
Residential Radon Exposure and Incidence of Childhood Lymphoma in Texas, 1995–2011

Abstract
:1. Introduction
2. Experimental Section
2.1. Study Population
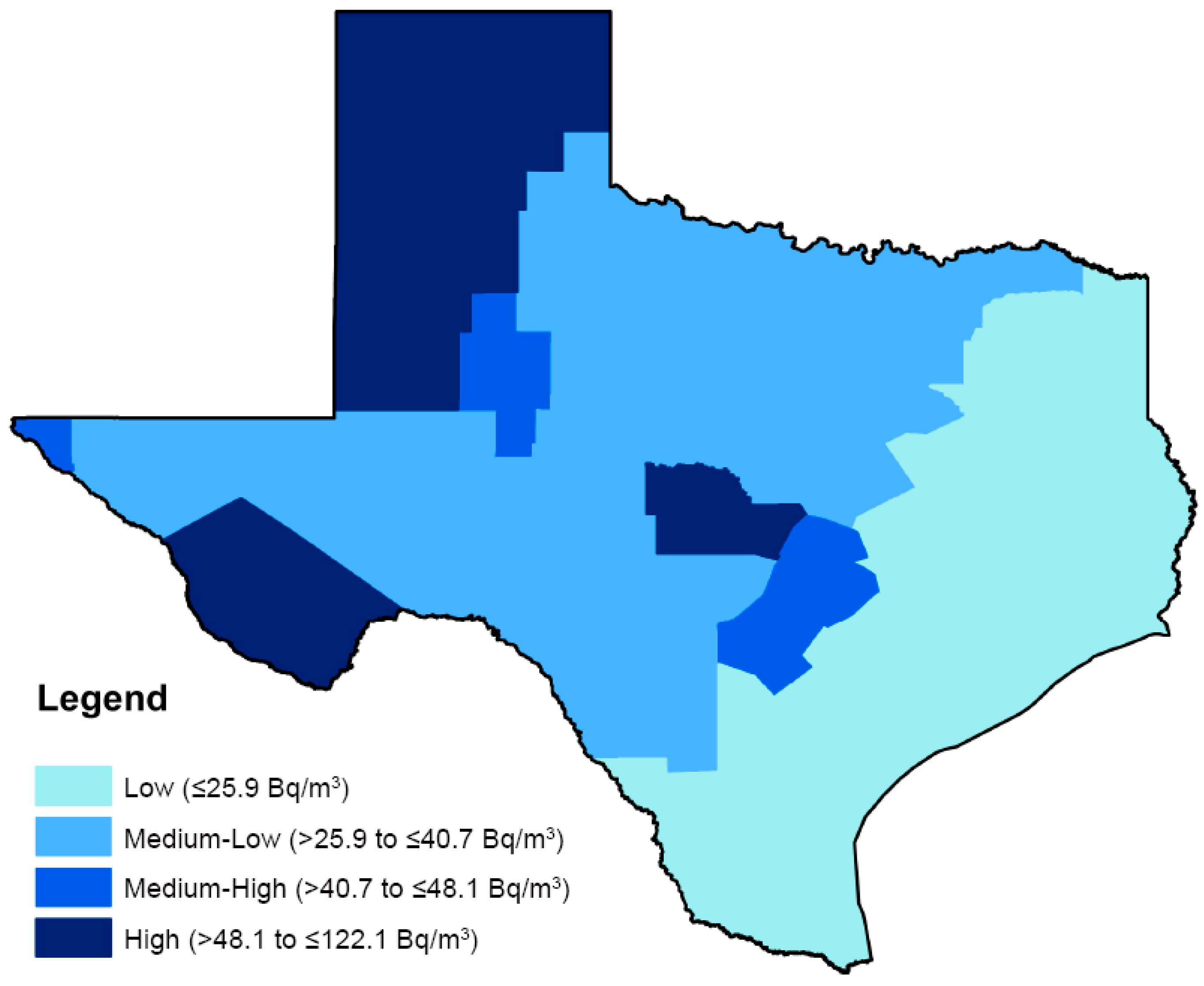
2.2. Exposure Assessment

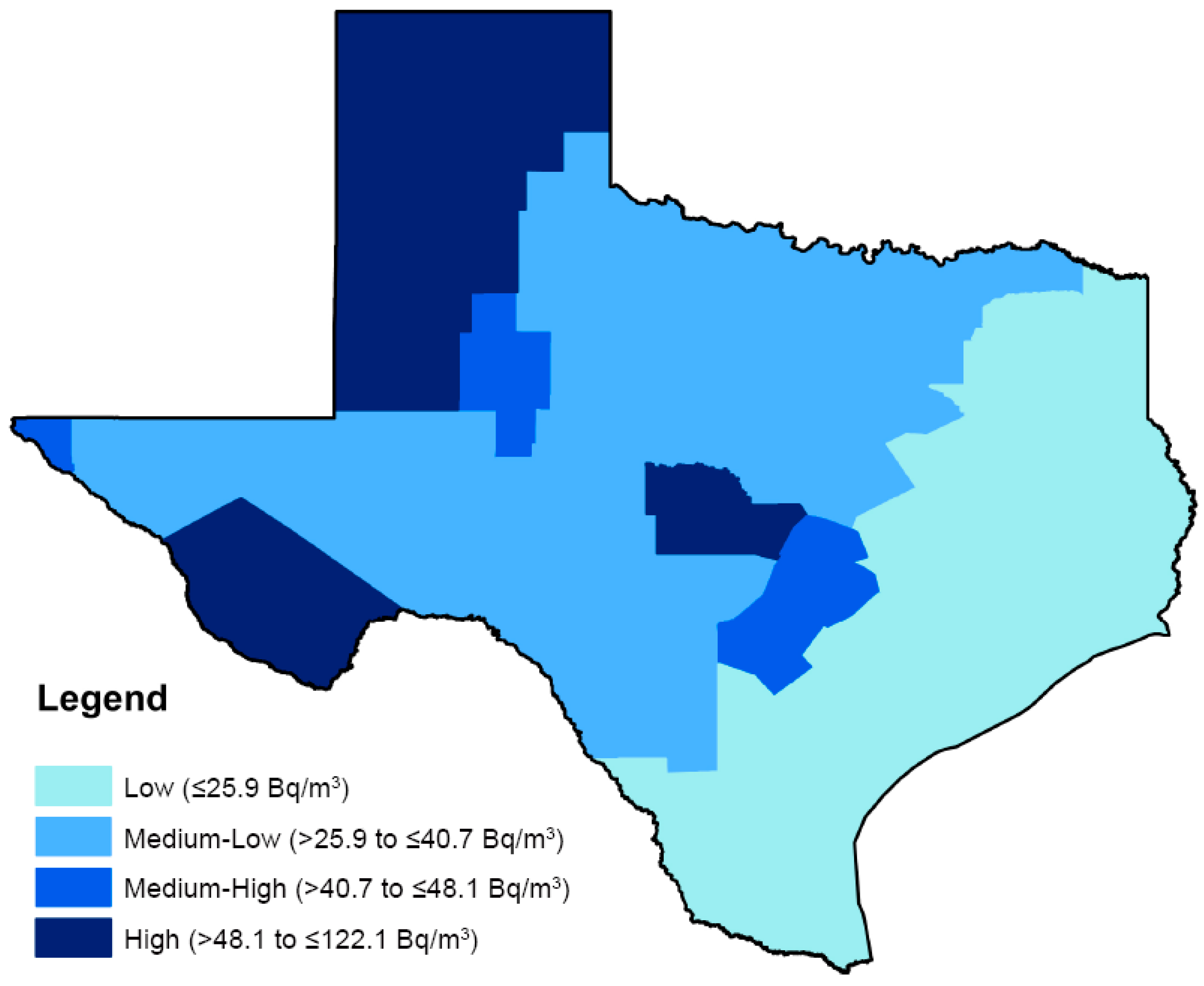{kind=link}
| Region Name | Region Number | Measurements for Analysis, n |
|---|---|---|
| Southwest Texas | 1 | 208 |
| El Paso | 2 | 97 |
| Big Bend | 3 | 122 |
| West Texas Shales | 4 | 241 |
| North Texas | 5 | 348 |
| Dallas/Fort Worth | 6 | 172 |
| East Texas | 7 | 296 |
| Llano Uplift | 8 | 213 |
| Central Texas (Austin-San Antonio) | 9 | 237 |
| Tertiary Sands Crescent | 10 | 204 |
| Harris County (Houston) | 11 | 122 |
| Gulf Coast | 12 | 215 |
| Texas Panhandle | 13 | 258 |
2.3. Covariate Selection
2.4. Statistical Analyses
3. Results and Discussion
3.1. Results
| Characteristic | All Lymphomas (n = 2147) | Hodgkin Lymphoma (n = 1248) | NHL Excluding BL (n = 658) | Burkitt Lymphoma (n = 241) | Diffuse Large B-Cell Lymphoma (n = 315) | Total TX Population <20 Years Old * (n = 6,523,632) |
|---|---|---|---|---|---|---|
| Age of Diagnosis (years), n (%) | ||||||
| <5 | 197 (9.2) | 38 (3.0) | 110 (16.7) | 49 (20.3) | 49 (20.3) | 1,610,302 (24.7) |
| 5 to <10 | 316 (14.7) | 117 (9.4) | 123 (18.7) | 76 (31.5) | 76 (31.5) | 1,660,902 (25.5) |
| 10 to <15 | 534 (24.9) | 323 (25.9) | 148 (22.5) | 63 (26.1) | 63 (26.1) | 1,642,973 (25.2) |
| 15 to <20 | 1100 (51.2) | 770 (61.7) | 277 (42.1) | 53 (22.0) | 53 (22.0) | 1,609,455 (24.7) |
| Sex, n (%) | ||||||
| Male | 1314 (61.2) | 702 (56.3) | 404 (61.4) | 208 (86.3) | 208 (86.3) | 3,348,530 (51.3) |
| Female | 833 (38.8) | 546 (43.8) | 254 (38.6) | 33 (13.7) | 33 (13.7) | 3,175,102 (48.7) |
