The Impact of Water and Sanitation on Childhood Mortality in Nigeria: Evidence from Demographic and Health Surveys, 2003–2013


Abstract
:1. Introduction
2. Methods
2.1. Data Source
2.2. Outcome Variables
2.3. Exposure Variables

{kind=link}
| Variable | Improved | Unimproved |
|---|---|---|
| Water source | Piped water connection to household, public taps or standpipes, boreholes or tube wells, protected dug well, protected spring and rainwater collection. | Unprotected dug well, unprotected spring, cart with small tank or drum, surface water (e.g., river, dam, lake, pond, stream, canal or irrigation channel) and bottled water. |
| Sanitation facility | Pour-flush system, piped sewer system, septic tank, ventilated improved pit latrine (VIP) and pit latrine with slab. | Pit latrine without slab, bucket, hanging toilet or latrine, no facilities, bush or field and shared or public facility. |
2.4. Potential Confounding Variables
2.5. Statistical Analysis
3. Results and Discussion
| Variable | Total Live Births | % of Weighted Total ˟ | Prevalence ˟ by Survey (%) | |||
|---|---|---|---|---|---|---|
| Unweighted ʶ | Weighted ˟ | 2003 | 2008 | 2013 | ||
| Household environmental factor | ||||||
| Water (n = 61,995) | ||||||
| Improved water | 31,530 | 32,821 | 51.4 | 35.4 | 50.4 | 55.4 |
| Unimproved water | 30,531 | 29,174 | 45.7 | 62.9 | 47.7 | 40.6 |
| Sanitation (n = 62,994) | ||||||
| Improved | 28,416 | 30,086 | 47.1 | 12.6 | 51.1 | 50.3 |
| Unimproved | 34,511 | 32,908 | 51.6 | 85.8 | 47.0 | 48.9 |
| Combined water and sanitation (n = 61,648) | ||||||
| Improved water, improved sanitation | 18,106 | 19,680 | 30.8 | 9.7 | 31.2 | 34.6 |
| Improved water, unimproved sanitation | 13,299 | 13,013 | 20.4 | 25.7 | 18.8 | 20.7 |
| Unimproved water, improved sanitation | 9420 | 9370 | 14.7 | 2.9 | 19.1 | 13.1 |
| Unimproved water, unimproved sanitation | 20,878 | 19,585 | 30.7 | 60.0 | 27.8 | 27.5 |
| Socioeconomic factor | ||||||
| Residence type | ||||||
