Challenges to Achieving Sustainable Sanitation in Informal Settlements of Kigali, Rwanda

Abstract
:1. Introduction
2. Methods
3. Results
3.1. Socio-Economic Characteristics of Survey Respondents
3.2. Existing Sanitation Systems in Study Areas of Kigali

{kind=link}
{kind=link}
| Section (a): Type of Sanitation Systems | Section (b): Sanitation Systems | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Shared | Not Shared | Grand Total | |||||||
| N | % | N | % | N | % | N | % | ||
| Improved | Flush | 48 | 2.7 | 19 | 1 | 29 | 1.6 | 48 | 2.6 |
| Pit latrine with slab | 946 | 52.7 | 650 | 36.3 | 296 | 16.50 | 946 | 52.9 | |
| Other improved categories | 15 | 0.9 | 11 | 0.6 | 4 | 0.3 | 15 | 0.9 | |
| Improved Sub-Total | 1,009 | 56.3 ** | 680 | 37.9 | 329 | 18.4 * | 1,009 | 56.3 | |
| Unimproved | Open pit latrine without slab | 690 | 38.5 | 558 | 31.2 | 132 | 7.4 | 690 | 38.6 |
| Other unimproved categories | 90 | 5.0 | 74 | 4.1 | 16 | 0.9 | 90 | 5.0 | |