| Race/Ethnicity, n (%) ** | ||||||
| Non-Hispanic White | 1029 (47.9) | 590 (47.3) | 310 (47.1) | 129 (53.5) | 129 (53.5) | 2,790,778 (42.8) |
| Hispanic White | 787 (36.7) | 447 (35.8) | 261 (39.7) | 79 (32.8) | 79 (32.8) | 1,484,094 (22.7) |
| Non-Hispanic Black | 243 (11.3) | 158 (12.7) | 61 (9.3) | 24 (10.0) | 24 (10.0) | 820,640 (12.6) |
| Other † | 88 (4.1) | 53 (4.3) | 26 (4.0) | 9 (3.7) | 9 (3.7) | 1,428,120 (21.9) |
| County-level SES/Level of Urbanization †, n (%) | ||||||
| Urban, Higher SES | 1421 (66.2) | 818 (65.5) | 434 (66.0) | 169 (70.1) | 169 (70.1) | 4,326,761 (66.3) |
| Urban, Lower SES | 510 (23.8) | 296 (23.7) | 167 (25.4) | 47 (19.5) | 47 (19.5) | 1,520,114 (23.3) |
| Rural, Higher SES | 144 (6.7) | 86 (6.9) | 37 (5.6) | 21 (8.7) | 21 (8.7) | 425,312 (6.5) |
| Rural, Lower SES | 72 (3.4) | 48 (3.9) | 20 (3.0) | 4 (1.7) | 4 (1.7) | 251,445 (3.9) |
| Mean Residential Radon Concentration (Bq/m3) | 33.3 | 32.4 | 34.3 | 34.8 | 35.3 | ----- |
| Indoor Radon Concentration (Becquerel per Cubic Meter; Bq/m3) | |
|---|---|
| Arithmetic mean | 45.97 * |
| Geometric mean (95% CI) | 37.75 (25.19–56.58) |
| Minimum | 9.25 |
| Maximum | 122.10 |
| Percentile | |
| 25th | 25.90 |
| 50th | 40.70 |
| 75th | 48.10 |
| 90th | 96.20 |
| 99th | 122.10 |
| Lymphoma Subtype | Cases (n) | IR * | IRR * (95% CI) | aIRR * (95% CI) | p-for-Trend |
|---|---|---|---|---|---|
| All Lymphomas | |||||
| ≤25th percentile (reference) | 970 | 34.25 | 1.00 | 1.00 | 0.35 |
| >25th to ≤50th percentile | 711 | 30.92 | 0.88 (0.70–1.10) | 0.89 (0.79–1.00) | |
| >50th to ≤75th percentile | 373 | 33.38 | 0.98 (0.73–1.32) | 0.90 (0.77–1.04) | |
