Mobile, Cloud, and Big Data Computing: Contributions, Challenges, and New Directions in Telecardiology

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. The Development of Telecardiology
- How to improve the current ECG and ECHO instrumentation and the software so that any experienced cardiologist can remotely access to the files and offer timely assessment and treatment recommendation when he or she is away from the patient?
- How to make telecardiology services interoperable across hospitals?
2. ECG Telemedicine
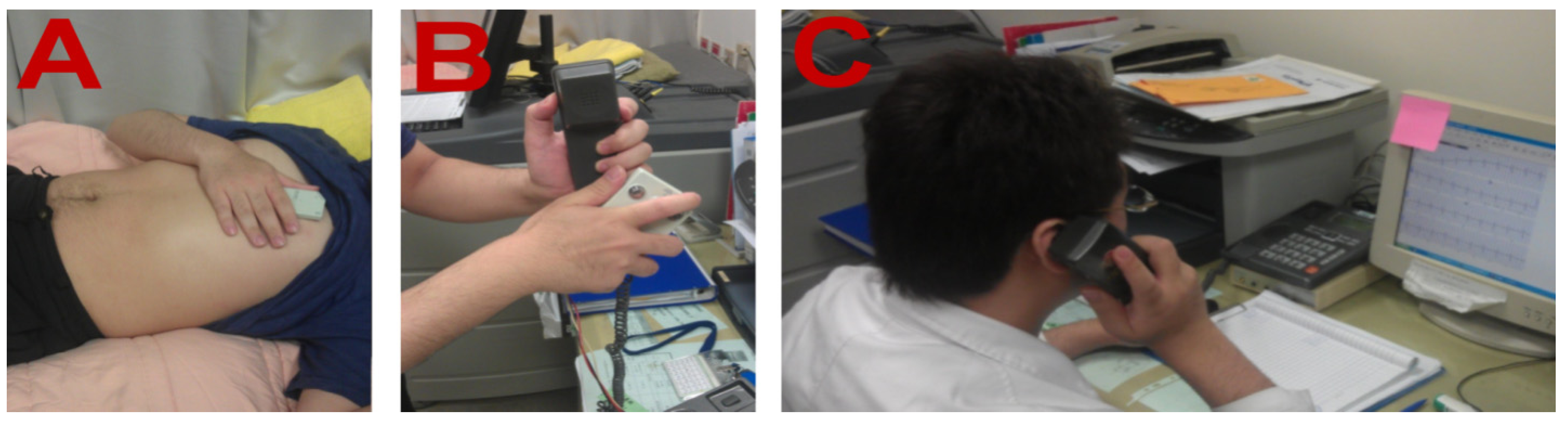
2.1. The Development of ECG Tele-Monitoring

2.2. Clinical Evaluations of 12-Lead ECG Home Monitoring
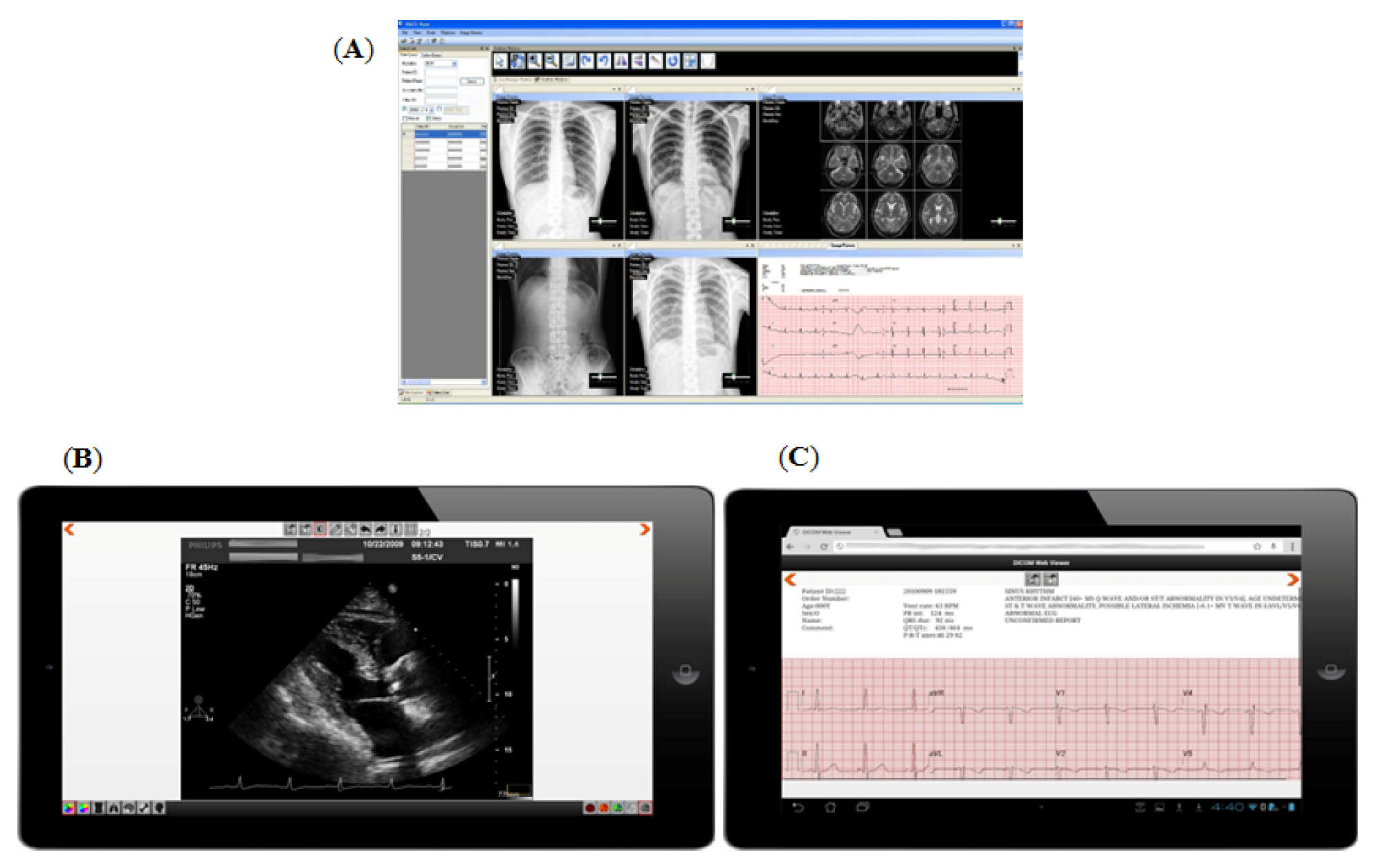
2.3. In-Hospital 12-Lead ECG and Imaging Teleconsultation

2.4. The Teleconsultation of Intensive Care Unit (ICU) and Coronary Care Unit (CCU)
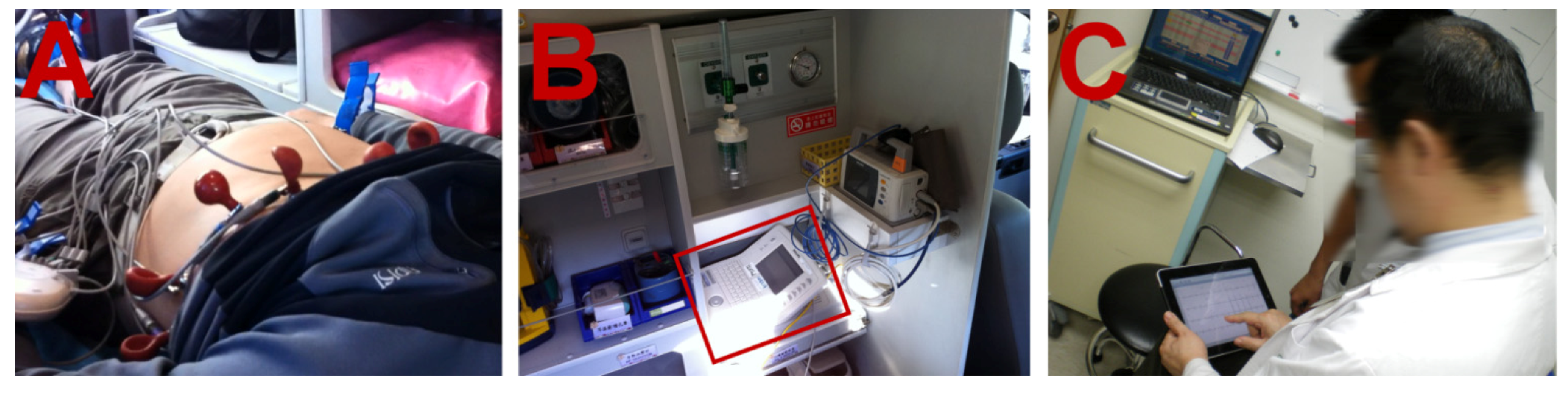
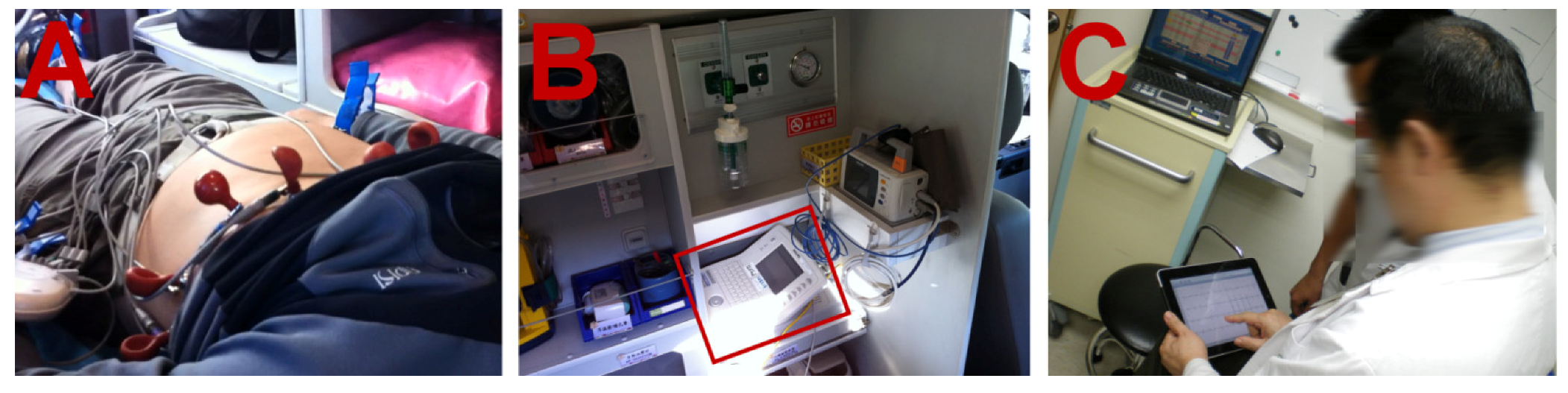
2.5. Pre-Hospital 12-Lead ECG Diagnosis
3. The Development of Tele-ECHO
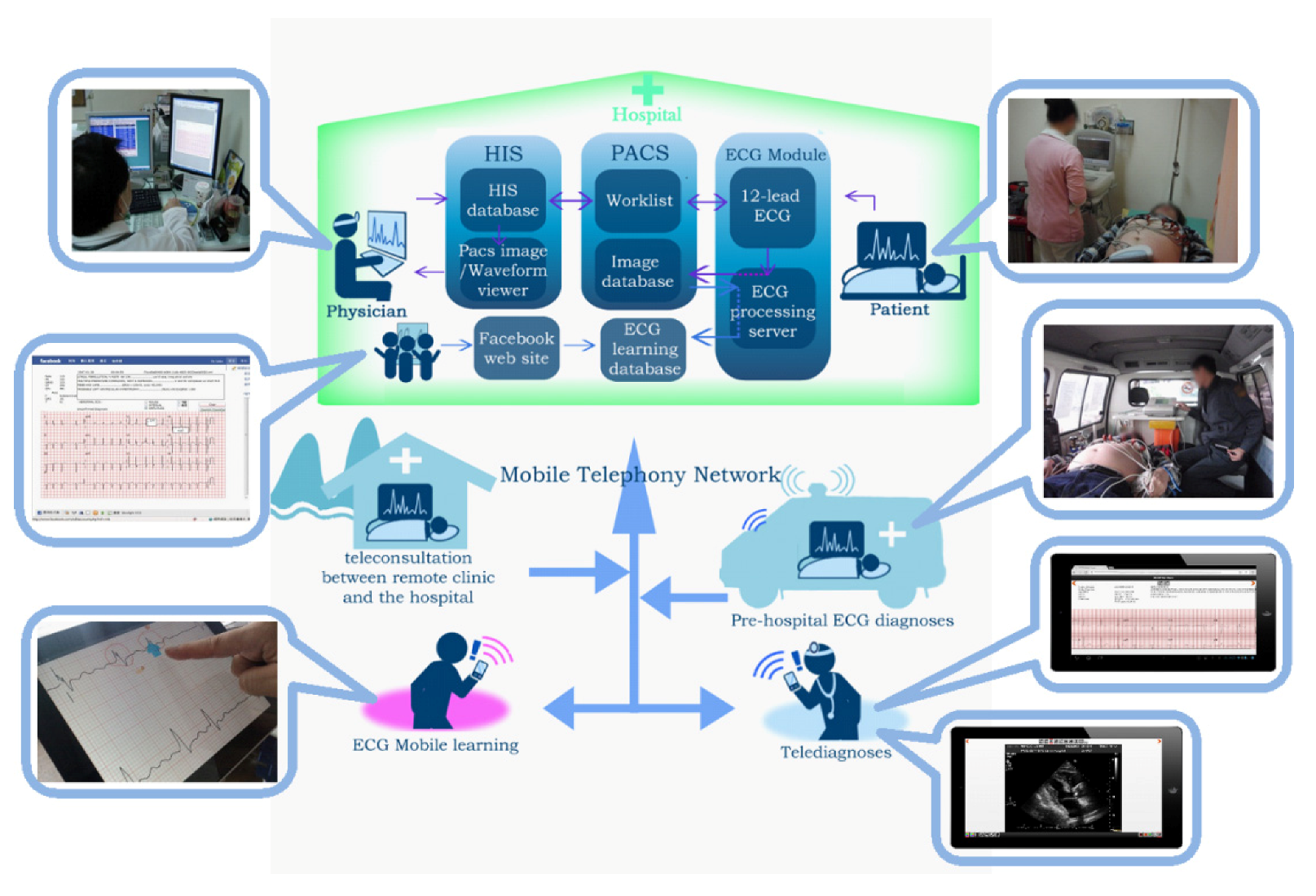
4. New Framework of Telecardiology

4.1. Cloud Computing Can Benefit Telecardiology and Large-Scale Medical Data Analysis
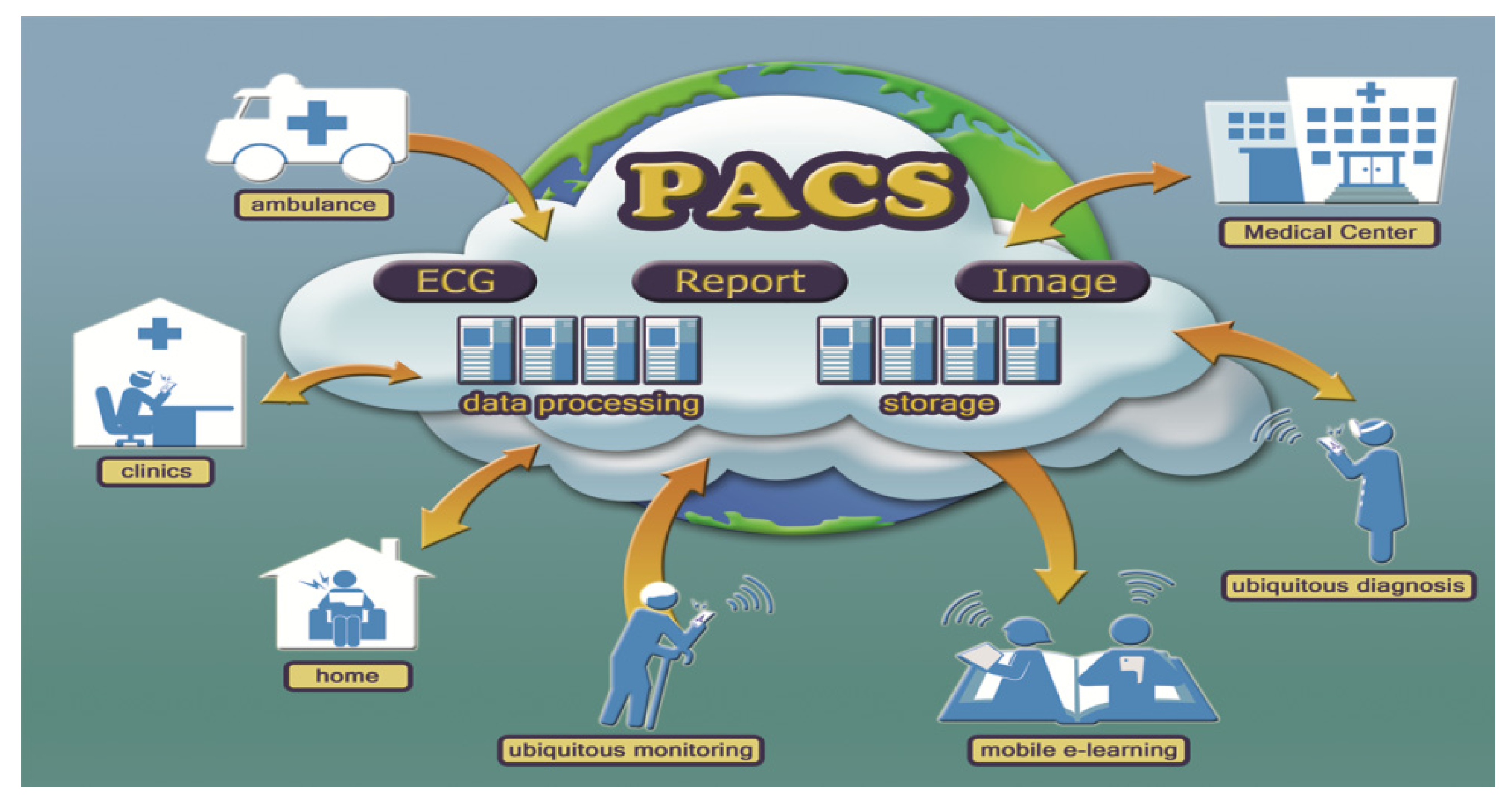
4.2. A Cloud-PACS Extended from Local to Global

5. The Feasibility of the Cloud Telecardiology Service
5.1. The Security of Data Transmission via Public Network
5.2. Privacy Protection in the Cloud
5.3. Data Confidentiality in the Cloud
5.4. Cloudlet Can Improve Network Latency
5.5. Next Generation Network/IP Multimedia Subsystem (NGN/IMS) Can Enhance Network Reliability and Accessibility
5.6. The Image Compression Technology Can Speed up Image Transmission
5.7. Cyber Foraging Can Improve Computing Efficiency of Mobile Devices
5.8. DICOM and Cloud-PACS Can Facilitate the Interoperability of ECG and Medical Images
5.9. Diagnostic ECG and Image Reports Can Facilitate the Development of ECG and Image Research and Education
6. Conclusions
Acknowledgments
Conflicts of Interest
References
- Sable, C. Telecardiology: Potential impact on acute care. Crit. Care Med. 2001, 29. [Google Scholar] [CrossRef]
- Nikus, K.; Virtanen, V.; Sclarovsky, S.; Eskola, M. The Role of Standard 12-lead ECG in a Telecardiology Consultation Service. In Telemedicine Techniques and Applications; Graschew, G., Rakowsky, S., Eds.; InTech: Rijeka, Croatia, 2011. [Google Scholar] [CrossRef]
- Evangelista, A.; Flachskampf, F.; Lancellotti, P.; Badano, L.; Aguilar, R.; Monaghan, M.; Zamorano, J.; Nihoyannopoulos, P. European Association of Echocardiography recommendations for standardization of performance, digital storage and reporting of echocardiographic studies. Eur. J. Echocardiogr. 2008, 9, 438–448. [Google Scholar] [CrossRef]