| Open defecation | 5 | 0.3 | - | - | - | - | 5 | 0.3 | |
| Unimproved Sub-Total | 785 | 43.7 | 632 | 35.3 | 148 | 8.3 | 785 | 43.6 | |
| Grand Total of both Improved and Unimproved | 1,794 | 100 | 1,312 | 73.2 | 477 | 26.7 | 1,794 | 100 | |
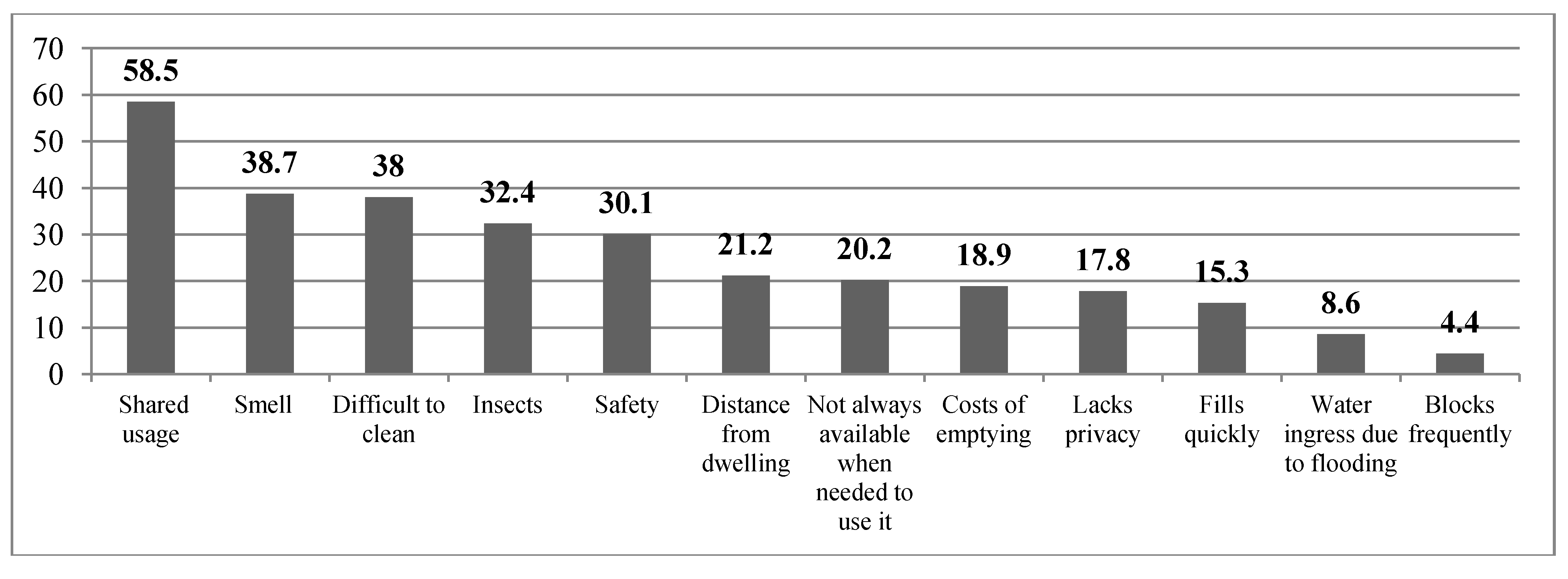
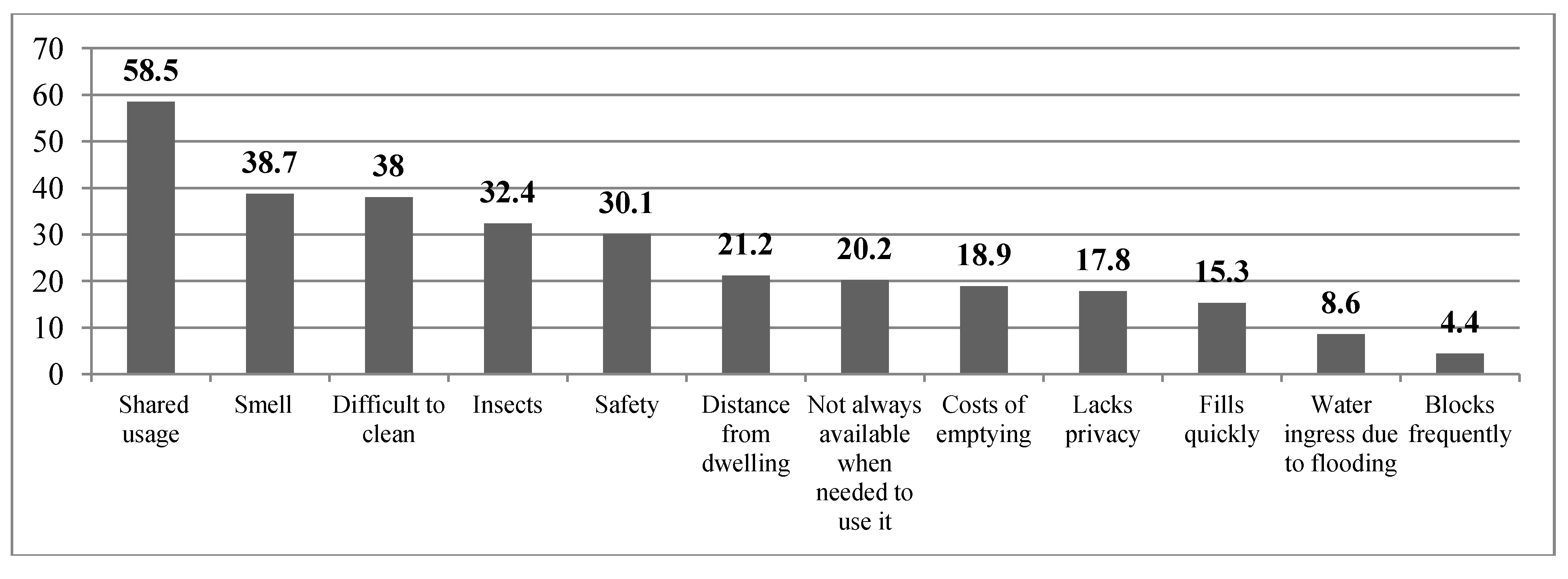
3.3. Issues Associated with Existing Sanitation Facilities in Informal Settlements of Kigali
“The ways of transmission are various. The lack of fresh water and soap in the house can hinder people from hand washing and uncovered pits or stagnant black water can attract flies. Effluent from tanks and pits can pollute surface and ground water used for human consumption with pathogens and pollutants.”
“Sometimes when I stay too long in the squatting position, to be able to stand up, I find support by touching the ground, where I can easily contaminate with diseases. It is a very embarrassing and stressful experience for us old people” (Woman with disability).