| Urban | 19,305 | 20,478 | 32.1 | 28.8 | 29.7 | 34.8 |
| Rural | 44,553 | 43,366 | 67.9 | 71.2 | 70.3 | 65.2 |
| Household wealth index | ||||||
| Poor | 25,243 | 23,783 | 37.3 | 42.3 | 40.2 | 33.6 |
| Middle | 25,262 | 25,569 | 40.1 | 40.5 | 37.7 | 42.0 |
| Rich | 13,353 | 14,492 | 22.7 | 17.2 | 22.1 | 24.3 |
| Mother’s education | ||||||
| No education | 31,203 | 30,947 | 48.5 | 51.8 | 46.7 | 49.4 |
| Primary | 13,871 | 13,539 | 21.2 | 23.6 | 23.0 | 19.1 |
| Secondary or higher | 18,784 | 19,357 | 30.3 | 24.5 | 30.2 | 31.5 |
| Mother’s literacy level (n = 63,532) | ||||||
| Cannot read at all | 38,905 | 38,283 | 60.0 | 63.9 | 59.4 | 59.7 |
| Able to read | 24,668 | 25,249 | 39.6 | 35.8 | 40.1 | 39.8 |
| Father’s education (n = 61,964) | ||||||
| No education | 24,634 | 24,365 | 38.2 | 39.7 | 37.1 | 38.8 |
| Primary | 12,825 | 12,843 | 20.1 | 23.0 | 21.5 | 18.4 |
| Secondary or higher | 24,431 | 24,756 | 38.8 | 34.0 | 38.2 | 40.2 |
| Mother’s working status (n = 61,857) | ||||||
| Not working | 21,544 | 21,289 | 33.3 | 37.4 | 34.6 | 31.5 |
| Working | 40,328 | 40,568 | 63.5 | 62.6 | 63.1 | 64.1 |
| Demographic factor | ||||||
| Currently breastfeeding | ||||||
| Yes | 35,885 | 35,691 | 55.9 | 58.2 | 56.4 | 55.0 |
| No | 27,973 | 28,153 | 44.1 | 41.8 | 43.6 | 45.0 |
| Mother’s age ( years) | ||||||
| <20 | 3460 | 3473 | 5.4 | 7.3 | 5.4 | 5.1 |
| 20–29 | 30,822 | 30,870 | 48.4 | 51.6 | 48.2 | 47.8 |
| 30–39 | 23,035 | 23,136 | 36.2 | 32.6 | 36.1 | 37.1 |
| 40–49 | 6541 | 6366 | 10.0 | 8.6 | 10.3 | 10.0 |
| Sex of child | ||||||
| Female | 31,385 | 31,491 | 49.3 | 48.8 | 49.1 | 49.6 |
| Male | 32,473 | 32,353 | 50.7 | 51.2 | 50.9 | 50.4 |
| Mother’s perceived baby size (n = 62,563) | ||||||
| Small or very small | 9107 | 9023 | 14.1 | 14.2 | 13.8 | 14.4 |
| Average or larger | 53,448 | 53,540 | 83.9 | 84.5 | 83.9 | 83.7 |
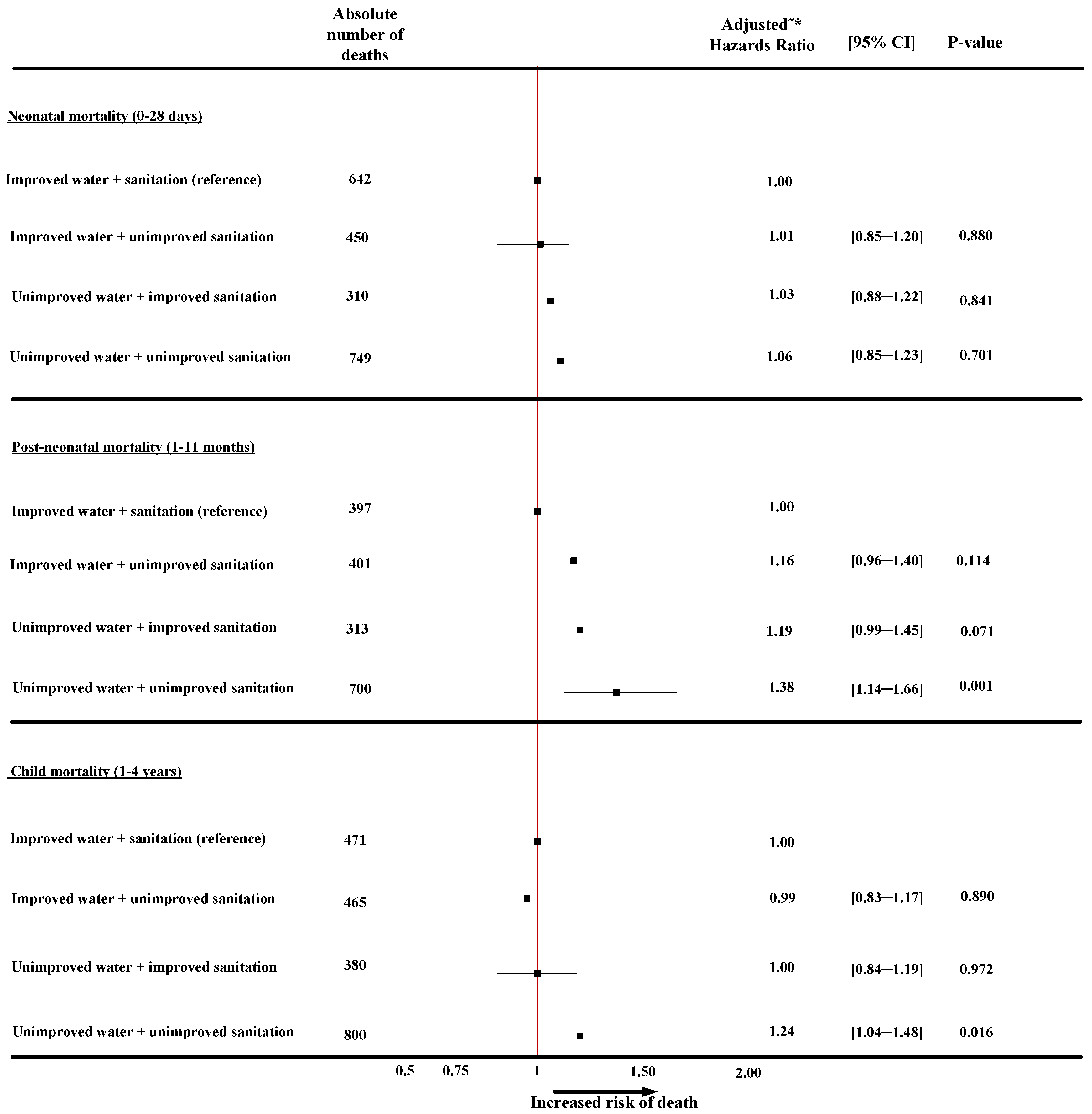
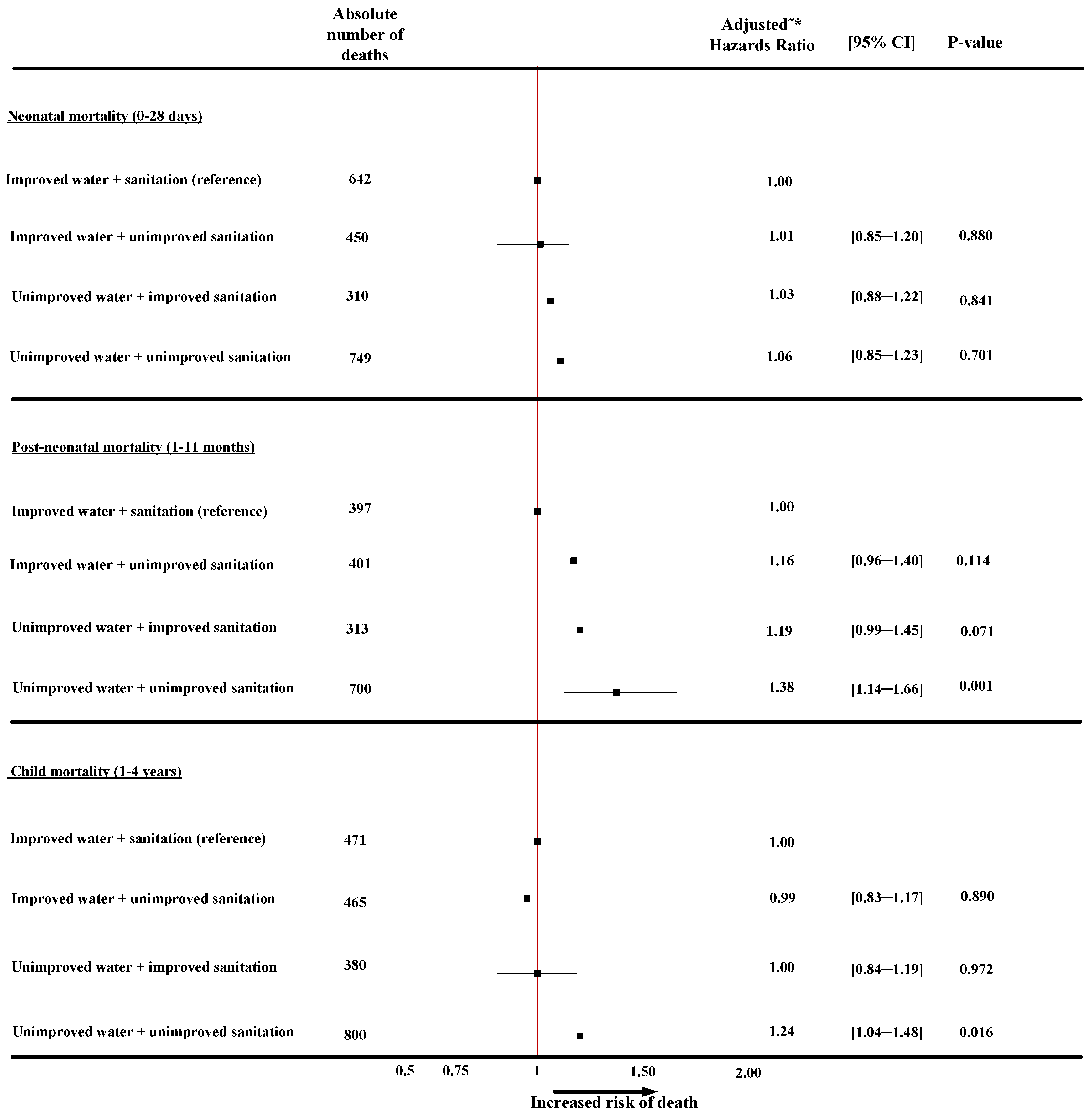
3.1. The Combined Effect of Water and Sanitation on Neonatal-Mortality