- Birati, E.; Roth, A. Telecardiology. Israel Med. Assoc. J. 2011, 13, 498–503. [Google Scholar]
- Sørensen, J.T.; Clemmensen, P.; Sejersten, M. Telecardiology: Past, present and future. Revista Española de Cardiología (English Edition) 2013, 66, 212–218. [Google Scholar]
- Backman, W.; Bendel, D.; Rakhit, R. The telecardiology revolution: Improving the management of cardiac disease in primary care. JRSM 2010, 103, 442–446. [Google Scholar] [CrossRef]
- Atar, S. Telecardiology—Close to the heart, but still out of reach. Israel Med. Assoc. J. 2011, 13, 496–497. [Google Scholar]
- Hsieh, J. C.; Hsu, M.W. A cloud computing based 12-lead ECG telemedicine service. BMC Med. Inform. Decis. Making 2012, 12. [Google Scholar] [CrossRef]
- Orlov, O.I.; Drozdov, D.V.; Doarn, C.R.; Merrell, R.C. Wireless ECG monitoring by telephone. Telemed. J. e-Health 2001, 7, 33–38. [Google Scholar] [CrossRef]
- Giannakakis, G.; Buliev, I. ECG signal recording, processing and transmission using a mobile phone. In Proceedings of the 1st International Conference on PErvasive Technologies Related to Assistive Environments, Athens, Greece, 15–19 July 2008; ACM Digital Library: New York, NY, USA, 2008. [Google Scholar] [CrossRef]
- Lee, H.J.; Lee, S.H.; Ha, K.-S.; Jang, H.C.; Chung, W.-Y.; Kim, J.Y.; Chang, Y.-S.; Yoo, D.H. Ubiquitous healthcare service using Zigbee and mobile phone for elderly patients. Int. J. Med. Inform. 2009, 78, 193–198. [Google Scholar] [CrossRef]
- Yousef, J.; Lars, A. Validation of a real-time wireless telemedicine system, using bluetooth protocol and a mobile phone, for remote monitoring patient in medical practice. Eur. J. Med. Res. 2005, 10, 254–262. [Google Scholar]
- Chu, Y.; Ganz, A. A mobile teletrauma system using 3G networks. Inform. Technol. Biomed Technol 2004, 8, 456–462. [Google Scholar] [CrossRef]
- Brunetti, N.D.; Amodio, G.; de Gennaro, L.; Dellegrottaglie, G.; Pellegrino, P.L.; di Biase, M.; Antonelli, G. Telecardiology applied to a region-wide public emergency health-care service. J. Thromb. Thrombolysis 2009, 28, 23–30. [Google Scholar] [CrossRef]
- Scalvini, S.; Piepoli, M.; Zanelli, E.; Volterrani, M.; Giordano, A.; Glisenti, F. Incidence of atrial fibrillation in an Italian population followed by their GPs through a telecardiology service. Int. J. Cardiol. 2005, 98, 215–220. [Google Scholar] [CrossRef]
- Klingenheben, T.; Israel, C.W. Use of telemedicine in the diagnosis of paroxysmal atrial fibrillation and to monitor the effect of antiarrhythmic drug therapy. Herzschrittmachertherapie and Elektrophysiologie 2006, 17, 225–228. [Google Scholar] [CrossRef]
