
Probable Post Traumatic Stress Disorder in Kenya and Its Associated Risk Factors: A Cross-Sectional Household Survey

Abstract
:1. Background
2. Methods
2.1. Study Population
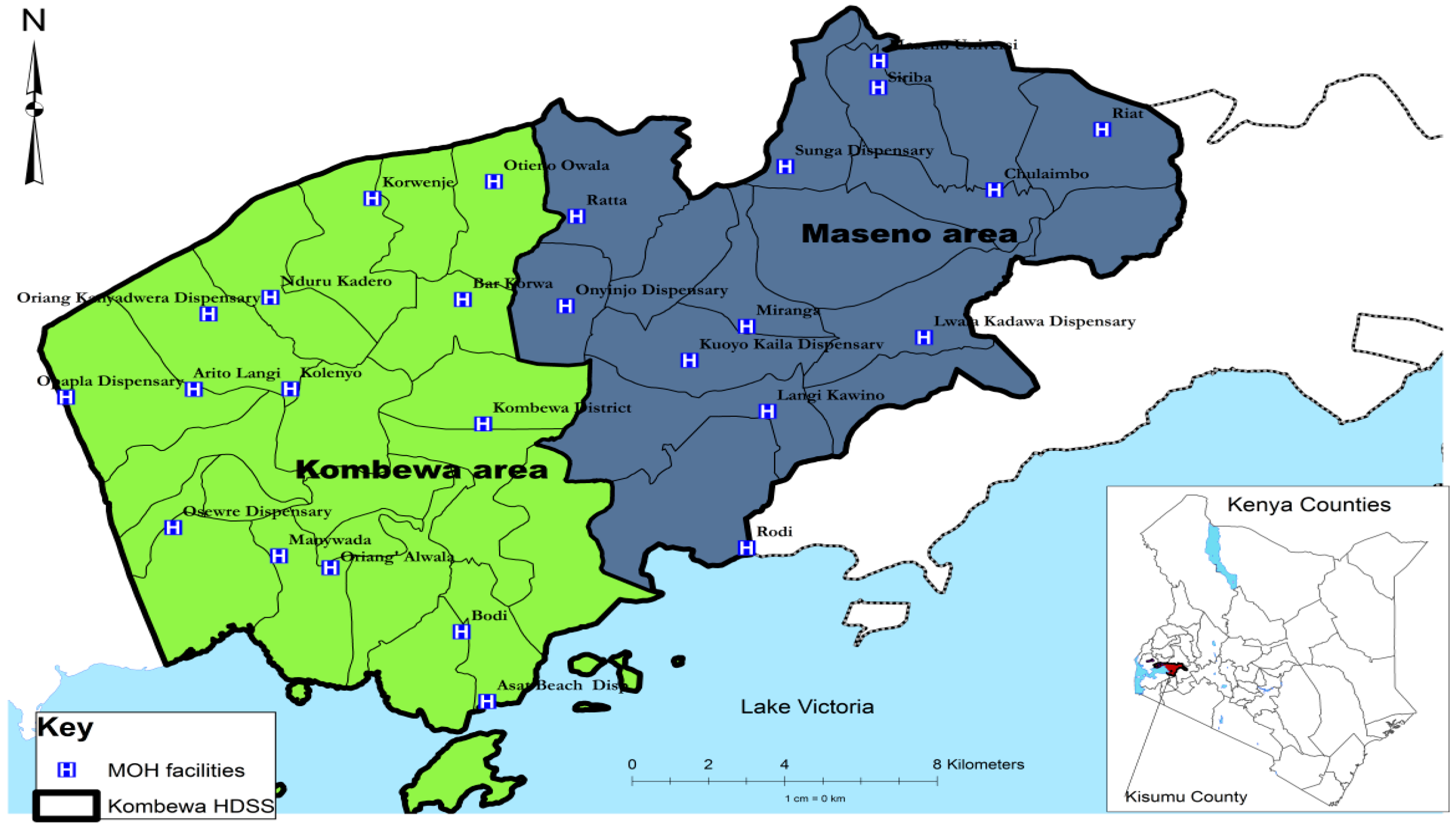
2.2. Study Site

2.3. Study Participants
2.4. Study Procedures
2.5. Statistical Analysis
2.6. Ethics
3. Results

{kind=link}
| Trauma Screening Questionnaire | Scores | |||
|---|---|---|---|---|
| Has a traumatic event or experience ever happened to you at any time in your life | Yes | 552 (48.2) | ||
| No | 528 (46.1) | |||
| Don’t apply | 66 (5.8) | |||
| Have you experienced, at least twice in the past week: Feeling upset by reminders of the event | Yes | 250 (50.1) | ||
| No | 241 (48.3) | |||
| Don’t apply | 8 (1.6) | |||
| Have you experienced, at least twice in the past week: Bodily reactions (such as fast heartbeat, stomach churning, sweatiness, dizziness) when reminded of the event | Yes | 166 (33.3) | ||
| No | 317 (63.5) | |||
| Don’t apply | 16 (3.2) | |||
| Have you experienced, at least twice in the past week: Difficulty falling or staying asleep | Yes | 191 (38.3) | ||
| No | 297 (59.5) | |||
| Don’t apply | 11 (2.2) | |||
| Have you experienced, at least twice in the past week: Irritability or outbursts of anger | Yes | 155 (31.2) | ||
| No | 334 (67.2) | |||
| Don’t apply | 8 (1.6) | |||
| Have you experienced, at least twice in the past week: Difficulty concentrating | Yes | 144 (29.0) | ||
| No | 344 (69.2) | |||
| Don’t apply | 9 (1.8) | |||
| Have you experienced, at least twice in the past week: Heightened awareness of potential dangers to yourself and others | Yes | 117 (23.6) | ||
| No | 360 (72.6) | |||
| Don’t apply | 19 (3.8) | |||
| Have you experienced, at least twice in the past week: Being jumpy or being startled at something unexpected | Yes | 102 (20.5) | ||
| No | 378 (75.9) | |||
| Don’t apply | 18 (3.6) | |||
| Total PTSD scores | 0 to 2 | 803 (70.1) | ||
| 3 to 5 | 222 (19.4) | |||
| 6 to 7 | 56 (4.9) | |||
| Above 7 | 65 (5.6) | |||
| Prevalence of probable PTSD (TSQ 6+): % (95% CI) | 10.6 (8.8–12.5) | |||
| Factors | N | Prevalence: n (%) | Unadjusted OR (95% C.I) | p-Value | |