| >75th percentile | 93 | 33.88 | 0.93 (0.67–1.30) | 1.05 (0.83–1.32) | |
| Hodgkin Lymphoma | |||||
| ≤25th percentile (reference) | 583 | 20.59 | 1.00 | 1.00 | 0.20 |
| >25th to ≤50th percentile | 391 | 17.00 | 0.86 (0.64–1.15) | 0.83 (0.71–0.98) | |
| >50th to ≤75th percentile | 227 | 20.32 | 0.99 (0.68–1.45) | 0.94 (0.77–1.14) | |
| >75th percentile | 47 | 17.12 | 0.81 (0.51–1.26) | 0.87 (0.63–1.20) | |
| NHL excluding BL | |||||
| ≤25th percentile (reference) | 289 | 10.20 | 1.00 | 1.00 | 0.96 |
| >25th to ≤50th percentile | 231 | 10.04 | 0.96 (0.74–1.25) | 1.00 (0.82–1.21) | |
| >50th to ≤75th percentile | 103 | 9.22 | 0.92 (0.66–1.29) | 0.82 (0.64–1.05) | |
| >75th percentile | 35 | 12.75 | 1.26 (0.83–1.93) | 1.37 (0.95–1.97) | |
| Burkitt Lymphoma | |||||
| ≤25th percentile (reference) | 98 | 3.46 | 1.00 | 1.00 | 0.54 |
| >25th to ≤50th percentile | 89 | 3.87 | 0.98 (0.65–1.48) | 1.01 (0.73–1.38) | |
| >50th to ≤75th percentile | 43 | 3.85 | 1.08 (0.64–1.80) | 1.04 (0.71–1.52) | |
| >75th percentile | 11 | 4.01 | 1.05 (0.52–2.14) | 1.33 (0.70–2.53) | |
| Diffuse Large B-Cell | |||||
| ≤25th percentile (reference) | 123 | 4.34 | 1.00 | 1.00 | 0.22 |
| >25th to ≤50th percentile | 119 | 5.17 | 1.11 (0.80–1.55) | 1.11 (0.85–1.44) | |
| >50th to ≤75th percentile | 56 | 5.01 | 1.11 (0.74–1.68) | 1.01 (0.73–1.39) | |
| >75th percentile | 17 | 6.19 | 1.42 (0.81–2.49) | 1.73 (1.03–2.91) |
3.2. Discussion
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Cancer Incidence and Survival among Children and Adolescents: United States Seer Program 1975–1995; Ries, L.S.M.; Gurney, J.; Linet, M.; Tamra, T.; Young, J.; Bunin, G. (Eds.) National Cancer Institute, SEER Program: Bethesda, MD, USA, 1999.