- Board, Q.D.H.I. Tele-cardiology for Patients with Chronic Heart Failure: The “SHL” experience in Israel and Germany. Stud. Health Technol. Inform. 2005, 114, 235–237. [Google Scholar]
- Atoui, H.; Télisson, D.; Fyan, J.; Rubel, P. Ambient intelligence and pervasive architecture designed within the EPI-MEDICS personal ECG monitor. Int. J. Healthcare Inform. Syst. Inform. 2008, 3, 68–80. [Google Scholar] [CrossRef]
- Hsieh, J.C.; Yu, K.C.; Yang, C.C. The realization of ubiquitous 12-lead ECG diagnosis in emergency telemedicine. Telemed. e-Health 2009, 15, 898–906. [Google Scholar] [CrossRef]
- Brunetti, N.D.; de Gennaro, L.; Dellegrottaglie, G.; Procacci, V.; di Biase, M. Fast and furious: Telecardiology in acute myocardial infarction triage in the emergency room setting. Eur. Res. Telemed. 2013, 2, 75–78. [Google Scholar] [CrossRef]
- Nallamothu, B.K.; Bates, E.R.; Herrin, J.; Wang, Y.; Bradley, E.H.; Krumholz, H.M. Times to treatment in transfer patients undergoing primary percutaneous coronary intervention in the United States national registry of myocardial infarction (NRMI)-3/4 Analysis. Circulation 2005, 111, 761–767. [Google Scholar] [CrossRef]
- Smith, S.C.; Feldman, T.E.; Hirshfeld, J.W.; Jacobs, A.K.; Kern, M.J.; King, S.B.; Morrison, D.A.; O’Neill, W.W.; Schaff, H.V.; Whitlow, P.L.; et al. ACC/AHA/SCAI 2005 Guideline update for percutaneous coronary intervention. A report of the American college of cardiology/American heart association task force on practice guidelines. J. Am. Coll. Cardiol. 2006, 47. [Google Scholar] [CrossRef]
- Hsieh, J.C.; Lo, H.C. The clinical application of a PACS-dependent 12-lead ECG and image information system in E-medicine and telemedicine. J. Digital Imaging 2010, 23, 501–513. [Google Scholar] [CrossRef]
- Mildenberger, P.; Eichelberg, M.; Martin, E. Introduction to the DICOM standard. Eur. Radiol. 2002, 12, 920–927. [Google Scholar] [CrossRef]
- Huang, H.K. PACS and imaging informatics: Basic principles and applications; Wiley: Hoboken, NJ, USA, 2009. [Google Scholar]
- Costa, C.; Oliveira, J.L. Telecardiology through ubiquitous Internet services. Int. J. Med. Inform. 2012, 81, 612–621. [Google Scholar] [CrossRef]
- Marcin, J.P.; Marcin, M.; Sadorra, C.; Dharmar, M. The Role of telemedicine in treating the critically ill. ICU Director 2012, 3, 70–74. [Google Scholar] [CrossRef]
- Lilly, C.M.; Cody, S.; Zhao, H.; Landry, K.; Baker, S.P.; McIlwaine, J.; Chandler, M.W.; Irwin, R.S. Hospital mortality, length of stay, and preventable complications among critically ill patients before and after tele-ICU reengineering of critical care processes. JAMA 2011, 305. [Google Scholar] [CrossRef]
