Overall Accessibility to Traveling by Rail for the Elderly with and without Functional Limitations: The Whole-Trip Perspective

Abstract
:1. Introduction
Definition of Concepts
2. Research Problems
- To model overall accessibility grounded in elderly travelers’ functional ability, their travel behavior and the barriers encountered in the environment.
- To explore how railway accessibility is related to functional ability, travel behavior and barriers in the travel environment for the elderly.
- To determine functional ability and its relationships to kinds and number of functional limitations/diseases in the elderly.
- To determine barriers encountered in the whole-trip travel environment by the elderly with varying degrees of functional ability and kinds of functional limitations/diseases.
- To determine travel behavior in the whole-trip travel environment as a function of functional ability for older persons with various kinds of functional limitations/diseases.
- To determine travel behavior as a function of barriers encountered by the elderly with varying functional ability and kinds of functional limitations/diseases.
3. Method
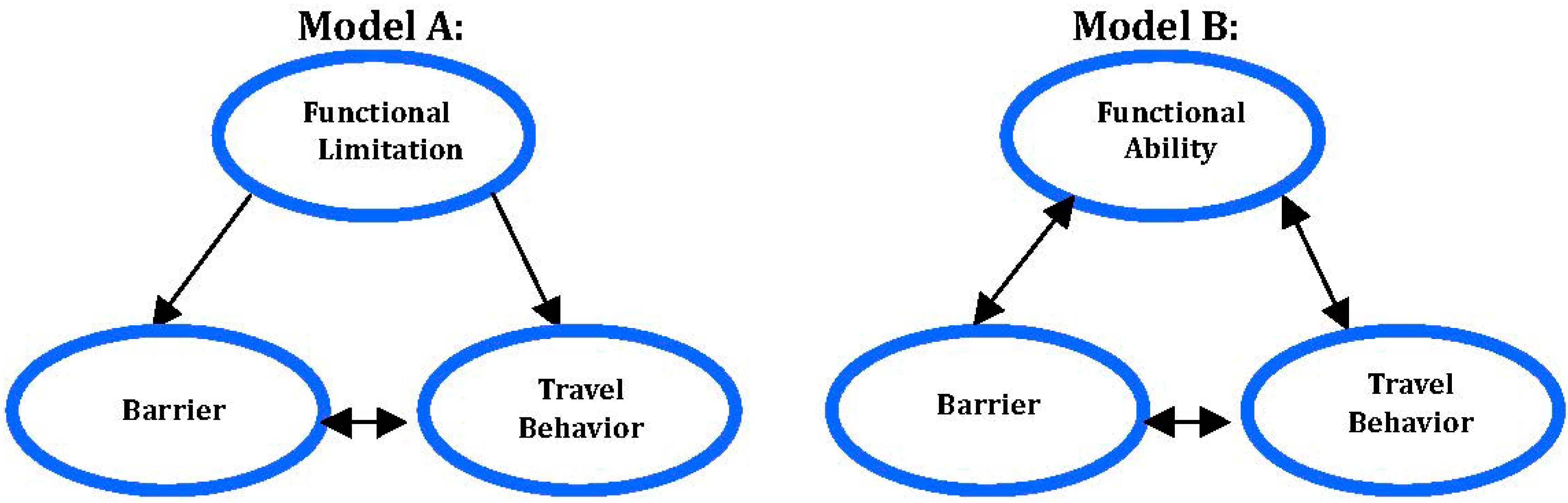
3.1. Theoretical Model
3.2. The Sample and Procedure
3.3. The Self-Report Questionnaire

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Descriptive | Reduction in Functional Ability | ||||
|---|---|---|---|---|---|
| All n (%) | None n (%) | Somewhat n (%) | Very n (%) | Cramér’s V (p) | |
| Gender: | 0.11 (0.026) | ||||
| Women | 312 (54) | 177 (58) | 109 (36) | 21 (7) | |
| Men | 262 (46) | 141 (56) | 106 (42) | 6 (2) | |
| Age: | 0.14 (0.004) | ||||
| 65–74 | 314 (55) | 192 (63) | 104 (34) | 10 (3) | |
| 75–85 | 257 (45) | 124 (49) | 110 (44) | 17 (7) | |
| Retired: | 568 (95) | 295 (56) | 206 (39) | 26 (5) | 0.06 (0.321) |
| Income/month (SEK): | 0.17 (0.000) | ||||
| 0–16 499 | 148 (27) | 62 (43) | 71 (49) | 12 (8) | |
| 16 500–33 499 | 228 (42) | 121 (54) | 89 (40) | 12 (5) | |
| 33 500 and above | 165 (30) | 116 (71) | 47 (29) | 1 (1) | |
| Living: | 0.09 (0.107) | ||||
| Family/nursing home | 390 (68) | 229 (60) | 135 (35) | 17 (4) | |
| Alone | 181 (32) | 89 (51) | 77 (44) | 10 (6) | |
| Car in household: | 408 (71) | 240 (60) | 148 (37) | 11 (3) | 0.17 (˂0.001) |
| Driver’s license: | 458 (80) | 262 (58) | 174 (39) | 13 (3) | 0.18 (˂0.001 |
| Discount card: | 439 (77) | 266 (62) | 158 (37) | 6 (1) | 0.23 (˂0.001) |
| Mobility service: | 43 (8) | 5 (12) | 22 (52) | 15 (36) | 0.33 (˂0.001) |
3.4. Six Constructs and Their Measurement
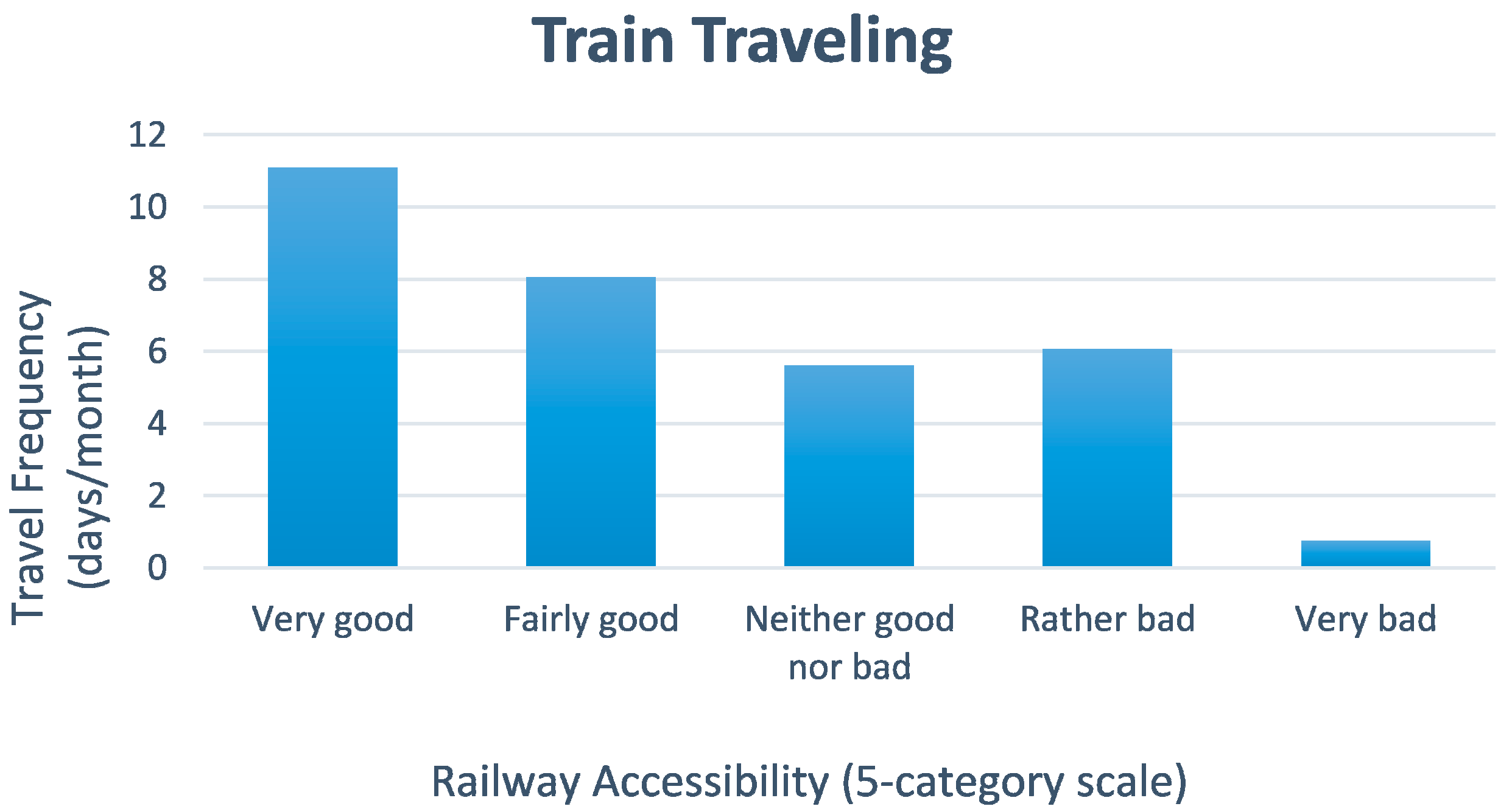
- Railway accessibility: The perceived railway accessibility was measured in one question (5-category scale).
