
Trabectedin in Soft Tissue Sarcomas

1
University of Washington, 1959 NE Pacific St, Seattle, WA 98195, USA
2
Fred Hutchinson Cancer Research Center, University of Washington, 825 Eastlake Avenue East, G-3630, Seattle, WA 98109-1023, USA
*
Author to whom correspondence should be addressed.
Mar. Drugs 2015, 13(2), 974-983; https://doi.org/10.3390/md13020974
Submission received: 23 December 2014
/
Revised: 27 January 2015
/
Accepted: 2 February 2015
/
Published: 12 February 2015
(This article belongs to the Collection Marine Compounds and Cancer)
{kind=link}
Abstract
:Soft tissue sarcomas are a group of rare tumors derived from mesenchymal tissue, accounting for about 1% of adult cancers. There are over 60 different histological subtypes, each with their own unique biological behavior and response to systemic therapy. The outcome for patients with metastatic soft tissue sarcoma is poor with few available systemic treatment options. For decades, the mainstay of management has consisted of doxorubicin with or without ifosfamide. Trabectedin is a synthetic agent derived from the Caribbean tunicate, Ecteinascidia turbinata. This drug has a number of potential mechanisms of action, including binding the DNA minor groove, interfering with DNA repair pathways and the cell cycle, as well as interacting with transcription factors. Several phase II trials have shown that trabectedin has activity in anthracycline and alkylating agent-resistant soft tissue sarcoma and suggest use in the second- and third-line setting. More recently, trabectedin has shown similar progression-free survival to doxorubicin in the first-line setting and significant activity in liposarcoma and leiomyosarcoma subtypes. Trabectedin has shown a favorable toxicity profile and has been approved in over 70 countries for the treatment of metastatic soft tissue sarcoma. This manuscript will review the development of trabectedin in soft tissue sarcomas.
1. Introduction
Soft tissue sarcomas are a group of rare solid tumors of mesenchymal origin. Surgical resection with or without radiation is the mainstay of management for localized disease. However, approximately 50% of patients with high-grade tumors will develop recurrent disease. Systemic therapy may additionally be considered in the localized setting, but its role in management remains controversial. The outcome of patients with metastatic soft tissue sarcoma is poor with a median overall