
Image-Guided Laparoscopic Surgical Tool (IGLaST) Based on the Optical Frequency Domain Imaging (OFDI) to Prevent Bleeding

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
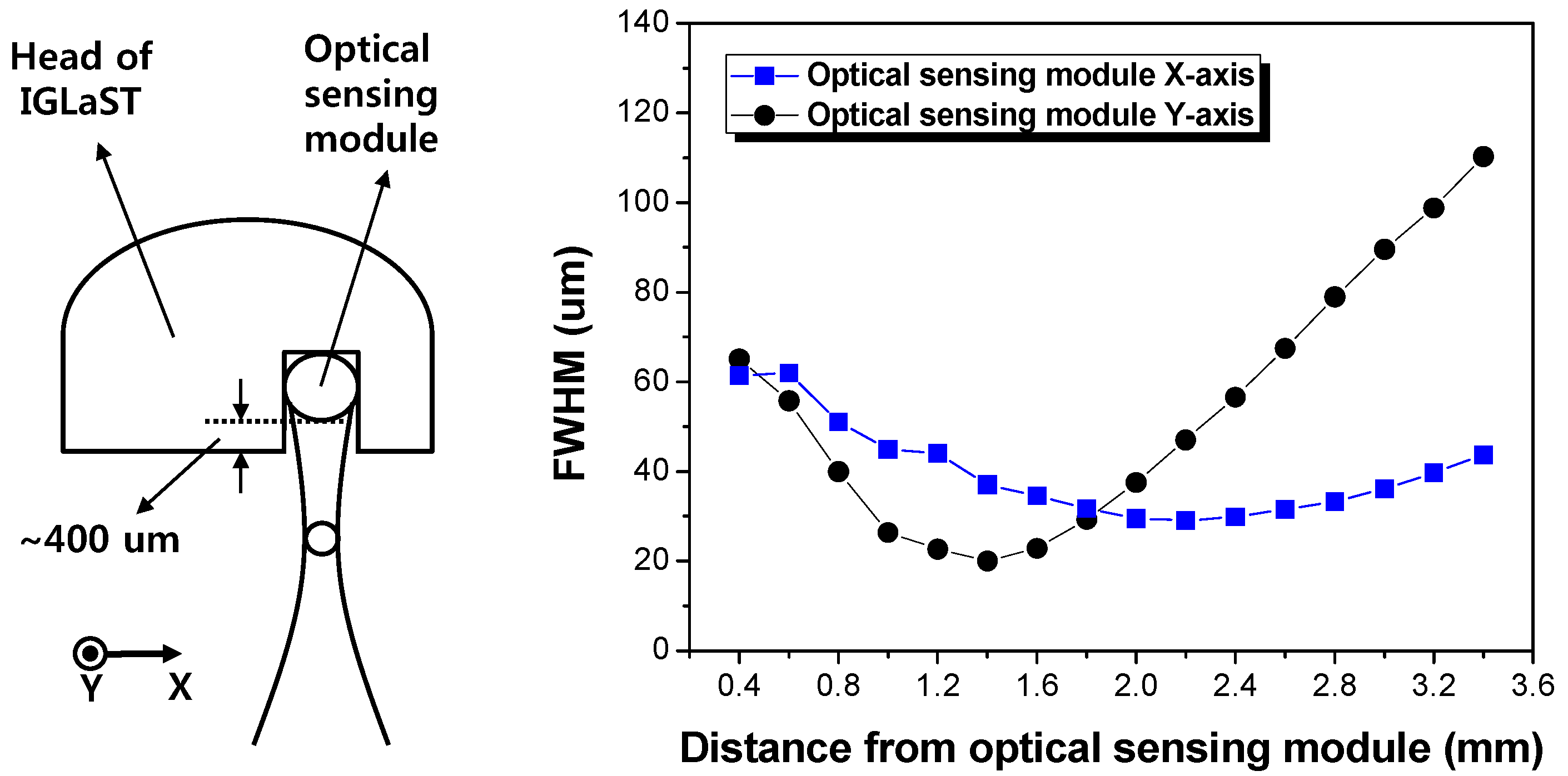