- Functional limitation/disease: Self-reported functional limitations/diseases were assessed by one question with 15 response categories. The categories were selected through literature review of functional limitations and of transport research. Here, functional limitation/disease refers to a medical diagnosis or symptom. Three additional questions assessed authority-evaluated needs, e.g., mobility service, disabled parking permit and one question on disability aids (eight response categories).
- Functional ability: Self-reported degree of functional ability and health status (5-category scales). Functional ability refers to the self-reported severity of one’s functional limitation(s) or disease(s).
- Travel behavior: Actual travel behavior was assessed with questions on the following eight travel aspects: travel frequency, mode of conveyance, destination, purpose of trip, ticket purchase, luggage brought, travel companion(s), and change of transportation modes.
- Barrier: The main part of the questionnaire measured the perceptions of specific barriers in the travel environment encountered during the whole trip (i.e., the whole travel chain, door-to-door). Subsections were on barriers in: (a) long-distance train traveling, (b) train traveling in general, and (c) public transport, including other transport modes than train. The questions on barriers were in the format of scales and open questions. Additionally, one question contained 30 alternatives regarding willingness to travel more often by long-distance train depending on different potential barriers. Thus, most barriers were pre-defined by us and selected through literature review, although the respondent were also allowed to suggest barriers.
- Overall accessibility: Taken together, the five empirical constructs presented above [(a) railway accessibility; (b) functional limitation/disease; (c) functional ability; (d) travel behavior; and (e) barriers)], constitute the theoretical construct “overall accessibility” to whole-trip traveling.
4. Results of Questionnaire Study
4.1. Functional Limitations/Diseases
- (a).
- cognitive deficits in attention/memory/concentration and reading/writing/speech (ρ = 0.40, n = 7),
- (b).
- musculoskeletal impairments with chronic pain and restricted mobility (ρ = 0.39, n = 31), and
- (c).
- sensory impairments regarding hearing and vision (ρ = 0.32, n = 56).
| Functional Limitation/Disease 1 | Degree of Reduction in Functional Ability 2 | N 1 | Cramér’s V 3 Value (p) | ||
