
Ambulatory Care Visits to Pediatricians in Taiwan: A Nationwide Analysis


Abstract
:1. Introduction
2. Methods
2.1. Database
2.2. Study Population
2.3. Statistical Analysis
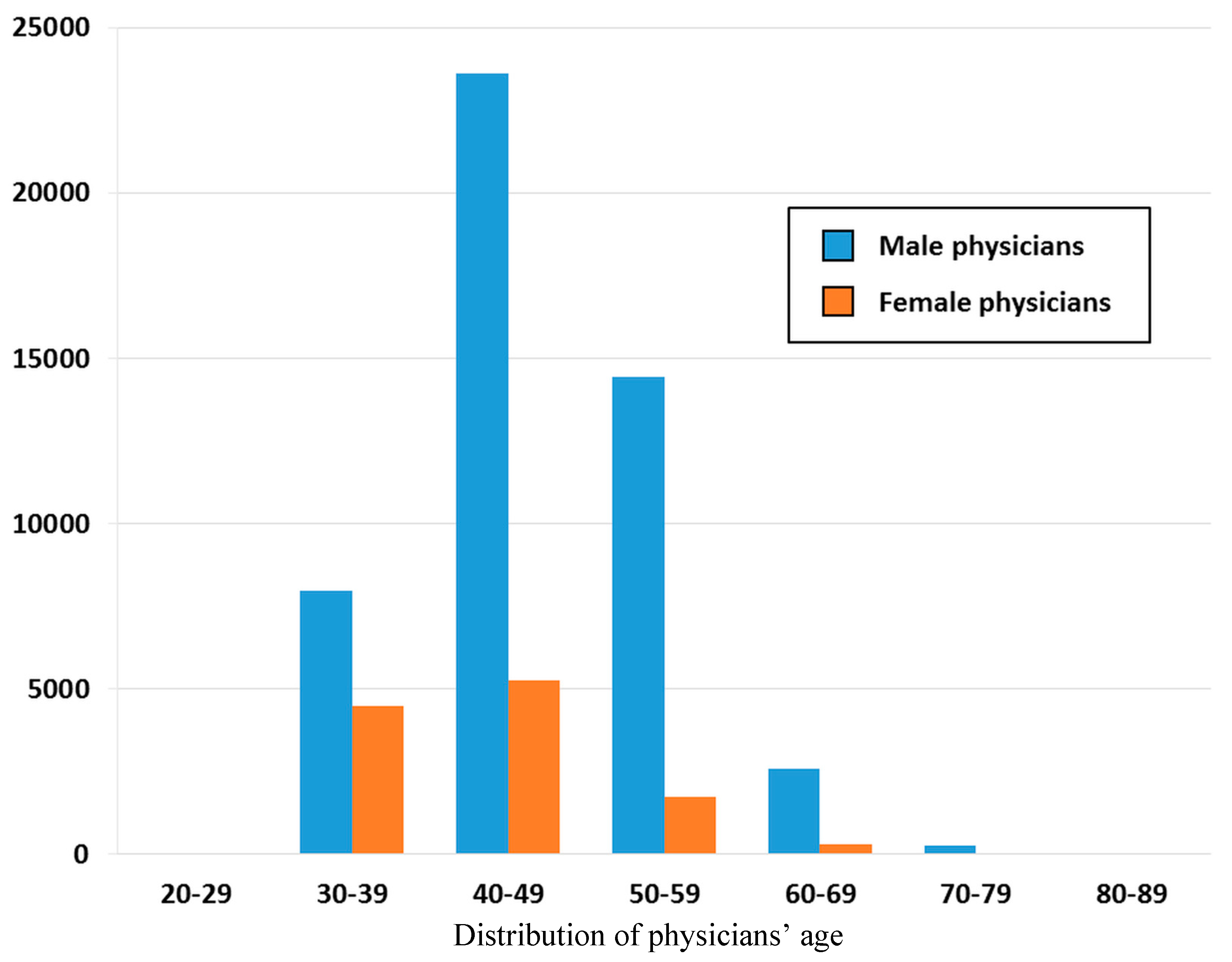
3. Results

{kind=link}
{kind=link}
{kind=link}
| Specialty | Number of Visits (%) | Cost Claimed (%) | Average Cost Claimed per Visit |
|---|---|---|---|
| Family medicine | 116,551 (18.8) | 51,157,561 (8.3) | 439 |
| Internal medicine | 70,615 (11.4) | 42,547,879 (6.9) | 602 |
| Otorhinolaryngology | 67,881 (11.0) | 29,718,395 (4.8) | 438 |
| Pediatrics | 60,717 (9.8) | 31,574,986 (5.1) | 520 |
| Ophthalmology | 37,692 (6.1) | 25,422,291 (4.1) | 674 |
| Obstetrics& Gynecology | 35,697 (5.8) | 19,674,700 (3.2) | 551 |
| Others | 230,607 (37.2) | 418,023,780 (67.6) | 1813 |
| Total | 619,760 (100.0) * | 618,119,592 (100.0) | 997 |

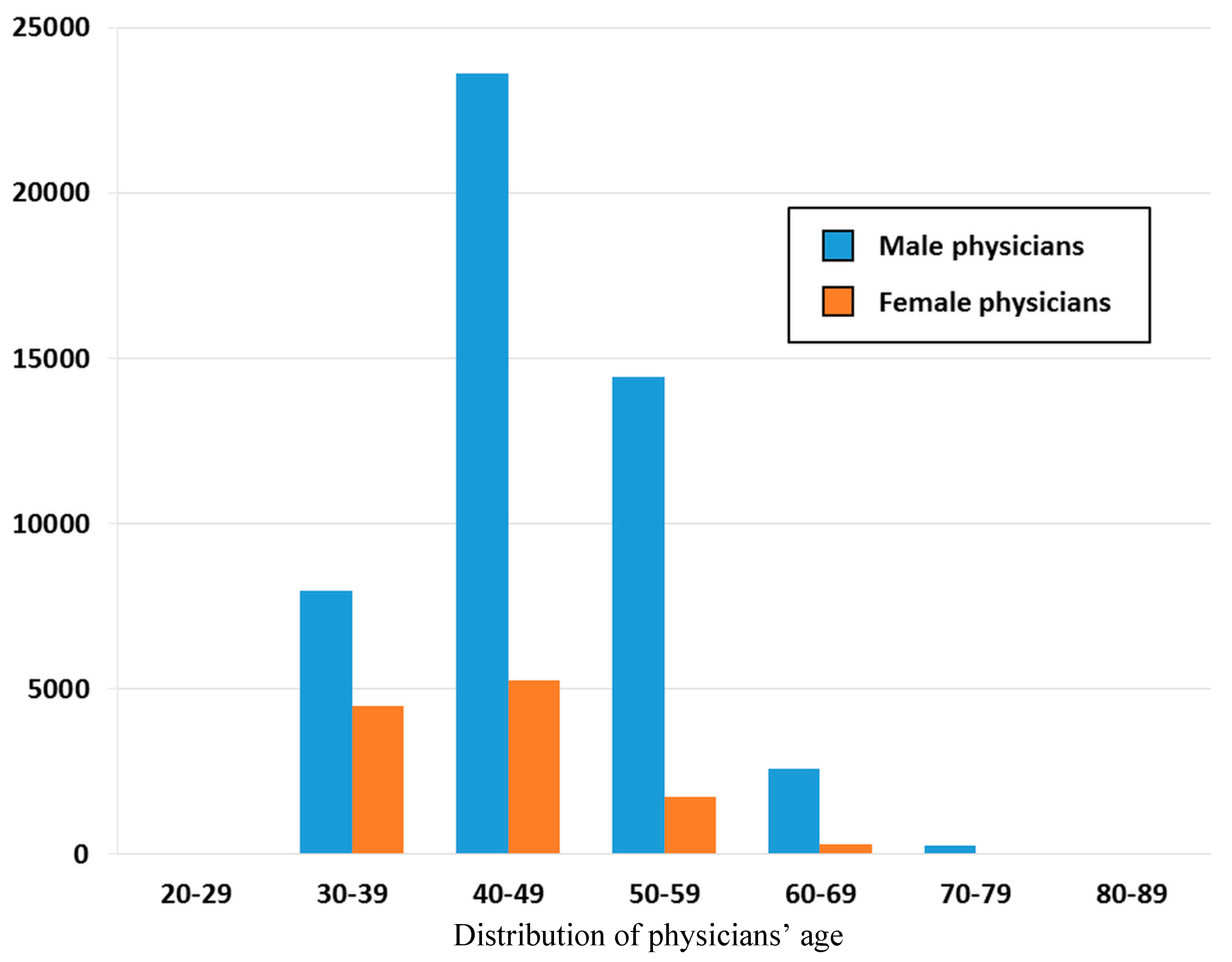
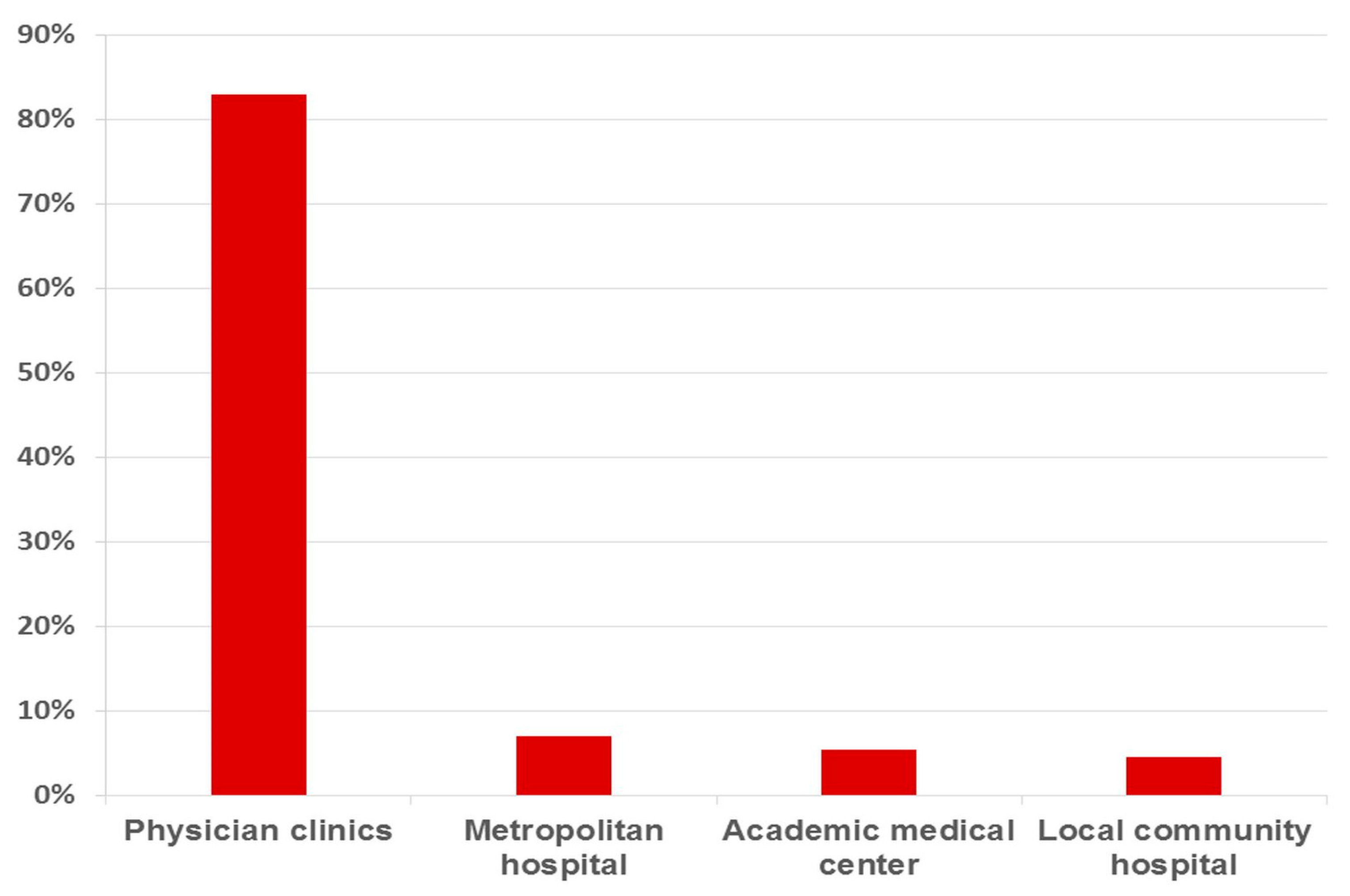
| Facility Level | 20–29 Years | 30–39 Years | 40–49 Years | 50–59 Years | 60–69 Years | 70–79 Years | 80–89 Years | Total |
|---|---|---|---|---|---|---|---|---|
| Physician clinics | 20 | 9538 | 24,559 | 13,758 | 2307 | 251 | 12 | 50,448 * |
| Local community hospital | 3 | 827 | 1223 | 578 | 167 | 25 | 2 | 2825 |
| Metropolitan hospital | 7 | 1525 | 1755 | 734 | 171 | 0 | 2 | 4194 |
| Academic medical center | 21 | 545 | 1321 | 1104 | 240 | 19 | 0 | 3250 |
| Total | 51 | 12,435 | 28,858 | 16,174 | 2885 | 295 | 16 | 60,717 |
| ICD9CM * | Diagnosis Group | Total N = 60,717 | Academic Medical Center N = 3250 | Metropolitan Hospital N = 4194 | Local Community Hospital N = 2825 | Physicians Clinics N = 50,448 |