|---|---|---|---|---|---|
| Prevalence of PTSD | 1146 | 121 (10.6) | |||
| Sex | Male | 601 | 40 (6.7) | 1 | - |
| Female | 545 | 81 (14.9) | 2.4 (1.64–3.65) | <0.001 | |
| Age group | <30 years | 281 | 39 (13.9) | 1 | - |
| 30–60 years | 448 | 52 (11.6) | 0.8 (0.52–1.27) | 0.367 | |
| >60 years | 171 | 23 (13.5) | 1.0 (0.55–1.68) | 0.898 | |
| Household size | ≤6 people | 566 | 61 (10.8) | 1 | - |
| >6 people | 580 | 60 (10.3) | 1.0 (0.66–1.39) | 0.812 | |
| Marital Status | Married/cohabiting | 714 | 65 (9.1) | 1 | - |
| Single | 183 | 22 (12.0) | 1.4 (0.82–2.28) | 0.236 | |
| Widowed/divorced | 248 | 34 (13.7) | 1.6 (1.01–2.47) | 0.041 | |
| Education | None | 131 | 15 (11.5) | 1 | - |
| Primary | 625 | 68 (10.9) | 0.9 (0.52–1.71) | 0.849 | |
| Secondary | 319 | 35 (11.0) | 1.0 (0.50–1.81) | 0.883 | |
| Post secondary | 71 | 3 (4.2) | 0.3 (0.10–1.22) | 0.098 | |
| Employment status | Unemployed | 563 | 47 (8.4) | 1 | - |
| Self employed | 484 | 67 (13.8) | 1.8 (1.19–2.62) | 0.005 | |
| Employed | 99 | 7 (7.1) | 0.8 (0.37–1.91) | 0.669 | |
| Positive | 269 | 30 (11.2) | 1.1 (0.72–1.79) | 0.584 | |
| Asset Groups | Lowest, Q1 | 403 | 35 (8.7) | 1 | - |
| Q2 | 409 | 50 (12.2) | 1.5 (0.93–2.31) | 0.101 | |
| Highest, Q3 | 334 | 36 (10.8) | 1.3 (0.78–2.07) | 0.338 | |
| Life events | 0–1 | 361 | 18 (5.0) | 1 | - |
| 2–3 | 476 | 48 (10.1) | 2.1 (1.22–3.74) | 0.008 | |
| 4 or more | 309 | 55 (17.8) | 4.1 (2.37–7.20) | <0.001 | |
| Perceived lack of social support | No lack: 0 | 3 | 1 (33.3) | 1 | - |
| Moderate lack: 1–7 | 312 | 31 (9.9) | 0.2 (0.02–2.50) | 0.223 | |
| Severe lack: 8+ | 828 | 89 (10.8) | 0.2 (0.02–2.68) | 0.247 | |
| Total social group size | 3 or less | 144 | 12 (8.3) | 1 | - |
| –8 | 519 | 56 (10.8) | 1.3 (0.69–2.56) | 0.391 | |
| 9 or more | 480 | 53 (11.0) | 1.4 (0.71–2.63) | 0.352 | |
| Presence of CMD | No | 1027 | 75 (7.3) | 1 | - |
| Yes | 119 | 46 (38.7) | 8.0 (5.16–12.39) | <0.001 | |
| Carer for >4 h | No | 26 | 3 (11.5) | 1 | - |
| Yes | 171 | 14 (8.2) | 0.7 (0.18–2.56) | 0.573 | |
| Spent time at institution <16 years | No | 919 | 84 (9.1) | 1 | - |
| Yes | 220 | 37 (16.8) | 2.0 (1.32–3.05) | 0.001 | |