|---|---|---|---|---|---|
| None (a) n (%) | Somewhat (b), (c) n (%) | Very (d), (e) n (%) | |||
| No functional limitation/disease | 106 (80) | 19 (18) | 2 (2) | 127 | 0.23 (˂0.001) |
| Restricted mobility | 7 (9) | 56 (69) | 18 (22) | 81 | 0.46 (˂0.001) |
| Chronic pain | 8 (14) | 35 (64) | 12 (22) | 55 | 0.34 (˂0.001) |
| Reading, writing or speech disability | 0 (0) | 6 (50) | 6 (50) | 12 | 0.32 (˂0.001) |
| Attention, memory or concentration disability Chest disease | 4 (17) 4 (16) | 13 (56) 16 (64) | 6 (26) 5 (20) | 23 25 | 0.24 (˂0.001) 0.21 (˂0.001) |
| Rheumatic disease | 5 (19) | 16 (62) | 5 (19) | 26 | 0.20 (˂0.001) |
| Cardiovascular disease | 34 (35) | 56 (58) | 6 (6) | 96 | 0.20 (˂0.001) |
| Hearing impairment | 47 (40) | 63 (53) | 9 (8) | 119 | 0.18 (˂0.001) |
| Vision impairment | 49 (40) | 62 (51) | 10 (8) | 121 | 0.17 (˂0.001) |
| Mental ill-health | 4 (24) | 11 (65) | 2 (12) | 17 | 0.12 (0.017) |
| Neurological disorder | 3 (25) | 8 (67) | 1 (8) | 12 | 0.09 (0.086) |
| Diabetes | 29 (48) | 26 (43) | 6 (19) | 61 | 0.09 (0.095) |
| Asthma, allergy, hyper- sensitivity | 29 (45) | 31 (48) | 4 (6) | 64 | 0.08 (0.164) |
| Epilepsy | 2 (40) | 2 (40) | 1 (20) | 5 | 0.07 (0.270) |
| Travel sickness Respondent suggested FL/D | 11 (58) | 8 (42) | 0 (0) | 19 67 | 0.04 (0.600) |
4.1.1. Age and Gender
4.1.2. Jointly Existing Functional Limitations/Diseases
| Functional Limitations/Diseases | PCA Component 1 |
|---|---|
| Functional Limitations: | |
| Attention, memory or concentration disability | C1 (0.83) |
| Reading, writing or speech disability | C1 (0.72) |
| Mental ill-health | C1 (0.54) |
| Chronic pain | C2 (0.79) |
| Restricted mobility | C2 (0.74) |
| Hearing impairment | C3 (0.78) |
| Vision impairment | C3 (0.73) |
| Diseases: | |
| Chest disease | C4 (0.68) |
| Cardiovascular disease | C4 (0.60) |
| Asthma, allergy, hypersensitivity | C4 (0.59), C5 (41) |
| Epilepsy | C5 (0.80) |
| Neurological disorder | C2 (0.34), C5 (0.51) |
| Rheumatic disease | C6 (0.77) |
| Diabetes | C3 (0.40), C6 (0.55) |
| Travel sickness | C7 (0.55) |
4.2. Functional Ability
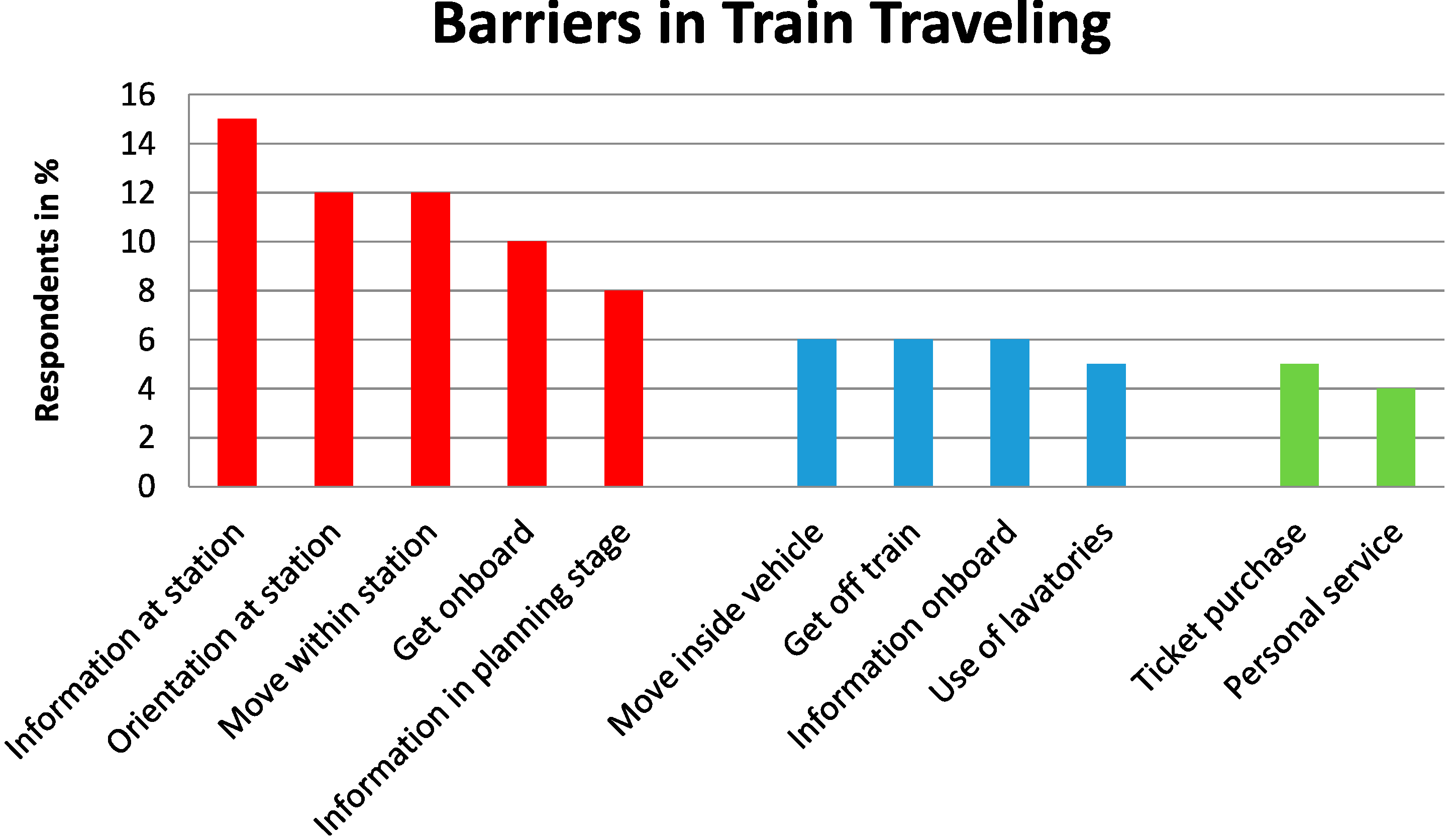
4.3. Barriers

4.4. Travel Behavior
- (a)
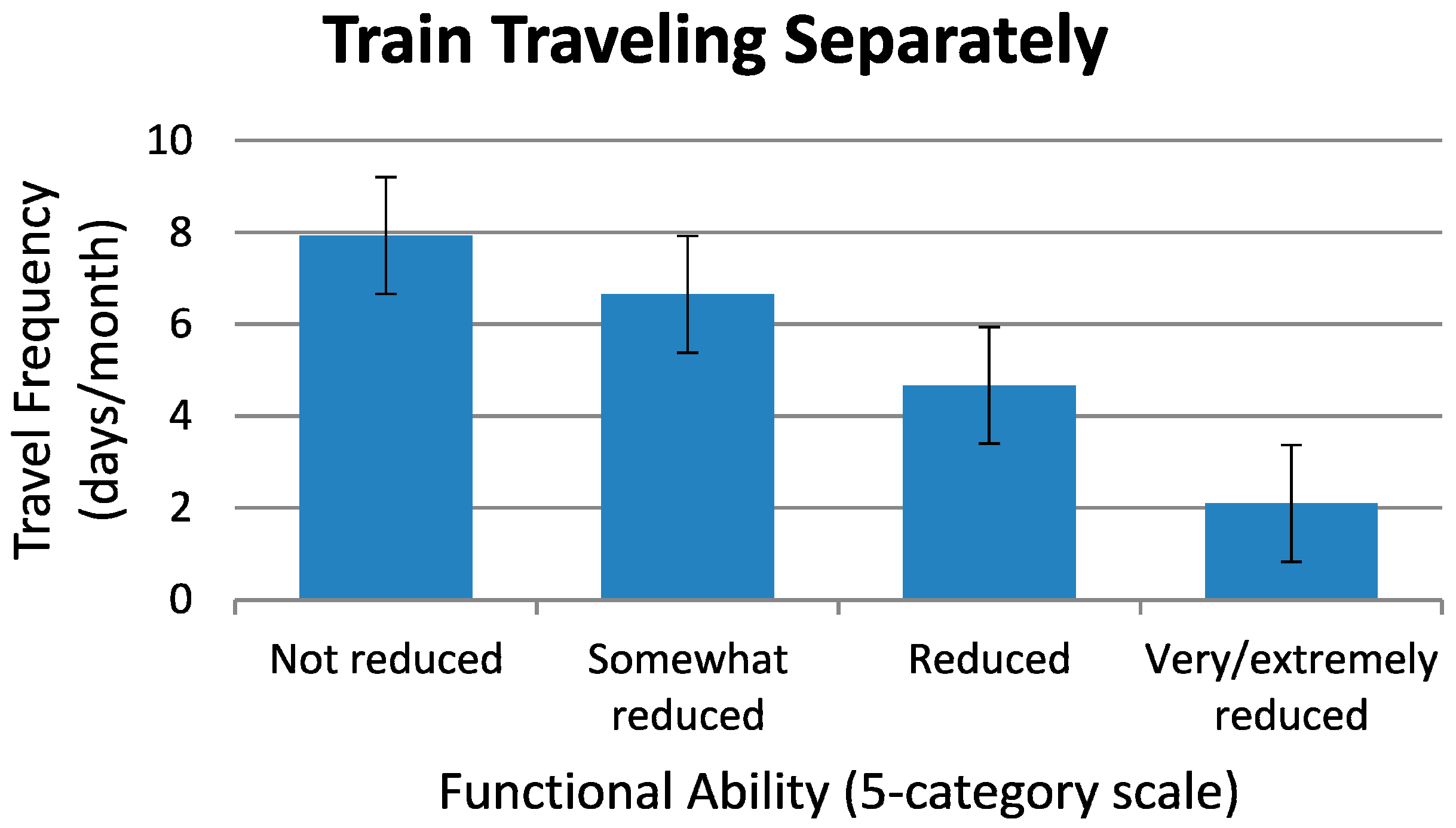
- Train traveling. The respondents were found to travel on average 7 days per month with train. Our concept “train traveling” includes underground, commuter trains, trams, local trains, and long-distance trains.