3.2. The Combined Effect of Water and Sanitation on Post-Neonatal Mortality
| Variables | (Model 0) ˇ | (Model 1) ^ | (Model 2) ^ | (Model 3) ^ | (Model 4) ^ |
|---|---|---|---|---|---|
| HR (95% CI) | HR (95% CI) | HR (95% CI) | HR (95% CI) | HR (95% CI) | |
| Year of survey | |||||
| 2003 | Ref | Ref | Ref | Ref | Ref |
| 2008 | 0.83 (0.69–1.01) | 0.86 (0.71–1.03) | 0.86 (0.71–1.03) | 0.86 (0.71–1.04) | 0.86 (0.71–1.04) |
| 2013 | 0.68 (0.56–0.82) | 0.69 (0.57–0.83) | 0.69 (0.57–0.84) | 0.69 (0.57–0.84) | 0.69 (0.57–0.85) |
| Socioeconomic factor | |||||
| Residence type | |||||
| Urban | Ref | ||||
| Rural | 1.46 (1.27–1.67) | ||||
| Household wealth index | |||||
| Rich | Ref | ||||
| Poor | 1.51 (1.28–1.78) | 1.38 (1.16–1.64) | 1.37 (1.14–1.64) | 1.37 (1.13–1.65) | 1.36 (1.12–1.65) |
| Middle | 1.28 (1.08–1.52) | 1.23 (1.04–1.46) | 1.22 (1.03–1.46) | 1.22 (1.02–1.46) | 1.22 (1.02–1.46) |
| Mother’s education | |||||
| Secondary or higher | Ref | ||||
| No education | 1.24 (1.07–1.44) | ||||
| Primary | 1.24 (1.06–1.46) | ||||
| Mother’s literacy level | |||||
| Able to read | Ref | ||||
| Cannot read at all | 1.24 (1.10–1.40) | ||||
| Father’s education | |||||
| Secondary or higher | Ref | ||||
| No education | 1.15 (1.02–1.31) | ||||
| Primary | 1.14 (0.98–1.32) | ||||
| Mother’s working status | |||||
| Not working | Ref | ||||
| Working | 0.83 (0.75–0.94) | ||||
| Demographic factor | |||||
| Mother’s age | |||||
| 30–39 | Ref | Ref | Ref | Ref | |
| <20 | 3.69 (2.98–4.58) | 3.46 (2.79–4.28) | 3.45 (2.79–4.27) | 3.46 (2.79–4.28) | 3.45 (2.79–4.27) |
| 20–29 | 1.17 (1.03–1.32) | 1.17 (1.03–1.33) | 1.17 (1.03–1.33) | 1.17 (1.04–1.33) | 1.17 (1.03–1.33) |
| 40–49 | 1.21 (1.00–1.47) | 1.09 (0.90–1.33) | 1.09 (0.90–1.33) | 1.09 (0.90–1.33) | 1.09 (0.90–1.33) |
| Sex of child | |||||
| Female | Ref | Ref | Ref | Ref | Ref |
| Male | 1.37 (1.23–1.53) | 1.39 (1.24–1.55) | 1.39 (1.24–1.55) | 1.39 (1.24–1.55) | 1.38 (1.24–1.55) |
| Mother’s perceived baby size | |||||
| Average or larger | Ref | Ref | Ref | Ref | Ref |
