
Caesarean Section—A Density-Equalizing Mapping Study to Depict Its Global Research Architecture

Abstract
:1. Introduction
2. Experimental Section
2.1. NewQIS Platform
2.2. Data Source
2.3. Search Strategy
2.4. Timeframe
2.5. Data Analysis and Categorization
2.6. Research Activity in Relation to Epidemiologic Data
2.7. Economic Analysis of Caesarean Section Research Activity
2.8. Analysis of Collaborations
3. Results and Discussion
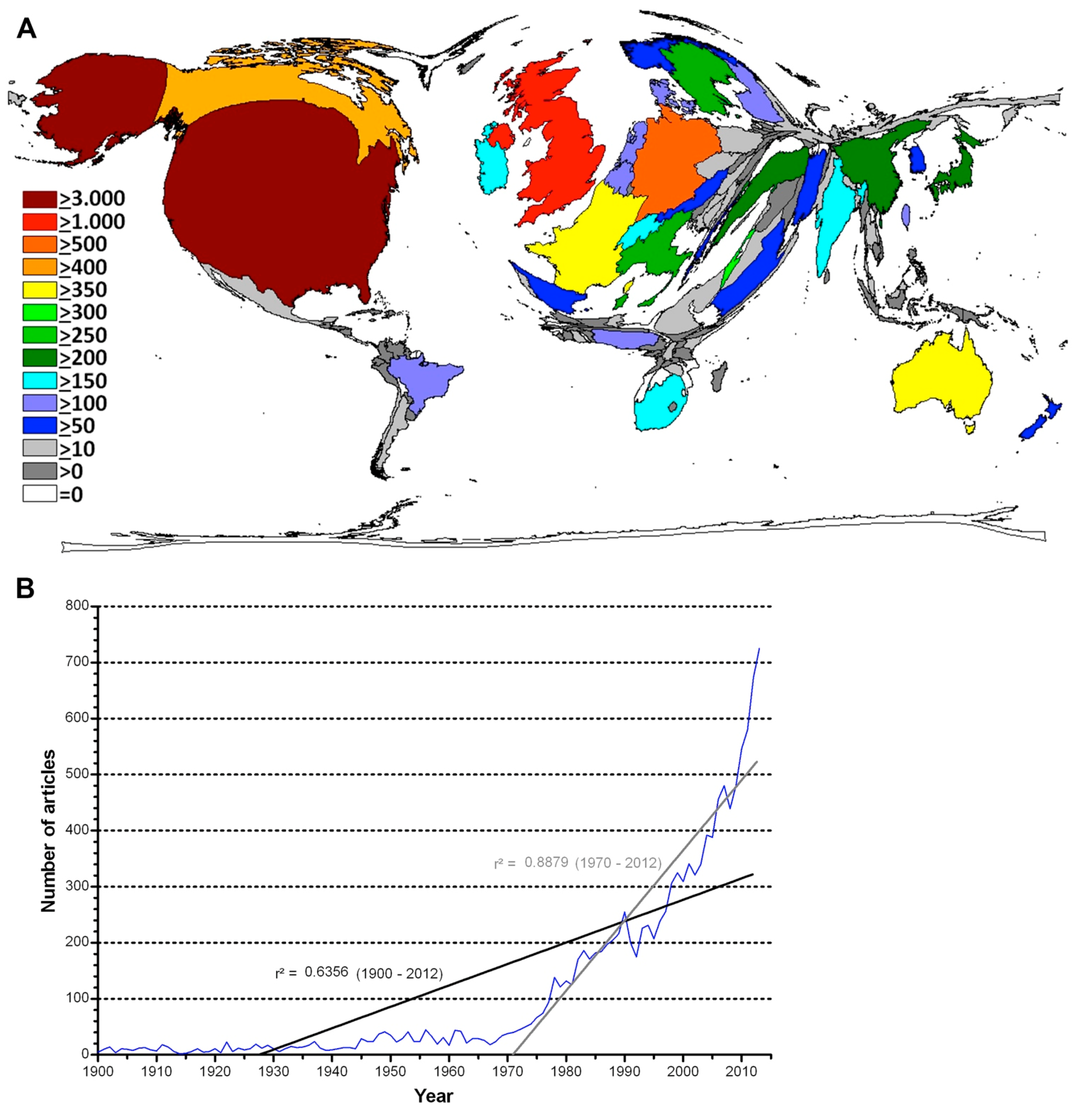
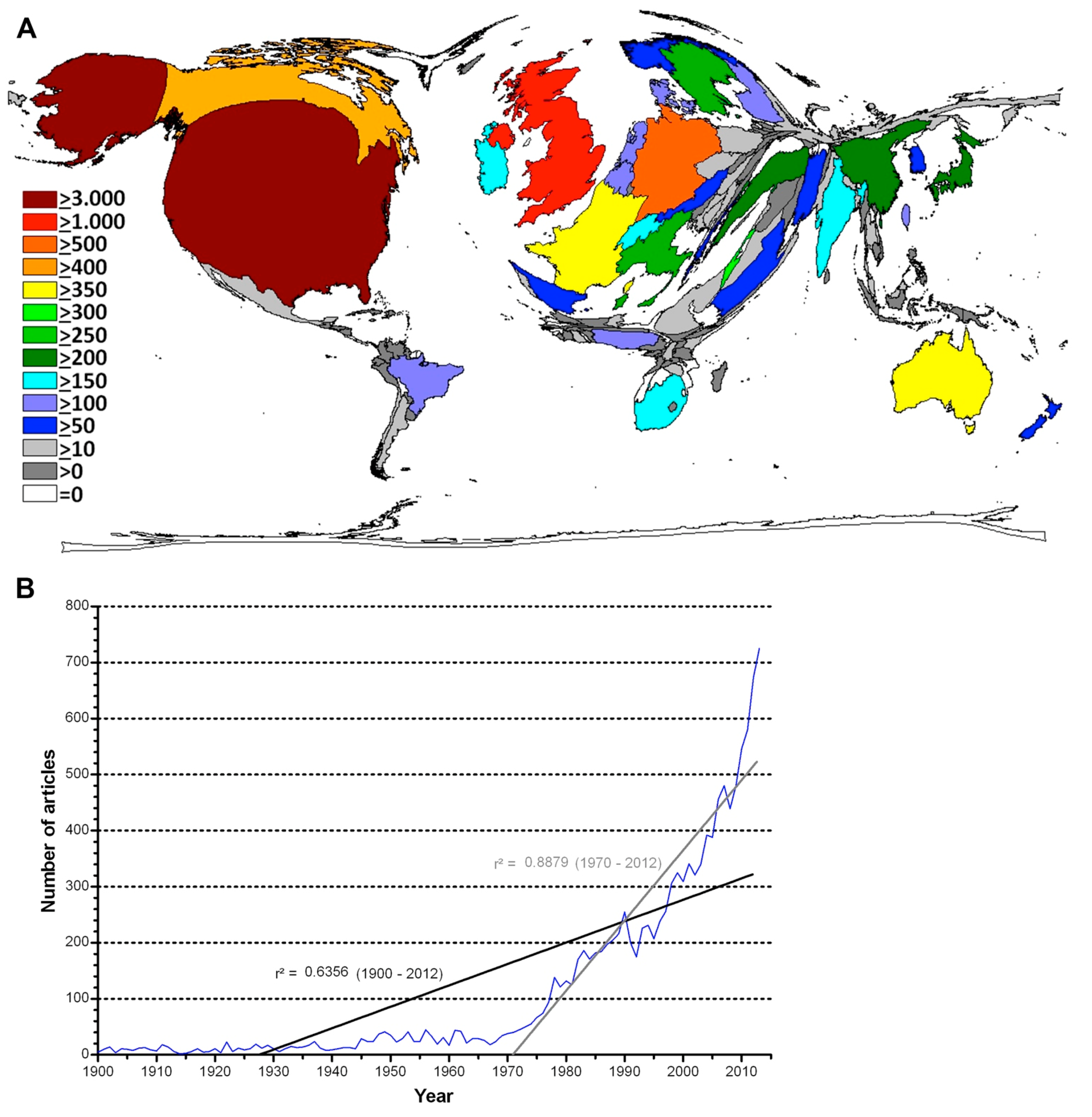
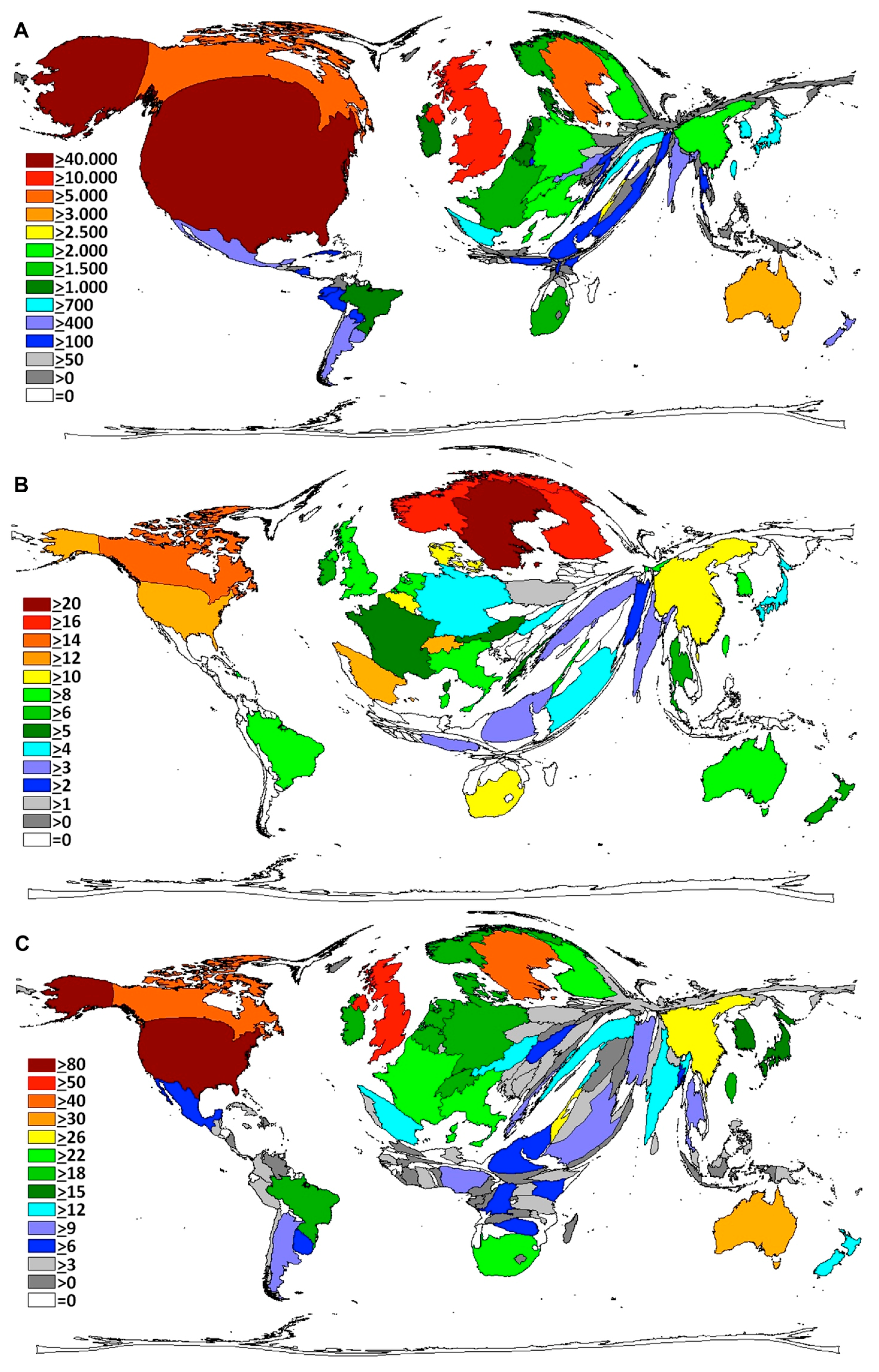
3.1. Global Caesarean Section Research Activity
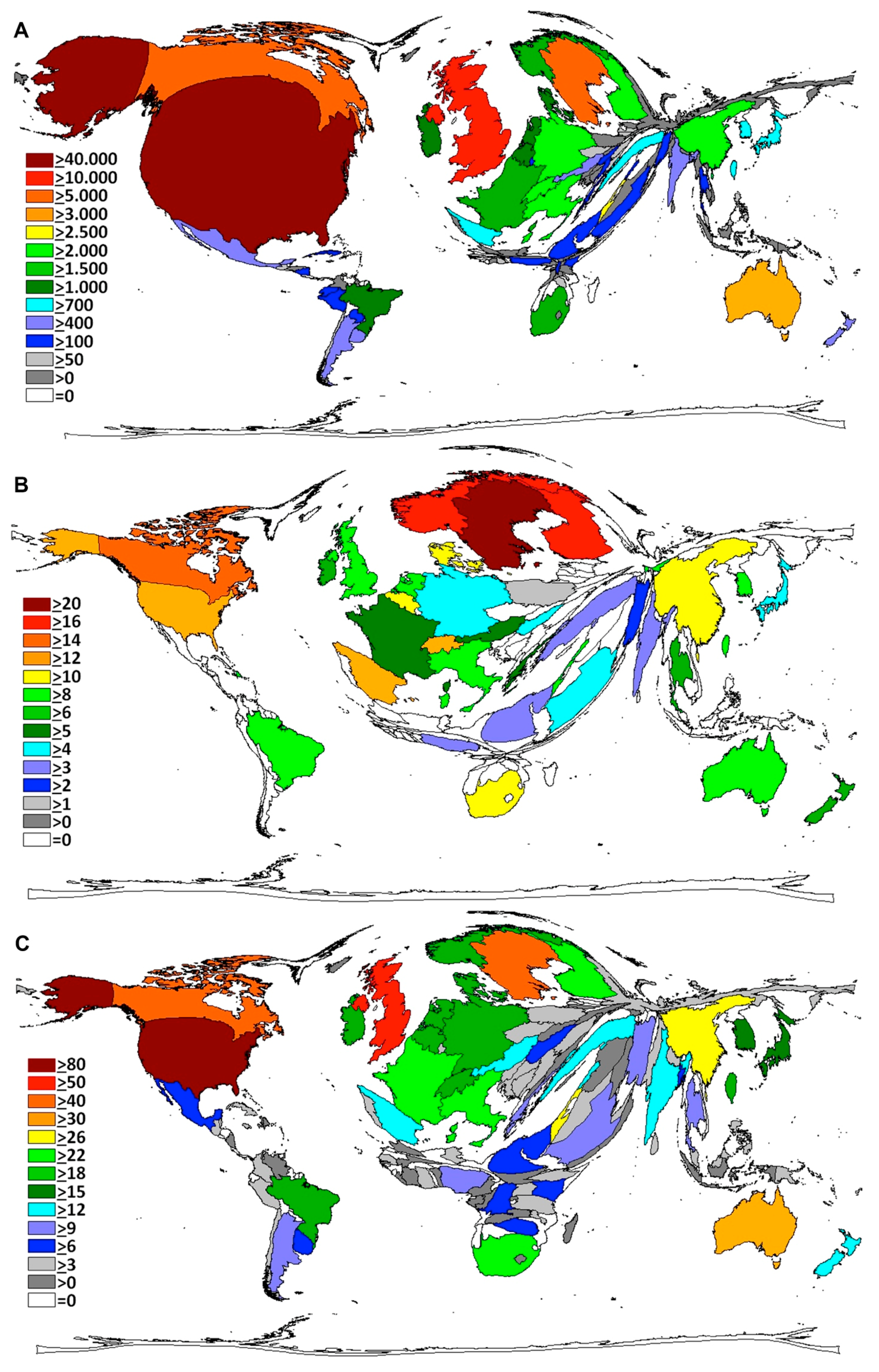
3.2. Research Activity in Relation to Caesarean Section Epidemiologic Data
3.3. Economic Analysis of Caesarean Section Research Activity

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Number of CS (in Thousands) | Number of Publications | Number of Publications/Number of CS (per 1000 CS) | Type of Country Based on GNI | |
|---|---|---|---|---|---|
| 1. | Sweden | 18.51 | 251 | 13.56 | HIG |
| 2. | Finland | 9.62 | 125 | 13.00 | HIG |
| 3. | Israel | 26.74 | 313 | 11.71 | HIG |
| 4. | Ireland | 18.08 | 191 | 10.57 | HIG |
| 5. | United Kingdom | 163.46 | 1712 | 10.47 | HIG |
| 6. | Norway | 9.63 | 93 | 9.66 | HIG |
| 7. | Denmark | 13.27 | 116 | 8.74 | HIG |
| 8. | Switzerland | 21.10 | 155 | 7.35 | HIG |
| 9. | Belgium | 18.92 | 120 | 6.34 | HIG |
| 10. | Netherlands | 24.98 | 136 | 5.45 | HIG |
| 11. | Canada | 92.84 | 491 | 5.29 | HIG |
| 12. | New Zealand | 11.83 | 59 | 4.99 | HIG |
| 13. | Australia | 80.90 | 373 | 4.61 | HIG |
| 14. | Austria | 20.60 | 82 | 3.98 | HIG |
| 15. | United States | 1332.90 | 3679 | 2.76 | HIG |
| 16. | Germany | 185.15 | 506 | 2.73 | HIG |
| 17. | France | 141.38 | 352 | 2.49 | HIG |
| 18. | Italy | 208.57 | 292 | 1.40 | HIG |
| 19. | Japan | 179.92 | 220 | 1.22 | HIG |
| 20. | Nigeria | 108.50 | 101 | 0.93 | LMIG |