| Did not live continuously with both natural parents until age 16 | No | 963 | 102 (10.6) | 1 | - |
| Yes | 176 | 19 (10.8) | 1.0 (0.61–1.72) | 0.936 | |
| Factors | Adjusted OR * (95% C.I) | p-Value | |
|---|---|---|---|
| Gender | Female | 2.0 (1.25 to 3.17) | 0.004 |
| Marital status | Single | 1.8 (1.03 to 3.13) | 0.038 |
| Widowed/divorced | 0.7 (0.44 to 1.29) | 0.294 | |
| Employment | Self employed | 1.9 (1.24 to 3.00) | 0.003 |
| Employed | 1.1 (0.47 to 2.77) | 0.770 | |
| Total life events | 2–3 | 2.1 (1.17 to 3.87) | 0.013 |
| 4 or more | 3.8 (2.10 to 6.89) | <0.001 | |
| Any CMD | 7.0 (4.21 to 11.68) | <0.001 | |
| Spent time at institution <16 years | 1.8 (1.10 to 2.79) | 0.018 | |
| Factors | N | Prevalence: n (%) | Unadjusted OR (95% C.I) | p-Value | |
|---|---|---|---|---|---|
| Serious illness, injury or assault to self | No | 818 | 72 (8.8) | 1 | - |
| Yes | 328 | 49 (14.9) | 1.8 (1.23 to 2.68) | 0.003 | |
| Serious illness, injury or assault to a close relative | No | 819 | 65 (7.9) | 1 | - |
| Yes | 327 | 56 (17.1) | 2.4 (1.63 to 3.52) | <0.001 | |
| Death of an immediate family member of yours | No | 443 | 29 (6.6) | 1 | - |
| Yes | 703 | 92 (13.1) | 2.1 (1.39 to 3.32) | 0.001 | |
| Death of a close family friend or other relative | No | 693 | 75 (10.8) | 1 | - |
| Yes | 453 | 46 (10.2) | 0.9 (0.63 to 1.37) | 0.719 | |
| Separation due to marital differences, divorce or steady relationship broken | No | 1115 | 114 (10.2) | 1 | - |
| Yes | 31 | 7 (22.6) | 2.6 (1.08 to 6.08) | 0.033 | |
| Serious problem with a close friend, neighbour or relative | No | 1046 | 109 (10.4) | 1 | - |
| Yes | 100 | 12 (12.0) | 1.2 (0.62 to 2.21) | 0.624 | |
| Being made redundant or sacked from your job | No | 1093 | 119 (10.9) | 1 | - |
| Yes | 53 | 2 (3.8) | 0.3 (0.08 to 1.34) | 0.118 | |
| Looking for work without success for >1 month | No | 997 | 106 (10.6) | 1 | - |
| Yes | 149 | 15 (10.1) | 0.9 (0.53 to 1.66) | 0.834 | |
| Major financial crisis, like losing an equivalent of 3months income | No | 881 | 83 (9.4) | 1 | - |
| Yes | 265 | 38 (14.3) | 1.6 (1.07 to 2.43) | 0.023 | |
| Problem with police involving court appearance | No | 1108 | 114 (10.3) | 1 | - |
