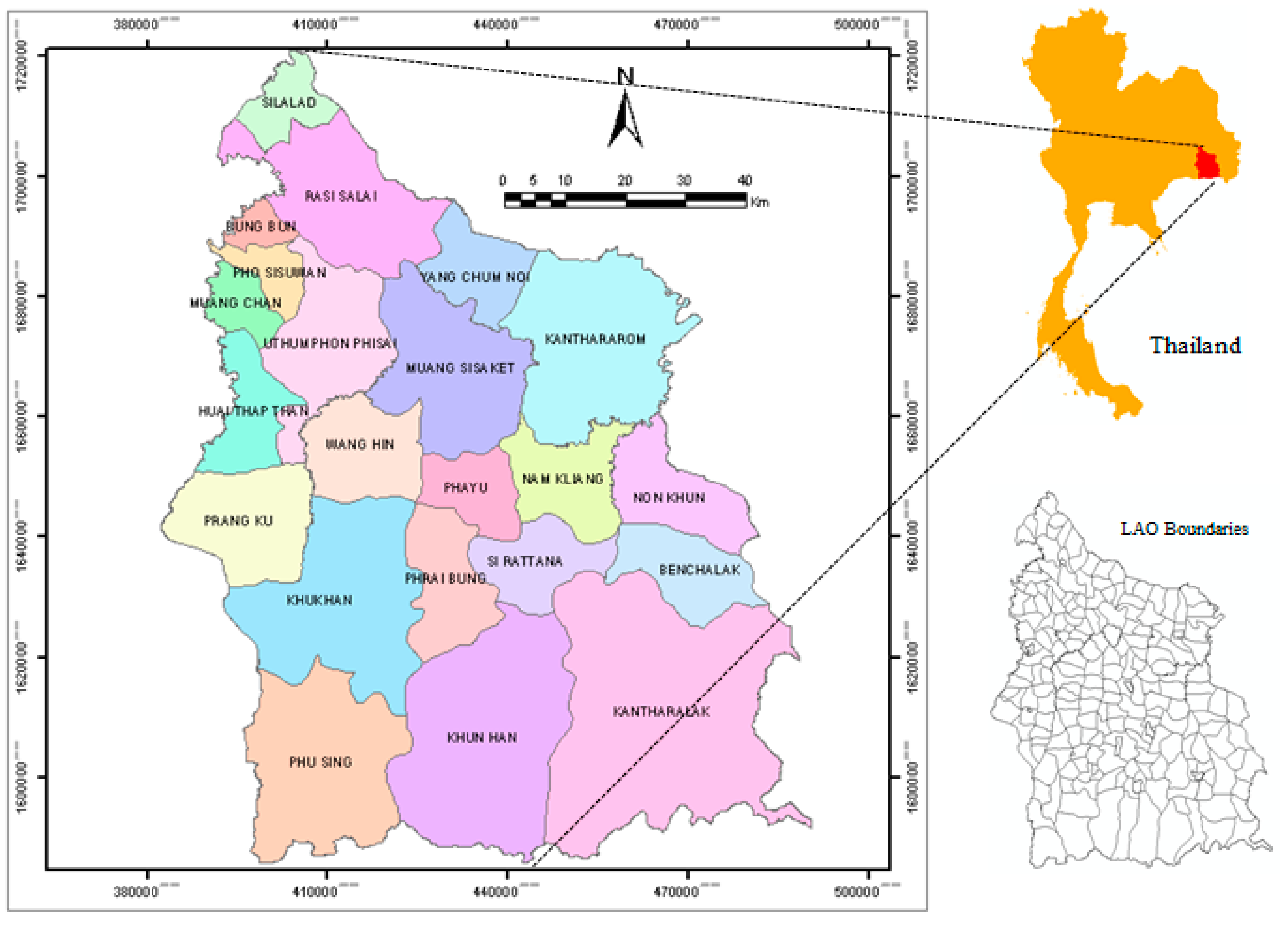
2.1. Study Area

2.2. Data Collection and Manipulation
2.2.1. TB Registration Data
2.2.2. Spatial Data
2.2.3. Demographic Data
2.3. Incidence Rates Calculation and Adjustment
2.4. Spatial Pattern Detection
2.4.1. Global Detection
2.4.2. Local Detection
2.5. Spatial Scan Statistic
3. Results and Discussion
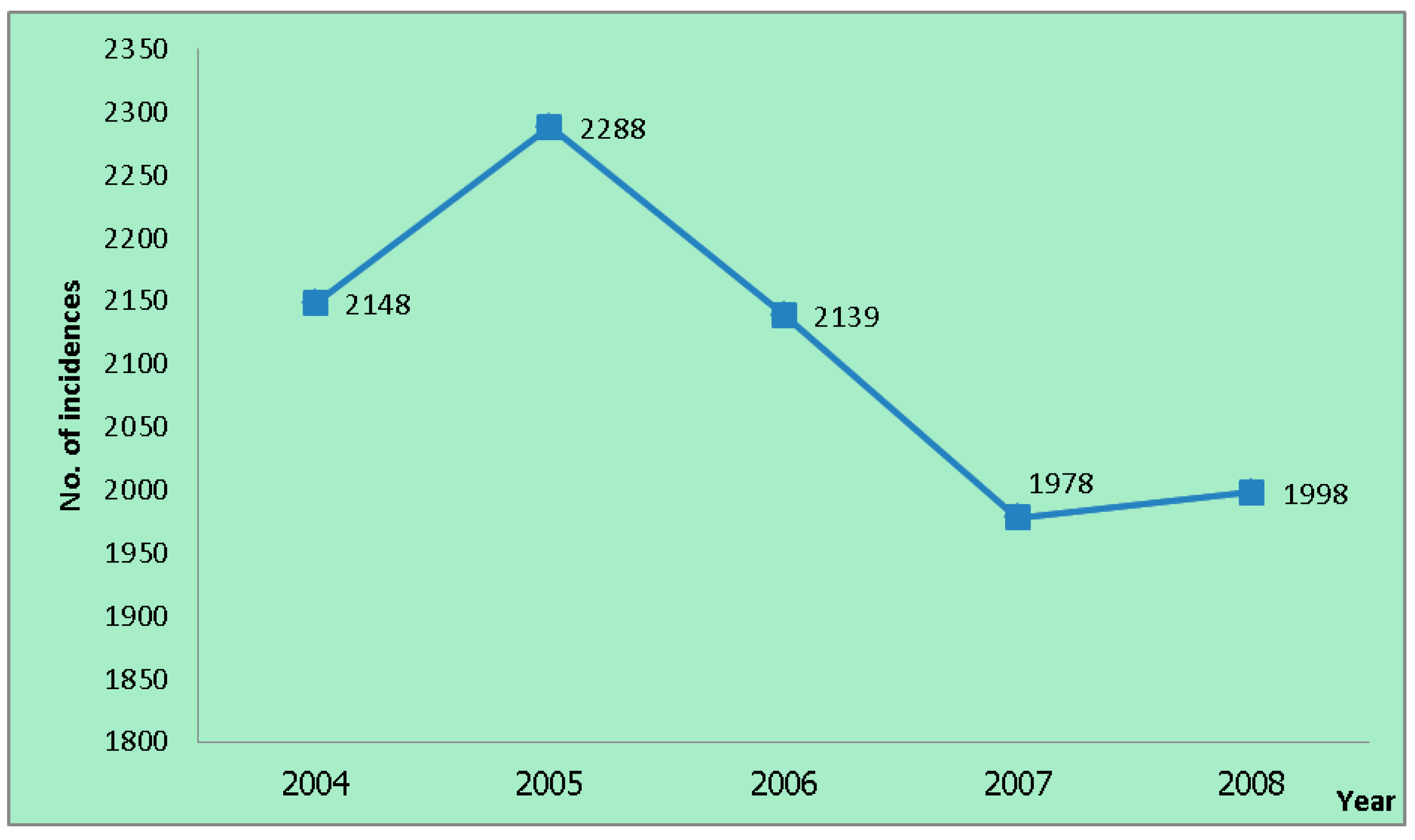
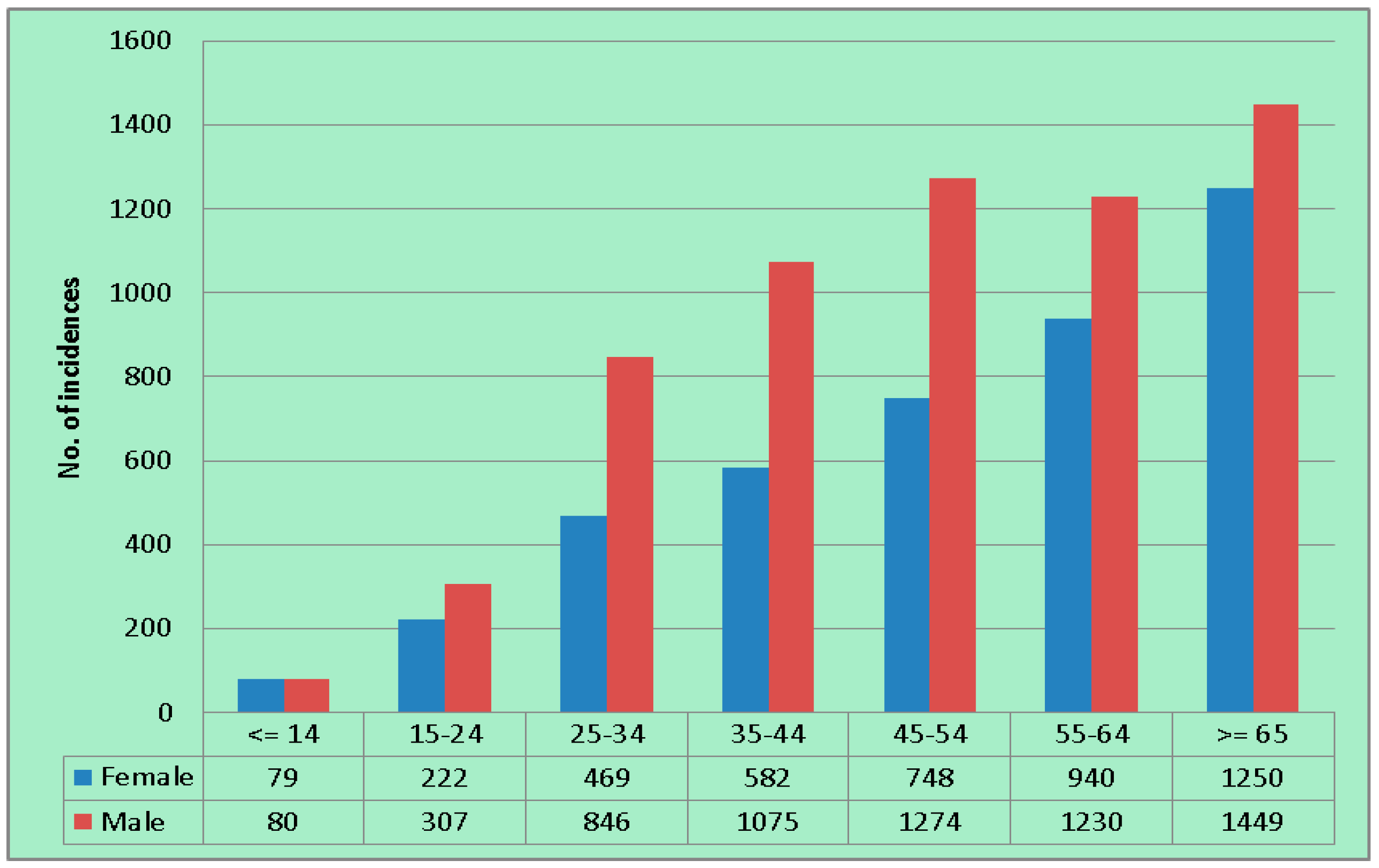
3.1. Descriptive Analysis of TB Case Notification



3.2. Spatial Pattern of TB
3.2.1. Global Spatial Pattern

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Moran’s Index | Interpretation |
|---|---|---|
| 2004 | 0.1888 | Clustered |
| 2005 | 0.2721 | Clustered |
| 2006 | 0.3081 | Clustered |
| 2007 | 0.2682 | Clustered |
| 2008 | 0.1910 | Clustered |
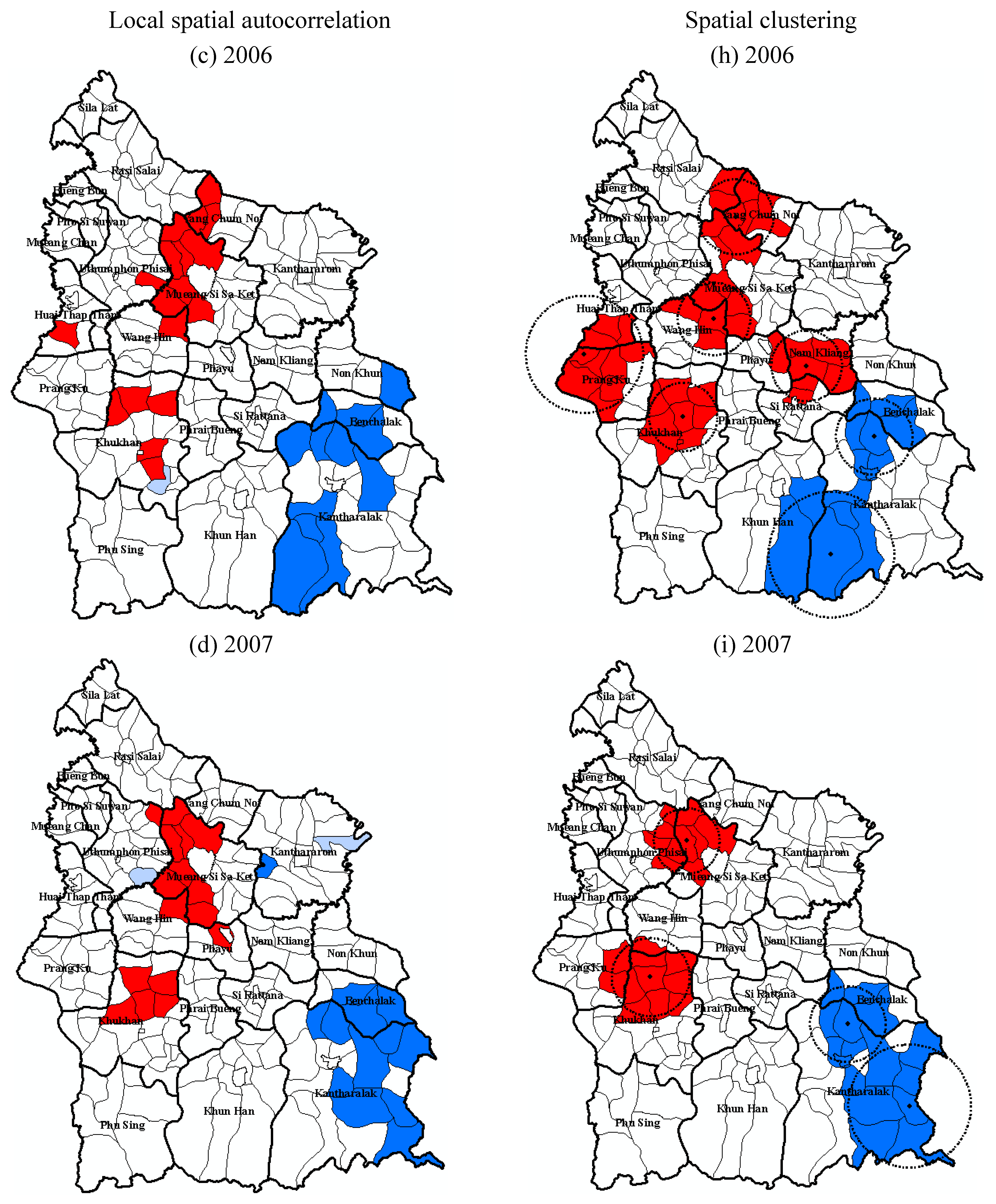
3.2.2. Local Spatial Pattern



3.3. Discussion
3.3.1. Age Standardization of TB Incidence Data
3.3.2. Comparison between the Local Spatial Pattern Detection Techniques
3.3.3. The Variations in the Spatial Patterns