| Small or very small | 1.97 (1.74–2.34) | 1.93 (1.70–2.20) | 1.93 (1.70–2.20) | 1.94 (1.70–2.20) | 1.93 (1.70–2.20) |
| Currently breastfeeding | |||||
| Yes | Ref | Ref | Ref | Ref | Ref |
| No | 1.83 (1.62–2.06) | 1.95 (1.73–2.20) | 1.95 (1.73–2.20) | 1.95 (1.73–2.20) | 1.95 (1.73–2.20) |
| Household environmental factors | |||||
| Source of water | |||||
| Improved | Ref | Ref | |||
| Unimproved | 1.18 (1.06–1.33) | 1.02 (0.91–1.15) | |||
| Type of sanitation facility | |||||
| Improved | Ref | Ref | |||
| Unimproved | 1.20 (1.07–1.35) | 1.02 (0.89–1.16) |
| Variables | (Model 0) ˇ | (Model 1) ^ | (Model 2) ^ | (Model 3) ^ | (Model 4) ^ |
|---|---|---|---|---|---|
| HR (95% CI) | HR (95% CI) | HR (95% CI) | HR (95% CI) | HR (95% CI) | |
| Year of survey | |||||
| 2003 | Ref | Ref | Ref | Ref | Ref |
| 2008 | 0.70 (0.58–0.85) | 0.73 (0.61–0.89) | 0.75 (0.62–0.91) | 0.74 (0.60–0.90) | 0.73 (0.60–0.90) |
| 2013 | 0.55 (0.45–0.67) | 0.57 (0.47–0.70) | 0.59 (0.48–0.73) | 0.58 (0.47–0.71) | 0.59 (0.47–0.72) |
| Socioeconomic factor | |||||
| Residence type | |||||
| Urban | Ref | ||||
| Rural | 1.51 (1.30–1.75) | ||||
| Household wealth index | |||||
| Rich | Ref | Ref | Ref | Ref | Ref |
| Poor | 2.08 (1.72–2.51) | 1.75 (1.42–2.15) | 1.64 (1.32–2.04) | 1.73 (1.37–2.18) | 1.60 (1.27–2.03) |
| Middle | 1.72 (1.42–2.07) | 1.56 (1.28–1.89) | 1.51 (1.23–1.84) | 1.55 (1.26–1.89) | 1.46 (1.18–1.80) |
| Mother’s education | |||||
| Secondary or higher | Ref | ||||
| No education | 1.57 (1.34–1.83) | ||||
| Primary | 1.21 (1.01–1.45) | ||||
| Mother’s literacy level | |||||
| Able to read | Ref | ||||
| Cannot read at all | 1.54 (1.35–1.76) | ||||
| Father’s education | |||||
| Secondary or higher | Ref | Ref | Ref | Ref | Ref |
| No education | 1.53 (1.33–1.75) | 1.24 (1.07–1.45) | 1.23 (1.06–1.43) | 1.25 (1.07–1.45) | 1.22 (1.05–1.42) |
| Primary | 1.32 (1.11–1.57) | 1.15 (0.97–1.37) | 1.15 (0.96–1.36) | 1.15 (0.97–1.37) | 1.14 (0.96–1.36) |