survival (OS) of about 12 months. Systemic therapy is at the core of management for patients with metastatic disease; however, there are few effective agents available. Doxorubicin and ifosfamide have shown consistent activity, and recently, the anti-angiogenic agent, pazopanib, has been approved based on the results of a randomized, placebo-controlled phase III trial showing a significant, but modest, benefit in progression-free survival (PFS) for patients treated with pazopanib [1].
Trabectedin is a synthetic, marine-derived alkylating agent derived from the Caribbean tunicate, Ecteinascidia turbinata [2]. The success of trabectedin in preliminary clinical trials for soft tissue sarcomas has led to the approval of the drug in many countries and a large, randomized phase III trial. With limited systemic therapy options available for sarcomas as a whole, trabectedin has the opportunity to be significantly beneficial for patients with metastatic disease.
2. Mechanism of Action
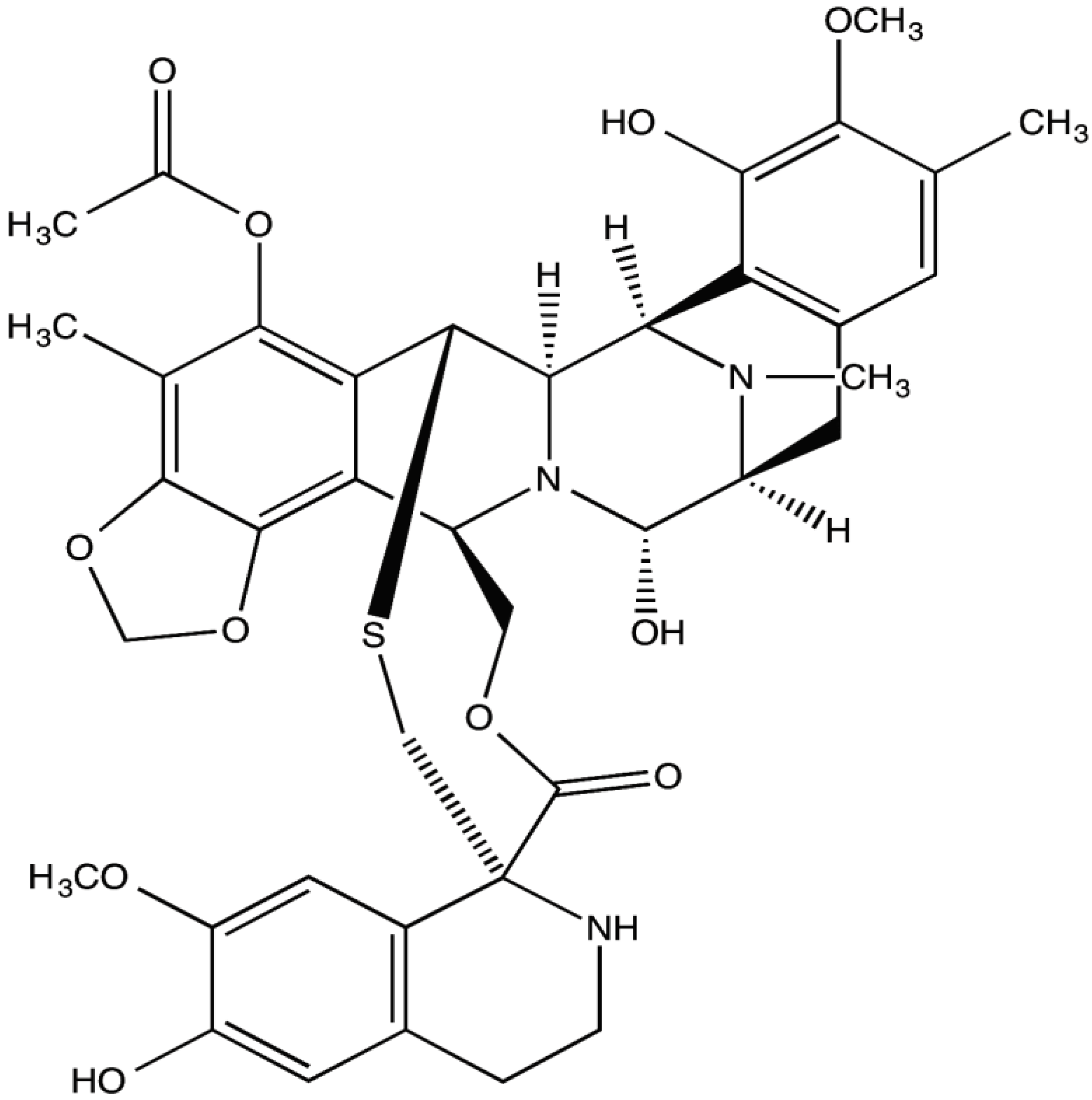
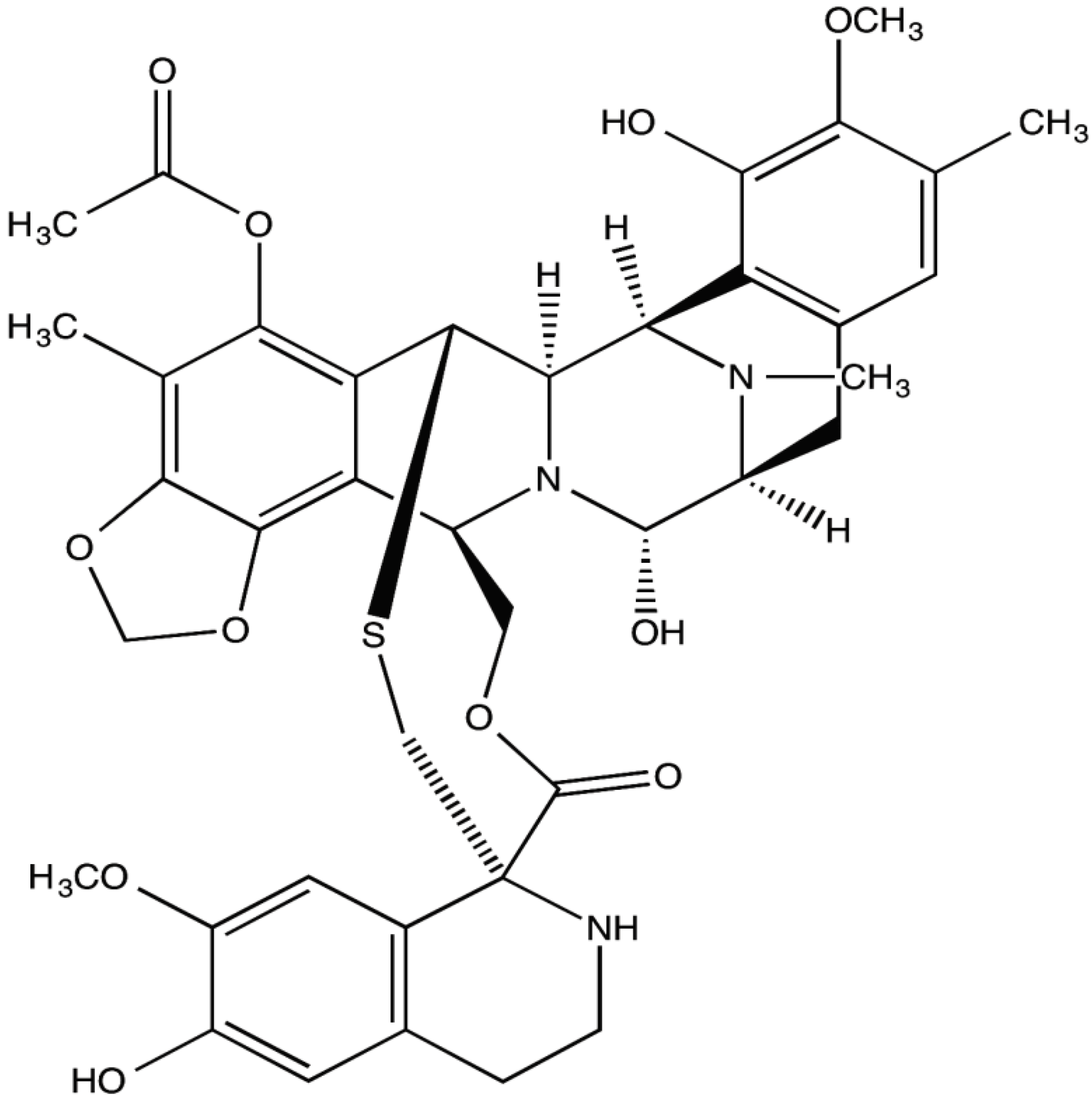
Trabectedin is a natural alkaloid composed of three tetrahydroisoquinolone rings (Figure 1). The unique structure of trabectedin allows it to bind to the N2 amino group of guanine residues in the minor groove of the DNA double helix and can lead to double-strand breaks [3,4]. Studies have suggested that the nucleotide excision repair mechanism may be essential for the antitumor activity of trabectedin and that the resulting double-strand breaks are more persistent if there is loss of homologous repair [5,6]. Evidence shows that disruption of DNA by trabectedin ultimately causes apoptosis and sensitization of cancer cells to Fas-mediated cell death [7]. Multiple studies, including specific experiments in soft tissue sarcomas, have also validated that trabectedin works at the tumor microenvironment with selective activity against monocytes and tumor-associated macrophages [8,9]. The inhibition of these immune factors allows for the prevention of angiogenesis and further disease progression [10,11]. Deprivation of inflammatory-mediated support in the tumor microenvironment may be one of the most important aspects of trabectedin’s mechanism of action, making the drug efficacious as a cancer treatment. Other mechanisms for the chemotherapeutic actions of trabectedin may include modulation of the cell cycle and interaction with transcription factors [12,13].