3.3.4. Limitations
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization. TB: A Global Emergency, WHO Report on the TB Epidemic; World Health Organization: Geneva, Switzerland, 1994; p. 28. [Google Scholar]
- World Health Organization. Global Tuberculosis Report 2014; World Health Organization: Geneva, Switzerland, 2014; p. 152. [Google Scholar]
- Rangsriwong, S. Annual Epidemiological Surveillance Report 2010; Bureau of Epidemiology: Bangkok, Thailand, 2011. [Google Scholar]
- Tiwari, N.; Adhikari, C.M.S.; Tewari, A.; Kandpal, V. Investigation of geo-spatial hotspots for the occurrence of tuberculosis in Almora district, India, using GIS and spatial scan statistic. Int. J. Health Geogr. 2006, 5. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, N.; Kandpal, V.; Tewan, A.; Rao, K.R.M.; Tolia, V. Investigation of tuberculosis clusters in Dehradun city of India. Asian Pac. J. Trop. Med. 2010, 3, 486–490. [Google Scholar] [CrossRef]
- Couceiro, L.; Santana, P.; Nunes, C. Pulmonary tuberculosis and risk factors in Portugal: A spatial analysis. Int. J. Tuberc. Lung Dis. 2011, 15, 1445–1454. [Google Scholar] [CrossRef] [PubMed]
- Onozuka, D.; Hagihara, A. Geographic prediction of tuberculosis clusters in Fukuoka, Japan, using the space-time scan statistic. BMC Infect. Dis. 2007, 7. [Google Scholar] [CrossRef] [PubMed]
- Randremanana, R.V.; Sabatier, P.; Rakotomanana, F.; Randriamanantena, A.; Richard, V. Spatial clustering of pulmonary tuberculosis and impact of the care factors in Antananarivo city. Trop. Med. Int. Health 2009, 14, 429–437. [Google Scholar] [CrossRef] [PubMed]
- Nunes, C. Tuberculosis incidence in Portugal: Spatiotemporal clustering. Int. J. Health Geogr. 2007, 6. [Google Scholar] [CrossRef] [PubMed]
- Munch, Z.; Van-Lill, S.W.P.; Booysen, C.N.; Zietsman, H.L.; Enarson, D.A.; Beyers, N. Tuberculosis transmission patterns in a high-incidence area: A spatial analysis. Int. J. Tuberc. Lung Dis. 2003, 7, 271–277. [Google Scholar] [PubMed]