- American Cancer Society. Cancer Facts & Figures 2014; American Cancer Society: Atlanta, GA, USA, 2014. [Google Scholar]
- Englund, A.; Hopstadius, C.; Enblad, G.; Gustafsson, G.; Ljungman, G. Hodgkin lymphoma—A survey of children and adolescents treated in Sweden 1985–2009. Acta Oncol. 2015, 54, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Reiter, A. Non-Hodgkin lymphoma in children and adolescents. Klin. Padiatr. 2013, 225, S87–S93. [Google Scholar] [CrossRef] [PubMed]
- El-Galaly, T.C.; Mylam, K.J.; Bøgsted, M.; Brown, P.; Rossing, M.; Gang, A.O.; Haglund, A.; Arboe, B.; Clausen, M.R.; Jensen, P.; et al. Role of routine imaging in detecting recurrent lymphoma: A review of 258 patients with relapsed aggressive non-Hodgkin and Hodgkin lymphoma. Am. J. Hematol. 2014, 89, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Gebauer, J.; Fick, E.M.; Waldmann, A.; Langer, T.; Kreitschmann-Andermahr, I.; Lehnert, H.; Katalinic, A.; Brabant, G. Self-reported endocrine late effects in adults treated for brain tumours, Hodgkin and non-Hodgkin lymphoma—A registry based study in northern Germany. Eur. J. Endocrinol. 2015, 173, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Rihani, R.; Bazzeh, F.; Faqih, N.; Sultan, I. Secondary hematopoietic malignancies in survivors of childhood cancer. Cancer 2010, 116, 4385–4394. [Google Scholar] [CrossRef] [PubMed]
- Tieu, M.T.; Cigsar, C.; Ahmed, S.; Ng, A.; Diller, L.; Millar, B.A.; Crystal, P.; Hodgson, D.C. Breast cancer detection among young survivors of pediatric Hodgkin lymphoma with screening magnetic resonance imaging. Cancer 2014, 120, 2507–2513. [Google Scholar] [CrossRef] [PubMed]
- Venkatramani, R.; Kamath, S.; Wong, K.; Olch, A.J.; Malvar, J.; Sposto, R.; Goodarzian, F.; Freyer, D.R.; Keens, T.G.; Mascarenhas, L. Pulmonary outcomes in patients with Hodgkin lymphoma treated with involved field radiation. Pediatr. Blood Cancer 2014, 61, 1277–1281. [Google Scholar] [CrossRef] [PubMed]
- Robison, L.L.; Green, D.M.; Hudson, M.; Meadows, A.T.; Mertens, A.C.; Packer, R.J.; Sklar, C.A.; Strong, L.C.; Yasui, Y.; Zeltzer, L.K. Long-term outcomes of adult survivors of childhood cancer. Cancer 2005, 104, 2557–2564. [Google Scholar] [CrossRef] [PubMed]
- Miligi, L.; Benvenuti, A.; Mattioli, S.; Salvan, A.; Tozzi, G.A.; Ranucci, A.; Legittimo, P.; Rondelli, R.; Bisanti, L.; Zambon, P.; et al. Risk of childhood leukaemia and non-Hodgkin’s lymphoma after parental occupational exposure to solvents and other agents: The setil study. Occup. Environ. Med. 2013, 70, 648–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mcnally, R.J.Q.; Parker, L. Environmental factors and childhood acute leukemias and lymphomas. Leuk. Lymphoma 2006, 47, 583–598. [Google Scholar] [CrossRef] [PubMed]
- Lightfoot, T.J.; Roman, E. Causes of childhood leukaemia and lymphoma. Toxicol. Appl. Pharmacol. 2004, 199, 104–117. [Google Scholar] [CrossRef] [PubMed]
- Crump, C.; Sundquist, K.; Sieh, W.; Winkleby, M.A.; Sundquist, J. Perinatal and family risk factors for non-Hodgkin lymphoma in early life: A Swedish national cohort study. J. Natl. Cancer Inst. 2012, 104, 923–930. [Google Scholar] [CrossRef] [PubMed]
- Crump, C.; Sundquist, K.; Sieh, W.; Winkleby, M.A.; Sundquist, J. Perinatal and family risk factors for Hodgkin lymphoma in childhood through young adulthood. Am. J. Epidemiol. 2012, 176, 1147–1158. [Google Scholar] [CrossRef] [PubMed]
- Cogliano, V.J.; Baan, R.; Straif, K.; Grosse, Y.; Lauby-Secretan, B.; El Ghissassi, F.; Bouvard, V.; Benbrahim-Tallaa, L.; Guha, N.; Freeman, C.; et al. Preventable exposures associated with human cancers. J. Natl. Cancer Inst. 2011, 103, 1827–1839. [Google Scholar] [CrossRef] [PubMed]
- Darby, S.; Hill, D.; Doll, R. Radon: A likely carcinogen at all exposures. Ann. Oncol. 2001, 12, 1341–1351. [Google Scholar] [CrossRef] [PubMed]
- Zielinski, J.M.; Carr, Z.; Krewski, D.; Repacholi, M. World health organization’s international radon project. J. Toxicol. Environ. Health Part A 2006, 69, 759–769. [Google Scholar] [CrossRef] [PubMed]