- Goran, S.F. A second set of eyes: An introduction to tele-ICU. Crit. Care Nurse 2010, 30, 46–55. [Google Scholar] [CrossRef]
- Nikus, K.; Lähteenmäki, J.; Lehto, P.; Eskola, M. The role of continuous monitoring in a 24/7 telecardiology consultation service—A feasibility study. J. of Electrocardiol. 2009, 42, 473–480. [Google Scholar] [CrossRef]
- Zhang, P.; Kumabe, A.; Kogure, Y.; Akutagawa, M.; Kinouchi, Y.; Zhang, Q. New functions developed for ICU/CCU remote monitoring system using a 3G mobile phone and evaluations of the system. In Proceedings of the Conference of Medicine and Biological Society, Vancouver, Canada, 21–24 August 2008. [CrossRef]
- Ting, H.H.; Krumholz, H.M.; Bradley, E.H.; Cone, D.C.; Curtis, J.P.; Drew, B.J.; Field, J.M.; French, W.J.; Gibler, W.B.; Goff, D.C. Implementation and integration of prehospital ECGs into systems of care for acute coronary syndrome. A scientific statement from the American Heart Association Interdisciplinary Council on quality of care and outcomes research, emergency cardiovascular care committee, council on cardiovascular nursing, and council on clinical cardiology. Circulation 2008, 118, 1066–1079. [Google Scholar] [CrossRef]
- Grim, P.; Feldman, T.; Martin, M.; Donovan, R.; Nevins, V.; Childers, R.W. Cellular telephone transmission of 12-lead electrocardiograms from ambulance to hospital. Amer. J. Cardiol. 1987, 60, 715–720. [Google Scholar] [CrossRef]
- Pavlopoulos, S.; Kyriacou, E.; Berler, A.; Dembeyiotis, S.; Koutsouris, D. A novel emergency telemedicine system based on wireless communication technology-ambulance. IEEE Trans. Inf. Technol. Biomed. 1998, 2, 261–267. [Google Scholar] [CrossRef]
- Clark, E.N.; Sejersten, M.; Clemmensen, P.; Macfarlane, P.W. Automated electrocardiogram interpretation programs versus cardiologists’ triage decision making based on teletransmitted data in patients with suspected acute coronary syndrome. Amer. J. Cardiol. 2010, 106, 1696–1702. [Google Scholar] [CrossRef]
- Sejersten, M.; Sillesen, M.; Hansen, P.R.; Nielsen, S.L.; Nielsen, H.; Trautner, S.; Hampton, D.; Wagner, G.S.; Clemmensen, P. Effect on treatment delay of prehospital teletransmission of 12-lead electrocardiogram to a cardiologist for immediate triage and direct referral of patients with ST-segment elevation acute myocardial infarction to primary percutaneous coronary intervention. Amer. J. Cardiol. 2008, 101, 941–946. [Google Scholar] [CrossRef]
- Väisänen, O.; Mäkijärvi, M.; Silfvast, T. Prehospital ECG transmission: Comparison of advanced mobile phone and facsimile devices in an urban Emergency Medical Service System. Resuscitation 2003, 57, 179–185. [Google Scholar] [CrossRef]