| Mother’s working status | |||||
| Not working | Ref | ||||
| Working | 0.86 (0.77–0.96) | ||||
| Demographic factor | |||||
| Mother’s age | |||||
| 30–39 | Ref | Ref | Ref | Ref | Ref |
| < 20 | 3.54 (2.80–4.47) | 3.10 (2.44–3.95) | 3.08 (2.42–3.91) | 3.10 (2.44–3.95) | 3.07 (2.42–3.90) |
| 20–29 | 1.18 (1.04–1.33) | 1.15 (1.02–1.31) | 1.15 (1.02–1.31) | 1.15 (1.02–1.31) | 1.15 (1.02–1.31) |
| 40–49 | 1.01 (0.83–1.23) | 0.89 (0.74–1.09) | 0.90 (0.74–1.09) | 0.89 (0.74–1.09) | 0.90 (0.74–1.09) |
| Sex of child | |||||
| Female | Ref | ||||
| Male | 1.03 (0.92–1.15) | ||||
| Mother’s perceived baby size | |||||
| Average or larger | Ref | Ref | Ref | Ref | Ref |
| Small or very small | 1.29 (1.12–1.49) | 1.19 (1.03–1.37) | 1.18 (1.03–1.36) | 1.17 (1.02–1.35) | 1.18 (1.03–1.36) |
| Currently breastfeeding | |||||
| Yes | Ref | Ref | Ref | Ref | Ref |
| No | 1.37 (1.22–1.55) | 1.51 (1.34–1.70) | 1.51 (1.34–1.71) | 1.51 (1.34–1.70) | 1.52 (1.34–1.71) |
| Household environmental factors | |||||
| Source of water | |||||
| Improved | Ref | Ref | |||
| Unimproved | 1.44 (1.27–1.62) | 1.16 (1.02–1.31) | |||
| Type of sanitation facility | |||||
| Improved | Ref | Ref | |||
| Unimproved | 1.35 (1.19–1.53) | 1.02(0.88–1.17) |
3.3. The Combined Effect of Water and Sanitation on Child Mortality
| Variables | (Model 0) ˇ | (Model 1) ^ | (Model 2) ^ | (Model 3) ^ | (Model 4) ^ |
|---|---|---|---|---|---|
| HR (95% CI) | HR (95% CI) | HR (95% CI) | HR (95% CI) | HR (95% CI) | |
| Year of survey | |||||
| 2003 | Ref | Ref | Ref | Ref | Ref |
| 2008 | 0.76 (0.62–0.93) | 0.79 (0.66–0.95) | 0.80 (0.67–0.97) | 0.76 (0.63–0.92) | 0.76 (0.63–0.92) |
| 2013 | 0.52 (0.42–0.63) | 0.54 (0.45–0.66) | 0.55 (0.45–0.67) | 0.52 (0.43–0.64) | 0.53 (0.43–0.64) |
| Socioeconomic factor | |||||
| Residence type | |||||
| Urban | Ref | ||||
| Rural | 2.31 (1.98–2.69) | ||||
| Household wealth index | |||||
| Rich | Ref | Ref | Ref | Ref | Ref |
| Poor | 3.21 (2.68–3.84) | 2.29 (1.87–2.79) | 2.21 (1.80–2.71) | 2.45 (1.97–3.06) | 2.33 (1.86–2.90) |