Recent studies have also proposed specific mechanisms of action for trabectedin in myxoid/round cell liposarcoma. The most common translocation in the disease is t(12;16)(q13;p11), creating a FUS-CHOP fusion gene, and rarely, a t(12;22)(q13;q12) translocation takes place resulting in a EWS-CHOP fusion gene. These fusion-encoded proteins are believed to function as abnormal transcription factors [14]. Notably, an in vivo study showed that mesenchymal stem cells expressing the FUS-CHOP protein were committed to adipocytic differentiation, but were unable to terminally differentiate [15]. Trabectedin administration in this experiment downregulated FUS:CHOP expression, which promoted terminal adipocytic differentiation. Others have hypothesized that trabectedin prevents the binding of the FUS-CHOP oncogenic chimera protein to its target promoters, which may modulate the transcription of genes that are essential for adipocytic differentiation [14,16]. Recent studies have also characterized regulatory networks leading to trabectedin resistance, as well as have uncovered the antiangiogenic activity of trabectedin in myxoid/round cell liposarcoma [17,18].
Figure 1.
Chemical structure of trabectedin.
3. Phase I Trials
A number of phase I trials have assessed differential dosing and infusion schedules for the administration of trabectedin [19,20,21,22,23,24,25]. Results from these studies have established the optimal regimen of administration to be a 1.5-mg/m2 infusion over 24 h every three weeks [26]. Notably, Taamma and colleagues performed a phase I trial of trabectedin in 52 patients with treatment refractory tumors that recommended the current optimal dosing schedule of 1.5 mg/m2 for a 24-h continuous infusion [22]. The most prevalent dose limiting toxicities in the study were hematological in nature. At the recommended dose, severe neutropenia was reported in 33% of cycles, severe thrombocytopenia in 10% of cycles and reversible, but severe, elevations in transaminase levels in 38% of cycles. The investigators also observed that patients with baseline hepatobiliary function abnormalities had a higher likelihood of severe hematological toxicity, indicating the need for dose reduction in such patients.
Combination therapies of trabectedin with other chemotherapeutic agents, including gemcitabine, doxorubicin, Doxil and cisplatin, have also been assessed in phase I trials [27,28,29,30,31,32]. The most promising results from these studies in sarcoma patients have been from the trials administering trabectedin in combination with doxorubicin. One of the trials showed a response rate (RR) of 18% and stable disease in 56% of soft tissue sarcoma patients (n = 29) [31]. Another study assessing combination therapy with doxorubicin reported a RR of 12% with median PFS of 9.2 months for 41 patients with solid tumors [27]. Of the 41 patients, 20 had liposarcoma and 11 had leiomyosarcoma. With success in phase I trials, the efficacy of combination therapy with doxorubicin and trabectedin is currently under investigation in larger studies.
4. Phase II Trials
Two phase II trials in 2004 provided the initial analysis of trabectedin in soft tissue sarcomas. The first of these studies was run on 54 pretreated soft tissue sarcoma patients and reported a low response rate of 4%, but a high disease control rate at six months of 24% [33]. Trabectedin was administered at a dose of 1.5 mg/m2, over 24 h every three weeks. Approximately half of the patients in the study eventually developed grade 3/4 aspartate aminotransferase (AST) and alanine aminotransferase (ALT) levels. Another common adverse event was neutropenia, being grade 3/4 in 61% of patients. In this trial, four patients (7.4%) discontinued trabectedin due to adverse events. In addition, there were two treatment-related deaths, and both were patients who developed acute renal failure.
The second phase II trial, published in 2004, again reported a low response rate of 8% and a one-year overall survival rate of 53% in 36 previously treated sarcoma patients [34]. This study also utilized the same dosing schedule of trabectedin (1.5 mg/m2, over 24 h every three weeks). The toxicity profile of the drug was similar to previous trials with patients experiencing elevations in transaminases, fatigue and hematological toxicity. Growth factors, such as, granulocyte-colony stimulating factor (G-CSF), can be administered to help prevent hematological toxicity; however, a recent retrospective study showed that G-CSF administration has only been used in about 10% of phase II trials on trabectedin in solid tumors [35].