“When you are passing by, the bad smell from the toilets hit your face and you do your best to leave the place as quick as possible” (One male tenant).
“When constructing the toilets and paths to the toilet, they do not give any considerations to the disabled; everything is constructed to suit the ordinary normal person”.
“The path to the latrine is not safe at night. I fear I will get injured by stones or sharp objects left on my way. Thus I am obliged to defecate beside the house like a kid and my wife has to wipe it off early in the morning”.
“I am frightened to use our toilets because I fear that the toilets will collapse at any time and I will fall downer the hole and die; so I prefer other alternatives such as using a bucket, or practicing open defecation” (Male tenant).
“My toilet is okay, the only problem is that it is not properly constructed and does not promote privacy. If I am inside, people outside can see me while using it”, complained one female tenant.
“People in settlements still practiced open defecation in open spaces between houses, in corners, on people’s fences and this is mostly done by kids, drunkards, homeless youth or outsiders; the reasons of such malpractice was said to be due to local bars not having a toilet as well as lack of public toilets in the settlement, unavailability of toilet due to a large number of people sharing a facility, poor hygienic conditions of the facility, people without facilities or simply because of poor attitude of some people” (Female owner occupier).
“Pit latrines fill up quickly here in informal settlements as a result of the large number of users. Due to the diminishing space available in informal settlements, households must resort to emptying their pit latrine and as constructing a new latrine is impractical, but the issue is the fact we do not even have emptiers around here...”
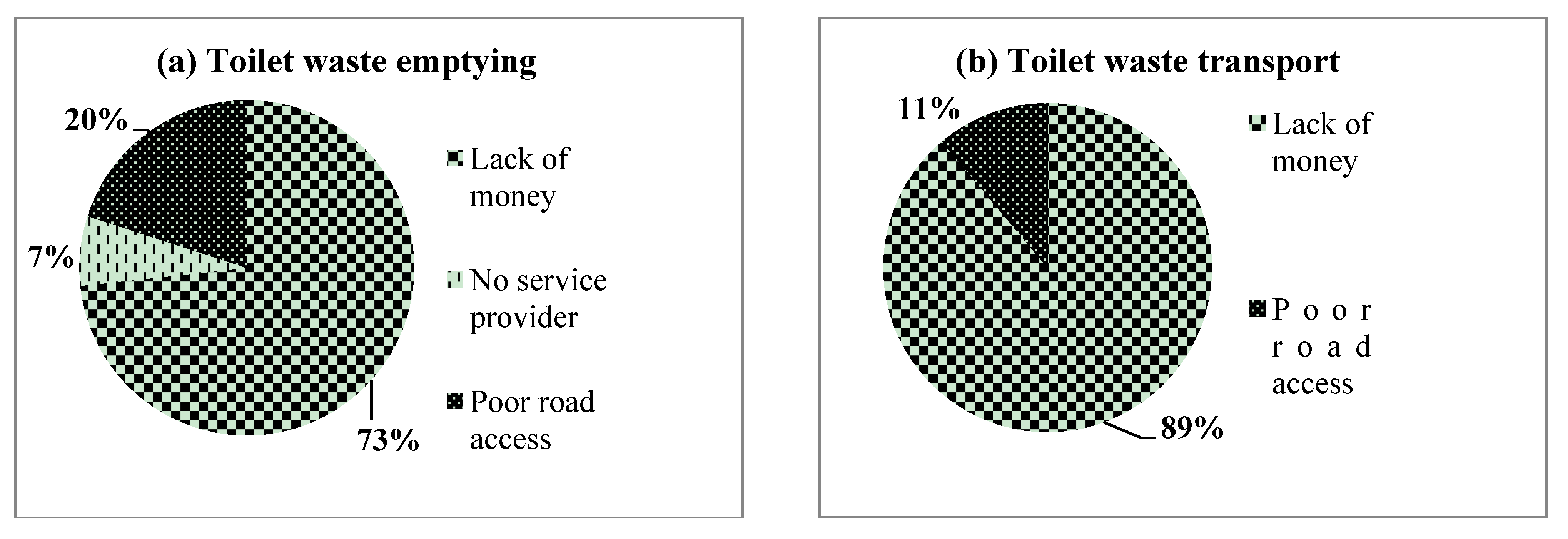
3.4. Constraints to Sustainable Sanitation in Informal Settlements of Kigali

“Landlords become resistant when asked for improved sanitation and are more concerned with making money. For instance, when tenants request for improved sanitation landlords respond harshly telling them to look for other houses where they will find what they want and if they are not satisfied with what is there, that there are many people who can be comfortable with what is present” (Female tenant).