- Touray, K.; Adetifa, I.M.; Jallow, A.; Rigby, J.; Jeffries, D.; Cheung, Y.B.; Donkor, S.; Adegbola, R.A.; Hill, P.C. Spatial analysis of tuberculosis in an urban West African setting: Is there evidence of clustering? Trop. Med. Int. Health 2010, 15, 664–672. [Google Scholar] [CrossRef] [PubMed]
- Maciel, E.L.N.; Pan, W.; Dietze, R.; Peres, R.L.; Vinhas, S.A.; Ribeiro, F.K.; Palaci, M.; Rodrigues, R.R.; Zandonade, E.; Golub, J.E. Spatial patterns of pulmonary tuberculosis incidence and their relationship to socio-economic status in Vitoria, Brazil. Int. J. Tuberc. Lung Dis. 2010, 14, 1395–1402. [Google Scholar] [PubMed]
- Jia, Z.W.; Jia, X.W.; Liu, Y.X.; Dye, C.; Chen, F.; Chen, C.S.; Zhang, W.Y.; Li, X.W.; Cao, W.C.; Liu, H.L. Spatial analysis of tuberculosis cases in migrants and permanent residents, Beijing, 2000–2006. Emerg. Infect. Dis. 2008, 11, 1413–1420. [Google Scholar] [CrossRef] [PubMed]
- Sisaket Provincial Statistical Data Center. General Information of Sisaket Province. Available online: http://sisaket.nso.go.th/sisaket/HTML/aboutpro.html (accessed on 12 March 2012).