| Yes | 38 | 7 (18.4) | 2.0 (0.85 to 4.57) | 0.115 | |
| Something you valued being lost or stolen | No | 990 | 83 (8.4) | 1 | - |
| Yes | 156 | 38 (24.4) | 3.5 (2.29 to 5.41) | <0.001 | |
| Bullying | No | 1093 | 113 (10.3) | 1 | - |
| Yes | 53 | 8 (15.1) | 1.5 (0.71 to 3.35) | 0.275 | |
| Violence at work | No | 1098 | 117 (10.7) | 1 | - |
| Yes | 48 | 4 (8.3) | 0.8 (0.27 to 2.16) | 0.609 | |
| Violence at home | No | 932 | 76 (8.2) | 1 | - |
| Yes | 214 | 45 (21.0) | 3.0 (2.00 to 4.49) | <0.001 | |
| Sexual abuse | No | 1140 | 121 (10.6) | 1 | - |
| Yes | 6 | 0 (-) | - | - | |
| Being expelled from school | No | 1113 | 116 (10.4) | 1 | - |
| Yes | 33 | 5 (15.2) | 1.5 (0.58 to 4.05) | 0.387 | |
| Running away from you home | No | 1119 | 112 (10.0) | 1 | - |
| Yes | 27 | 9 (33.3) | 4.5 (1.97 to 10.24) | <0.001 | |
| Being homeless | No | 1132 | 118 (10.4) | 1 | - |
| Yes | 14 | 3 (21.4) | 2.3 (0.64 to 8.52) | 0.196 | |
4. Discussion
4.1. Overall Findings
4.2. Comparison with Other Relevant Studies
Prevalence
4.3. Strengths of Study
4.4. Limitations of Study
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems; Tenth Revision; World Health Organization: Geneva, Switzerland, 1993. [Google Scholar]
- Summerfield, D. A critique of seven assumptions behind psychological trauma programmes in war affected areas. Soc. Sci. Med. 1999, 48, 1449–1462. [Google Scholar] [CrossRef]
- Njenga, F.; Nguthi, A.; Kangethe, R. War and mental disorders in Africa. World Psychiatry 2006, 5, 38–39. [Google Scholar] [PubMed]
- World Bank. World Development Indicators, Kenya 2015. Available online: http://data.worldbank.org/country/kenya (accessed on 23 October 2015).
- Kenya 2009 Census. Available online: http://www.prb.org/pdf11/kenya-population-data-sheet-2011.pdf (accessed on 23 October 2015).
- Kimanga, D.O.; Ogola, S.; Umuro, M.; Nganga, A.; Kimondo, L.; Mureithi, P.; Muttunga, J.; Waruiru, W.; Mohammed, I.; Sharrif, S.; et al. Available online: http://www.ncbi.nlm.nih.gov/pubmed/24445338 (accessed on 17 January 2014).
- The Millennium Development Goals Report; United Nations: New York, NY, USA, 2007.