- Kreuzer, M.; Grosche, B.; Schnelzer, M.; Tschense, A.; Dufey, F.; Walsh, L. Radon and risk of death from cancer and cardiovascular diseases in the German uranium miners cohort study: Follow-up 1946–2003. Radiat. Environ. Biophys. 2010, 49, 177–185. [Google Scholar] [CrossRef] [PubMed]
- William Field, R.; Krewski, D.; Lubin, J.H.; Zielinski, J.M.; Alavanja, M.; Catalan, V.S.; Klotz, J.B.; Létourneau, E.G.; Lynch, C.F.; Lyon, J.L.; et al. An overview of the North American residential radon and lung cancer case-control studies. J. Toxicol. Environ. Health Part A 2006, 69, 599–631. [Google Scholar] [CrossRef] [PubMed]
- Bräuner, E.V.; Andersen, Z.J.; Andersen, C.E.; Pedersen, C.; Gravesen, P.; Ulbak, K.; Hertel, O.; Loft, S.; Raaschou-Nielsen, O. Residential radon and brain tumour incidence in a Danish cohort. PLoS ONE 2013, 8. [Google Scholar] [CrossRef] [PubMed]
- Robertson, A.; Allen, J.; Laney, R.; Curnow, A. The cellular and molecular carcinogenic effects of radon exposure: A review. Int. J. Mol. Sci. 2013, 14, 14024–14063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Darby, S.H.D.; Deo, H.; Auvinen, A.; Barros-Dios, J.M.; Baysson, H.; Bochicchio, F.; Falk, R.; Farchi, S.; Figueiras, A.; Hakama, M.; et al. Residential radon and lung cancer—Detailed results of a collaborative analysis of individual data on 7148 persons with lung cancer and 14,208 persons without lung cancer from 13 epidemiologic studies in Europe. Scand. J. Work Environ. Health 2006, 32, 1–84. [Google Scholar] [PubMed]
- Krewski, D.; Lubin, J.H.; Zielinski, J.M.; Alavanja, M.; Catalan, V.S.; William Field, R.; Klotz, J.B.; Létourneau, E.G.; Lynch, C.F.; Lyon, J.L.; et al. A combined analysis of North American case-control studies of residential radon and lung cancer. J. Toxicol. Environ. Health Part A 2006, 69, 533–597. [Google Scholar] [CrossRef] [PubMed]
- Nezahat, H.; Colin, R.M.; Francesco, B.; Richard, G.E.H. Calculation of lifetime lung cancer risks associated with radon exposure, based on various models and exposure scenarios. J. Radiol. Prot. 2015, 35, 539–555. [Google Scholar]
- Tong, J.; Qin, L.; Cao, Y.; Li, J.; Zhang, J.; Nie, J.; An, Y. Environmental radon exposure and childhood leukemia. J. Toxicol. Environ. Health Part B 2012, 15, 332–347. [Google Scholar] [CrossRef] [PubMed]
- Wakefield, M.; Kohler, J.A. Indoor radon and childhood cancer. Lancet 1991, 338, 1537–1538. [Google Scholar] [CrossRef]
- Raaschou-Nielsen, O. Indoor radon and childhood leukaemia. Radiat. Prot. Dosim. 2008, 132, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Neuberger, J.S.; Gesell, T.F. Childhood cancers, radon, and γ radiations. Lancet 2002, 360, 1437–1438. [Google Scholar] [CrossRef]
- Raaschou-Nielsen, O.; Andersen, C.E.; Andersen, H.P.; Gravesen, P.; Lind, M.; Schüz, J.; Ulbak, K. Domestic radon and childhood cancer in Denmark. Epidemiology 2008, 19, 536–543. [Google Scholar] [PubMed]
- Henshaw, D.L.; Eatough, J.P.; Richardson, R.B. Radon as a causative factor in induction of myeloid leukaemia and other cancers. Lancet 1990, 335, 1008–1012. [Google Scholar] [CrossRef]
- NRC (National Research Council). Health Risks from Exposure to Low Levels of Ionizing Radiation; Beir VII Phase 2; NRC, National Academies Press: Washington, DC, USA, 2006. [Google Scholar]
- Zablotska, L.B.; Lane, R.S.D.; Frost, S.E.; Thompson, P.A. Leukemia, lymphoma and multiple myeloma mortality (1950–1999) and incidence (1969–1999) in the Eldorado uranium workers cohort. Environ. Res. 2014, 130, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.J.C.; Browning, T.; Ransom, S. Final Report of the Texas Indoor Radon Survey; Texas Department of Health: Austin, TX, USA, 1994. [Google Scholar]
- Langlois, P.H.; Lee, M.; Lupo, P.J.; Rahbar, M.H.; Cortez, R.K. Residential radon and birth defects: A population-based assessment. Birth Defects Res. Part A: Clin. Mol. Teratol. 2015. [Google Scholar] [CrossRef] [PubMed]
- Texas Cancer Registry, Cancer Epidemiology and Surveillance Branch, Texas Department of State Health Services. The Source of Cancer Data in Texas. Published 2015. Avaliable online: http://www.dshs.state.tx.us/tcr/default.shtm. (accessed on 5 May 2015).