| Middle | 2.37 (1.98–2.84) | 1.95 (1.61–2.36) | 1.91 (1.58–2.32) | 2.03 (1.67–2.47) | 1.95 (1.60–2.37) |
| Mother’s education | |||||
| Secondary or higher | Ref | ||||
| No education | 3.13 (2.64–3.72) | ||||
| Primary | 2.04 (1.68–2.47) | ||||
| Mother’s literacy level | |||||
| Able to read | Ref | ||||
| Cannot read at all | 2.46 (2.14–2.84) | ||||
| Father’s education | |||||
| Secondary or higher | Ref | Ref | Ref | Ref | Ref |
| No education | 2.36 (2.05–2.71) | 1.80 (1.54–2.09) | 1.78 (1.53–2.08) | 1.79 (1.53–2.08) | 1.76 (1.51―2.06) |
| Primary | 1.78 (1.53–2.07) | 1.45 (1.24–1.69) | 1.44 (1.24–1.68) | 1.45 (1.24–1.69) | 1.44 (1.23―1.68) |
| Mother’s working status | |||||
| Not working | Ref | ||||
| Working | 0.81 (0.72–0.91) | ||||
| Demographic factor | |||||
| Mother’s age | |||||
| 30–39 | Ref | ||||
| <20 | 1.54 (1.15–2.05) | ||||
| 20–29 | 1.10 (0.98–1.22) | ||||
| 40–49 | 1.20 (1.03–1.41) | ||||
| Sex of child | |||||
| Female | Ref | ||||
| Male | 1.05 (0.95–1.17) | ||||
| Mother’s perceived baby size | |||||
| Average or larger | Ref | ||||
| Small or very small | 1.35 (1.17–1.55) | ||||
| Currently breastfeeding | |||||
| Yes | Ref | Ref | Ref | Ref | Ref |
| No | 1.03 (0.93–1.14) | 1.13 (1.02–1.25) | 1.13 (1.02–1.26) | 1.13 (1.02–1.25) | 1.13 (1.02―1.26) |
| Household environmental factors | |||||
| Source of water | |||||
| Improved | Ref | Ref | |||
| Unimproved | 1.50 (1.33–1.69) | 1.09 (0.96–1.23) | |||
| Type of sanitation facility | |||||
| Improved | Ref | Ref | |||
| Unimproved | 1.34 (1.19–1.51) | 0.89 (0.79–1.02) |
3.4. Discussion
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Diarrhoea: Why Children are still Dying and What Can Be Done; UNICEF/WHO: Geneva, Switzerland, 2009.
- Report of the Joint Monitoring Programme: Progress on Sanitation and Drinking-Water; UNICEF/WHO: New York, NY, USA, 2013.
- Progress on Drinking Water and Sanitation Joint Monitoring Programme; UNICEF/WHO: Geneva, Switzerland, 2012.