- Oluoch, T.; Mohammed, I.; Bunnell, R.; Kaiser, R.; Kim, A.A.; Gichangi, A.; Mwangi, M.; Dadabhai, S.; Marum, L.; Orago, A.; et al. Correlates of HIV infection among sexually active adults in Kenya: A national population-based survey. Open AIDS J. 2011, 5, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Mugawebster, F.; Jenkins, R. Health care models guiding mental health policy in Kenya 1965–1997. Int. J. Ment. Health Syst. 2010. [Google Scholar] [CrossRef]
- Muga, F.; Jenkins, R. Public perceptions, explanatory models and service utilisation regarding mental illness and mental health care in Kenya. Soc. Psychiatr. Psychiatr. Epidemiol. 2008, 43, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Kiima, D.M.; Njenga, F.G.; Okonji, M.M.; Kigama, P.A. Kenya mental health country profile. Int. Rev. Psychiatry 2004, 16, 31–47. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, R.; Njenga, F.; Okonji, M.; Kigamwa, P.; Baraza, M.; Ayuyo, J.; Singleton, N.; McManus, S.; Kiima, D. Prevalence of common mental disorders in a rural district of Kenya, and socio-demographic risk factors. Int. J. Environ. Res. Public Health 2012, 9, 1810–1819. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, R.; Njenga, F.; Okonji, M.; Kigamwa, P.; Baraza, M.; Ayuyo, J.; Singleton, N.; McManus, S.; Kiima, D. Psychotic symptoms in Kenya—Prevalence and risk factors, including their relationship with common mental disorders. Int. J. Environ. Res. Public Health 2012, 9, 1748–1756. [Google Scholar] [CrossRef] [PubMed]
- Okonji, M.; Njenga, F.; Kiima, D.; Ayuyo, J.; Kigamwa, P.; Shah, A.; Jenkins, R. Traditional health practitioners and mental health in Kenya. Int. Psychiatry 2008, 5, 46–48. [Google Scholar]
- Kiima, D.; Njenga, F.; Shah, A.; Okonji, M.; Ayuyo, J.; Baraza, M.; Parker, E.; Jenkins, R. Attitudes to depression among community health workers in Kenya. Epidemiol. Psychiatr. 2009, 18, 352–356. [Google Scholar]
- Muga, F.; Jenkins, R. Training, attitudes and practice of district health workers in Kenya. Soc. Psychiatr. Psychiatr. Epidemiol. 2008, 43, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Kiima, D.; Jenkins, R. Mental health policy in Kenya—An integrated approach to scaling up equitable care for poor populations. Int. J. Ment. Health Syst. 2010. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, R.; Kiima, D.; Njenga, F.; Okonji, M.; Kingora, J.; Kathuku, D.; Lock, S. Integration of mental health into primary care in Kenya. World Psychiatry 2010, 9, 118–120. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, R.; Kiima, D.; Okonji, M.; Njenga, F.; Kingora, J.; Lock, S. Integration of mental health in primary care and community health working in Kenya: Context, rationale, coverage and sustainability. Ment. Health Fam. Med. 2010, 7, 37–47. [Google Scholar] [PubMed]
- Jenkins, R.; Othieno, C.; Okeyo, S.; Kaseje, D.; Aruwa, J.; Oyugi, H.; Bassett, P.; Kauye, F. Short structured general mental health in service training programme in Kenya improves patient health and social outcomes but not detection of mental health problems—A pragmatic cluster randomised controlled trial. Int. J. Ment. Health Syst. 2013. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, R.; Othieno, C.; Okeyo, S.; Aruwa, J.; Kingora, J.; Jenkins, B. Health system challenges to integration of mental health delivery in primary care in Kenya-perspectives of primary care health workers. BMC Health Serv. Res. 2013. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, R.; Othieno, C.; Okeyo, S.; Aruwa, J.; Wallcraft, J.; Jenkins, B. Exploring the perspectives and experiences of health workers at primary health facilities in Kenya following training. Int. J. Ment. Health Syst. 2012. [Google Scholar] [CrossRef] [PubMed]
- Othieno, C.; Jenkins, R.; Okeyo, S.; Aruwa, J.; Wallcraft, B.; Jenkins, B. Perspectives and concerns of clients at primary health care facilities involved in evaluation of a national mental health training programme for primary care in Kenya. Int. J. Ment. Health Syst. 2013. [Google Scholar] [CrossRef] [PubMed]
- Johnson, K.; Scott, J.; Sasyniuk, T.; Ndetei, D.; Kisielewski, M.; Rouhani, S.; Bartels, S.; Mutiso, V.; Mbwayo, A.; Rae, D.; et al. A national population based assessment of the 2007–2008 election related violence in Kenya. Confl. Health 2014. [Google Scholar] [CrossRef] [PubMed]
- Sifuna, P.; Oyugi, M.; Ogutu, B.; Andagalu, B.; Otieno, A.; Owira, V.; Otsyula, N.; Oyieko, J.; Cowden, J.; Otieno, L.; et al. Health & Demographic Surveillance System Profile: The Kombewa Health and Demographic Surveillance System (Kombewa HDSS). Int. J. Epidemiol. 2014. [Google Scholar] [CrossRef]
- Kish, L. A procedure for objective respondent selection within households. J Am Stat Assoc. 1949, 46, 380–387. [Google Scholar] [CrossRef]
- Health and Social Care Information Centre. Adult Psychiatric Morbidity in Englad-2007, Results of a household survey. Available online: http://www.hscic.gov.uk/pubs/psychiatricmorbidity07 (accessed on 23 October 2015).