| 21. | Saudi Arabia | 76.83 | 66 | 0.86 | HIG |
| 22. | South Africa | 224.75 | 189 | 0.84 | UMIG |
| 23. | Turkey | 285.78 | 221 | 0.77 | UMIG |
| 24. | Spain | 127.17 | 74 | 0.58 | HIG |
| 25. | Republic of Korea | 170.40 | 86 | 0.50 | HIG |
| 26. | Iran | 581.57 | 83 | 0.14 | UMIG |
| 27. | Brazil | 1425.20 | 132 | 0.09 | UMIG |
| 28. | India | 2287.61 | 176 | 0.08 | LMIG |
| 29. | China | 4696.71 | 217 | 0.05 | UMIG |
| Country | Number of Publications | GDP Current USD | Number of Publications/GDP * 100,000,000 Current USD | Type of Country Based on GNI | |
|---|---|---|---|---|---|
| 1. | Israel | 313 | 2.90551E+11 | 107.7265027 | HIG |
| 2. | Ireland | 191 | 2.32077E+11 | 82.30012236 | HIG |
| 3. | United Kingdom | 1712 | 2.67845E+12 | 63.91744765 | HIG |
| 4. | South Africa | 189 | 3.66058E+11 | 51.63117449 | UMIG |
| 5. | Finland | 125 | 2.67329E+11 | 46.75893024 | HIG |
| 6. | Sweden | 251 | 5.7968E+11 | 43.29975268 | HIG |
| 7. | Denmark | 116 | 3.35878E+11 | 34.53639595 | HIG |
| 8. | New Zealand | 59 | 1.85788E+11 | 31.75665583 | HIG |
| 9. | Turkey | 221 | 8.22135E+11 | 26.88122398 | UMIG |
| 10. | Canada | 491 | 1.82677E+12 | 26.87806272 | HIG |
| 11. | Australia | 373 | 1.56037E+12 | 23.90454884 | HIG |
| 12. | Belgium | 120 | 5.24806E+11 | 22.86561292 | HIG |
| 13. | Switzerland | 155 | 6.85434E+11 | 22.61340379 | HIG |
| 14. | Iran | 83 | 3.68904E+11 | 22.49905691 | UMIG |
| 15. | United States | 3679 | 1.67681E+13 | 21.9404703 | HIG |
| 16. | Nigeria | 101 | 5.21803E+11 | 19.35595217 | LMIG |
| 17. | Austria | 82 | 4.28322E+11 | 19.14447999 | HIG |
| 18. | Norway | 93 | 5.1258E+11 | 18.14349424 | HIG |
| 19. | Netherlands | 136 | 8.53539E+11 | 15.93365317 | HIG |
| 20. | Italy | 292 | 2.14948E+12 | 13.5846524 | HIG |
| 21. | Germany | 506 | 3.73026E+12 | 13.56473604 | HIG |
| 22. | France | 352 | 2.80643E+12 | 12.54263436 | HIG |
| 23. | India | 176 | 1.87514E+12 | 9.38595843 | LMIG |