2.1. Design of IGLaST
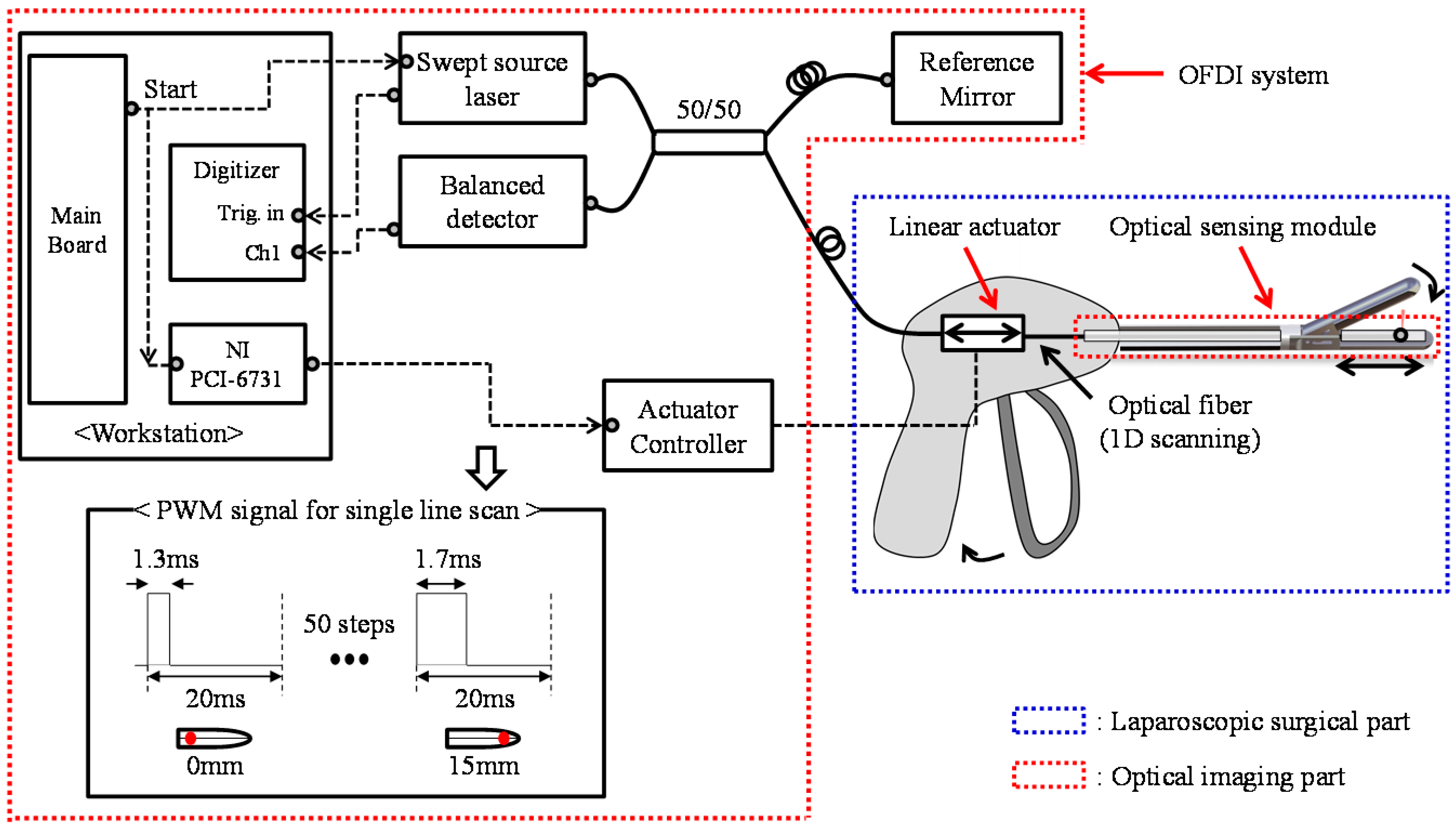
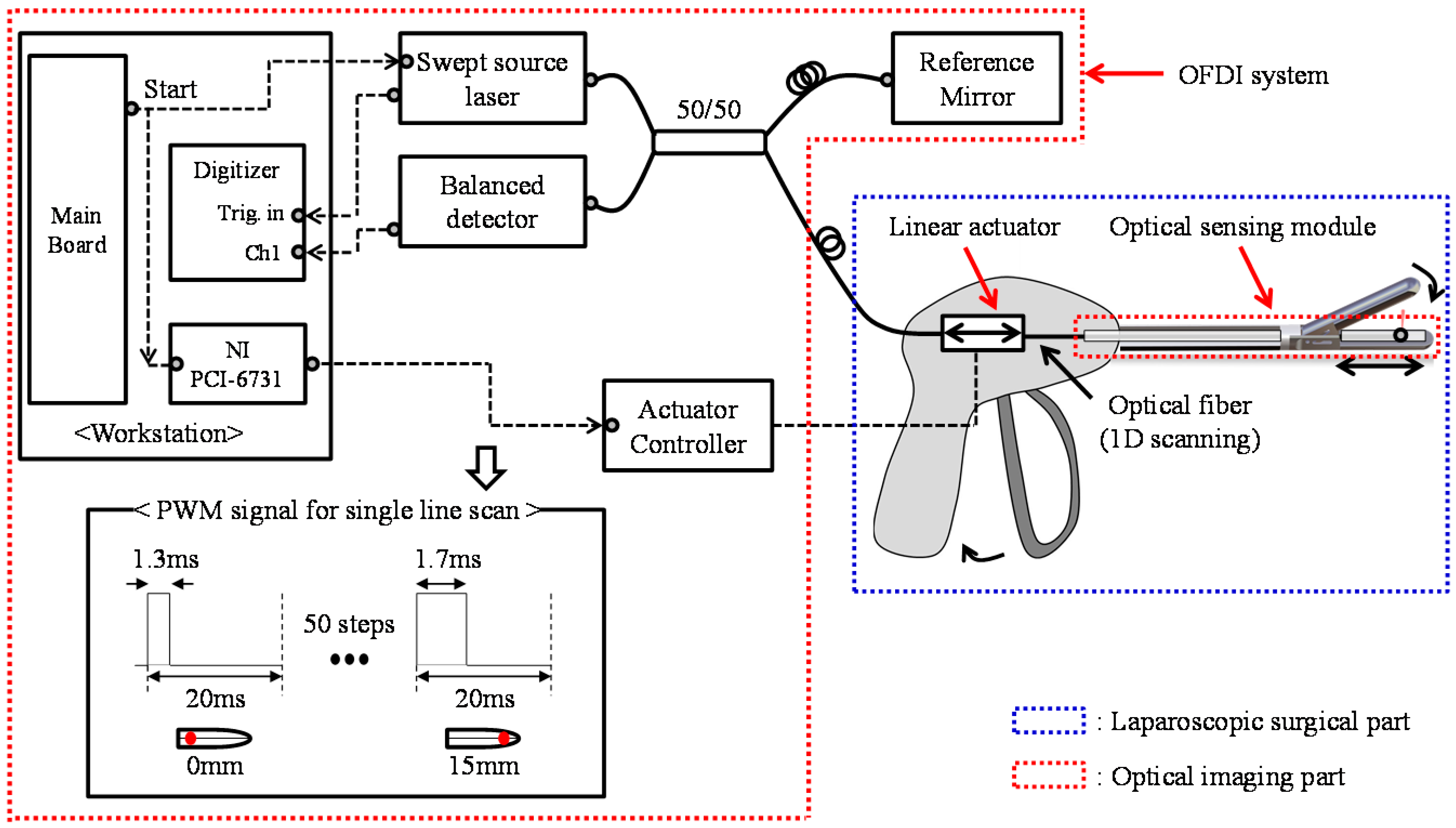