- Department of Provincial Administration. Thailand Population Statistics. 2008. Available online: http://stat.bora.dopa.go.th/stat/y_stat51.html (accessed on 24 May 2015).
- Bureau of Tuberculosis. National Tuberculosis Control Programme Guidelines; Bureau of Tuberculosis: Bangkok, Thailand, 2013; p. 186. [Google Scholar]
- Lai, P.C.; So, F.M.; Chan, K.W. Spatial Epidemiological Approaches in Disease Mapping and Analysis; CRC Press: New York, NY, USA, 2009. [Google Scholar]
- Bland, M. An Introduction to Medical Statistics, 2nd ed.; Oxford University Press: New York, NY, USA, 1995. [Google Scholar]
- Bonita, R.; Beaglehole, R.; Kjellström, T. Basic Epidemiology, 2nd ed.; World Health Organization: Geneva, Switzerland, 2006; p. 212. [Google Scholar]
- Faramnuayphol, P.; Vapattanawong, P. Difference of Mortality among Areas in Thailand; Health Information System Development Office: Bangkok, Thailand, 2005; pp. 14–17. [Google Scholar]
- Rothman, K.J.; John D. Boice, J. Epidemiologic Analysis with a Programmable Calculator; U.S. Government Printing Office: Washington, DC, USA, 1979.
- Breslow, N.E.; Day, N.E. Statistical Methods in Cancer Research; Oxford University Press: Oxford, UK, 1987; Volume II. [Google Scholar]
- Souris, M. SavGIS: GIS software. Available online: http://www.savgis.org/ (accessed on 30 November 2014).
- Moran, P.A.P. Notes on continuous stochastic phenomena. Biometrika 1950, 37, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Tsai, P.J.; Lin, M.L.; Chu, C.M.; Perng, C.H. Spatial autocorrelation analysis of health care hotspots in Taiwan in 2006. BMC Public Health 2009, 9. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, D.U.; Robinson, T.P.; Stevenson, M.; Stevens, K.B.; Rogers, D.J.; Clements, A.C.A. Spatial Analysis in Epidemiology; Oxford University Press Inc.: New York, NY, USA, 2008. [Google Scholar]
- Kulldorff, M. Software for the Spatial and Space-Time Scan Statistics. Available online: http://www.satscan.org (accessed on 24 September 2010).