- Hsieh, J.C.; Lin, B.X.; Wu, F.R.; Chang, P.C.; Tsuei, Y.W.; Yang, C.C. Ambulance 12-lead electrocardiography transmission via cell phone technology to cardiologists. Telemedicine and E-Health 2010, 16, 910–915. [Google Scholar] [CrossRef]
- Meadows-Pitt, M.; Fields, W. The impact of prehospital 12-lead electrocardiograms on door-to-balloon time in patients with ST-elevation myocardial infarction. J. Emerg. Nurs. 2013. In Press. [Google Scholar]
- Martinoni, A.; de Servi, S.; Boschetti, E.; Zanini, R.; Palmerini, T.; Politi, A.; Musumeci, G.; Belli, G.; de Paolis, M.; Ettori, F. Importance and limits of pre-hospital electrocardiogram in patients with ST elevation myocardial infarction undergoing percutaneous coronary angioplasty. Eur. J. Cardiovasc. Prev. Rehabil. 2011, 18, 526–532. [Google Scholar] [CrossRef]
- Maharaj, R.C.; Geduld, H.; Wallis, L.A. Door-to-needle time for administration of fibrinolytics in acute myocardial infarction in Cape Town. S. Afr. Med. J. 2012, 102, 241–244. [Google Scholar]
- Sable, C. Digital echocardiography and telemedicine applications in pediatric cardiology. Pediatr. Cardiol. 2002, 23, 358–369. [Google Scholar] [CrossRef]
- Giansanti, D.; Morelli, S. Digital tele-echocardiography: A look inside. Annali dell’Istituto superiore di sanità 2009, 45, 357–362. [Google Scholar]
- Pian, L.; Gillman, L.M.; McBeth, P.B.; Xiao, Z.; Ball, C.G.; Blaivas, M.; Hamilton, D.R.; Kirkpatrick, A.W. Potential use of remote telesonography as a transformational technology in underresourced and/or remote settings. Emerg. Med. Int. 2013, 1–9. [Google Scholar]
- Finley, J.P.; Sharratt, G.P.; Nanton, M.A.; Chen, R.P.; Bryan, P.; Wolstenholme, J.; MacDonald, C. Paediatric echocardiography by telemedicine-nine years’ experience. J. Telemed. Telecare 1996, 3, 200–204. [Google Scholar]
- Trippi, J.A.; Kopp, G.; Lee, K.S.; Morrison, H.; Risk, G.; Jones, J.H.; Cordell, W.H.; Chrapla, M.; Nelson, D. The feasibility of dobutamine stress echocardiography in the emergency department with telemedicine interpretation. J. Am. Soc. Echocardiogr. 1996, 9, 113–118. [Google Scholar] [CrossRef]
- Widmer, S.; Ghisla, R.; Ramelli, G.P.; Taminelli, F.; Widmer, B.; Caoduro, L.; Gallino, A. Tele-echocardiography in paediatrics. Eur. J. Pediatr. 2003, 162, 271–275. [Google Scholar]
- Grant, B.; Morgan, G.J.; McCrossan, B.A.; Crealey, G.E.; Sands, A.J.; Craig, B.; Casey, F.A. Remote diagnosis of congenital heart disease: the impact of telemedicine. Arch. Dis. Child. 2010, 95, 276–280. [Google Scholar] [CrossRef]