- (b)
- Car use. For the group of respondents as a whole, the car was the most frequently used travel mode: 93% traveled by car at least occasionally and 36% used it 4–7 days per week. A majority of the respondents had both driver’s license and a car in the household (see Table 1). Of those who responded to both these questions (driver’s license and car ownership), 92% of the men and 71% of the women, owned a driver’s license, but 78% of the men and only 49% of the women had a car in the household. Thus, fewer women than men could independently use a car in the household. Although most respondents traveled by car as driver or passenger, at least occasionally, a majority of our respondents (77%) also used public transport often enough to have acquired a discount card.
- (c)
- Local bus and the underground. Apart from the car, local bus was the most frequently used modes of travel, followed by the underground.
- (d)
- Long-distance bus and aircraft. Long-distance bus was the least used modes of transport, indeed 76% of the respondents reported never using it. Most of the respondents (66%) also traveled by air, occasionally.
- (e)
- Long-distance train. More than half of our respondents, 61%, never traveled by long-distance train. Moreover, most of our respondents (all 65–85 years old) had not recently traveled by long-distance train. Therefore, the part of the questionnaire concerned with the long-distance train journeys during the last year only involved 145 persons (or 25% of all respondents). Our respondents with no car in the household or with high income were more likely to have traveled by train during the last year than those with a car or with lower income (odds ratios were 3.5 and 2.1, respectively).
- (f)
- Traveling abroad. Most of the respondents traveled abroad, at least once in a while. Only 13% reported that they never traveled outside Sweden. But, during the last year, a majority of the respondents (86%) had not made a long-distance journey or journey abroad. Of those who had, more than half had traveled “by car” (60%), followed “by air” (48%) and/or “by train” (28%). The respondents were also asked what transport mode they would normally use for travels abroad or long-distance journeys; and “by air” was the most common answer (81%).
- (g)
- Buying tickets. Ticket purchases were most commonly made at a staffed point-of-sale (83%), followed by the Internet (59%) and by telephone service (42%). Ticket-machine (26%) and cell-phone (10%) purchases were least common. The percentage of missing answers was high for these questions, that is, up to 43%. Still, it is worth noticing that in our group of elderly, staffed point-of-sale was the most preferred.
4.5. Railway Accessibility
4.6. Interrelationships among Four Basic Research Constructs