- Steliarova-Foucher, E.S.C.; Lacour, B.; Kaatsch, P. International classification of childhood cancer, third edition. Cancer 2005, 103, 1457–1467. [Google Scholar] [CrossRef] [PubMed]
- Gardner, W.; Mulvey, E.P.; Shaw, E.C. Regression analyses of counts and rates: Poisson, overdispersed poisson, and negative binomial models. Psychol. Bull. 1995, 118, 392–404. [Google Scholar] [CrossRef] [PubMed]
- Hayat, M.J.; Higgins, M. Understanding poisson regression. J. Nurs. Educ. 2014, 53, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Coxe, S.; West, S.G.; Aiken, L.S. The analysis of count data: A gentle introduction to poisson regression and its alternatives. J. Personal. Assess. 2009, 91, 121–136. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.L.; Wilkinson, M.L.; Poston, W.S.C.; Keith Haddock, C.; Jahnke, S.A.; Sue Day, R. Adiposity predicts self-reported frequency of poor health days among male firefighters. J. Occup. Environ. Med. 2014, 56, 667–672. [Google Scholar] [CrossRef] [PubMed]
- Evrard, A.S.; Hémon, D.; Billon, S.; Laurier, D.; Jougla, E.; Tirmarche, M.; Clavel, J. Ecological association between indoor radon concentration and childhood leukaemia incidence in France, 1990–1998. Eur. J. Cancer Prev. 2005, 14, 147–157. [Google Scholar] [CrossRef] [PubMed]
- George, A.C. The history, development and the present status of the radon measurement programme in the United States of America. Radiat. Prot. Dosim. 2015. [Google Scholar] [CrossRef] [PubMed]
- Vogiannis, E.G.; Nikolopoulos, D. Radon sources and associated risk in terms of exposure and dose. Front. Public Health 2015, 2. [Google Scholar] [CrossRef] [PubMed]
- Casey, J.A.; Ogburn, E.L.; Rasmussen, S.G.; Irving, J.K.; Pollak, J.; Locke, P.A.; Schwartz, B.S. Predictors of indoor radon concentrations in Pennsylvania, 1989–2013. Environ. Health Perspect. 2015. [Google Scholar] [CrossRef] [PubMed]
- Hendry, J.H.; Simon, S.L.; Wojcik, A.; Sohrabi, M.; Burkart, W.; Cardis, E.; Laurier, D.; Tirmarche, M.; Hayata, I. Human exposure to high natural background radiation: What can it teach us about radiation risks? J. Radiol. Prot. 2009, 29, A29–A42. [Google Scholar] [CrossRef] [PubMed]
- Sam, K.; John, R.D.; Carolyn, H.; Moiz, M.; Oscar, T.; David, W.W.; Gary, L.D.; Mario, C.; Barber, L.E. Toxicological Profile for Radon. U.S. Department of Health and Human Services, P.H.S., Agency for Toxic Substances and Disease Registry; Agency for Toxic Substances and Disease Registry (US): Atlanta, GA, USA, 2012. [Google Scholar]
- Al-Zoughool, M.; Krewski, D. Health effects of radon: A review of the literature. Int. J. Radiat. Biol. 2009, 85, 57–69. [Google Scholar] [CrossRef] [PubMed]
- Darby, S.; Hill, D.; Auvinen, A.; Barros-Dios, J.M.; Baysson, H.; Bochicchio, F.; Deo, H.; Falk, R.; Forastiere, F.; Hakama, M.; et al. Radon in homes and risk of lung cancer: Collaborative analysis of individual data from 13 European case-control studies. BMJ 2005, 330. [Google Scholar] [CrossRef] [PubMed]
- Ruano-Ravina, A.; Pereyra, M.F.; Castro, M.T.; Pérez-Ríos, M.; Abal-Arca, J.; Barros-Dios, J.M. Genetic susceptibility, residential radon, and lung cancer in a radon prone area. J. Thorac. Oncol. 2014, 9, 1073–1080. [Google Scholar] [CrossRef] [PubMed]
- Torres-Durán, M.; Ruano-Ravina, A.; Parente-Lamelas, I.; Leiro-Fernández, V.; Abal-Arca, J.; Montero-Martínez, C.; Pena-Álvarez, C.; Castro-Añón, O.; Golpe-Gómez, A.; Martínez, C.; et al. Residential radon and lung cancer characteristics in never smokers. Int. J. Radiat. Biol. 2015. [Google Scholar] [CrossRef] [PubMed]
- Axelsson, G.; Andersson, E.; Barregard, L. Lung cancer risk from radon exposure in dwellings in Sweden: How many cases can be prevented if radon levels are lowered? Cancer Causes Control 2015, 26, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Hauri, D.; Spycher, B.; Huss, A.; Zimmermann, F.; Grotzer, M.; von der Weid, N.; Weber, D.; Spoerri, A.; Kuehni, C.; Röösli, M.; et al. Domestic radon exposure and risk of childhood cancer: A prospective census-based cohort study. Environ. Health Perspect. 2013, 121, 1239–1244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Řeřicha, V.; Kulich, M.; Řeřicha, R.; Shore, D.L.; Sandler, D.P. Incidence of leukemia, lymphoma, and multiple myeloma in Czech uranium miners: A case-cohort study. Environ. Health Perspect. 2006, 114, 818–822. [Google Scholar] [CrossRef] [PubMed]