|---|---|---|---|---|---|---|
| 465 | Acute upper respiratory infections | 13,461 (22.2) | 104 (0.2) | 287 (0.5) | 271 (0.5) | 12,799 (21.0) |
| 466 | Acute bronchitis & bronchiolitis | 7041 (11.6) | 121 (0.2) | 469 (0.8) | 348 (0.6) | 6103 (10.1) |
| 461 | Acute sinusitis | 3072 (5.1) | 58 (0.1) | 120 (0.2) | 86 (0.1) | 2808 (4.6) |
| 463 | Acute tonsilitis | 3030 (5.0) | 37 (0.1) | 163 (0.3) | 112 (0.2) | 2718 (4.5) |
| 460 | Acute nasopharyngitis | 2597 (4.3) | 13 (0.0) ** | 34 (0.1) | 33 (0.1) | 2517 (4.1) |
| 462 | Acute pharyngitis | 2580 (4.2) | 52 (0.1) | 118 (0.2) | 146 (0.2) | 2264 (3.7) |
| 558 | Other noninfectious gastroenteritis and colitis | 2032 (3.3) | 58 (0.1) | 120 (0.2) | 61 (0.1) | 1793 (2.9) |
| 464 | Acute laryngitis & tracheitis | 1688 (2.8) | 9 (0.0) ** | 20 (0.0) ** | 17 (0.0) ** | 1642 (2.7) |
| V20 | Health supervision of infant or child | 1644 (2.7) | 121 (0.2) | 239 (0.4) | 301 (0.5) | 983 (1.6) |
| 780 | Non-specific symptoms | 1544 (2.5) | 68 (0.1) | 170 (0.3) | 94 (0.2) | 1212 (2.0) |
| NHI Code * | Procedure | No. of Visits | % |
|---|---|---|---|
| 32001C | Chest view (including each view of chest film) | 425 | 0.7% |
| 08001C | Complete blood count | 404 | 0.7% |
| 57021C | Humidity or aerosol therapy- time | 383 | 0.6% |
| 08013C | White blood cell differential count | 374 | 0.6% |
| 06012C | General urine examination | 304 | 0.5% |
| 09026C | S-GPT/ALT | 225 | 0.4% |
| 09005C | Blood glucose | 212 | 0.3% |
| 57110C | Blood sampling | 208 | 0.3% |
| 18007B | Doppler color flow mapping | 178 | 0.3% |
| 09015C | Serum creatinine | 176 | 0.3% |