Early promising results in these phase II studies led the European Organization for the Research and Treatment of Cancer (EORTC) to initiate a phase II trial of trabectedin in 104 patients treated in the second- and third-line setting [36]. This trial also reported a low response rate of 8%. The six-month PFS was 29%, and the median overall survival (OS) was reported as 9.2 months. Subsequently, a further phase II trial in 36 patients was run to evaluate the activity of trabectedin in the first-line setting. The overall response rate was reported as 17%, and the one-year PFS and OS rates were 21% and 72%, respectively [37]. This study also importantly concluded that trabectedin has similar ranges of objective responses and overall survival rates in the first-line setting to the two most active drugs in soft tissue sarcomas: doxorubicin and ifosfamide.
Demetri and colleagues performed a phase II trial randomizing 270 patients with leiomyosarcoma and liposarcoma to receive either 1.5 mg/m2 of trabectedin over 24 h every three weeks, or 0.58 mg/m2 over 3 h every week for three out of four weeks [38]. Patients were required to have experienced documented disease progression while on doxorubicin and ifosfamide prior to trial entry. The 24-h infusion schedule showed a significantly longer median time to progression (TTP) (3.7 vs. 2.3 months) and PFS (3.3 vs. 2.3 months), as compared to the 3-h infusion schedule. No significant difference in overall survival was observed between the two arms of the trial; however, there was a strong trend favoring the 24-h infusion schedule (13.9 months vs. 11.8 months). Trabectedin was generally well tolerated in this study, with the most frequently reported grade 3/4 adverse events being neutropenia and elevated transaminases. Febrile neutropenia occurred in 1% of patients, and the majority of adverse events were mild to moderate. There was also no documentation of cumulative toxicities. Another phase II trial recommended the use of trabectedin as a neoadjuvant therapy for patients with advanced myxoid liposarcoma [39].
The results of these phase II trials led to licensing approval of trabectedin by the European Union for advanced soft tissue sarcoma in 2007, and the drug is now approved in over 70 countries.
5. Phase III Trials
Trabectedin has yet to be approved by the FDA in the United States, and consequently a phase III trial has been performed randomizing over 500 patients with leiomyosarcoma and liposarcoma to receive either trabectedin or dacarbazine (2:1 ratio). The primary end point of the trial is overall survival. This trial has closed to enrollment, and the results are eagerly awaited (NCT01343277).
In addition, there is an ongoing worldwide, expanded access program (NCT00210665). A recent analysis from this study reported that of the 1,895 soft tissue sarcoma patients entered into the program, patients with leiomyosarcoma and liposarcoma had significantly longer OS compared to all other histological subtypes (16.2 vs. 8.4 months, respectively), as well as a higher objective response rate (6.9% vs. 4%, respectively) [40].
Another phase III trial randomized 121 patients with translocation-related sarcomas to receive trabectedin or doxorubicin in the first-line setting with progression-free survival as the primary end point [41]. There was no significant difference in PFS between the two arms of the trial. At the time of analysis, 63.9% and 58.3% of patients were alive in the trabectedin and doxorubicin arms, respectively (with no statistically significant difference in overall survival). The response rate according to RECIST 1.0 was significantly higher in the doxorubicin (27%) compared to the trabectedin (5.9%) arm of the trial. In contrast, the response according to Choi criteria showed fewer differences between the doxorubicin (45.9%) and trabectedin (37.3%) arms, in terms of response rate.
6. Retrospective Studies
Trabectedin has shown particular activity in myxoid/round cell liposarcoma. In a retrospective analysis of 51 patients treated at five referral centers, a median overall response rate of 51% was reported, and the median PFS was 14 months [42]. Progression-free survival at six months was also reported as 88%. In another retrospective study assessing the efficacy of trabectedin in specific translocation-related sarcomas, the rate of PFS at six months was documented as 64% in myxoid/round cell liposarcoma (n = 27) and 22% in synovial sarcoma (n = 45) [43]. These results suggest that trabectedin may have significant activity in these two histological subtypes and should be further analyzed in larger randomized clinical trials.
Other retrospective studies have shown that trabectedin may also be effective in uterine leiomyosarcoma. In a study assessing 66 patients with metastatic uterine leiomyosarcoma, PFS for the entire cohort was 3.3 months with 16% of patients achieving a partial response and 35% showing stable disease [44]. Furthermore, a prospective phase II trial of trabectedin in uterine leiomyosarcoma reported a median PFS of 5.8 months and OS of 26.1 months [45]. Two patients in the study also had a partial response to trabectedin administration (10%).
Retrospective analysis was also used to assess the effect of age on the efficacy and safety of trabectedin administration in the treatment of soft tissue sarcomas [46]. Patients under the age of 60 were part of the younger cohort, and patients 60 or older were a part of the older cohort. The analysis pooled five prior phase II trials and showed similar response rates (younger 10.1% vs. older 9.6%), no significant difference in median progression-free survival (younger 2.5 vs. older 3.7 months) and similar overall survival rates between cohorts (younger 13.0 vs. older 14.0 months). However, older patients did show a higher incidence of grade 3/4 neutropenia (43.6% vs. 60.2%) and fatigue (6.3% vs. 14.4%). A small subset of patients 70 or older were also included in the analysis and showed no significant differences in efficacy or safety outcomes. This study therefore indicates that trabectedin can have meaningful benefits and an acceptable safety profile in young and elderly patients.
