Comments on the Eslicarbazepine Acetate Section of the Article ‘Therapeutic Drug Monitoring of the Newer Anti-Epilepsy Medications’

Abstract
:
{kind=link}
{kind=link}
{kind=link}
The Rationale behind this Communication
The Review Provides Useful Information Related to Anti-Epileptic Drugs (AEDs)
The Referred Chapter Provides Additional Room for Discussion on the Particular Characteristics of Eslicarbazepine Acetate
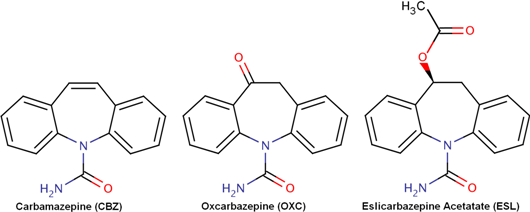
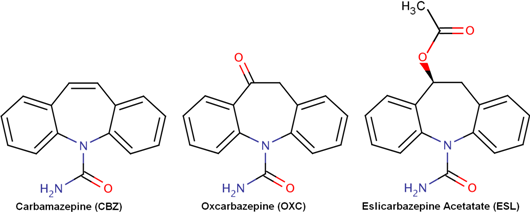
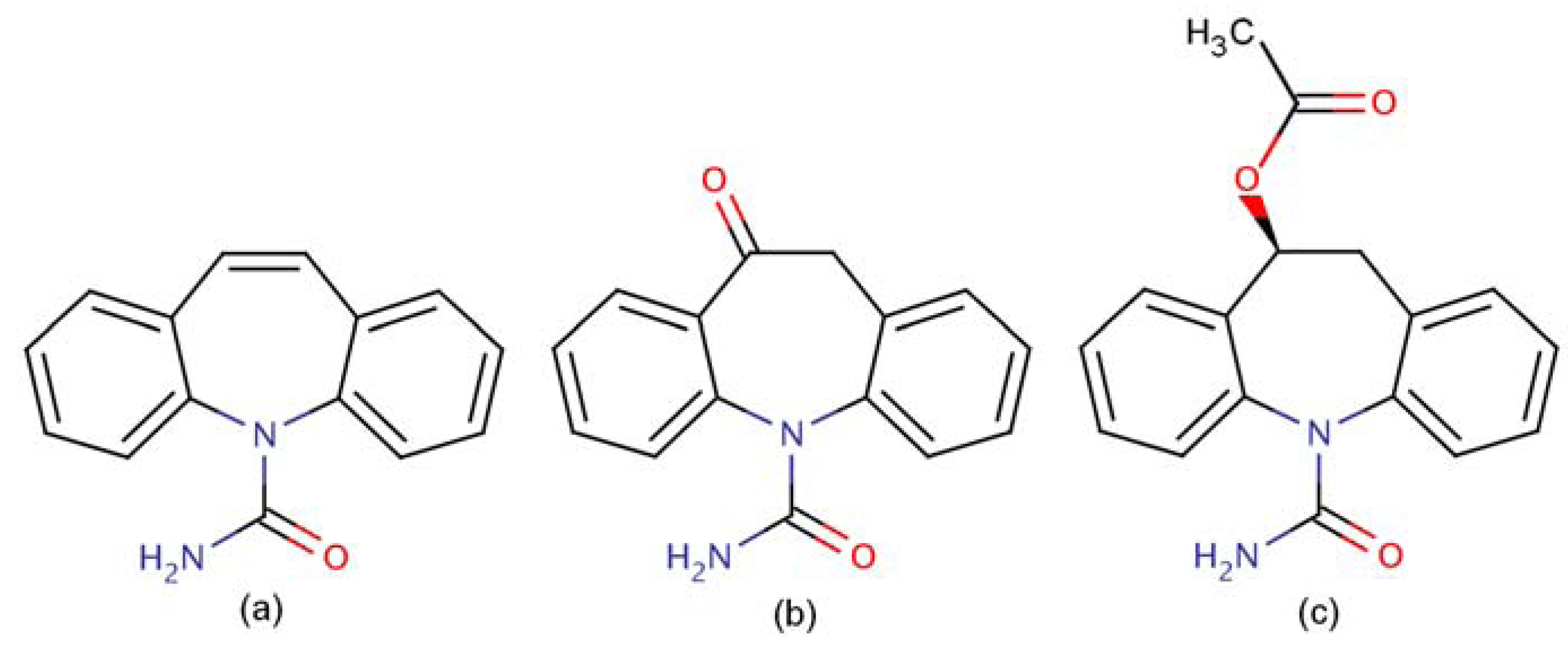
The Chemical Structure of Each Dibenzazepine Is Unique and Different, Substantiating the Differences in Their Plasma Kinetics and Clinical Effects
Eslicarbazepine Acetate and Its Main Active Metabolites Differ from CBZ by Not Auto-inducing Its Metabolism
Some Critical Pharmacokinetic and Safety Related Information Seem To Be Incorrect Despite the Accuracy of the Text
The Concerns on Interpretation of TDM Was Based on a Misinterpretation of the Different Pharmacokinetic Profile of ESL Compared to OXC
The Model Recommended To Detect ESL and Its Metabolites Is a More Complicated Quadrupole HPLC-MS Method
Summary
References
- Krasowski, M.D. Therapeutic drug monitoring of the newer anti-epilepsy medications. Pharmaceuticals (Basel) 2010, 3, 1909–1935. [Google Scholar]
- Almeida, L.; Soares-de-Silva, P. Eslicarbazepine acetate (BIA 2-093). Neurotherapeutics 2007, 4, 88–96. [Google Scholar]
- Zebinix® (Eslicarbazepine acetate) Summary of Product Characteristics. European Medicines Agency (EMA). 01-10-2010. Available online: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000988/WC500047225.pdf accessed on 17 December 2010.