4.6.1. Model A—Barriers Identified for Travelers’ Kinds of Functional Limitations/Diseases
4.6.2. Model A—Travel Behavior Identified for Travelers’ Kinds of Functional Limitations/Diseases
4.6.3. Model A—Railway Accessibility for Travelers’ Kinds of Functional Limitations/Diseases
| Functional Limitation/Disease | ρ | n |
|---|---|---|
| Travel sickness | −0.04 | 16 |
| Restricted mobility | 0.14 ** | 74 |
| Vision impairment | 0.04 | 115 |
| Hearing impairment | 0.05 | 113 |
| Reading, writing or speech disability | 0.07 | 11 |
| Attention, memory or concentration disability | 0.07 | 20 |
| Chronic pain | 0.12 ** | 51 |
| Asthma, allergy, hypersensitivity | 0.04 | 60 |
| Mental ill-health | 0.10 * | 17 |
| Cardiovascular disease | 0.04 | 90 |
| Chest disease | 0.07 | 23 |
| Epilepsy | 0.09 * | 5 |
| Neurological disorder | 0.04 | 12 |
| Rheumatic disorder | −0.01 | 24 |
| Diabetes | −0.02 | 57 |
4.6.4. Model B vs. Model A: Functional Ability for Person’s with Various Kinds of Functional Limitations/Diseases
| Number of Functional Limitations/Diseases Per Respondent 2 | Degree of Reduction in Functional Ability 3 | |||
|---|---|---|---|---|
| 0 | None (a) n (%) | Somewhat (b), (c) n (%) | Very (d), (e) n (%) | n |
| 0 | 149 (81) | 33 (18) | 2 (1) | 184 4 |
| 1 | 111 (62) | 64 (36) | 4 (2) | 179 |
| 2 | 38 (38) | 58 (58) | 4 (4) | 100 |
| 3 | 12 (24) | 31 (63) | 6 (12) | 49 |
| 4 | 2 (10) | 16 (80) | 2 (10) | 20 |
| 5 | 1 (7) | 10 (67) | 4 (27) | 15 |
| 6–8 | 0 (0) | 3 (60) | 5 (62) | 8 |
4.6.5. Model B—Identify Barriers for Travelers with Different Degrees of Functional Ability
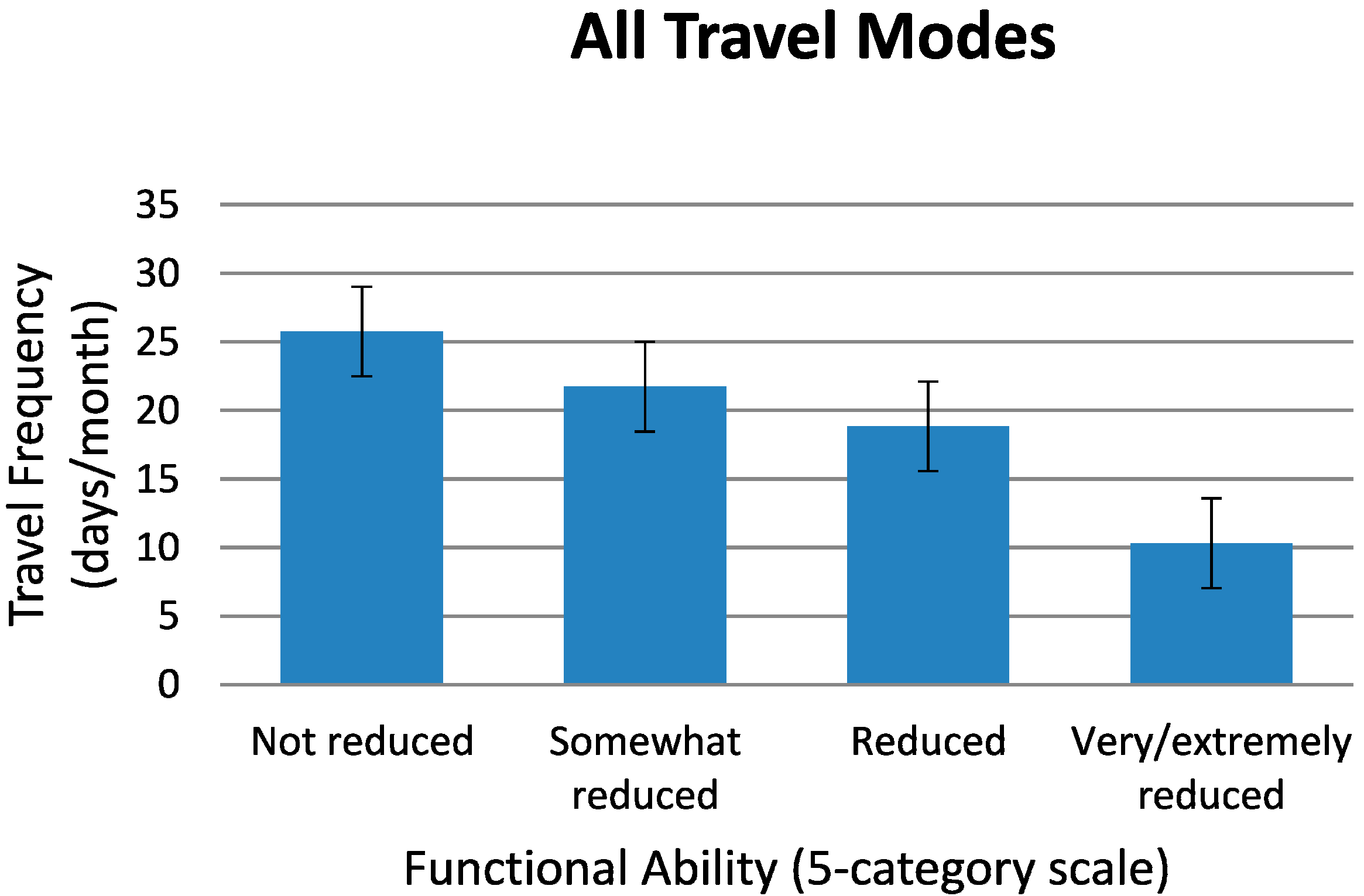
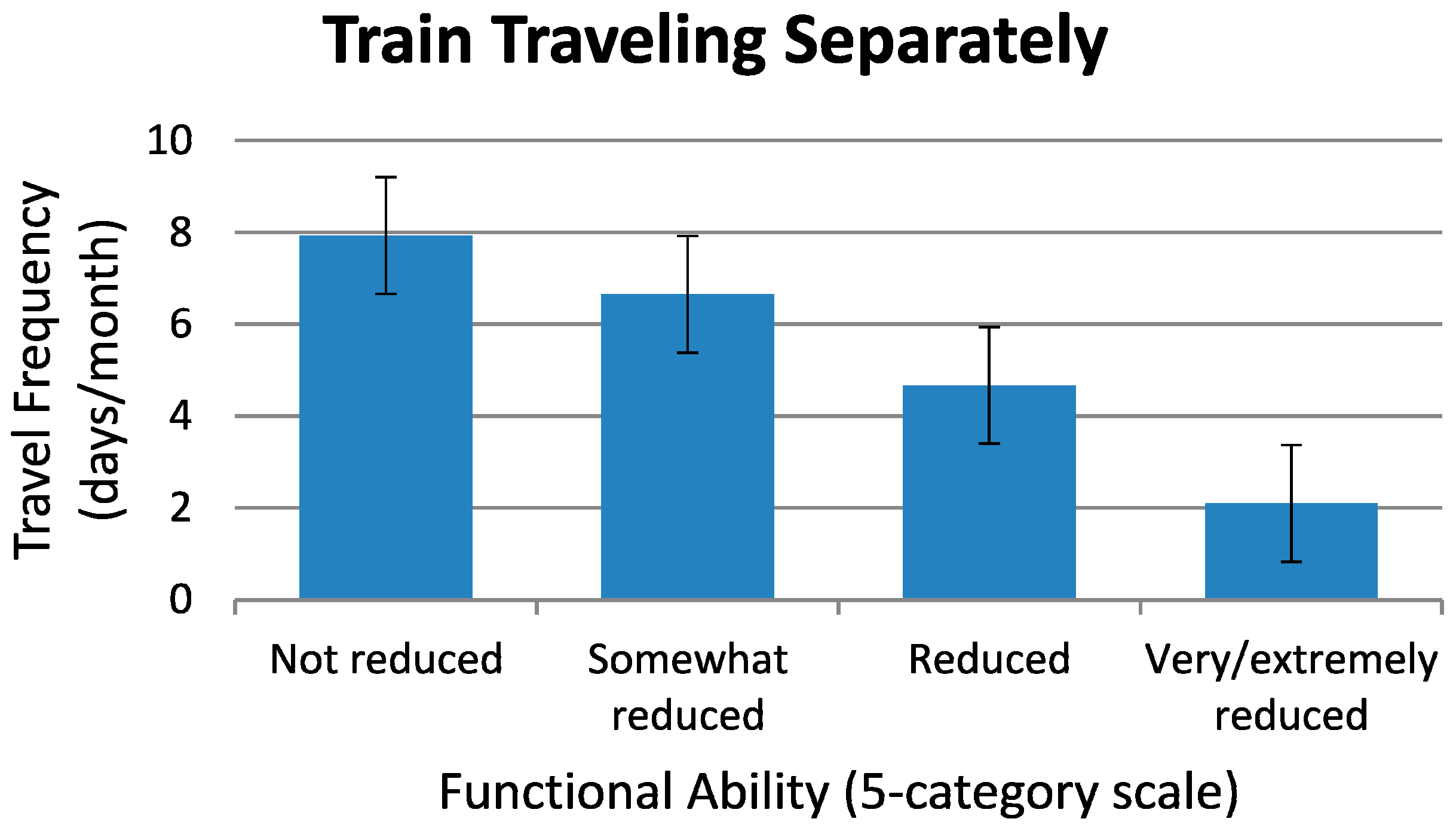
4.6.6. Model B—Travel Behavior as a Function of Travelers’ Degrees of Functional Ability

4.6.7. Model A and B—Interrelationship between Travel Behavior and Barriers
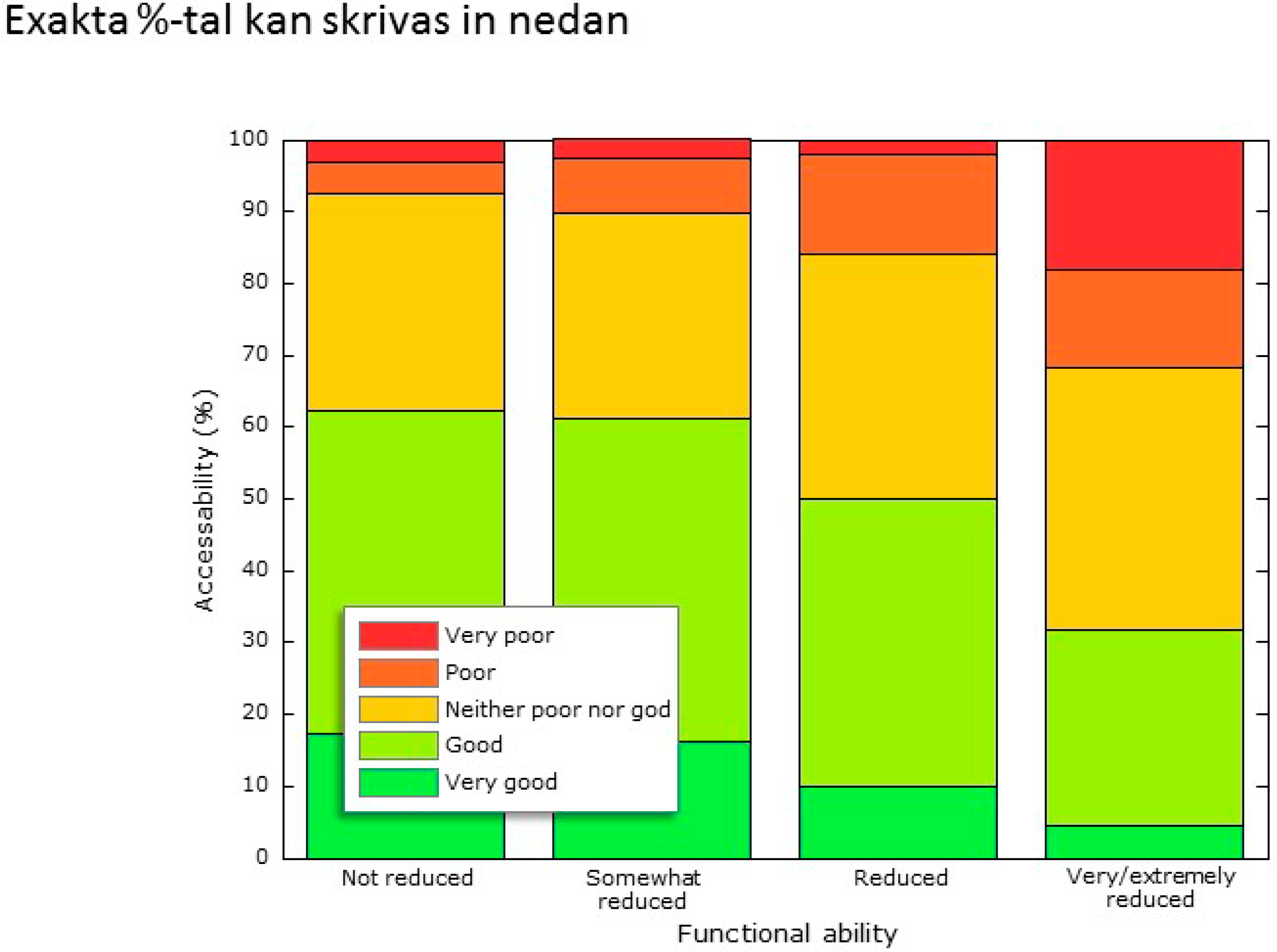
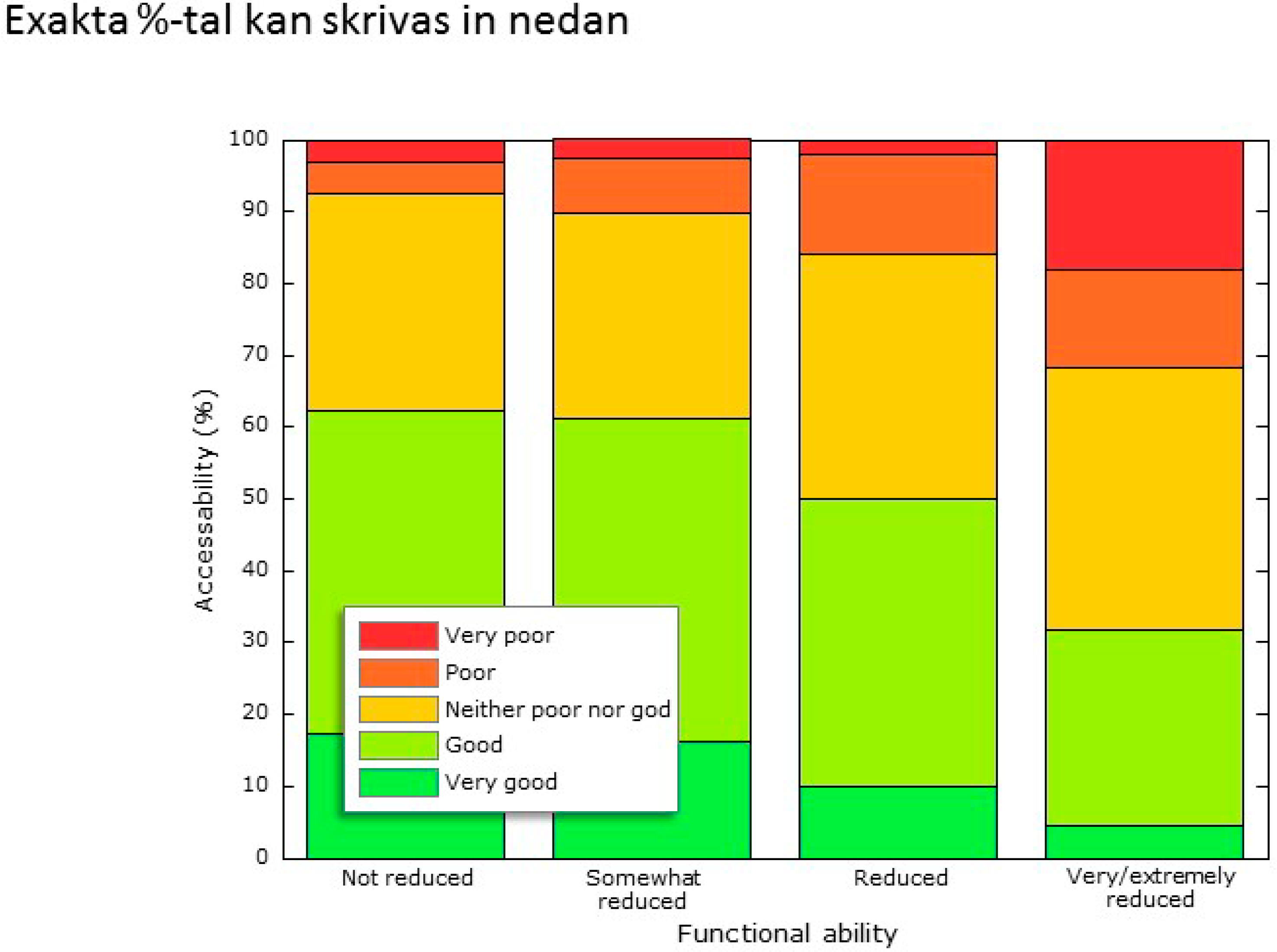
4.6.8. Model B—Railway Accessibility for Travelers with Different Degrees of Functional Ability
4.6.9. Model A & Model B—Railway Accessibility and Its Relationship to Barriers
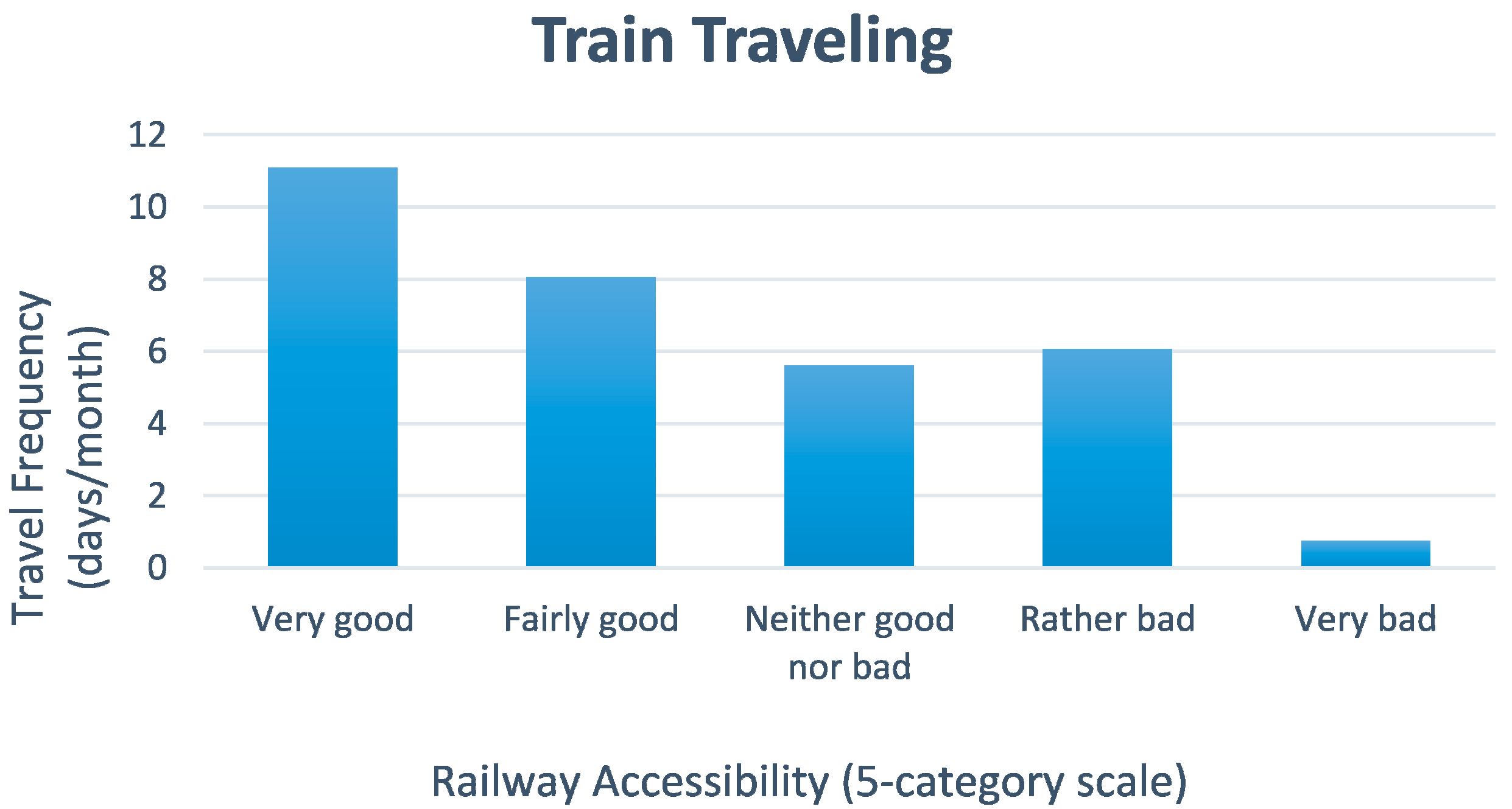
4.6.10. Model A & Model B—Railway Accessibility and Its Relationship to Travel Behavior
4.6.11. Model A & Model B—Railway Accessibility and Its Relationship to Travel Behavior and Barriers for Respondents with Different Kinds of Functional Limitations/Diseases and/or Degrees of Functional Ability
5. Discussion
6. Conclusions
6.1. Railway Accessibility
- Functional limitations/diseases. The elderly with the functional limitations/diseases of restricted mobility & chronic pain, perceived railway accessibility to be lower than those with other types of functional limitations/diseases. For each of five of the functional limitations/diseases (out of 15), neurological disease, chronic pain, restricted mobility, diabetes & vision impairment, perceived railway accessibility was correlated with the degree of functional ability.