7. Conclusions
Trabectedin has shown consistent activity in patients with previously treated soft tissue sarcoma. The results of a number of phase II trials have led to the drug being approved in over 70 countries worldwide. The results of a phase III trial randomizing leiomyosarcoma and liposarcoma patients to receive trabectedin or dacarbazine are awaited and could lead to the drug being approved by the FDA.
Acknowledgments
SMP, ETL and RLJ are supported by the Bob and Eileen Gilman Family Sarcoma Research Fund.
Author Contributions
All authors provided significant contributions in writing and editing the manuscript.
Conflicts of Interest
Jones has been an investigator on clinical trials sponsored by Pharmamar and Johnson and Johnson.
References
- Van der Graaf, W.T.A.; Blay, J.-Y.; Chawla, S.P.; Kim, D.-W.; Bui-Nguyen, B.; Casali, P.G.; Schöffski, P.; Aglietta, M.; Staddon, A.P.; Beppu, Y.; et al. Pazopanib for metastatic soft-tissue sarcoma (palette): A randomised, double-blind, placebo-controlled phase 3 trial. Lancet 2012, 379, 1879–1886. [Google Scholar]
- Cuevas, C.; Francesch, A. Development of yondelis[registered sign] (trabectedin, et-743). A semisynthetic process solves the supply problem. Nat. Prod. Rep. 2009, 26, 322–337. [Google Scholar] [CrossRef] [PubMed]
- D’Incalci, M.; Galmarini, C.M. A review of trabectedin (et-743): A unique mechanism of action. Mol. Cancer Ther. 2010, 9, 2157–2163. [Google Scholar] [CrossRef] [PubMed]
- Guirouilh-Barbat, J.; Redon, C.; Pommier, Y. Transcription-coupled DNA double-strand breaks are mediated via the nucleotide excision repair and the mre11-rad50-nbs1 complex. Mol. Biol. Cell 2008, 19, 3969–3981. [Google Scholar] [CrossRef] [PubMed]
- Soares, D.G.; Escargueil, A.E.; Poindessous, V.; Sarasin, A.; de Gramont, A.; Bonatto, D.; Henriques, J.A.P.; Larsen, A.K. Replication and homologous recombination repair regulate DNA double-strand break formation by the antitumor alkylator ecteinascidin 743. Proc. Natl. Acad. Sci. USA 2007, 104, 13062–13067. [Google Scholar] [CrossRef] [PubMed]
- Tavecchio, M.; Simone, M.; Erba, E.; Chiolo, I.; Liberi, G.; Foiani, M.; D’Incalci, M.; Damia, G. Role of homologous recombination in trabectedin-induced DNA damage. Eur. J. Cancer 2008, 44, 609–618. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Serra, J.; Maffiotte, E.; Martín, J.; Bex, T.; Navarro-Palou, M.; Ros, T.; Plazas, J.M.; Vögler, O.; Gutiérrez, A.; Amat, J.C.; et al. Yondelis® (et-743, trabectedin) sensitizes cancer cell lines to cd95-mediated cell death: New molecular insight into the mechanism of action. Eur. J. Pharmacol. 2011, 658, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Allavena, P.; Signorelli, M.; Chieppa, M.; Erba, E.; Bianchi, G.; Marchesi, F.; Olimpio, C.O.; Bonardi, C.; Garbi, A.; Lissoni, A.; et al. Anti-inflammatory properties of the novel antitumor agent yondelis (trabectedin): Inhibition of macrophage differentiation and cytokine production. Cancer Res. 2005, 65, 2964–2971. [Google Scholar] [CrossRef] [PubMed]
- Germano, G.; Frapolli, R.; Belgiovine, C.; Anselmo, A.; Pesce, S.; Liguori, M.; Erba, E.; Uboldi, S.; Zucchetti, M.; Pasqualini, F.; et al. Role of macrophage targeting in the antitumor activity of trabectedin. Cancer Cell 2013, 23, 249–262. [Google Scholar] [CrossRef] [PubMed]
- Galmarini, C.M.; Incalci, M.; Allavena, P. Trabectedin and plitidepsin: Drugs from the sea that strike the tumor microenvironment. Mar. Drugs 2014, 12, 719–733. [Google Scholar] [CrossRef] [PubMed]
- D'Incalci, M.; Badri, N.; Galmarini, C.M.; Allavena, P. Trabectedin, a drug acting on both cancer cells and the tumour microenvironment. Br. J. Cancer 2014, 111, 646–650. [Google Scholar] [CrossRef] [PubMed]
- Bonfanti, M.; la Valle, E.; Fernandez Sousa Faro, J.M.; Faircloth, G.; Caretti, G.; Mantovani, R.; D'Incalci, M. Effect of ecteinascidin-743 on the interaction between DNA binding proteins and DNA. Anti-Cancer Drug Des. 1999, 14, 179–186. [Google Scholar]