2.2. OFDI for IGLaST
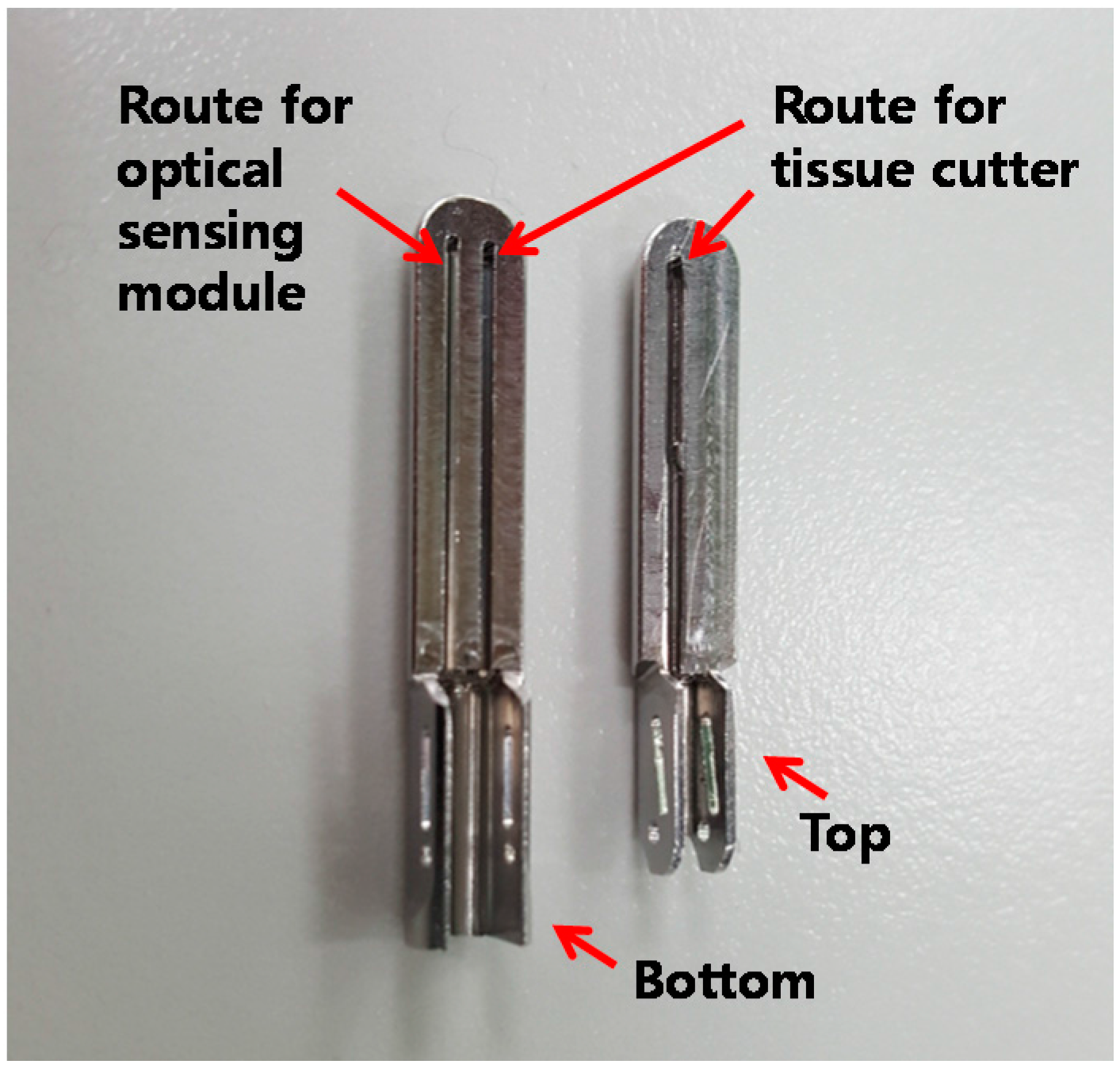