- Functional ability. For all elderly participants taken together those who had a high functional ability (particularly participants with travel sickness, diabetes and asthma/allergy/hypersensitivity) also found the railway accessibility (n = 519), to be higher than those who had a low functional ability.
- Barriers. For the most recent long-distance train journey, railway accessibility was weakly correlated with all barriers that had been encountered during the whole trip, the weather inclusive. Those who perceived railway accessibility to be low, also to a greater extent reported that they would not travel by train more often, even if barriers were removed and the travel environment would be improved.
- Travel behavior. The elderly who perceived railway accessibility to be high, also reported that they traveled more often (travel behavior) than those who perceived it to be low. That is, the better the railway accessibility, the higher the travel frequency.
6.2. Overall Accessibility
6.3. Barriers to Be Remedied for a More Independent Travel Behavior
- Different kinds of barriers dominate among the travelers with different kinds of functional limitations/diseases. For example, persons with neurological and rheumatic diseases and those with restricted mobility, found it “difficult to move around onboard long-distance trains” or “move around within stations”. No other associations were established between specific barriers and the kinds of functional limitations/diseases of our elderly participants.
- “Lower ticket price” and “shorter travel time/better punctuality” would help to reduce/remove barriers that are central to the elderly travelers with high functional ability.
- Compared to our other respondents, the elderly with the most severely reduced functional ability more often attributed barriers to their “own health”.
- For elderly who are already frequent train travelers, “lower ticket prices” and “ease of buying tickets for the whole journey” were important barriers to more frequent train traveling.
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Statistics Sweden. The Future Population of Sweden 2012–2060: 10 Million already in the Year 2018. Available online: http://www.scb.se/statistik/_publikationer/LE0001_2012K03_TI_05_A05TI1203.pdf (accessed on 17 September 2014).
- The Swedish Ministry of Social Affairs. Empati och high tech. In Empathy and High Tech; The Swedish Ministry of Social Affairs: Västerås, Sweden, 2012. [Google Scholar]
- Spinney, J.E.L.; Scott, D.M.; Newbold, K.B. Transport mobility benefits and quality of life: A time-use perspective of elderly Canadians. Transp. Policy 2009, 16, 1–11. [Google Scholar] [CrossRef]