| ATC Code * | Drug Classification | No. of Visits | % |
|---|---|---|---|
| R06A | Antihistamines for systemic use | 29,608 | 48.8 |
| R05C | Expectorants | 19,457 | 32.0 |
| R05D | Cough suppressants | 16,091 | 26.5 |
| M01A | Anti-inflammatory, non-steroids | 15,003 | 24.7 |
| R03C | Adrenergics for systemic use | 14,865 | 24.5 |
| N02B | Other analgesics and antipyretics | 14,021 | 23.1 |
| R01B | Nasal decongestants for systemic use | 11,451 | 18.9 |
| R05F | Cough suppressants & expectorants combinations | 9142 | 15.1 |
| A03A | Drugs for functional bowel disorders | 7640 | 12.6 |
| R03D | Other systemic drugs for obstructive airway diseases | 6463 | 10.6 |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Mahnke, C.B. The growth and development of a specialty: The history of pediatrics. Clin. Pediatr. 2000, 39, 705–714. [Google Scholar] [CrossRef]
- Wu, M.H.; Chen, H.C.; Wang, J.K.; Chiu, H.H.; Huang, S.C.; Huang, S.K. Population-based study of pediatric sudden death in Taiwan. J. Pediatr. 2009, 155. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.H. Trends in low fertility and policy responses in Taiwan. Jpn. J. Popul. 2012, 10, 78–88. [Google Scholar]
- Lin, M.C.; Lai, M.S. Pediatricians’ role in caring for preschool children in Taiwan under the national health insurance program. J. Formos. Med. Assoc. 2009, 108, 849–855. [Google Scholar] [CrossRef]
- Freed, G.L.; Dunham, K.M.; Gebremariam, A.; Wheeler, J.R.; Research Advisory Committee of the American Board of Pediatrics. Which pediatricians are providing care to America’s children? An update on the trends and changes during the past 26 years. J. Pediatr. 2010, 157. [Google Scholar] [CrossRef] [PubMed]