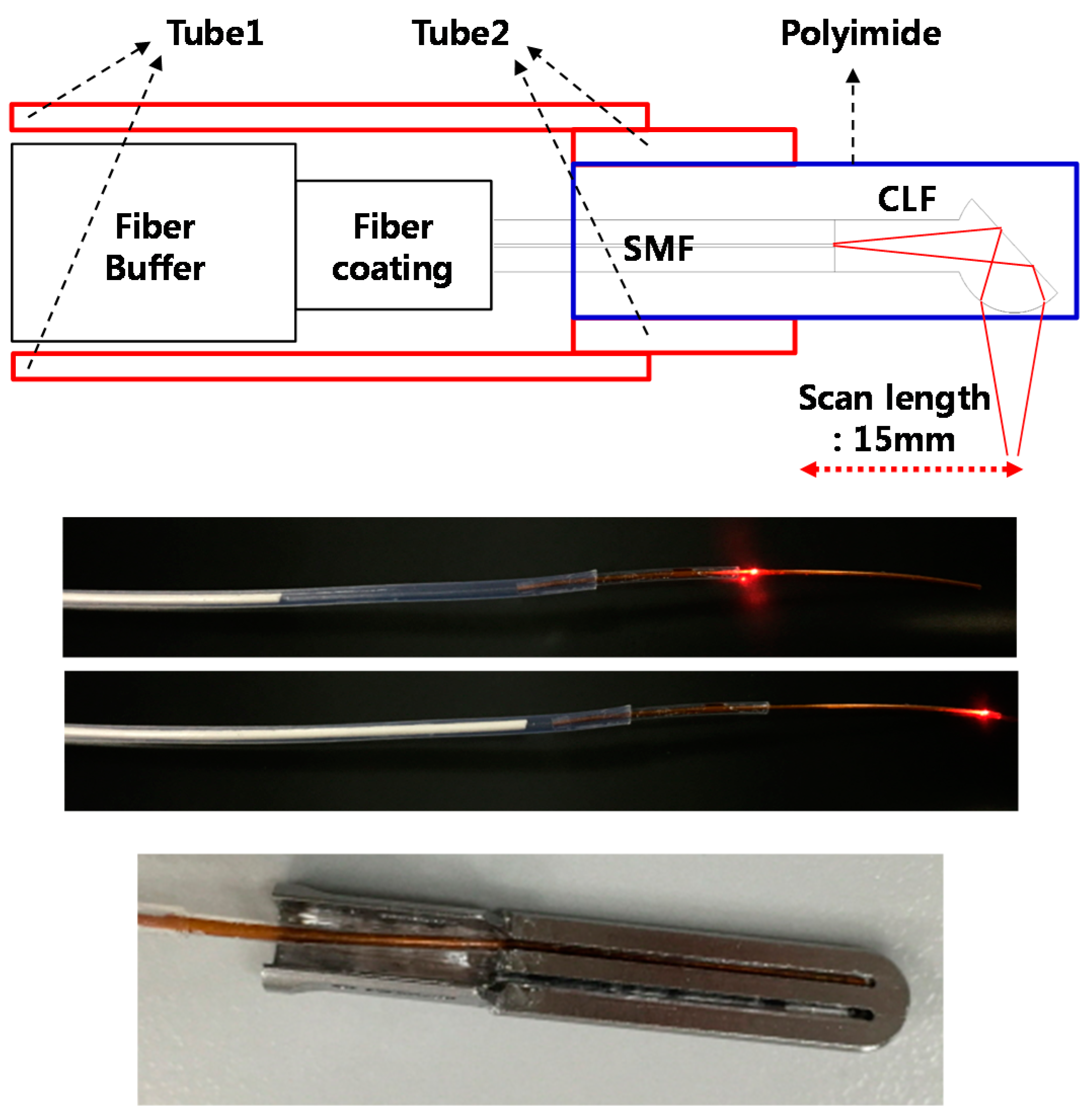
2.3. Realization of IGLaST