- Rothman, K.J.; Mosquin, P.L. Sparse-data bias accompanying overly fine stratification in an analysis of beryllium exposure and lung cancer risk. Ann. Epidemiol. 2013, 23, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Barros-Dios, J.M.; Ruano-Ravina, A.; Gastelu-Iturri, J.; Figueiras, A. Factors underlying residential radon concentration: Results from Galicia, Spain. Environ. Res. 2007, 103, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Wakefield, J.; Elliott, P. Issues in the statistical analysis of small area health data. Stat. Med. 1999, 18, 2377–2399. [Google Scholar] [CrossRef]
- Muirhead, C.R.; Butland, B.K.; Green, B.M.R.; Draper, G.J. An analysis of childhood leukaemia and natural radiation in Britain. Radiat. Prot. Dosim. 1992, 45, 657–660. [Google Scholar]
- Collman, G.W.; Loomis, D.P.; Sandler, D.P. Childhood cancer mortality and radon concentration in drinking water in North Carolina. Br. J. Cancer 1991, 63, 626–629. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, W.K.; Schmitz-Feuerhake, I. Radium-226-contaminated drinking water: Hypothesis on an exposure pathway in a population with elevated childhood leukemia. Environ. Health Perspect. Suppl. 1993, 101, 113–115. [Google Scholar] [CrossRef]
- Kohli, S.N.B.H.; Löfman, O. Childhood leukaemia in areas with different radon levels: A spatial and temporal analysis using GIS. J. Epidemiol. Community Health 2000, 54, 822–826. [Google Scholar] [CrossRef] [PubMed]
- Thorne, R.F.N.; Mott, M.G. Radon in Devon and Cornwall and paediatric malignancies. Eur. J. Cancer 32A, 282–285. [CrossRef]
- Butland, B.K.; Muirhead, C.R.; Draper, G.J. Letters to the Editor: Radon and leukaemia. Lancet 1990, 335, 1338–1339. [Google Scholar]
- Whitworth, K.W.; Symanski, E.; Coker, A.L. Childhood lymphohematopoietic cancer incidence and hazardous air pollutants in southeast Texas, 1995–2004. Environ. Health Perspect. 2008, 116, 1576–1580. [Google Scholar] [CrossRef] [PubMed]
- Heck, J.E.; Wu, J.; Lombardi, C.; Qiu, J.; Meyers, T.J.; Wilhelm, M.; Cockburn, M.; Ritz, B. Childhood cancer and traffic-related air pollution exposure in pregnancy and early life. Environ. Health Perspect. 2013, 121, 1385–1391. [Google Scholar] [CrossRef] [PubMed]
- Danysh, H.E.; Mitchell, L.E.; Zhang, K.; Scheurer, M.E.; Lupo, P.J. Traffic-related air pollution and the incidence of childhood central nervous system tumors: Texas, 2001–2009. Pediatr. Blood Cancer 2015, 62, 1572–1578. [Google Scholar] [CrossRef] [PubMed]
- Scheurer, M.; Danysh, H.; Follen, M.; Lupo, P. Association of traffic-related hazardous air pollutants and cervical dysplasia in an urban multiethnic population: A cross-sectional study. Environ. Health 2014, 13, 52. [Google Scholar] [CrossRef] [PubMed]
- Urayama, K.Y.; von Behren, J.; Reynolds, P.; Hertz, A.; Does, M.; Buffler, P.A. Factors associated with residential mobility in children with leukemia: Implications for assigning exposures. Ann. Epidemiol. 2009, 19, 834–840. [Google Scholar] [CrossRef] [PubMed]
- Lupo, P.J.; Symanski, E.; Chan, W.; Mitchell, L.E.; Waller, D.K.; Canfield, M.A.; Langlois, P.H. Differences in exposure assignment between conception and delivery: The impact of maternal mobility. Paediatr. Perinat. Epidemiol. 2010, 24, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Canfield, M.A.; Ramadhani, T.A.; Langlois, P.H.; Waller, D.K. Residential mobility patterns and exposure misclassification in epidemiologic studies of birth defects. J. Expos. Sci. Environ. Epidemiol. 2006, 16, 538–543. [Google Scholar] [CrossRef] [PubMed]
- Rahman, N.M.; Tracy, B.L. Radon control systems in existing and new construction: A review. Radiat. Prot. Dosim. 2009, 135, 243–255. [Google Scholar] [CrossRef] [PubMed]