- Dowie, R.; Mistry, H.; Young, T.A.; Franklin, R.C.; Gardiner, H.M. Cost implications of introducing a telecardiology service to support fetal ultrasound screening. J. Telemed. Telecare 2008, 14, 421–426. [Google Scholar] [CrossRef]
- McCrossan, B.A.; Sands, A.J.; Kileen, T.; Doherty, N.N.; Casey, F.A. A fetal telecardiology service: Patient preference and socio‐economic factors. Prenatal Diag. 2012, 32, 883–887. [Google Scholar]
- Huang, T.; Moon-Grady, A.J.; Traugott, C.; Marcin, J. The availability of telecardiology consultations and transfer patterns from a remote neonatal intensive care unit. J. Telemed. Telecare 2008, 14, 244–248. [Google Scholar]
- Andersen, G.N.; Haugen, B.O.; Graven, T.; Salvesen, Ø.; Mjølstad, O.C.; Dalen, H. Feasibility and reliability of point-of-care pocket-sized echocardiography. Eur. J. Echocardiogr. 2011, 12, 665–670. [Google Scholar] [CrossRef]
- Panoulas, V.F.; Daigeler, A.-L.; Malaweera, A.S.; Lota, A.S.; Baskaran, D.; Rahman, S.; Nihoyannopoulos, P. Pocket-size hand-held cardiac ultrasound as an adjunct to clinical examination in the hands of medical students and junior doctors. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 323–330. [Google Scholar]
- Choi, B.G.; Mukherjee, M.; Dala, P.; Young, H.A.; Tracy, C.M.; Katz, R.J.; Lewis, J.F. Interpretation of remotely downloaded pocket-size cardiac ultrasound images on a web-enabled smartphone: Validation against workstation evaluation. J. Am. Soc. Echocardiogr. 2011, 24, 1325–1330. [Google Scholar]
- Prinz, C.; Dohrmann, J.; Buuren, F.V.; Bitter, T.; Bogunovic, N.; Horstkotte, D.; Faber, L. Diagnostic performance of handheld echocardiography for the assessment of basic cardiac morphology and function: A validation study in routine cardiac patients. Echocardiography 2012, 29, 887–894. [Google Scholar] [CrossRef]
- Karson, T.H.; Zepp, R.C.; Chandra, S.; Morchead, A.; Thomas, J.D. Digital storage of echocardiograms offers superior image quality to analog storage, even with 20: 1 digital compression: results of the Digital Echo Record Access Study. J. Am. Soc. Echocardiogr. 1996, 9, 769–778. [Google Scholar] [CrossRef]
- Langer, S.G. Challenges for data storage in medical imaging research. J. Digital Imaging 2011, 24, 203–207. [Google Scholar] [CrossRef]
- Teng, C.C.; Mitchell, J.; Walker, C.; Swan, A.; Davila, C.; Howard, D.; Needham, T. A medical image archive solution in the cloud. Softw. Eng. Serv. Sci. 2010, 431–434. [Google Scholar]
- Agrawal, D.; Das, S.; Abbadi, A. In Big data and cloud computing: current state and future opportunities. In Proceedings of the 14th International Conference on Extending Database Technology, Uppsala, Sweden, 22–24 March 2011; ACM Digital Library: New York, NY, USA, 2011. [Google Scholar] [CrossRef]