3. Results
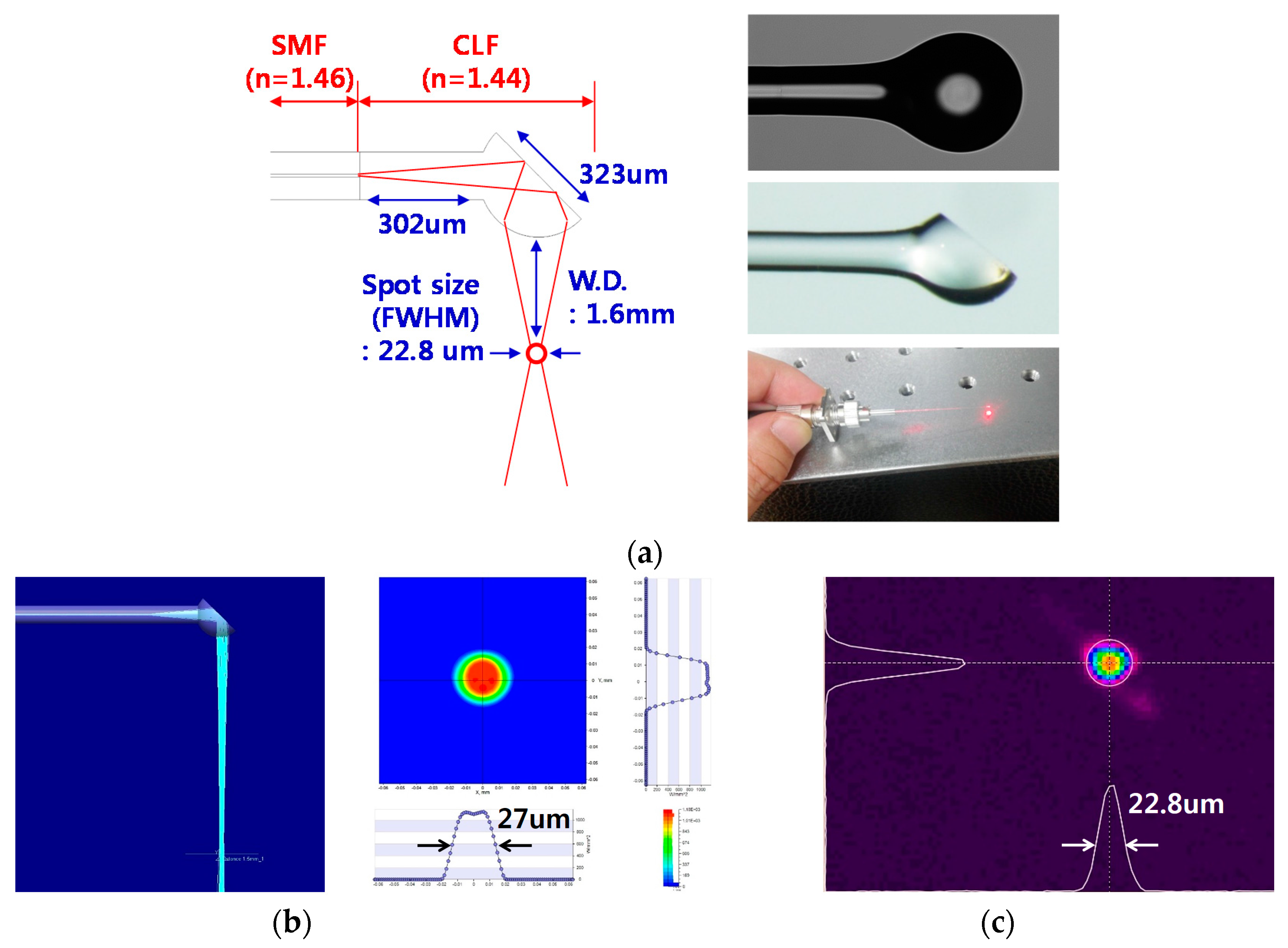
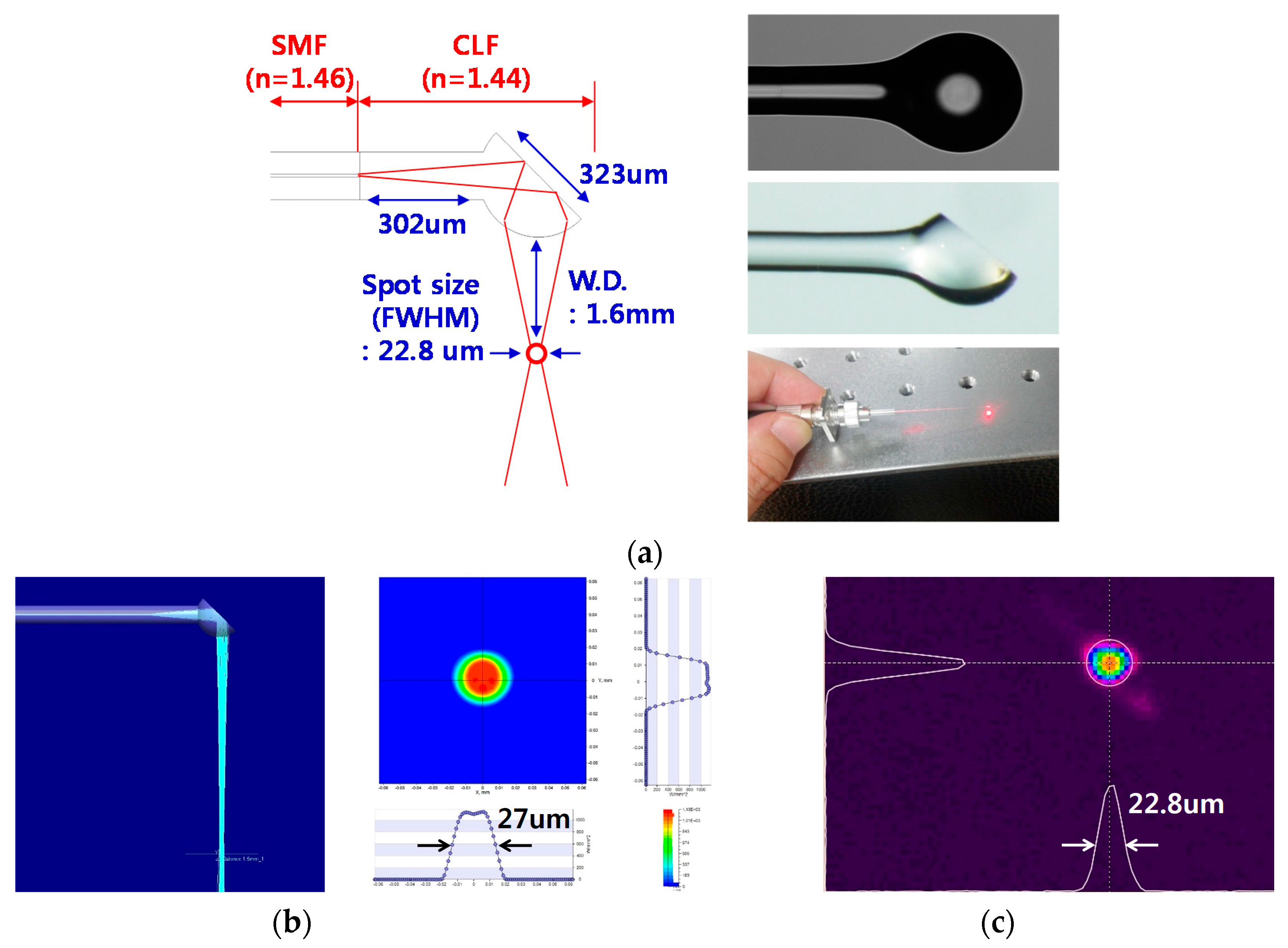