- Brewin, C.R.; Rose, S.; Andrews, B.; Green, J.; Tata, P.; McEvedy, C.; Turner, S.W.; Foa, E.B. Brief screening instrument for post-traumatic stress disorder. Br. J. Psychiatry 2002, 181, 158–162. [Google Scholar] [PubMed]
- Foa, E.B.; Riggs, D.S.; Dancu, C.V.; Rothbaum, B.O. Reliability and validity of a brief instrument for assessing post-traumatic stress disorder. J. Trauma. Stress 1993, 6, 459–473. [Google Scholar] [CrossRef]
- Galea, A.; Brewin, C.; Gruber, M.; Jones, R.; King, D.; King, L.; McNally, R.; Ursano, R.; Petukhova, M.; Kessler, R. Exposure to Hurricane related stressors and mental illness after hurricane Katrina. Arch. Gen. Psychiatry 2007, 64, 1247–1434. [Google Scholar] [CrossRef] [PubMed]
- Lewis, G.; Pelosi, A.; Araya, R.C.; Dunn, G. Measuring psychiatric disorder in the community: A standardised assessment for use by lay interviewers. Psychol. Med. 1992, 22, 465–489. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, R.; Bebbington, P.; Brugha, T.; Farrell, M.; Gill, B.; Lewis, G.; Meltzer, H.; Petticrew, M. The national psychiatric morbidity surveys of Great Britain—Strategy and methods. Psychol. Med. 1997, 27, 765–774. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, H.; Gill, B.; Petticrew, M.; Hinds, K. OPCS Survey of Psychiatric Morbidity: Report 1. The Prevalence of Psychiatric Morbidity among Adults Ages 16–64 Living in Private Households in Great Britain; HMSO: London, UK, 1995. [Google Scholar]
- Singleton, N.; Bumpstead, R.; O’Brien, M.; Lee, A.; Meltzer, H. Psychiatric morbidity among adults living in private households, 2000. Int. Rev. Psychiatry 2003, 15, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.; Kirkwood, B.R.; Pednekar, S.; Weiss, H.; Mabey, D. Risk factors for common mental disorders in women: Population-based longitudinal study. Br. J. Psychiatry 2006, 189, 547–555. [Google Scholar] [CrossRef] [PubMed]
- Araya, R.; Rojas, G.; Aritsch, R.; Acuna, J.; Lewis, G. Common mental disorders in Santiago, Chile: Prevalence and socio-demographic correlates. Br. J. Psychiatry 2001, 178, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Ickramasinghe, S.C.; Rajapakse, L.; Abeysinghe, R.; Prince, M. The Clinical Interview Schedule-Revised (CIS-R): Modification and validation in Sri Lanka. Int. J. Methods Psychiatry Res. 2002, 11, 169–177. [Google Scholar] [CrossRef]
- Ngoma, M.C.; Prince, M.; Mann, A. Common mental disorders among those attending primary health clinics and traditional healers in urban Tanzania. Br. J. Psychiatry 2003, 183, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, R.; Mbatia, J.; Singleton, N.; White, B. Common mental disorders and risk factors in urban Tanzania. Int. J. Environ. Res. Public Health 2010, 7, 2543–2558. [Google Scholar] [CrossRef] [PubMed]
- Breeze, E.; Maidment, A.; Bennett, N.; Flatley, J.; Carey, S. Health Sur. for England, 1992; HMSO: London, UK, 1994. [Google Scholar]
- Mc Manus, S.; Melzer, H.; Wesseley, S. Chapter 3 Post Traumatic Stress Disorder. In Adult Psychiatric Morbidity Survey 2007—The Health and Social Care; Information Centre—Social Care Statistics: Washington, DC, USA, 2009; pp. 53–70. [Google Scholar]
- Statacorp. Stata Statistical Software: Release 11.2; StataCorp LP: College Station, TX, 2003. [Google Scholar]
- Moser, C. The asset vulnerability framework: Reassessing urban poverty reduction strategies. World Dev. 1998, 26, 1–19. [Google Scholar] [CrossRef]