“Sometimes, we think that landlords are rich and yet they are not, and when you analyse you find that they cannot afford to construct a good standard toilet, because the landlords have also many dependents and more pressing needs and priorities than having a proper toilet”.
“My toilet has no roof because I have no money; when I get money, another urgent problem occurs and then I prefer to solve that one first” (A female owner-occupier).
“The major challenge faced is the cost of constructing a toilet which is very expensive. Even if they pay us rent every month, it is too little to construct a toilet” (Male resident- landlord);
“Space is the biggest obstacle of all; it is impossible to construct more than three toilets on my land” (Female absentee-landlord).
“Although pit emptying services are too expensive (USD 150) and few can afford to pay this amount of money, they (emptying services) had been banned by the authorities because people had dumped the sewage into the drainage channels; yet those who afford to pay for emptying are limited by the roads which are too narrow in the settlement for pit emptying trucks to reach their toilets, so I think the facilities that are in close proximity to roads could be easily emptied” (A male owner-occupier).
“We really do not have sustainable mechanism to deal with sewage here because there is nowhere to dump the sewage; it is a big problem...”(KCC official).
“The facility that I think is suitable for older people is the flush toilet as it gives support but the challenge is there is no water access in the settlement and this would also increase water bills yet money is one of my biggest challenges in accessing a good toilet” (Old woman).
4. Discussion
4.1. Challenges to Achieving Sustainable Sanitation in Informal Settlements of Kigali
4.2. Sustainable Sanitation Technologies Appropriate to Informal Settlements of Kigali
5. Conclusions
Acknowledgments
Conflicts of Interest
References
- Sano, J.C. Urban Environmental Infrastructure in Kigali City, Rwanda: Challenges and Opportunities for Modernised Decentralised Sanitation Systems in Poor Neighbourhoods. M. Sc. Thesis, Wageningen University, Wageningen, The Netherlands, August 2007. [Google Scholar]
- Oosterveer, P.; Spaargaren, G. Meeting Social Challenges in Developing Sustainable Environmental Infrastructures in East African Cities. In Social Perspectives on the Sanitation Challenge; Springer: Berlin, Germany, 2010; pp. 11–30. [Google Scholar]
- Shah, N. Characterizing Slums and Slum-Dwellers: Exploring Household-level Indonesian Data. 2012. Available online: http://storage.globalcitizen.net/data/topic/knowledge/uploads/20120920133613196030_slums_Shah.pdf (accessed on 24 August 2013).
- Dinye, R.D.; Acheampong, E.O. Challenges of slum dwellers in Ghana: The case study of Ayigya, Kumasi. Mod. Soc. Sci. J. 2013, 2, 228–255. [Google Scholar]
- WHO/UNICEF. Progress on Sanitation and Drinking-Water: 2010 Update; WHO Joint Monitoring Programe: Paris, France, 2010. [Google Scholar]
- Schouten, M.; Mathenge, R. Communal sanitation alternatives for slums: A case study of Kibera, Kenya. Phys. Chem. Earth. 2010, 35, 815–822. [Google Scholar] [CrossRef]
- National Institute of Statistics for Rwanda. 2012 Population and Housing Census: Provisional Results. Republic of Rwanda National Institute of Statistics for Rwanda: Kigali, Rwanda, 2012. [Google Scholar]
- National Institute of Statistics of Rwanda. Rwanda Demographic and Health Survey 2010: Final Report; National Institute of Statistics for Rwanda Republic of Rwanda: Kigali, Rwanda, 2010. [Google Scholar]
- Hohne, A. State and Drivers of Change of Kigali’s Sanitation—A Demand Perspective. Proceedings of the East Africa Practitioners Workshop on Pro Poor Urban Sanitation and Hygiene, Kigali, Rwanda, 2011; Available online: http://www.google.ca/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&ved=0CC0QFjAA&url=http%3A%2F%2Fwww.irc.nl%2Fcontent%2Fdownload%2F162378%2F590890%2Ffile%2F&ei=YjWgUotLYjs0gXQ9oG4Aw&usg=AFQjCNFHdLyZFqAHU0kaWajsyyA5A3oaAA&bvm=bv.57155469,d.d2k (accessed on 20August 2013).