- Kulldorff, M. A spatial scan statistic. Commun. Stat. Theory Methods 1997, 26, 1481–1496. [Google Scholar] [CrossRef]
- Agay-Shay, K.; Amitai, Y.; Peretz, C.; Linn, S.; Friger, M.; Peled, A. Exploratory spatial data analysis of congenital malformations (CM) in Israel, 2000–2006. ISPRS Int. J. Geoinf. 2013, 2, 237–255. [Google Scholar] [CrossRef]
- Julious, S.A.; Nicholl, J.; George, S. Why do we continue to use standardized mortality ratios for small area comparison? J. Public Health Med. 2001, 23, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Pickle, L.W.; White, A.A. Effects of the choice of age-adjustment method on maps of death rates. Stat. Med. 1995, 14, 615–627. [Google Scholar] [CrossRef] [PubMed]
- Schoenbach, V.J. Standardization of Rates And Ratios. Available online: http://www.epidemiolog.net (accessed on 9 December 2015).
- Bains, N. Standardization of Rates; Association of Public Health Epidemiologists in Ontario: Ontario, Canada, 2009. [Google Scholar]
- Eayres, D. Commonly Used Public Health Statistics and Their Confidence Intervals; Association of Public Health Observatiories: York, United Kingdom, 2008. [Google Scholar]
- Buescher, P.A. Age-adjusted death rates. In Statistical Primer; Department of Health and Human Services, Ed.; The North Carolina Department of Health and Human Services: North Carolina, NC, USA, 2010; Volume 13. [Google Scholar]
- Bhatti, N.; Law, M.R.; Morris, J.K.; Halliday, R.; Moore-Gillon, J. Increasing incidence of tuberculosis in England and Wales: A study of the likely causes. BMJ 1995, 310, 967–969. [Google Scholar] [CrossRef] [PubMed]
- Faramnuayphol, P.; Chongsuvivatwong, V.; Pannarunothai, S. Geographical variation of mortality in Thailand. J. Med. Assoc. Thai. 2008, 91, 1455–1460. [Google Scholar] [PubMed]
- Leung, C.C.; Yew, W.W.; Tam, C.M.; Chan, C.K.; Chang, K.C.; Law, W.S.; Wong, M.Y.; Au, K.F. Socio-economic factors and tuberculosis: A district-based ecological analysis in Hong Kong. Int. J. Tuberc. Lung Dis. 2004, 8, 958–964. [Google Scholar] [PubMed]
- Mangtani, P.; Jolley, D.J.; Watson, J.M.; Rodrigues, L.C. Socioeconomic deprivation and notification rates for tuberculosis in London during 1982–1991. BMJ 1995, 310, 963–966. [Google Scholar] [CrossRef] [PubMed]
- Anselin, L. Review of Cluster Analysis Software; The North American Association of Central Cancer Registries, Inc.: Illinois, IL, USA, 2004. [Google Scholar]
- Anselin, L. Local indicators of spatial association-LISA. Geogr. Anal. 1995, 27, 93–115. [Google Scholar] [CrossRef]
- Hanson, C.E.; Wieczorek, W.F. Alcohol mortality: A comparison of spatial clustering methods. Soc. Sci. Med. 2002, 55, 791–802. [Google Scholar] [CrossRef]
- Nødtvedt, A.; Guitian, J.; Egenvall, A.; Emanuelson, U.; Pfeiffer, D.U. The spatial distribution of atopic dermatitis cases in a population of insured Swedish dogs. Prev. Vet. Med. 2007, 78, 210–222. [Google Scholar] [CrossRef] [PubMed]
- Naish, S.; Tong, S. Hot spot detection and spatio-temporal dynamics of dengue in Queensland, Australia. Int. Arch. Photogramm. Remote Sens. Spat. Inf. Sci. 2014, 1, 197–204. [Google Scholar] [CrossRef]