- Morris, S.S.; Carletto, C.; Hoddinott, J.; Christiaensen, L.J. Validity of rapid estimates of household wealth and income for health surveys in rural Africa. J. Epidemiol. Community Health 2000, 54, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Karsberg, S.H.; Elklit, A. Victimization and PTSD in A rural Kenyan youth sample. Clin. Pract. Epidemiol. Ment. Health 2012, 8, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Ndetei, D.M.; Ongecha-Owuor, F.A.; Khasakhala, L.; Mutiso, V.; Odhiambo, G.; Kokonya, D.A. Traumatic experiences of Kenya secondary school students. J. Child Adolesc. Ment. Health 2007, 19, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Atwoli, L.; Kathuku, D.M.; Ndetei, D.M. Post traumatic stress disorder among Mau Mau concentration camp survivors in Kenya. East Afr. Med. J. 2006, 83, 352–359. [Google Scholar] [CrossRef] [PubMed]
- Pham, P.N.; Weinstein, H.M.; Longman, T. Trauma and PTSD symptoms in Rwanda: Implications for attitudes toward justice and reconciliation. JAMA: J. Am. Med. Assoc. 2004, 292, 602–612. [Google Scholar] [CrossRef] [PubMed]
- Neuner, F.; Schauer, M.; Karunakara, U.; Klaschik, C.; Robert, C.; Elbert, T. Psychological trauma and evidence for enhanced vulnerability for posttraumatic stress disorder through previous trauma among West Nile refugees. BMC Psychiatry 2004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atwoli, L.; Stein, D.J.; Williams, D.R.; Mclaughlin, K.A.; Petukhova, M.; Kessler, R.C.; Koenen, K.C. Trauma and posttraumatic stress disorder in South Africa: Analysis from the South African stress and health study. BMC Psychiatry 2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seedat, S.; Nyamai, C.; Njenga, F.; Vythilingum, B.; Stein, D.J. Trauma exposure and post traumatic stress symptoms in urban African schools. Br. J. Psychiatry 2004, 184, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Chiu, W.T.; Demler, O.; Merikangas, K.R.; Walters, E.E. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 617–627. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Rose, S.; Koenen, K.C.; Karam, E.G.; Stang, P.E.; Stein, D.J.; Heeringa, S.G.; Hill, E.D.; Liberzon, I.; McLaughlin, K.A.; et al. How well can post traumatic stress disorder be predicted from pre-trauma risk factors? An exploratory study in the WHO Word Mental Health Surveys. World Psychiatry 2014, 13, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Clancey, K.; Gove, W. Sex differences in respondents reports of psychiatric symptoms: An analysis of response bias. Am. Sociol. Rev. 1974, 80, 205–216. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jenkins, R.; Othieno, C.; Omollo, R.; Ongeri, L.; Sifuna, P.; Mboroki, J.K.; Kiima, D.; Ogutu, B. Probable Post Traumatic Stress Disorder in Kenya and Its Associated Risk Factors: A Cross-Sectional Household Survey. Int. J. Environ. Res. Public Health 2015, 12, 13494-13509. https://doi.org/10.3390/ijerph121013494
Jenkins R, Othieno C, Omollo R, Ongeri L, Sifuna P, Mboroki JK, Kiima D, Ogutu B. Probable Post Traumatic Stress Disorder in Kenya and Its Associated Risk Factors: A Cross-Sectional Household Survey. International Journal of Environmental Research and Public Health. 2015; 12(10):13494-13509. https://doi.org/10.3390/ijerph121013494
Chicago/Turabian StyleJenkins, Rachel, Caleb Othieno, Raymond Omollo, Linnet Ongeri, Peter Sifuna, James Kingora Mboroki, David Kiima, and Bernhards Ogutu. 2015. "Probable Post Traumatic Stress Disorder in Kenya and Its Associated Risk Factors: A Cross-Sectional Household Survey" International Journal of Environmental Research and Public Health 12, no. 10: 13494-13509. https://doi.org/10.3390/ijerph121013494