| 24. | Saudi Arabia | 66 | 7.4845E+11 | 8.818229043 | HIG |
| 25. | Republic of Korea | 86 | 1.30455E+12 | 6.592291451 | HIG |
| 26. | Brazil | 132 | 2.24567E+12 | 5.877970573 | UMIG |
| 27. | Spain | 74 | 1.39304E+12 | 5.312122451 | HIG |
| 28. | Japan | 220 | 4.91956E+12 | 4.47194182 | HIG |
| 29. | China | 217 | 9.24027E+12 | 2.348416111 | UMIG |
| Country | Number of Publications | GDP per Capita Current 1000 USD | Number of Publications/ GDP per Capita Current 1000 USD | |
|---|---|---|---|---|
| 1. | United States | 3679 | 53.042 | 69.36012971 |
| 2. | United Kingdom | 1712 | 41.7811 | 40.97546498 |
| 3. | Germany | 506 | 46.2514 | 10.94020938 |
| 4. | Canada | 491 | 51.9643 | 9.448794653 |
| 5. | Israel | 313 | 36.0507 | 8.682216989 |
| 6. | France | 352 | 42.5604 | 8.270598961 |
| 7. | Italy | 292 | 35.6856 | 8.182572242 |
| 8. | Japan | 220 | 38.6337 | 5.694510233 |
| 9. | Australia | 373 | 67.463 | 5.528956613 |
| 10. | Sweden | 251 | 60.3809 | 4.156943669 |
| 11. | Ireland | 191 | 50.4784 | 3.783796634 |
| 12. | Republic of Korea | 86 | 25.977 | 3.310620934 |
| 13. | Netherlands | 136 | 50.7925 | 2.677560663 |
| 14. | Belgium | 120 | 46.9296 | 2.557021581 |
| 15. | Finland | 125 | 49.1506 | 2.543203949 |
| 16. | Saudi Arabia | 66 | 25.9618 | 2.542196612 |
| 17. | Spain | 74 | 29.8821 | 2.476398914 |
| 18. | Denmark | 116 | 59.8186 | 1.93919617 |
| 19. | Switzerland | 155 | 84.7484 | 1.828943083 |
| 20. | Austria | 82 | 50.5107 | 1.623418404 |
| 21. | New Zealand | 59 | 41.8243 | 1.410663179 |
| 22. | Norway | 93 | 100.8984 | 0.921719274 |
3.4. Citation Analysis
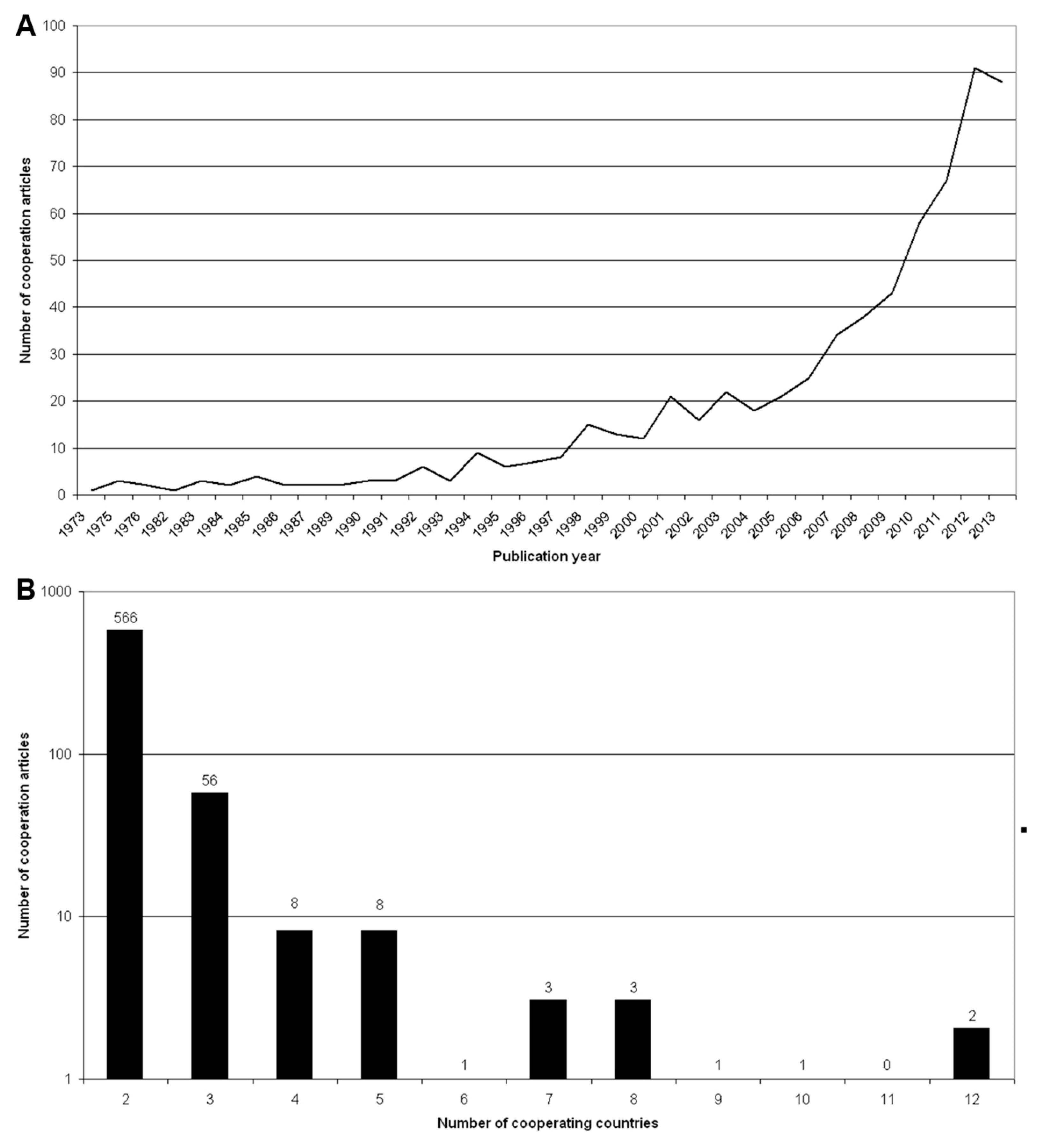
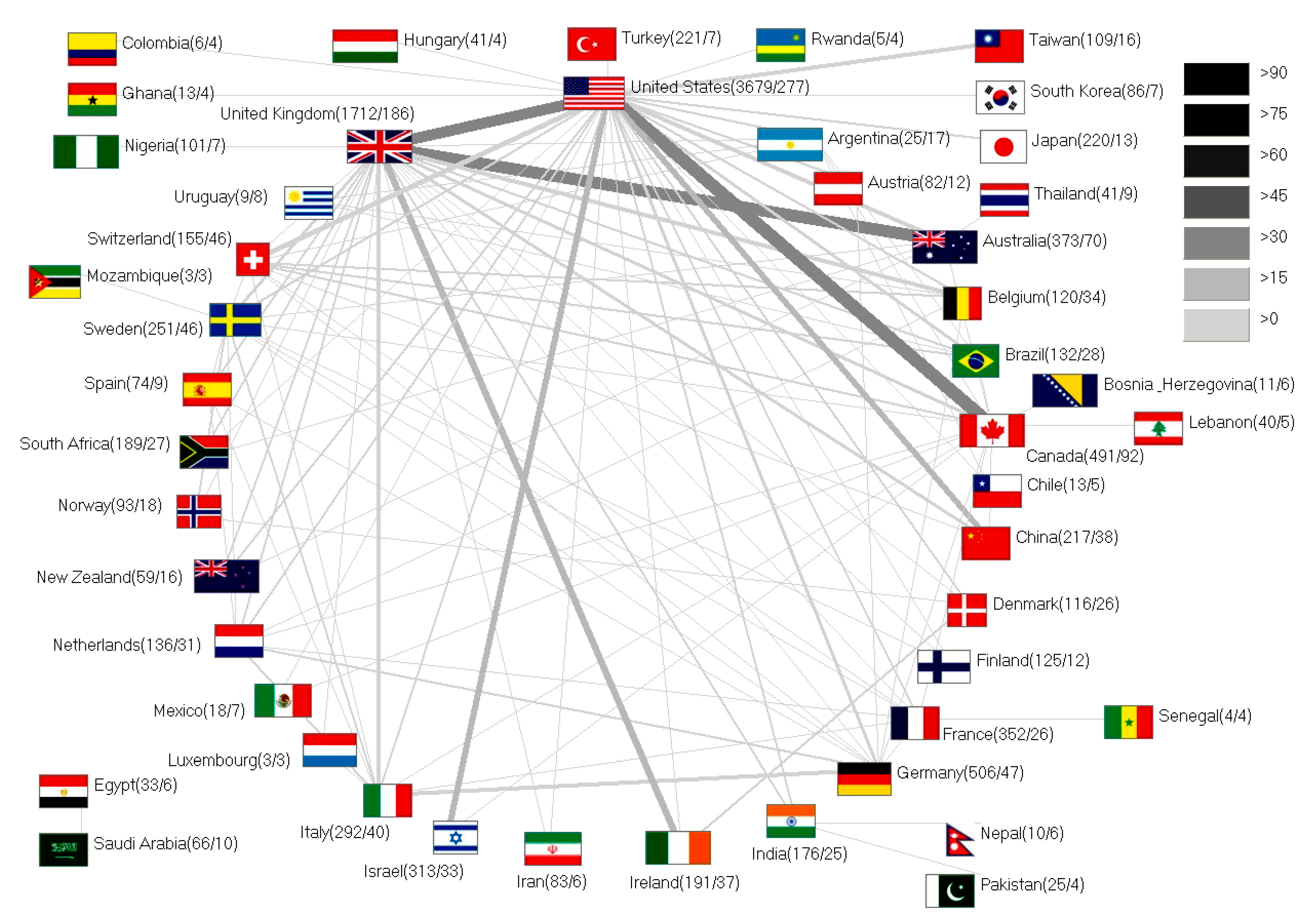
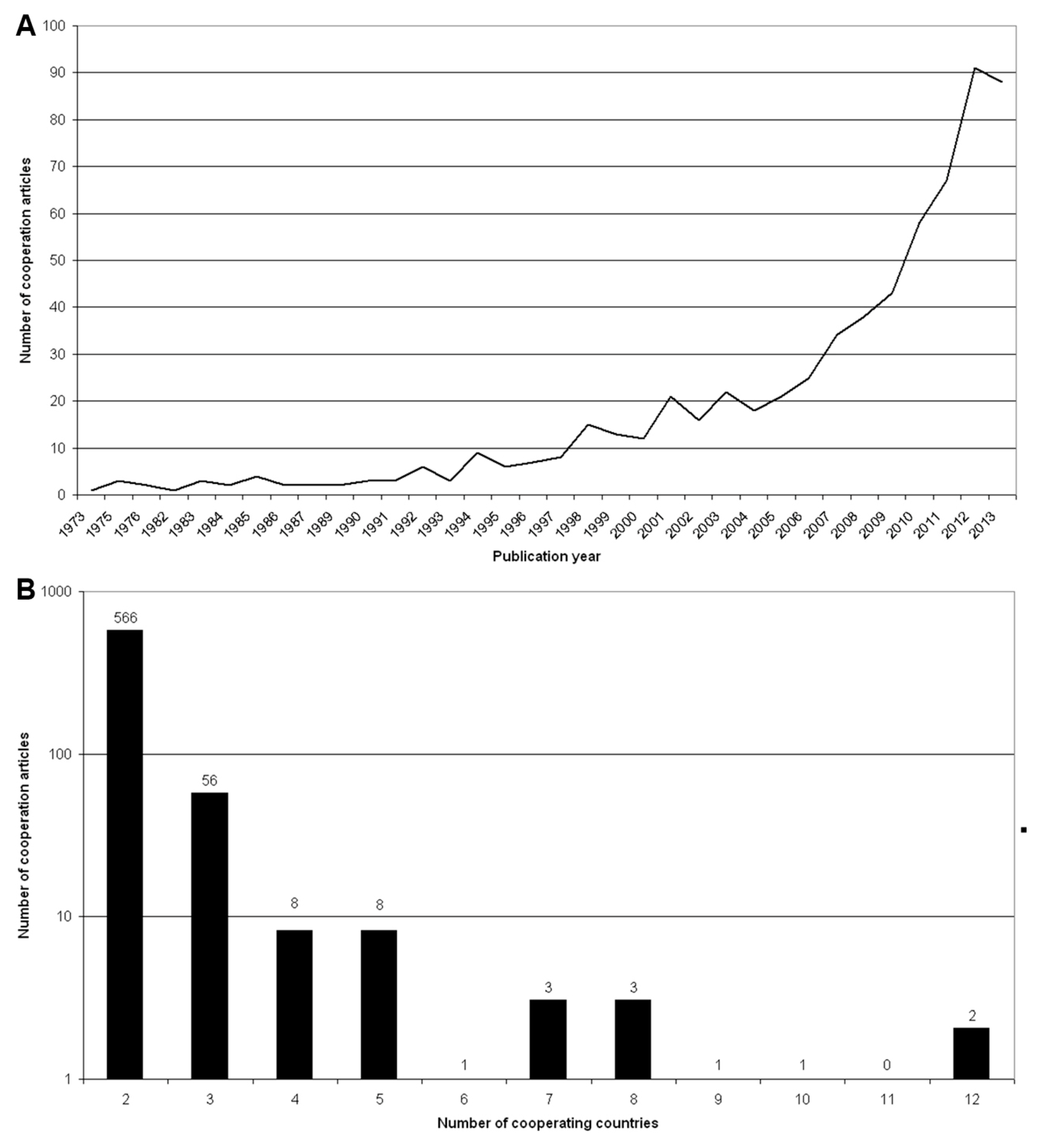
3.5. International Collaboration Analysis

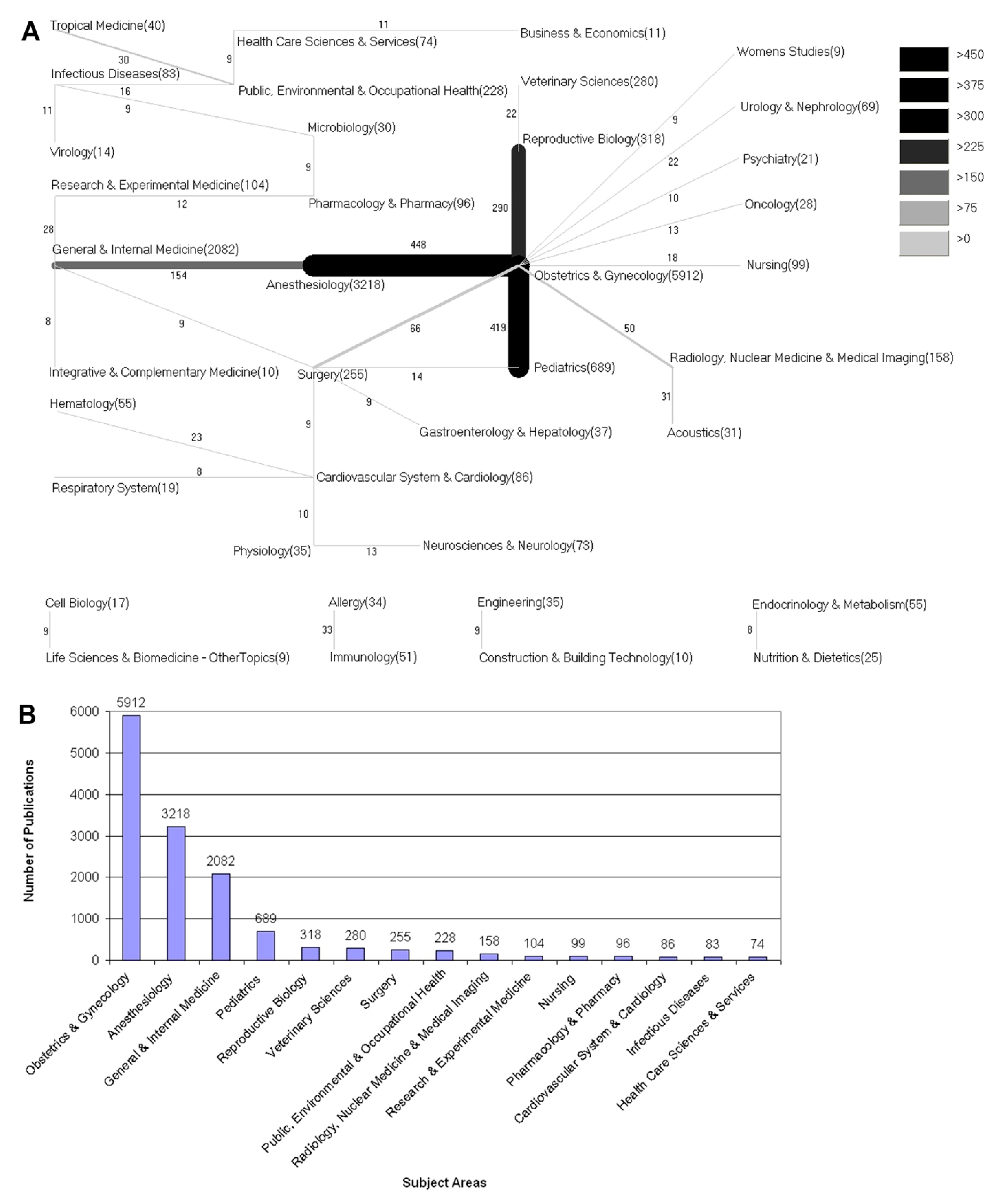
3.6. Subject Area Analysis
3.7. Discussion