- Erba, E.; Bergamaschi, D.; Bassano, L.; Damia, G.; Ronzoni, S.; Faircloth, G.T.; D’Incalci, M. Ecteinascidin-743 (et-743), a natural marine compound, with a unique mechanism of action. Eur. J. Cancer 2001, 37, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Di Giandomenico, S.; Frapolli, R.; Bello, E.; Uboldi, S.; Licandro, S.A.; Marchini, S.; Beltrame, L.; Brich, S.; Mauro, V.; Tamborini, E.; et al. Mode of action of trabectedin in myxoid liposarcomas. Oncogene 2014, 33, 5201–5210. [Google Scholar] [CrossRef] [PubMed]
- Charytonowicz, E.; Terry, M.; Coakley, K.; Telis, L.; Remotti, F.; Cordon-Cardo, C.; Taub, R.N.; Matushansky, I. Pparγ agonists enhance et-743-induced adipogenic differentiation in a transgenic mouse model of myxoid round cell liposarcoma. J. Clin. Investig. 2012, 122, 886–898. [Google Scholar] [CrossRef] [PubMed]
- Forni, C.; Minuzzo, M.; Virdis, E.; Tamborini, E.; Simone, M.; Tavecchio, M.; Erba, E.; Grosso, F.; Gronchi, A.; Aman, P.; et al. Trabectedin (et-743) promotes differentiation in myxoid liposarcoma tumors. Mol. Cancer Ther. 2009, 8, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Dossi, R.; Frapolli, R.; Di Giandomenico, S.; Paracchini, L.; Bozzi, F.; Brich, S.; Castiglioni, V.; Borsotti, P.; Belotti, D.; Uboldi, S.; et al. Antiangiogenic activity of trabectedin in myxoid liposarcoma: Involvement of host timp-1 and timp-2 and tumor thrombospondin-1. Int. J. Cancer 2015, 136, 721–729. [Google Scholar] [PubMed]
- Uboldi, S.; Calura, E.; Beltrame, L.; Fuso Nerini, I.; Marchini, S.; Cavalieri, D.; Erba, E.; Chiorino, G.; Ostano, P.; D’Angelo, D.; et al. A systems biology approach to characterize the regulatory networks leading to trabectedin resistance in an in vitro model of myxoid liposarcoma. PLoS One 2012, 7, e35423. [Google Scholar] [CrossRef] [PubMed]
- Forouzesh, B.; Hidalgo, M.; Chu, Q.; Mita, A.; Mita, M.; Schwartz, G.; Jimeno, J.; Gómez, J.; Alfaro, V.; Lebedinsky, C.; et al. Phase I and pharmacokinetic study of trabectedin as a 1- or 3-h infusion weekly in patients with advanced solid malignancies. Clin. Cancer Res. 2009, 15, 3591–3599. [Google Scholar] [CrossRef] [PubMed]
- Puchalski, T.; Ryan, D.; Garcia-Carbonero, R.; Demetri, G.; Butkiewicz, L.; Harmon, D.; Seiden, M.; Maki, R.; Lopez-Lazaro, L.; Jimeno, J.; et al. Pharmacokinetics of ecteinascidin 743 administered as a 24-h continuous intravenous infusion to adult patients with soft tissue sarcomas: Associations with clinical characteristics, pathophysiological variables and toxicity. Cancer Chemother. Pharmacol. 2002, 50, 309–319. [Google Scholar] [CrossRef] [PubMed]
- Ryan, D.P.; Supko, J.G.; Eder, J.P.; Seiden, M.V.; Demetri, G.; Lynch, T.J.; Fischman, A.J.; Davis, J.; Jimeno, J.; Clark, J.W. Phase I and pharmacokinetic study of ecteinascidin 743 administered as a 72-h continuous intravenous infusion in patients with solid malignancies. Clin. Cancer Res. 2001, 7, 231–242. [Google Scholar] [PubMed]
- Taamma, A.; Misset, J.L.; Riofrio, M.; Guzman, C.; Brain, E.; Lopez Lazaro, L.; Rosing, H.; Jimeno, J.M.; Cvitkovic, E. Phase I and pharmacokinetic study of ecteinascidin-743, a new marine compound, administered as a 24-h continuous infusion in patients with solid tumors. J. Clin. Oncol. 2001, 19, 1256–1265. [Google Scholar] [PubMed]
- Twelves, C.; Hoekman, K.; Bowman, A.; Vermorken, J.B.; Anthoney, A.; Smyth, J.; van Kesteren, C.; Beijnen, J.H.; Uiters, J.; Wanders, J.; et al. Phase I and pharmacokinetic study of yondelis™ (ecteinascidin-743; et-743) administered as an infusion over 1 h or 3 h every 21 days in patients with solid tumours. Eur. J. Cancer 2003, 39, 1842–1851. [Google Scholar] [CrossRef] [PubMed]
- Van Kesteren, C.; Cvitkovic, E.; Taamma, A.; López-Lázaro, L.; Jimeno, J.M.; Guzman, C.; Mathôt, R.A.A.; Schellens, J.H.M.; Misset, J.-L.; Brain, E.; et al. Pharmacokinetics and pharmacodynamics of the novel marine-derived anticancer agent ecteinascidin 743 in a phase I dose-finding study. Clin. Cancer Res. 2000, 6, 4725–4732. [Google Scholar] [PubMed]