- McCaig, L.F.; Besser, R.E.; Hughes, J.M. Trends in antimicrobial prescribing rates for children and adolescents. JAMA 2002, 287, 3096–3102. [Google Scholar] [CrossRef] [PubMed]
- Linder, J.A.; Bates, D.W.; Lee, G.M.; Finkelstein, J.A. Antibiotic treatment of children with sore throat. JAMA 2005, 294, 2315–2322. [Google Scholar] [CrossRef] [PubMed]
- Olson, K.L.; Mandl, K.D. Temporal patterns of medications dispensed to children and adolescents in a national insured population. PLoS ONE 2012, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, T.; Smith, M.A.; Camp, P.G.; Shajari, S.; MacLeod, S.M.; Carleton, B.C. Prescription drug dispensing profiles for one million children: A population-based analysis. Eur. J. Clin. Pharmacol. 2013, 69, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Thrane, N.; Steffensen, F.H.; Mortensen, J.T.; Schønheyder, H.C.; Sørensen, H.T. A population-based study of antibiotic prescriptions for Danish children. Pediatr. Infect. Dis. J. 1999, 18, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Mendoza, R.; Costa, M.M.; Ottoni, E.J.; Bertaco, A.S.; Santos, J.C.; D’avila, N.E.; Faria, C.S.; Zenobini, E.C.; Gomesa, A. Antibiotic use in community-based pediatric outpatients in southern region of Brazil. J. Trop. Pediatr. 2005, 51, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Lass, J.; Odlind, V.; Irs, A.; Lutsar, I. Antibiotic prescription preferences in paediatric outpatient setting in Estonia and Sweden. Springerplus 2013, 2. [Google Scholar] [CrossRef] [PubMed]