- Fayehun, O.A. Household Environmental Health Hazards and Child Survival in Sub-Saharan Africa. DHS Working papers, Demographic and Health Research 2010, No. 74. Available online: http://dhsprogram.com/pubs/pdf/WP74/WP74.pdf (accessed on 15 May 2013).
- The Physical School Environment: An Essential Element of a Health-Promoting School; WHO: Geneva, Switzerland, 2003.
- USAID. Nigeria Water and Sanitation Profile. March 2010. Available online: www.washplus.org/sites/default/files/nigeria.pdf (accessed on 25 August 2013).
- Effective Financing of Local Governments to Provide Water and Sanitation Services, August 2008; WaterAid Nigeria: Abuja, Nigeria, 2008.
- Fort, A.L.; Kothari, M.T.; Abderrahim, N. Association between Maternal, Birth, and Newborn Characteristics and Neonatal Mortality in Five Asian Countries. DHS Working Papers 2008, No. 55. Available online: http://www.path.org/publications/files/MCHN_dhs_nnm_asian.pdf (accessed on 29 December 2012).
- Aiello, A.E.; Larson, E.L.; Sedlak, R. Hidden heroes of the health revolution Sanitation and personal hygiene. Amer. J. Infect. Control 2008, 36, S128–S151. [Google Scholar] [CrossRef]
- Fink, G.; Günther, I. The Impact and Cost of Water and Sanitation Infrstructure; Development Economics Prospects Group, World Bank: Zurich, Switzerland, 2011. [Google Scholar]
- National Population Commission, Federal Republic of Nigeria. Final Report on Nigeria Demographic and Health Survey; ORC Macro: Calverton, MD, USA, 2013.
- Levels and Trends in Child Mortality; UNICEF/WHO: Geneva, Switzerland, 2012.
- UNICEF Nigeria. Launch of Hand Washing Campaign in Abuja. 2008. Available online: http://www.unicef.org/nigeria/media_2364.html (accessed on 15 January 2014).
- National Population Commission, Federal Republic of Nigeria. Final Report on Nigeria Demographic and Health Survey 2008; ORC Macro: Calverton, MD, USA.
- National Population Commission, Federal Republic of Nigeria. Final Report on Nigeria Demographic and Health Survey 2003; ORC Macro: Calverton, MD, USA.
- Fink, G.; Günther, I. Water, Sanitation and Children’s Health: Evidence from 172 DHS Surveys; Development Economics Prospects Group, World Bank: Zurich, Switzerland, 2010. [Google Scholar]
- Woldemicael, G. The effects of water supply and sanitation on childhood mortality in urban Eritrea. J. Biosoc. Sci. 2000, 32, 207–227. [Google Scholar] [CrossRef]
- Fink, G.; Günther, I.; Hill, K. The effect of water and sanitation on child health: Evidence from the demographic and health surveys 1986–2007. Int. J. Epidemiol. 2011, 40, 1196–1204. [Google Scholar] [CrossRef]
- Titaley, C.R.; Dibley, M.J.; Roberts, C.L.; Hall, J.; Agho, K. Iron and folic acid supplements and reduced early neonatal deaths in Indonesia. Bull. WHO 2010, 88, 500–508. [Google Scholar]
- Deon, F.; Pritchett, L.H. Estimating wealth effects without expenditure data—Or tears: An application to educational enrollments in states of India. Demography 2001, 38, 115–132. [Google Scholar]
- Rutstein, S.; Rojas, G. Guide to Demographic and Health Survey (DHS); ORC Macro: Calverton, MD, USA, 2006. [Google Scholar]
- Ali, H.A. The Effect of Water and Sanitation on Child Mortality in Egypt; Environmental Economics Unit, Göteborg University: Göteborg, Sweden, 2003. [Google Scholar]
- Obungu, W.; Kizito, P.M.; Bicego, G. Trends, Age Patterns, and Determinants of Early Childhood Mortality in Kenya. Available online: http://www.dhsprogram.com/pubs/pdf/FA12/FA12.pdf (accessed on 17 November 2013).