- Parkinson, J. Improving servicing of on-site sanitation-a neglected issue for the UN Year of Sanitation. Water 2008, 21, 40–42. [Google Scholar]
- Lubaale, G.N.; Musyoki, S.M. Pro-poor Sanitation and Hygiene in East Africa: Turning Challenges to Opportunities. Proceedings of the East Africa Practitioners Workshop on Pro Poor Urban Sanitation and Hygiene, Kigali, Rwanda, 2011; Available online: http://www.irc.nl/page/64589 (accessed on 12 September 2011).
- Scheinberg, A.; Spies, S.; Simpson, M.H.; Mol, A.P.J. Assessing urban recycling in low-and middle-income countries: Building on modernised mixtures. Habitat Int. 2011, 35, 188–198. [Google Scholar] [CrossRef]
- Satterthwaite, D. The Under-Estimation of Urban Poverty in Low and Middle-Income Nations; IIED: London, UK, 2004. [Google Scholar]
- Tilley, E.; Morel, A.; Zurbru, C.; Schertenleib, R. Compendium of Sanitation Systems and Technologies; Swiss Federal Institute of Aquatic Science and Technology (Eawag): Geneva, Switzerland, 2008. [Google Scholar]
- Tsinda, A.; Abbott, P. A Review and Analysis of the Situation Pertaining to the Provision of Sanitation to Low-Income Settlements in Kigali City (Rwanda); Diagnostic Report, Institute of Policy Analysis and Research; IPAR-Rwanda: Kigali, Rwanda, 2012. [Google Scholar]
- Chevalier, J.M.; Buckles, D.J. Participatory Action Research. Theory and Methods for Engaged Inquiry; Routledge: London, UK, 2013. [Google Scholar]
- Lüthi, C.; Panesar, A.; Schütze, T. Sustainable Sanitation in Cities: A Framework for Action, Sustainable Sanitation Alliance (SuSanA) & International Forum on Urbanism (IFoU); Papiroz Publishing House: Rijswijk, The Netherlands, 2011. [Google Scholar]
- Grimason, A.M.; Davison, K.; Tembo, K.C.; Jabu, G.C.; Jackson, M.H. Problems associated with the use of pit latrines in Blantyre, Republic of Malawi. J. R. Soc. Promote. Health 2000, 120, 175–182. [Google Scholar] [CrossRef]
- Mtungila, J.; Chipofya, V. Issues and challenges of providing adequate sanitation to people living on the shore of lake Malawi: Case of Monkey Bay, Malawi. Desalination 2009, 248, 338–343. [Google Scholar] [CrossRef]
- Moe, C.L.; Rheingans, R.D. Global challenges in water, sanitation and health. J. Water Health 2006, 4, 41–57. [Google Scholar]
- Saywell, D.; Shaw, R. On-plot Sanitation in Urban Areas; Water and Environmental Health at London and Loughborough (WELL): London, UK, 2005. [Google Scholar]
- Bolaane, B.; Ikgopoleng, H. Towards improved sanitation: Constraints and opportunities in accessing waterborne sewerage in major villages of Botswana. Habitat Int. 2011, 35, 486–493. [Google Scholar] [CrossRef]
- Cross, P.; Morel, A. Pro-poor strategies for urban water supply and sanitation services delivery in Africa. Water Sci. Technol.: J. Int. Assoc. Water Pollut. Res. 2005, 51, 51–57. [Google Scholar]
- UN-HABITAT. UN-Habitat Annual Report 2009; United Nations Human Settlements Programme: Nairobi, Kenya, 2010. [Google Scholar]
- Adubofour, K.; Obiri-Danso, K.; Quansah, C. Sanitation survey of two urban slum Muslim communities in the Kumasi metropolis, Ghana. Environ. Urban. 2013, 25, 189–207. [Google Scholar] [CrossRef]