- Linder, P. Äldre människors res-och aktivitetsmönster—En litteraturstudie. In Older Persons’ Travel and Activity Patterns; Internal Report; Umeå University, Transportforskningsenheten: Umeå, Sweden, 2007. [Google Scholar]
- Gabriel, Z.; Bowling, A. Quality of life from the perspectives of older people. Ageing Soc. 2004, 24, 675–691. [Google Scholar] [CrossRef]
- Farquhar, M. Elderly people’s definitions of quality of life. Soc. Sci. Med. 1995, 41, 1439–1446. [Google Scholar] [CrossRef] [PubMed]
- Su, F.; Bell, M.G.H. Transport for older people: Characteristics and solutions. Res. Trans. E 2009, 25, 46–55. [Google Scholar] [CrossRef]
- Schmöcker, J.-D.; Quddus, M.A.; Noland, R.B.; Bell, M.G.H. Mode choice of older and disabled people: A case study of shopping trips in London. J. Transp. Geogr. 2008, 16, 257–267. [Google Scholar] [CrossRef] [Green Version]
- Rosenkvist, J.; Risser, R.; Iwarsson, S.; Wendel, K.; Ståhl, A. The challenge of using public transport: Descriptions by people with cognitive functional limitations. J. Transp. Land Use 2009, 2, 65–80. [Google Scholar] [CrossRef]
- Su, F.; Schmöcker, J.-D.; Bell, M.G.H. Mode choice of older people before and after shopping. J. Transp. Land Use 2009, 2, 29–46. [Google Scholar] [CrossRef]
- Maynard, A. Can measuring the benefits of accessible transport enable a seamless journey? J. Transp. Land Use 2009, 2, 21–30. [Google Scholar]
- Gould, P.R. Spatial Diffusion; Association of American Geographers, Commission on College Geographers: Washington, DC, USA, 1969. [Google Scholar]
- Envall, P. Accessibility Planning: A Chimera? Ph.D. Thesis, University of Leeds, Leeds, UK, 2007. [Google Scholar]
- Redman, L.; Friman, M.; Gärling, T.; Hartig, T. Quality attributes of public transport that attract car users: A research review. Transp. Policy 2013, 25, 119–127. [Google Scholar] [CrossRef]
- Rietveld, P. Six reasons why supply oriented indicators systematically overestimate service quality in public transport. Transp. Rev. 2005, 25, 309–328. [Google Scholar] [CrossRef]
- Olsson, L.E.; Friman, M.; Pareigis, J.; Edvardsson, B. Measuring service experience: Applying the satisfaction with travel scale in public transport. J. Retail. Consum. Serv. 2012, 19, 413–418. [Google Scholar] [CrossRef]
- Jensen, G.; Iwarsson, S.; Ståhl, A. Theoretical understanding and methodological challenges in accessibility assessments, focusing the environmental component: an example from travel chains in urban public bus transport. Disabil. Rehabil. 2002, 24, 231–242. [Google Scholar] [PubMed]
- Canter, D.V. The Psychology of Place; Architectural Press: London, UK, 1977. [Google Scholar]
- World Health Organization (WHO). Health Topics. Disabilities. Available online: http://www.who.int/topics/disabilities/en/ (accessed on 17 September 2014).