- Mell, P.; Grance, T. Final Version of NIST Cloud Computing Definition Published. Available online: http://csrc.nist.gov/publications/nistpubs/800-145/SP800-145.pdf (accessed on 8,November 2013).
- Chia, C.C.; Syed, Z. Computationally generated cardiac biomarkers: Heart rate patterns to predict death following coronary attacks. In Proceedings of the 11th SIAM International Conference on Data Mining (SDM11), Mesa, AZ, USA, 28–30 April 2011; pp. 735–746.
- Keyes, R.W.; Romano, C.; Arnold, D.; Luan, S. Radiation Therapy Calculations Using an On-demand Virtual Cluster via Cloud Computing. Available online: http://arxiv.org/pdf/1009.5282v1.pdf (accessed on 8 November 2013).
- Raju, P.K.; Prasad, S. Telemedicine and cardiology—Decade of our experience. J. Indian Coll. Cardiol. 2012, 2, 4–16. [Google Scholar] [CrossRef]
- Philbin, J.; Prior, F.; Nagy, P. Will the next generation of PACS be sitting on a cloud? J. Digital Imaging 2011, 24, 179–183. [Google Scholar] [CrossRef]
- Silva, L.A.B.; Costa, C.; Oliveira, J.L. A PACS archive architecture supported on cloud services. Int. J. Comput. Assist. Radiol. Surg. 2012, 7, 349–358. [Google Scholar] [CrossRef]
- Ratib, O.; Rosset, A.; Heuberger, J. Open source software and social networks: Disruptive alternatives for medical imaging. Eur. J. Radiol. 2011, 78, 259–265. [Google Scholar] [CrossRef]
- Kagadis, G.C.; Alexakos, C.; Langer, S.G.; French, T. Using an open-source PACS virtual machine for a digital angiography unit: Methods and initial impressions. J. Digital Imaging 2012, 25, 81–90. [Google Scholar] [CrossRef]
- Rostrom, T.; Teng, C.C. Secure communications for PACS in a cloud environment. Eng. Med. Biol. Soc. 2011, 8219–8222. [Google Scholar]
- Norcen, R.; Podesser, M.; Pommer, A.; Schmidt, H.-P.; Uhl, A. Confidential storage and transmission of medical image data. Comp. Biol. Med. 2003, 33, 277–292. [Google Scholar] [CrossRef]
- Pearson, S.; Shen, Y.; Mowbray, M. A privacy manager for cloud computing. Cloud Comput. Lect. Note. Comput. Sci. 2009, 5931, 90–106. [Google Scholar] [CrossRef]
- Mowbray, M.; Pearson, S.; Shen, Y. Enhancing privacy in cloud computing via policy-based obfuscation. J. Supercomp. 2012, 61, 267–291. [Google Scholar] [CrossRef]
- Satyanarayanan, M.; Bahl, P.; Caceres, R.; Davies, N. The case for vm-based cloudlets in mobile computing. Pervasive Comput. IEEE 2009, 8, 14–23. [Google Scholar] [CrossRef]
- Rikitake, K.; Araki, Y.; Kawahara, Y.; Minami, M.; Morikawa, H. NGN/IMS-based Ubiquitous Health Monitoring System. In Proceedings of 6th IEEE Consumer Communications and Networking Conference, Las Vegas, NV, USA, 10–13 January 2011; pp. 1–2.