- Korhonen, P.; Halonen, R.; Kalliokoski, P.; Kokotti, H. Indoor radon concentrations caused by construction materials in 23 workplaces. Sci. Total Environ. 2001, 272, 143–145. [Google Scholar] [CrossRef]
- Keller, G.; Hoffmann, B.; Feigenspan, T. Radon permeability and radon exhalation of building materials. Sci. Total Environ. 2001, 272, 85–89. [Google Scholar] [CrossRef]
- Meinert, R.; Schüz, J.; Kaletsch, U.; Kaatsch, P.; Michaelis, J. Leukemia and non-Hodgkin’s lymphoma in childhood and exposure to pesticides: Results of a register-based case-control study in Germany. Am. J. Epidemiol. 2000, 151, 639–646. [Google Scholar] [CrossRef] [PubMed]
- Meinert, R.; Kaletsch, U.; Kaatsch, P.; Schüz, J.; Michaelis, J. Associations between childhood cancer and ionizing radiation: Results of a population-based case-control study in Germany. Cancer Epidemiol. Biomark. Prev. 1999, 8, 793–799. [Google Scholar]
- Spycher BD, L.J.; Zwahlen, M.; Röösli, M.; Niggli, F.; Grotzer, M.A.; Rischewski, J.; Egger, M.; Kuehni, C.E.; Swiss Pediatric Oncology Group; Swiss National Cohort Study Group. Background ionizing radiation and the risk of childhood cancer: A census-based nationwide cohort study. Environ. Health Perspect. 2015, 123, 622–628. [Google Scholar] [CrossRef] [PubMed]
- Allen, C.E.; Kelly, K.M.; Bollard, C.M. Pediatric lymphomas and histiocytic disorders of childhood. Pediatr. Clin. N. Am. 2015, 62, 139–165. [Google Scholar] [CrossRef] [PubMed]
- Diggle, P.; Elliott, P. Disease risk near point sources: Statistical issues for analyses using individual or spatially aggregated data. J. Epidemiol. Community Health 1995, 49, S20–S27. [Google Scholar] [CrossRef] [PubMed]
- Krieger, N.; Chen, J.T.; Waterman, P.D.; Rehkopf, D.H.; Subramanian, S.V. Painting a truer picture of us socioeconomic and racial/ethnic health inequalities: The public health disparities geocoding project. Am. J. Public Health 2005, 95, 312–323. [Google Scholar] [CrossRef] [PubMed]
- Yasui, Y.; Liu, Y.; Neglia, J.P.; Friedman, D.L.; Bhatia, S.; Meadows, A.T.; Diller, L.R.; Mertens, A.C.; Whitton, J.; Robison, L.L. A methodological issue in the analysis of second-primary cancer incidence in long-term survivors of childhood cancers. Am. J. Epidemiol. 2003, 158, 1108–1113. [Google Scholar] [CrossRef] [PubMed]
- Perez-Andreu, V.; Roberts, K.G.; Xu, H.; Smith, C.; Zhang, H.; Yang, W.; Harvey, R.C.; Payne-Turner, D.; Devidas, M.; Cheng, I.-M.; et al. A genome-wide association study of susceptibility to acute lymphoblastic leukemia in adolescents and young adults. Blood 2015, 125, 680–686. [Google Scholar] [CrossRef] [PubMed]
- Sultan, I.; Casanova, M.; Ferrari, A.; Rihani, R.; Rodriguez-Galindo, C. Differential features of nasopharyngeal carcinoma in children and adults: A seer study. Pediatr. Blood Cancer 2010, 55, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Hudson, T.J. Cancer genome variation in children, adolescents, and young adults. Cancer 2011, 117, 2262–2267. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peckham, E.C.; Scheurer, M.E.; Danysh, H.E.; Lubega, J.; Langlois, P.H.; Lupo, P.J. Residential Radon Exposure and Incidence of Childhood Lymphoma in Texas, 1995–2011. Int. J. Environ. Res. Public Health 2015, 12, 12110-12126. https://doi.org/10.3390/ijerph121012110
Peckham EC, Scheurer ME, Danysh HE, Lubega J, Langlois PH, Lupo PJ. Residential Radon Exposure and Incidence of Childhood Lymphoma in Texas, 1995–2011. International Journal of Environmental Research and Public Health. 2015; 12(10):12110-12126. https://doi.org/10.3390/ijerph121012110
Chicago/Turabian StylePeckham, Erin C., Michael E. Scheurer, Heather E. Danysh, Joseph Lubega, Peter H. Langlois, and Philip J. Lupo. 2015. "Residential Radon Exposure and Incidence of Childhood Lymphoma in Texas, 1995–2011" International Journal of Environmental Research and Public Health 12, no. 10: 12110-12126. https://doi.org/10.3390/ijerph121012110