- Prüss, A.; Mariotti, S.P. Preventing trachoma through environmental sanitation: A review of the evidence base. Bull. World Health Organ. 2000, 78, 267–273. [Google Scholar]
- Graczyk, T.K.; Knight, R.; Tamang, L. Mechanical transmission of human protozoan parasites by insects. Clin. Microbiol. Rev. 2005, 18, 128–132. [Google Scholar] [CrossRef]
- Thye, Y.P.; Templeton, M.R.; Ali, M. A critical review of technologies for pit latrine emptying in developing countries. Crit. Rev. Environ. Sci. Technol. 2011, 41, 1793–1819. [Google Scholar] [CrossRef]
- Tremolet, S.; Kolsky, P.; Perez, E. Financing On-Site Sanitation for the Poor: A Six Country Comparative Review and Analysis. Water and sanitation Programme. 2010. Available online: http://www.wsp.org/sites/wsp.org/files/publications/financing_analysis.pdf (accessed on 23 June 2012).
- Chinyama, A.; Chipato, P.; Mangore, E. Sustainable sanitation systems for low income urban areas-A case of the city of Bulawayo, Zimbabwe. Phys. Chem. Earth. 2012, 50, 233–238. [Google Scholar] [CrossRef]
- Kulabako, R.N.; Nalubega, M.; Wozei, E.; Thunvik, R. Environmental health practices, constraints and possible interventions in peri-urban settlements in developing countries—A review of Kampala, Uganda. Int. J. Environ. Health Res. 2010, 20, 231–257. [Google Scholar] [CrossRef]
- Isunju, J.B.; Schwartz, K.; Schouten, M.A.; Johnson, W.P.; van Dijk, M.P. Socio-economic aspects of improved sanitation in slums: A review. Public Health 2011, 125, 368–376. [Google Scholar] [CrossRef]
- Mara, D.; Alabaster, G. A new paradigm for low-cost urban water supplies and sanitation in developing countries. Water Policy 2008, 10, 119–129. [Google Scholar] [CrossRef]
- Thye, Y.P.; Templeton, M.R.; Ali, M. Pit Latrine Emptying: Technologies, Challenges and Solutions. London, UK, 2009. Available online: http://www.ewb-uk.org/system/files/Yoke+Thye+report.pdf (accessed on 23 August 2013).
- Jha, P. Health and social benefits from improving community hygiene and sanitation: An Indian experience. Int. J. Environ. Health Res. 2003, 13, S133–S140. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Tsinda, A.; Abbott, P.; Pedley, S.; Charles, K.; Adogo, J.; Okurut, K.; Chenoweth, J. Challenges to Achieving Sustainable Sanitation in Informal Settlements of Kigali, Rwanda. Int. J. Environ. Res. Public Health 2013, 10, 6939-6954. https://doi.org/10.3390/ijerph10126939
Tsinda A, Abbott P, Pedley S, Charles K, Adogo J, Okurut K, Chenoweth J. Challenges to Achieving Sustainable Sanitation in Informal Settlements of Kigali, Rwanda. International Journal of Environmental Research and Public Health. 2013; 10(12):6939-6954. https://doi.org/10.3390/ijerph10126939
Chicago/Turabian StyleTsinda, Aime, Pamela Abbott, Steve Pedley, Katrina Charles, Jane Adogo, Kenan Okurut, and Jonathan Chenoweth. 2013. "Challenges to Achieving Sustainable Sanitation in Informal Settlements of Kigali, Rwanda" International Journal of Environmental Research and Public Health 10, no. 12: 6939-6954. https://doi.org/10.3390/ijerph10126939