4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- O’Neill, S.M.; Kearney, P.M.; Kenny, L.C.; Henriksen, T.B.; Lutomski, J.E.; Greene, R.A.; Khashan, A.S. Caesarean delivery and subsequent pregnancy interval: A systematic review and meta-analysis. BMC Pregnancy Childbirth 2013, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, M.M.; Hancock, H. Women’s knowledge of options for birth after caesarean section. Women Birth 2012, 25, e19–e26. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.A.; Hamilton, B.E.; Osterman, M.J.; Curtin, S.C.; Matthews, T.J. Births: Final data for 2013. Natl. Vital Stat. Rep. 2015, 64, 1–65. [Google Scholar] [PubMed]
- Declercq, E.; Young, R.; Cabral, H.; Ecker, J. Is a rising cesarean delivery rate inevitable? Trends in industrialized countries, 1987 to 2007. Birth 2011, 38, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.A.; Hamilton, B.E.; Ventura, S.J.; Osterman, M.J.; Kirmeyer, S.; Mathews, T.J.; Wilson, E.C. Births: Final data for 2009. Natl. Vital Stat. Rep. 2011, 60, 1–70. [Google Scholar] [PubMed]
- WHO. Appropriate technology for birth. Lancet 1985, 326, 436–437. [Google Scholar] [CrossRef]
- Boley, J.P. The history of caesarean section. Can. Med. Assoc. J. 1935, 32, 557–559. [Google Scholar] [PubMed]
- Smith, P.W.; Watkins, K.; Hewlett, A. Infection control through the ages. Am. J. Infect. Control 2012, 40, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Solheim, K.N.; Esakoff, T.F.; Little, S.E.; Cheng, Y.W.; Sparks, T.N.; Caughey, A.B. The effect of cesarean delivery rates on the future incidence of placenta previa, placenta accreta, and maternal mortality. J. Matern.Fetal Neonatal Med. 2011, 24, 1341–1346. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, S.M.; Agerbo, E.; Kenny, L.C.; Henriksen, T.B.; Kearney, P.M.; Greene, R.A.; Mortensen, P.B.; Khashan, A.S. Cesarean section and rate of subsequent stillbirth, miscarriage, and ectopic pregnancy: A danish register-based cohort study. PLoS Med. 2014, 11. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, S.M.; Kearney, P.M.; Kenny, L.C.; Khashan, A.S.; Henriksen, T.B.; Lutomski, J.E.; Greene, R.A. Caesarean delivery and subsequent stillbirth or miscarriage: Systematic review and meta-analysis. PLoS ONE 2013, 8. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, K.; Henriksen, L. Cesarean section and disease associated with immune function. J. Allergy Clin. Immunol. 2015. [Google Scholar] [CrossRef] [PubMed]
- Sevelsted, A.; Stokholm, J.; Bonnelykke, K.; Bisgaard, H. Cesarean section and chronic immune disorders. Obstet. Gynecol. Surv. 2015, 70, 303–305. [Google Scholar] [CrossRef]
- Almqvist, C.; Cnattingius, S.; Lichtenstein, P.; Lundholm, C. The impact of birth mode of delivery on childhood asthma and allergic diseases—A sibling study. Clinical Experiment. Allergy 2012, 42, 1369–1376. [Google Scholar] [CrossRef] [PubMed]
- Curran, E.A.; Dalman, C.; Kearney, P.M.; Kenny, L.C.; Cryan, J.F.; Dinan, T.G.; Khashan, A.S. Association between obstetric mode of delivery and autism spectrum disorder: A population-based sibling design study. JAMA Psych. 2015, 72, 935–942. [Google Scholar] [CrossRef] [PubMed]
- Khashan, A.S.; Kenny, L.C.; Lundholm, C.; Kearney, P.M.; Gong, T.; Almqvist, C. Mode of obstetrical delivery and type 1 diabetes: A sibling design study. Pediatrics 2014, 134, E806–E813. [Google Scholar] [CrossRef] [PubMed]
- Samuelsson, U.; Lindell, N.; Bladh, M.; Akesson, K.; Carlsson, A.; Josefsson, A. Caesarean section per se does not increase the risk of offspring developing type 1 diabetes: A Swedish population-based study. Diabetologia 2015, 58, 2517–2524. [Google Scholar] [CrossRef] [PubMed]
- Stene, L.C.; Magnus, P.; Lie, R.T.; Sovik, O.; Joner, G.; Study, N.C.D. No association between preeclampsia or cesarean section and incidence of type 1 diabetes among children: A large, population-based cohort study. Pediatr. Res. 2003, 54, 487–490. [Google Scholar] [CrossRef] [PubMed]