- Villalona-Calero, M.A.; Eckhardt, S.G.; Weiss, G.; Hidalgo, M.; Beijnen, J.H.; van Kesteren, C.; Rosing, H.; Campbell, E.; Kraynak, M.; Lopez-Lazaro, L.; et al. A phase I and pharmacokinetic study of ecteinascidin-743 on a daily × 5 schedule in patients with solid malignancies. Clin. Cancer Res. 2002, 8, 75–85. [Google Scholar] [PubMed]
- Schöffski, P.; Dumez, H.; Wolter, P.; Stefan, C.; Wozniak, A.; Jimeno, J.; van Oosterom, A.T. Clinical impact of trabectedin (ecteinascidin-743) in advanced/metastatic soft tissue sarcoma. Expert Opin. Pharmacother. 2008, 9, 1609–1618. [Google Scholar] [CrossRef] [PubMed]
- Blay, J.-Y.; von Mehren, M.; Samuels, B.L.; Fanucchi, M.P.; Ray-Coquard, I.; Buckley, B.; Gilles, L.; Lebedinsky, C.; Elsayed, Y.A.; le Cesne, A. Phase I combination study of trabectedin and doxorubicin in patients with soft-tissue sarcoma. Clin. Cancer Res. 2008, 14, 6656–6662. [Google Scholar] [CrossRef] [PubMed]
- Messersmith, W.; Jimeno, A.; Ettinger, D.; Laheru, D.; Brahmer, J.; Lansey, D.; Khan, Y.; Donehower, R.; Elsayed, Y.; Zannikos, P.; et al. Phase I trial of weekly trabectedin (et-743) and gemcitabine in patients with advanced solid tumors. Cancer Chemother. Pharmacol. 2008, 63, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Sessa, C.; Cresta, S.; Noberasco, C.; Capri, G.; Gallerani, E.; Braud, F.D.; Zucchetti, M.; D’Incalci, M.; Locatelli, A.; Marsoni, S.; et al. Phase I clinical and pharmacokinetic study of trabectedin and cisplatin in solid tumours. Eur. J. Cancer 2009, 45, 2116–2122. [Google Scholar] [CrossRef] [PubMed]
- Sessa, C.; del Conte, G.; Christinat, A.; Cresta, S.; Perotti, A.; Gallerani, E.; Lardelli, P.; Kahatt, C.; Alfaro, V.; Iglesias, J.; et al. Phase I clinical and pharmacokinetic study of trabectedin and cisplatin given every three weeks in patients with advanced solid tumors. Investig. New Drugs 2013, 31, 1236–1243. [Google Scholar] [CrossRef]
- Sessa, C.; Perotti, A.; Noberasco, C.; De Braud, F.; Gallerani, E.; Cresta, S.; Zucchetti, M.; Viganò, L.; Locatelli, A.; Jimeno, J.; et al. Phase I clinical and pharmacokinetic study of trabectedin and doxorubicin in advanced soft tissue sarcoma and breast cancer. Eur. J. Cancer 2009, 45, 1153–1161. [Google Scholar] [CrossRef] [PubMed]
- Von Mehren, M.; Schilder, R.J.; Cheng, J.D.; Temmer, E.; Cardoso, T.M.; Renshaw, F.G.; Bayever, E.; Zannikos, P.; Yuan, Z.; Cohen, R.B. A phase I study of the safety and pharmacokinetics of trabectedin in combination with pegylated liposomal doxorubicin in patients with advanced malignancies. Ann. Oncol. 2008, 19, 1802–1809. [Google Scholar] [CrossRef] [PubMed]
- Yovine, A.; Riofrio, M.; Blay, J.Y.; Brain, E.; Alexandre, J.; Kahatt, C.; Taamma, A.; Jimeno, J.; Martin, C.; Salhi, Y.; et al. Phase II study of ecteinascidin-743 in advanced pretreated soft tissue sarcoma patients. J. Clin. Oncol. 2004, 22, 890–899. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Carbonero, R.; Supko, J.G.; Manola, J.; Seiden, M.V.; Harmon, D.; Ryan, D.P.; Quigley, M.T.; Merriam, P.; Canniff, J.; Goss, G.; et al. Phase II and pharmacokinetic study of ecteinascidin 743 in patients with progressive sarcomas of soft tissues refractory to chemotherapy. J. Clin. Oncol. 2004, 22, 1480–1490. [Google Scholar] [CrossRef] [PubMed]
- Le Cesne, A.; Yovine, A.; Blay, J.-Y.; Delaloge, S.; Maki, R.; Misset, J.-L.; Frontelo, P.; Nieto, A.; Jiao, J.; Demetri, G. A retrospective pooled analysis of trabectedin safety in 1132 patients with solid tumors treated in phase ii clinical trials. Investig. New Drugs 2012, 30, 1193–1202. [Google Scholar] [CrossRef]
- Le Cesne, A.; Blay, J.Y.; Judson, I.; Van Oosterom, A.; Verweij, J.; Radford, J.; Lorigan, P.; Rodenhuis, S.; Ray-Coquard, I.; Bonvalot, S.; et al. Phase ii study of et-743 in advanced soft tissue sarcomas: A european organisation for the research and treatment of cancer (eortc) soft tissue and bone sarcoma group trial. J. Clin. Oncol. 2005, 23, 576–584. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Carbonero, R.; Supko, J.G.; Maki, R.G.; Manola, J.; Ryan, D.P.; Harmon, D.; Puchalski, T.A.; Goss, G.; Seiden, M.V.; Waxman, A.; et al. Ecteinascidin-743 (et-743) for chemotherapy-naive patients with advanced soft tissue sarcomas: Multicenter phase II and pharmacokinetic study. J. Clin. Oncol. 2005, 23, 5484–5492. [Google Scholar] [CrossRef] [PubMed]