- Almeida, L.; Bialer, M.; Soares-da-Silva, P. Eslicarbazepine acetate. In The Treatment of Epilepsy, 3rd; Shorvon, S., Perucca, E., Engel, J., Eds.; Wiley-Blackwell: Oxford, UK, 2009; pp. 485–498. [Google Scholar]
- Almeida, L.; Potgieter, J.H.; Maia, J.; Potgieter, M.A.; Mota, F.; Soares-da-Silva, P. Pharmacokinetics of eslicarbazepine acetate in patients with moderate hepatic impairment. Eur. J. Clin. Pharmacol. 2008, 64, 267–273. [Google Scholar]
- Keränen, T.; Jolkklonen, J.; Jensen, P.K.; Menge, G.P.; Andersson, P. Absence of interaction between oxcarbazepine and erythromycine. Acta Neurol. Scand. 1992, 86, 120–123. [Google Scholar]
- Alves, G.; Figueiredo, I.; Castel-Branco, M.; Loureiro, A.; Falcão, A.; Caramona, M. Simultaneous and enantioselective liquid chromatographic determination of eslicarbazepine acetate, S-licarbazepine, R-licarbazepine and oxcarbazepine in mouse tissue samples using ultraviolet detection. Biomed. Chromatogr. 2007, 21, 1127–1134. [Google Scholar]
- Almeida, L.; Soares-de-Silva, P. Safety, tolerability, and pharmacokinetic profile of BIA 2-093, a novel putative antiepileptic, in a rising multiple-dose study in young healthy humans. J. Clin. Pharmacol. 2004, 44, 906–918. [Google Scholar]
- Almeida, L.; Falcão, A.; Maia, J.; Mazur, D.; Gellert, M.; Soares-da-Silva, P. Single-dose and steady-state pharmacokinetics of eslicarbazepine acetate (BIA 2-093) in healthy elderly and young subjects. J. Clin. Pharmacol. 2005, 45, 1062–1066. [Google Scholar]
- Falcão, A.; Maia, J.; Almeida, L.; Mazur, D.; Gellert, M.; Soares-da-Silva, P. Effect of gender on the pharmacokinetics of eslicarbazepine acetate (BIA 2-093), a new voltage-gated sodium channel blocker. Biopharm. Drug Dispos. 2007, 28, 249–256. [Google Scholar]
© 2010 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Öztiryaki, A.H.; Soares-da-Silva, P. Comments on the Eslicarbazepine Acetate Section of the Article ‘Therapeutic Drug Monitoring of the Newer Anti-Epilepsy Medications’. Pharmaceuticals 2010, 3, 3629-3632. https://doi.org/10.3390/ph3123629
Öztiryaki AH, Soares-da-Silva P. Comments on the Eslicarbazepine Acetate Section of the Article ‘Therapeutic Drug Monitoring of the Newer Anti-Epilepsy Medications’. Pharmaceuticals. 2010; 3(12):3629-3632. https://doi.org/10.3390/ph3123629
Chicago/Turabian StyleÖztiryaki, Ahmet H., and Patricio Soares-da-Silva. 2010. "Comments on the Eslicarbazepine Acetate Section of the Article ‘Therapeutic Drug Monitoring of the Newer Anti-Epilepsy Medications’" Pharmaceuticals 3, no. 12: 3629-3632. https://doi.org/10.3390/ph3123629