- Groneberg-Kloft, B.; Quarcoo, D.; Scutaru, C. Quality and quantity indices in science: Use of visualization tools. EMBO Rep. 2009, 10, 800–803. [Google Scholar] [CrossRef] [PubMed]
- Groneberg-Kloft, B.; Fischer, T.C.; Quarcoo, D.; Scutaru, C. New quality and quantity indices in science (NewQIS): The study protocol of an international project. J. Occup. Med. Toxicol. 2009, 4. [Google Scholar] [CrossRef] [PubMed]
- Gastner, M.T.; Newman, M.E. Diffusion-based method for producing density-equalizing maps. Proc. Natl. Acad. Sci. USA 2004, 101, 7499–7504. [Google Scholar] [CrossRef] [PubMed]
- Groneberg, D.A.; Schilling, U.; Scutaru, C.; Uibel, S.; Zitnik, S.; Mueller, D.; Klingelhoefer, D.; Kloft, B. Drowning—A scientometric analysis and data acquisition of a constant global problem employing density equalizing mapping and scientometric benchmarking procedures. Int. J. Health Geogr. 2011, 10. [Google Scholar] [CrossRef] [PubMed]
- Groneberg-Kloft, B.; Klingelhoefer, D.; Zitnik, S.E.; Scutaru, C. Traffic medicine-related research: A scientometric analysis. BMC Public Health 2013, 13. [Google Scholar] [CrossRef] [PubMed]
- Groneberg-Kloft, B.; Scutaru, C.; Kreiter, C.; Kolzow, S.; Fischer, A.; Quarcoo, D. Institutional operating figures in basic and applied sciences: Scientometric analysis of quantitative output benchmarking. Health Res. Policy Syst. 2008, 6. [Google Scholar] [CrossRef] [PubMed]
- Borger, J.A.; Neye, N.; Scutaru, C.; Kreiter, C.; Puk, C.; Fischer, T.C.; Groneberg-Kloft, B. Models of asthma: Density-equalizing mapping and output benchmarking. J. Occup. Med. Toxicol. 2008, 3 (Suppl. 1). [Google Scholar] [CrossRef] [PubMed]