- Magnusson, D. A theoretical framework: The interactional perspective. In Individual Development from an Interactional Perspective: A Longitudinal Study, Volume 1: Paths Through Life; Lawrence Erlbaum: Hillsdale, NJ, USA, 1988; Volume 1, pp. 15–43. [Google Scholar]
- SIKA Institute. RES 2005–2006 den nationella resvaneundersökningen. In The National Travel Habit Survey; SIKA Institute: Östersund, Sweden, 2007. [Google Scholar]
- Alsnih, R.; Hensher, D.A. The mobility and accessibility expectations of seniors in an aging population. Transp. Res. A-Policy 2003, 37, 903–916. [Google Scholar] [CrossRef]
- Wasfi, R.; Levinson, D.; el-Geneidy, A. Measuring the transportation needs of seniors. JTL̶ J. Transp. Lit. 2012, 6, 8–32. [Google Scholar] [CrossRef]
- Sundling, C.; Berglund, B.; Nilsson, M.E.; Emardson, R.; Pendrill, L. New perspective on the accessibility of railway transport for the vulnerable traveller. J. Phys. Conf. 2013, 459. [Google Scholar] [CrossRef]
- Iwarsson, S.; Jensen, G.; Ståhl, A. Travel chain enabler: Development of a pilot instrument for assessment of urban public bus transport accessibility. Technol. Disabil. 2000, 12, 3–12. [Google Scholar]
- Emardson, R.; Jarlemark, P.; Pendrill, L.; Sundling, C.; Nilsson, M.E.; Berglund, B. Measurements of accessibility to rail transport systems. In Advanced Mathematical and Computational Tools in Metrology and Testing IX; Pavese, F., Bär, M., Filtz, J.R., Forbes, A.B., Pendrill, L., Shirono, K., Eds.; World Scientific: Toh Tuck Link, Singapore, 2012; Volume IX, pp. 136–142. [Google Scholar]
- IBM. IBM SPSS Statistics for Windows, Version 20.0; IBM: New York, NY, USA, 2011.
- SCB/Statistics Sweden. Sveriges framtida befolkning 2012-2060. (Population Statistics.) Stockholm, Sweden: Demografiska rapporter: 2012:2. Statistics Sweden. Available online: www.scb.se/statistik/_.../BE0401_2012I60_BR_BE51BR1202.pdf (accessed on December 10, 2014).
- Statistics Sweden. Census Data on Household and Housing. Available online: http://www.scb.se/sv_/Hitta-statistik/Artiklar/Var-tredje-aldre-bor-ensam/ (accessed on 17 September 2014).
- Börjesson, M. Funktionshindrades Resmöjligheter: Sammanfattning av Senaste Årens Forskning (Travel Possibilities of Persons with Functional Limitations: Research Summary); Rapport VR 2002:2; VINNOVA: Stockholm, Sweden, 2002. [Google Scholar]
- Lennartsson, C.; Lundberg, O. What’s marital status got to do with it? Gender inequalities in economic resources, health and functional abilities among older adults. In Health Inequalities and Welfare Resources: Continuity and Change in Sweden; Fritzell, J., Lundberg, O., Eds.; Policy Press: Brighton, UK, 2007. [Google Scholar]
- Lennartsson, C.; Agahi, N.; Wånell, S.-E. Hälsa och levnadsvanor–bland äldre personer i Stockholms län. In Health and Living Habits–among Elder Persons in the County of Stockholm; Hälso- och sjukvårdsförvaltningen: Stockholm, Sweden, 2011. [Google Scholar]
- Statistics Sweden. Undersökningarna av Levnadsförhållanden (ULF/SILC). Available online: http://www.scb.se/Pages/ProductTables____12209.aspx (accessed on 17 September 2014).
- Trafikanalys. Färdtjänst och riksfärdtjänst 2011. Statistik 2012:17. In Special Transport Service and Inter-Municipal Transport Service 2011; Statistics 2012:17; Statistics Sweden: Stockholm, Sweden, 2012. [Google Scholar]
- Davidsson, G. Funktionshindrades resvanor. In Travel Behavior of Persons with Functional Limitations; Statistics Sweden: Stockholm, Sweden, 2001. [Google Scholar]
Appendix
| Question: | Response |
|---|---|
| I Would Travel More Often by Train, If… | Frequency * |
| If it would be less expensive to travel | 62% |
| If departure and arrival times were kept | 49% |
| If I knew I would be in time at the final destination | 48% |
| If I knew I would be in time for my connection | 47% |
| If I would not have to change modes of travel during the trip | 43% |
| If I knew I would get help if I need | 42% |
| If it would not be crowded onboard | 40% |
| If I knew I would be in time for the long-distance train | 33% |
| If the travel time would become shorter | 33% |
| If it would be easier to find an empty seat | 33% |
| If it would be easier to book/purchase tickets for the whole trip at the same time (even connections) | 33% |
| If there were service staff at the platform | 29% |
| If I would feel secure going to and from the station | 26% |
| If the attitude of the staff would be more service minded | 26% |
| If I would not be afraid of being harassed | 25% |
| If I could be sure I would manage the whole journey | 25% |
| If it would become easier to get help from staff onboard | 25% |
| If it would become easier to book/purchase tickets | 24% |
| If the environment would become less busy | 24% |
| If I would have more time to get on or off the train | 24% |
| If the departures were more frequent | 22% |
| If it were easier to get help from staff within the station area | 22% |
| If I were healthier and therefore could manage to travel | 20% |
| If the staff would be more proficient | 20% |
| If it would be easier to park at the station | 19% |
| If I would not have to keep track of so many things during the trip | 18% |
| If trains and stations were designed in a more homogenous way | 15% |
| If it would be possible to travel at other hours (for example at night) | 11% |
| If fellow passengers’ attitudes were better | 11% |
| If I would not have to travel under the ground | 9% |
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sundling, C.; Berglund, B.; Nilsson, M.E.; Emardson, R.; Pendrill, L.R. Overall Accessibility to Traveling by Rail for the Elderly with and without Functional Limitations: The Whole-Trip Perspective. Int. J. Environ. Res. Public Health 2014, 11, 12938-12968. https://doi.org/10.3390/ijerph111212938
Sundling C, Berglund B, Nilsson ME, Emardson R, Pendrill LR. Overall Accessibility to Traveling by Rail for the Elderly with and without Functional Limitations: The Whole-Trip Perspective. International Journal of Environmental Research and Public Health. 2014; 11(12):12938-12968. https://doi.org/10.3390/ijerph111212938
Chicago/Turabian StyleSundling, Catherine, Birgitta Berglund, Mats E. Nilsson, Ragne Emardson, and Leslie R. Pendrill. 2014. "Overall Accessibility to Traveling by Rail for the Elderly with and without Functional Limitations: The Whole-Trip Perspective" International Journal of Environmental Research and Public Health 11, no. 12: 12938-12968. https://doi.org/10.3390/ijerph111212938