- Sasson, C.; Cudnik, M.T.; Nassel, A.; Semple, H.; Magid, D.J.; Sayre, M.; Keseg, D.; Haukoos, J.S.; Warden, C.R. Identifying high-risk geographic areas for cardiac arrest using three methods for cluster analysis. Acad. Emerg. Med. 2012, 19, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Mansoer, J.R.; Kibuga, D.K.; Borgdorff, M.W. Altitude: A determinant for tuberculosis in Kenya? Int. J. Tuberc. Lung Dis. 1999, 3, 156–161. [Google Scholar] [PubMed]
- Vargas, M.H.; Furuya, M.E.Y.; Pérez-Guzmán, C. Effect of altitude on the frequency of pulmonary tuberculosis. Int. J. Tuberc. Lung Dis. 2004, 8, 1321–1324. [Google Scholar] [PubMed]
- Vree, M.; Hoa, N.B.; Sy, D.N.; Co, N.V.; Cobelens, F.G.J.; Borgdorff, M.W. Low tuberculosis notification in mountainous Vietnam is not due to low case detection: A cross-sectional survey. BMC Infect. Dis. 2007, 7. [Google Scholar] [CrossRef] [PubMed]
- Tanrikulu, A.C.; Acemoglu, H.; Palanci, Y.; Dagli, C.E. Tuberculosis in Turkey: High altitude and other socio-economic risk factors. Public Health 2008, 122, 613–619. [Google Scholar] [CrossRef] [PubMed]
- Kakchapati, S.; Yotthanoo, S.; Choonpradup, C. Modeling tuberculosis incidence in Nepal. Asian Biomed. 2010, 4, 355–360. [Google Scholar]
- Maylan, P.R.A.; Richman, D.D.; Kornbluth, R.S. Reduced intracellular growth of mycobacteria in human macrophages cultivated at physiologic oxygen pressure. Am. Rev. Respir. Dis. 1992, 145, 947–953. [Google Scholar] [CrossRef] [PubMed]
- Eisen, S.; Pealing, L.; Aldridge, R.W.; Siedner, M.J.; Necochea, A.; Leybell, I.; Valencia, T.; Herrera, B.; Wiles, S.; Friedlan, J.S.; et al. Effects of ascent to high altitude on human antimycobacterial immunity. PLoS ONE 2013, 8. [Google Scholar] [CrossRef] [PubMed]
- Cantwell, M.F.; McKenna, M.T.; McCray, E.; Onorato, I.M. Tuberculosis and race/ethnicity in the United States: Impact of socioeconomic status. Am. J. Respir. Crit. Care Med. 1998, 157, 1016–1020. [Google Scholar] [CrossRef] [PubMed]
- Tipayamongkholgul, M.; Podang, J.; Siri, S. Spatial analysis of social determinants for tuberculosis in Thailand. J. Med. Assoc. Thai. 2013, 96, S116–S120. [Google Scholar] [PubMed]
- Erazo, C.; Pereira, S.M.; Costa, M.C.N.; Evangelista-Filho, D.; Braga, J.U.; Barreto, M.L. Tuberculosis and living conditions in Salvador, Brazil: A spatial analysis. Rev. Panam. Salud Publ. 2014, 36, 24–30. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hassarangsee, S.; Tripathi, N.K.; Souris, M. Spatial Pattern Detection of Tuberculosis: A Case Study of Si Sa Ket Province, Thailand. Int. J. Environ. Res. Public Health 2015, 12, 16005-16018. https://doi.org/10.3390/ijerph121215040
Hassarangsee S, Tripathi NK, Souris M. Spatial Pattern Detection of Tuberculosis: A Case Study of Si Sa Ket Province, Thailand. International Journal of Environmental Research and Public Health. 2015; 12(12):16005-16018. https://doi.org/10.3390/ijerph121215040
Chicago/Turabian StyleHassarangsee, Siriwan, Nitin Kumar Tripathi, and Marc Souris. 2015. "Spatial Pattern Detection of Tuberculosis: A Case Study of Si Sa Ket Province, Thailand" International Journal of Environmental Research and Public Health 12, no. 12: 16005-16018. https://doi.org/10.3390/ijerph121215040