- Chuang, C.M.; Chan, I.C.; Lee, Y.S.; Tsao, P.C.; Yang, C.F.; Soong, W.J.; Chen, T.J.; Jeng, M.J. Role of pediatricians in the ambulatory care of children in Taiwan, 1999–2011. Pediatr. Neonatol. 2015, 56, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Liao, P.; Ku, M.; Lue, K.; Sun, H. Respiratory tract infection is the major cause of the ambulatory visits in children. Ital. J. Pediatr. 2011, 37. [Google Scholar] [CrossRef] [PubMed]
- National Health Insurance Research Database. Available online: http://w3.nhri.org.tw/nhird/ (accessed on 30 October 2015).
- World Health Organization ATC/DDD Index 2015. Available online: http://www.whocc.no/atc_ddd_index/ (accessed on 30 October 2015).
- Galdas, P.M.; Cheater, F.; Marshall, P. Men and health help-seeking behaviour: Literature review. J. Adv. Nurs. 2005, 49, 616–623. [Google Scholar] [CrossRef] [PubMed]
- Oliver, M.I.; Pearson, N.; Coe, N.; Gunnell, D. Help-seeking behaviour in men and women with common mental health problems: Cross-sectional study. Brit. J. Psychiatry 2005, 186, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Ek, S. Gender differences in health information behaviour: A Finnish population-based survey. Health Promot. Int. 2015, 30, 736–745. [Google Scholar] [CrossRef] [PubMed]
- Taiwan Medical Association. Stastics for 2014. 2015. Available online: http://www.tma.tw/tma_stats_2014/2014_stats.pdf (accessed on 20 July 2015).
- Globalization Medical Education. The Analysis of Variance of Physician Manpower over the Years. Available online: http://spaces.isu.edu.tw/~amed/Fileupload/results/20100809215021.pdf (accessed on 20 July 2015).