- Groneberg-Kloft, B.; Scutaru, C.; Fischer, A.; Welte, T.; Kreiter, C.; Quarcoo, D. Analysis of research output parameters: Density equalizing mapping and citation trend analysis. BMC Health Serv. Res. 2009, 9. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, S.; Bundschuh, M.; Scutaru, C.; Klingelhoefer, D.; Groneberg, D.A.; Gerber, A. Hepatitis B: Global scientific development from a critical point of view. J. Viral Hepat. 2013, 21, 786–793. [Google Scholar] [CrossRef] [PubMed]
- Pleger, N.; Kloft, B.; Quarcoo, D.; Zitnik, S.; Mache, S.; Klingelhoefer, D.; Groneberg, D.A. Bacterial meningitis: A density-equalizing mapping analysis of the global research architecture. Int. J. Environ. Res. Public Health 2014, 11, 10202–10214. [Google Scholar] [CrossRef] [PubMed]
- Gerber, A.; Klingelhoefer, D.; Groneberg, D.A.; Bundschuh, M. Silicosis: Geographic changes in research: An analysis employing density-equalizing mapping. J. Occup. Med. Toxicol. 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- Gerber, A.; Groneberg, D.A.; Klingelhofer, D.; Bundschuh, M. Gout: A critical analysis of scientific development. Rheumatol. Int. 2013, 33, 2743–2750. [Google Scholar] [CrossRef] [PubMed]
- Gibbons, L.; Belizan, J.; Lauer, J.; Betran, A.; Merialdi, M.; Althabe, F. The global numbers and costs of additionally needed and unnecessary caesarean sections performed per year: Overuse as a barrier to universal coverage. World Health Rep. 2010, 30, 1–31. [Google Scholar]
- Bundschuh, M.; Groneberg, D.A.; Klingelhoefer, D.; Gerber, A. Yellow fever disease: Density equalizing mapping and gender analysis of international research output. Parasit. Vect. 2013, 6. [Google Scholar] [CrossRef] [PubMed]
- Vogel, J.P.; Betran, A.P.; Vindevoghel, N.; Souza, J.P.; Torloni, M.R.; Zhang, J.; Tuncalp, O.; Mori, R.; Morisaki, N.; Ortiz-Panozo, E.; et al. Use of the Robson classification to assess caesarean section trends in 21 countries: A secondary analysis of two WHO multicountry surveys. Lancet. Glob. Health 2015, 3, e260–e270. [Google Scholar] [CrossRef]