- Habicht, J.P.; Davanzo, J.; Butz, W.P. Does breast-feeding really save lives, or are apparent benefits due to biases? Amer. J. Epidemiol. 1986, 123, 279–290. [Google Scholar]
- Victora, C.G.; Smith, P.G.; Vaughan, J.P.; Nobre, L.C.; Lombardi, C.; Teixeira, A.M.; Fuchs, S.C.; Moreira, L.B.; Gigante, L.P.; Barros, F.C. Infant feeding and deaths due to diarrhea: A case-control study. Amer. J. Epidemiol. 1989, 129, 1032–1041. [Google Scholar]
- Huttly, S.R.; Blum, D.; Kirkwood, B.R.; Emeh, R.N.; Feachem, R.G. The epidemiology of acute diarrhoea in a rural community in Imo State, Nigeria. Trans. Roy. Soc. Trop. Med. Hyg. 1987, 81, 865–870. [Google Scholar]
- VanDerslice, J.; Popkin, B.; Briscoe, J. Drinking-water quality, sanitation, and breast-feeding: Their interactive effects on infant health. Bull. WHO 1994, 72, 589–601. [Google Scholar]
- Trussell, J.; Hammerslough, C. A hazards—Model analysis of the covariates of infant and child mortality in Sri Lanka. Demography 1983, 20, 1–26. [Google Scholar] [CrossRef]
- Jinadu, M.K.; Olusi, S.O.; Agun, J.I.; Fabiyi, A.K. Childhood diarrhoea in rural Nigeria. I. Studies on prevalence, mortality and socio-environmental factors. J. Diarrhoeal Dis. Res. 1991, 9, 323–327. [Google Scholar]
- Jaspan, H.B.; Lawn, S.D.; Safrit, J.T.; Bekker, L. The maturing immune system: Implications for development and testing HIV-1 vaccines for children and adolescents. Aids 2006, 20, 483–494. [Google Scholar]
- Agha, S. The determinants of infant mortality in Pakistan. Soc. Sci. Med. 2000, 51, 199–208. [Google Scholar]
- Oti, S.O.; Odimegwu, C. Perinatal mortality in Nigeria: Do place of delivery and delivery assistants matter? Open Demogr. J. 2011, 4, 1–10. [Google Scholar]
- Golding, J.; Greenwood, R.; McCaw-Binns, A.; Thomas, P. Associations between social and environmental factors and perinatal mortality in Jamaica. Paediatr. Perinat. Epidemiol. 1994, 8, 17–39. [Google Scholar] [CrossRef]
- Mutunga, C.J. Environmental Determinants of Child Mortality in Kenya. Available online: http://www.econstor.eu/handle/10419/63263 (accessed on 10 November 2012).
- Khoury, M.J.; Marks, J.S.; McCarthy, B.J.; Zaro, S.M. Factors affecting the sex differential in neonatal mortality: The role of respiratory distress syndrome. Amer. J. Obstet. Gynecol. 1985, 151, 777–782. [Google Scholar]
- Mondal, N.; Hossain, K.; Ali, K. Factors influencing infant and child mortality: A case study of Rajshahi District, Bangladesh. J. Hum. Ecol. 2009, 26, 31–39. [Google Scholar]
- Neumann, L.E.; Moglia, M.; Cook, S.; Nguyen, M.N.; Sharma, A.K.; Nguyen, T.H.; Nguyen, B.V. Water use, sanitation and health in a fragmented urban water system: Case study and household survey. Urban Water J. 2013, 11, 198–210. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Ezeh, O.K.; Agho, K.E.; Dibley, M.J.; Hall, J.; Page, A.N. The Impact of Water and Sanitation on Childhood Mortality in Nigeria: Evidence from Demographic and Health Surveys, 2003–2013. Int. J. Environ. Res. Public Health 2014, 11, 9256-9272. https://doi.org/10.3390/ijerph110909256
Ezeh OK, Agho KE, Dibley MJ, Hall J, Page AN. The Impact of Water and Sanitation on Childhood Mortality in Nigeria: Evidence from Demographic and Health Surveys, 2003–2013. International Journal of Environmental Research and Public Health. 2014; 11(9):9256-9272. https://doi.org/10.3390/ijerph110909256
Chicago/Turabian StyleEzeh, Osita K., Kingsley E. Agho, Michael J. Dibley, John Hall, and Andrew N. Page. 2014. "The Impact of Water and Sanitation on Childhood Mortality in Nigeria: Evidence from Demographic and Health Surveys, 2003–2013" International Journal of Environmental Research and Public Health 11, no. 9: 9256-9272. https://doi.org/10.3390/ijerph110909256