- Demetri, G.D.; Chawla, S.P.; von Mehren, M.; Ritch, P.; Baker, L.H.; Blay, J.Y.; Hande, K.R.; Keohan, M.L.; Samuels, B.L.; Schuetze, S.; et al. Efficacy and safety of trabectedin in patients with advanced or metastatic liposarcoma or leiomyosarcoma after failure of prior anthracyclines and ifosfamide: Results of a randomized phase ii study of two different schedules. J. Clin. Oncol. 2009, 27, 4188–4196. [Google Scholar] [CrossRef] [PubMed]
- Gronchi, A.; Bui, B.N.; Bonvalot, S.; Pilotti, S.; Ferrari, S.; Hohenberger, P.; Hohl, R.J.; Demetri, G.D.; le Cesne, A.; Lardelli, P.; et al. Phase II clinical trial of neoadjuvant trabectedin in patients with advanced localized myxoid liposarcoma. Ann. Oncol. 2012, 23, 771–776. [Google Scholar] [CrossRef] [PubMed]
- Samuels, B.L.; Chawla, S.; Patel, S.; von Mehren, M.; Hamm, J.; Kaiser, P.E.; Schuetze, S.; Li, J.; Aymes, A.; Demetri, G.D. Clinical outcomes and safety with trabectedin therapy in patients with advanced soft tissue sarcomas following failure of prior chemotherapy: Results of a worldwide expanded access program study. Ann. Oncol. 2013, 24, 1703–1709. [Google Scholar] [CrossRef] [PubMed]
- Blay, J.-Y.; Leahy, M.G.; Nguyen, B.B.; Patel, S.R.; Hohenberger, P.; Santoro, A.; Staddon, A.P.; Penel, N.; Piperno-Neumann, S.; Hendifar, A.; et al. Randomised phase III trial of trabectedin versus doxorubicin-based chemotherapy as first-line therapy in translocation-related sarcomas. Eur. J. Cancer 2014, 50, 1137–1147. [Google Scholar] [CrossRef] [PubMed]
- Grosso, F.; Jones, R.L.; Demetri, G.D.; Judson, I.R.; Blay, J.-Y.; le Cesne, A.; Sanfilippo, R.; Casieri, P.; Collini, P.; Dileo, P.; et al. Efficacy of trabectedin (ecteinascidin-743) in advanced pretreated myxoid liposarcomas: A retrospective study. Lancet Oncol. 2007, 8, 595–602. [Google Scholar] [CrossRef] [PubMed]
- Cesne, A.L.; Cresta, S.; Maki, R.G.; Blay, J.Y.; Verweij, J.; Poveda, A.; Casali, P.G.; Balaña, C.; Schöffski, P.; Grosso, F.; et al. A retrospective analysis of antitumour activity with trabectedin in translocation-related sarcomas. Eur. J. Cancer 2012, 48, 3036–3044. [Google Scholar] [CrossRef] [PubMed]
- Sanfilippo, R.; Grosso, F.; Jones, R.L.; Banerjee, S.; Pilotti, S.; D’Incalci, M.; Tos, A.P.D.; Raspagliesi, F.; Judson, I.; Casali, P.G. Trabectedin in advanced uterine leiomyosarcomas: A retrospective case series analysis from two reference centers. Gynecol. Oncol. 2011, 123, 553–556. [Google Scholar] [CrossRef] [PubMed]
- Monk, B.J.; Blessing, J.A.; Street, D.G.; Muller, C.Y.; Burke, J.J.; Hensley, M.L. A phase II evaluation of trabectedin in the treatment of advanced, persistent, or recurrent uterine leiomyosarcoma: A gynecologic oncology group study. Gynecol. Oncol. 2012, 124, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Cesne, A.L.; Judson, I.; Maki, R.; Grosso, F.; Schuetze, S.; Mehren, M.V.; Chawla, S.P.; Demetri, G.D.; Nieto, A.; Tanovic, A.; et al. Trabectedin is a feasible treatment for soft tissue sarcoma patients regardless of patient age: A retrospective pooled analysis of five phase ii trials. Br. J. Cancer 2013, 109, 1717–1724. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Petek, B.J.; Loggers, E.T.; Pollack, S.M.; Jones, R.L. Trabectedin in Soft Tissue Sarcomas. Mar. Drugs 2015, 13, 974-983. https://doi.org/10.3390/md13020974
AMA Style
Petek BJ, Loggers ET, Pollack SM, Jones RL. Trabectedin in Soft Tissue Sarcomas. Marine Drugs. 2015; 13(2):974-983. https://doi.org/10.3390/md13020974
Chicago/Turabian StylePetek, Bradley J., Elizabeth T. Loggers, Seth M. Pollack, and Robin L. Jones. 2015. "Trabectedin in Soft Tissue Sarcomas" Marine Drugs 13, no. 2: 974-983. https://doi.org/10.3390/md13020974