- Krendzel, A.; Lopatin, S.; Mangues-Bafalluy, J. Implementation of NGN/IMS Technologies into Legacy Network Infrastructures. In Proceedings of World Telecommunication Congress, Vienna, Austria, 13–14 September 2010; pp. 1–6.
- Skodras, A.; Christopoulos, C.; Ebrahimi, T. The JPEG 2000 still image compression standard. IEEE Signal Process. Mag. 2001, 18, 36–58. [Google Scholar]
- Wiegand, T.; Sullivan, G.J.; Bjontegaard, G.; Luthra, A. Overview of the H264/AVC video coding standard. Circ. Syst. Video T. 2003, 13, 560–576. [Google Scholar] [CrossRef]
- Kim, D.K.; Kim, E.Y.; Yang, K.H.; Lee, C.K.; Yoo, S.K. A mobile tele-radiology imaging system with JPEG2000 for an emergency care. J. Digital Imaging 2011, 24, 709–718. [Google Scholar]
- Pedersen, P.C.; Dickson, B.W.; Chakareski, J. Telemedicine applications of mobile ultrasound. In Proceedings of IEEE International Workshop on Multimedia Signal Process, Rio de Janeiro, Brazil, 5–7 October 2009; pp. 1–6.
- Satyanarayanan, M. Pervasive computing: Vision and challenges. IEEE Personal Commun. 2001, 8, 10–17. [Google Scholar] [CrossRef]
- Kumar, K.; Lu, Y.-H. Cloud computing for mobile users: Can offloading computation save energy? Computer 2010, 43, 51–56. [Google Scholar] [CrossRef]
- Trigo, J.D.; Alesanco, A.; Martinez, I.; Garcia, J. A review on digital ECG formats and the relationships between them. Inform. Technol. Biomed. 2012, 16, 432–444. [Google Scholar] [CrossRef]
- Sakkalis, V.; Chiarugi, F.; Kostomanolakis, S.; Chronaki, C.; Tsiknakis, M.; Orphanoudakis, S. A gateway between the SCP-ECG and the DICOM supplement 30 waveform standard. Comput. Cardiol. 2003, 30, 25–28. [Google Scholar]
- van Ettinger, M.; Lipton, J.; de Wijs, M.; van der Putten, N.; Nelwan, S. An open source ECG toolkit with DICOM. Comput. Cardiology 2008, 35, 441–444. [Google Scholar]
- Chronaki, C.; Chiarugi, F.; Lees, P.; Bruun-Rasmussen, M.; Conforti, F.; Ruiz Fernandez, R.; Zywietz, C. Open ECG: A European project to promote the SCP-ECG standard, a further step towards interoperability in electrocardiography. Comput. Cardiology 2002, 29, 285–288. [Google Scholar]
- Lubbers, P.; Albers, B.; Salim, F. Overview of HTML5. In Pro HTML5 Programming; Apress: New York, NY, USA, 2011. [Google Scholar]
- Holzinger, A.; Treitler, P.; Slany, W. Making apps useable on multiple different mobile platforms: On interoperability for business application development on smartphones. Lect. Note. Computer Sci. 2012, 7465, 176–189. [Google Scholar]
- DICOM Part 16: Content Mapping Resource, NEMA, Rosslyn, Virginia 22209, USA. 2011. Available online: http://medical.nema.org/Dicom/2011/11_16pu.pdf (accessed on 17 August 2013).
- DICOM Supplement 23: Structured Reporting SOP Classes, NEMA, Rosslyn, Virginia 22209, USA. 2011. Available online: http://medical.nema.org/Dicom/supps/sup23_lb.pdf (accessed on 17 August 2013).
- Hussein, R.; Engelmann, U.; Schroeter, A.; Meinzer, H.P. DICOM structured reporting Part 1. Overview and characteristics1. Radiographics. 2004, 24, 891–896. [Google Scholar] [CrossRef]
- Hussein, R.; Engelmann, U.; Schroeter, A.; Meinzer, H.P. DICOM structured reporting Part 2. Problems and challenges in implementation for PACS workstations1. Radiographics. 2004, 24, 897–909. [Google Scholar] [CrossRef]
- Howe, D.; Costanzo, M.; Fey, P.; Gojobori, T.; Hannick, L.; Hide, W.; Hill, D.P.; Kania, R.; Schaeffer, M.; St Pierre, S. Big data: The future of biocuration. Nature 2008, 455, 47–50. [Google Scholar] [CrossRef]
- Bidgood, W.D., Jr. Clinical importance of the DICOM structured reporting standard. Int. J. Cardiac Imaging 1998, 14, 307–315. [Google Scholar] [CrossRef]
- Homorodean, C.; Olinic, M.; Olinic, D. Development of a methodology for structured reporting of information in echocardiography. Med. Ultrason. 2012, 14, 29–33. [Google Scholar]
- Swinfen Charitable Trust. Available online: http://www.swinfencharitabletrust.org (accessed on 28 October 2013).
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Hsieh, J.-C.; Li, A.-H.; Yang, C.-C. Mobile, Cloud, and Big Data Computing: Contributions, Challenges, and New Directions in Telecardiology. Int. J. Environ. Res. Public Health 2013, 10, 6131-6153. https://doi.org/10.3390/ijerph10116131
Hsieh J-C, Li A-H, Yang C-C. Mobile, Cloud, and Big Data Computing: Contributions, Challenges, and New Directions in Telecardiology. International Journal of Environmental Research and Public Health. 2013; 10(11):6131-6153. https://doi.org/10.3390/ijerph10116131
Chicago/Turabian StyleHsieh, Jui-Chien, Ai-Hsien Li, and Chung-Chi Yang. 2013. "Mobile, Cloud, and Big Data Computing: Contributions, Challenges, and New Directions in Telecardiology" International Journal of Environmental Research and Public Health 10, no. 11: 6131-6153. https://doi.org/10.3390/ijerph10116131