- Lynn, A.-M.; Lai, L.-J.; Lin, M.-H.; Chen, T.-J.; Hwang, S.-J.; Wang, P.-H. Pattern of ambulatory care visits to obstetrician-gynecologists in Taiwan: A nationwide analysis. Int. J. Environ. Res. Public Health 2015, 12, 6832–6841. [Google Scholar] [CrossRef] [PubMed]
- Liou, J.S. Exam the Social Inequality Issues from Disparity between Urban and Rural Infant Mortality. 2004. Available online: http://handle.ncl.edu.tw/11296/ndltd/83353925990290415649 (accessed on 20 July 2015).
- Liao, H.C. Spatial Accessibility to Pediatric Services in Taiwan. 2013. Available online: http://readopac2.ncl.edu.tw/nclJournal/search/detail.jsp?sysId=0006725343&dtdId=000040&search_type=detail&la=ch (accessed on 20 July 2015).
- Huang, S.S. Study on the Effect of Low Birth Rate to Supply and Demand of Pediatric Specialist Manpower in Taiwan. 2013. Available online: http://ir.kmu.edu.tw/handle/310902000/35668 (accessed on 20 July 2015).
- Halasa, N.B.; Griffin, M.R.; Zhu, Y.; Edwards, K.M. Decreased number of antibiotic prescriptions in office-based settings from 1993 to 1999 in children less than five years of age. Pediatr. Infect. Dis. J. 2002, 11, 1023–1028. [Google Scholar] [CrossRef]
- Nash, D.R.; Harman, J.; Wald, E.R.; Kelleher, K.J. Antibiotic prescribing by primary care physicians for children with upper respiratory tract infections. Arch Pediatr. Adolesc. Med. 2002, 15, 1114–1119. [Google Scholar] [CrossRef]
- Miller, G.E.; Hudson, J. Children and antibiotics: Analysis of reduced use, 1996–2001. Med. Care 2006, 44, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Finkelstein, J.A.; Metlay, J.P.; Davis, R.L.; Rifas-Shiman, S.L.; Dowell, S.F.; Platt, R. Antimicrobial use in defined populations of infants and young children. Arch Pediatr. Adolesc. Med. 2000, 154, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Perz, J.F.; Craig, A.S.; Coffey, C.S.; Jorgensen, D.M.; Mitchel, E.; Hall, S.; Schaffner, W.; Griffin, M.R. Changes in antibiotic prescribing for children after a community-wide campaign. JAMA 2002, 287, 3103–3109. [Google Scholar] [CrossRef] [PubMed]
- Tell, D.; Engström, S.; Mölstad, S. Adherence to guidelines on antibiotic treatment for respiratory tract infections in various categories of physicians: A retrospective cross-sectional study of data from electronic patient records. BMJ Open 2015, 5. [Google Scholar] [CrossRef] [PubMed]
- Hersh, A.L.; Shapiro, D.J.; Pavia, A.T.; Shah, S.S. Antibiotic prescribing in ambulatory pediatrics in the United States. Pediatrics 2011, 128, 1053–1061. [Google Scholar] [CrossRef] [PubMed]
- Taiwan Pediatric Association. Guidelines & Recommendations. Available online: http://www.pediatr.org.tw/english/guidelines.asp (accessed on 20 July 2015).
- Liu, F.C.; Chen, P.Y.; Huang, F.; Tsai, C.R.; Lee, C.Y.; Wang, L.C. Rapid diagnosis of Mycoplasma pneumoniae infection in children by polymerase chain reaction. J. Microbiol. Immunol. Infect. 2007, 40, 507–512. [Google Scholar] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, L.-Y.; Lynn, A.-M.; Chen, T.-J. Ambulatory Care Visits to Pediatricians in Taiwan: A Nationwide Analysis. Int. J. Environ. Res. Public Health 2015, 12, 14043-14054. https://doi.org/10.3390/ijerph121114043
Yang L-Y, Lynn A-M, Chen T-J. Ambulatory Care Visits to Pediatricians in Taiwan: A Nationwide Analysis. International Journal of Environmental Research and Public Health. 2015; 12(11):14043-14054. https://doi.org/10.3390/ijerph121114043
Chicago/Turabian StyleYang, Ling-Yu, An-Min Lynn, and Tzeng-Ji Chen. 2015. "Ambulatory Care Visits to Pediatricians in Taiwan: A Nationwide Analysis" International Journal of Environmental Research and Public Health 12, no. 11: 14043-14054. https://doi.org/10.3390/ijerph121114043