- Mund, M.; Kloft, B.; Bundschuh, M.; Klingelhoefer, D.; Groneberg, D.A.; Gerber, A. Global research on smoking and pregnancy—A scientometric and gender analysis. Int. J. Environ. Res. Public Health 2014, 11, 5792–5806. [Google Scholar] [CrossRef] [PubMed]
- Glynn, R.W.; Scutaru, C.; Kerin, M.J.; Sweeney, K.J. Breast cancer research output, 1945–2008: A bibliometric and density-equalizing analysis. Breast Cancer Res. 2010, 12. [Google Scholar] [CrossRef] [PubMed]
- Sachs, B. P.; Kobelin, C.; Castro, M. A.; Frigoletto, F. The risks of lowering the cesarean-delivery rate. New England J. Med. 1999, 340, 54–57. [Google Scholar] [CrossRef] [PubMed]
- Wagner, M. Fish can’t see water: The need to humanize birth. Int. J. Gynaecol. Obstetr. 2001, 75 (Suppl 1), S25–S37. [Google Scholar] [CrossRef]
- Belizan, J.M.; Althabe, F.; Cafferata, M.L. Health consequences of the increasing caesarean section rates. Epidemiology 2007, 18, 485–486. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brüggmann, D.; Löhlein, L.-K.; Louwen, F.; Quarcoo, D.; Jaque, J.; Klingelhöfer, D.; Groneberg, D.A. Caesarean Section—A Density-Equalizing Mapping Study to Depict Its Global Research Architecture. Int. J. Environ. Res. Public Health 2015, 12, 14690-14708. https://doi.org/10.3390/ijerph121114690
Brüggmann D, Löhlein L-K, Louwen F, Quarcoo D, Jaque J, Klingelhöfer D, Groneberg DA. Caesarean Section—A Density-Equalizing Mapping Study to Depict Its Global Research Architecture. International Journal of Environmental Research and Public Health. 2015; 12(11):14690-14708. https://doi.org/10.3390/ijerph121114690
Chicago/Turabian StyleBrüggmann, Dörthe, Lena-Katharina Löhlein, Frank Louwen, David Quarcoo, Jenny Jaque, Doris Klingelhöfer, and David A. Groneberg. 2015. "Caesarean Section—A Density-Equalizing Mapping Study to Depict Its Global Research Architecture" International Journal of Environmental Research and Public Health 12, no. 11: 14690-14708. https://doi.org/10.3390/ijerph121114690