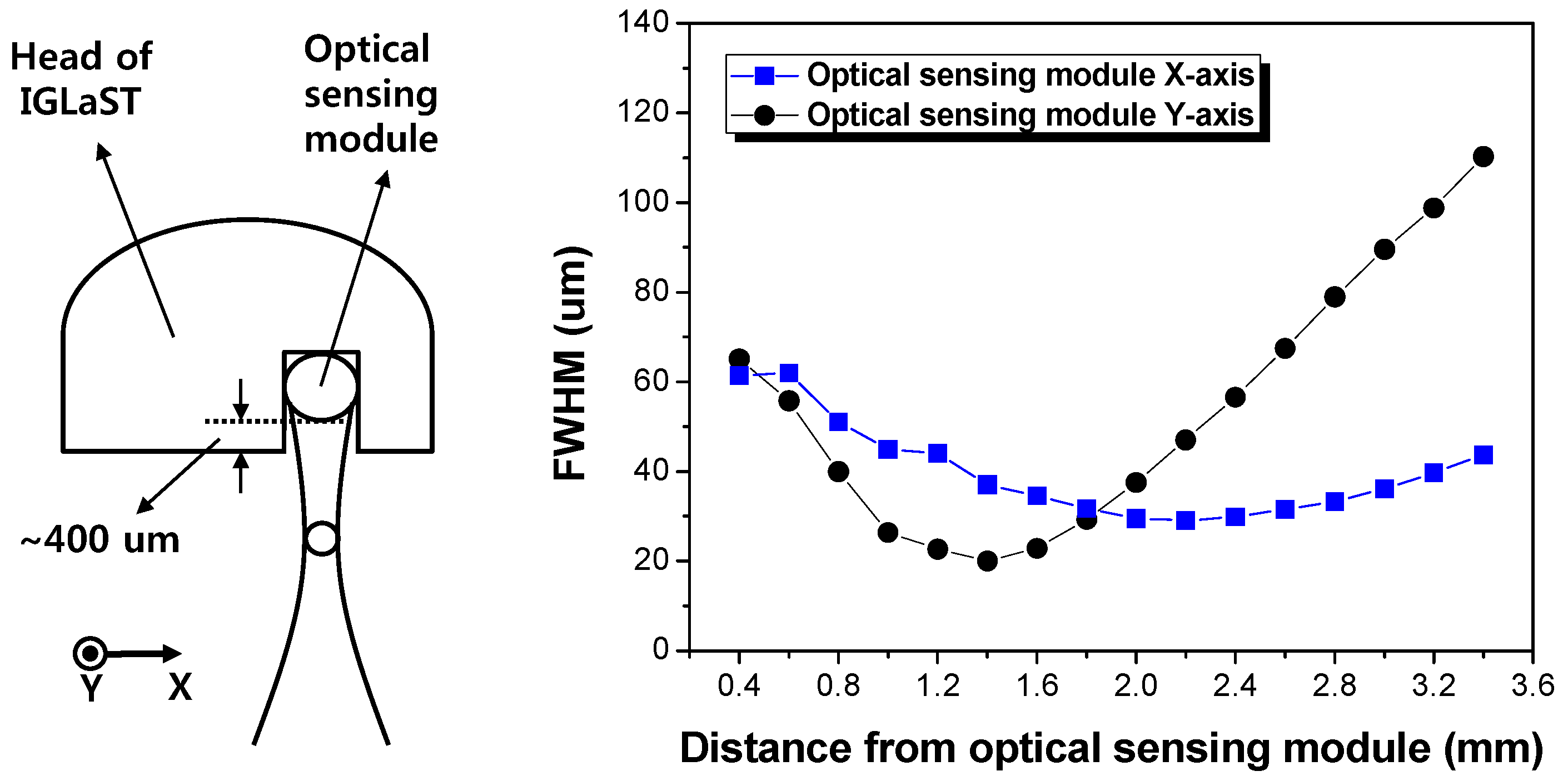
3.1. Optical Properties
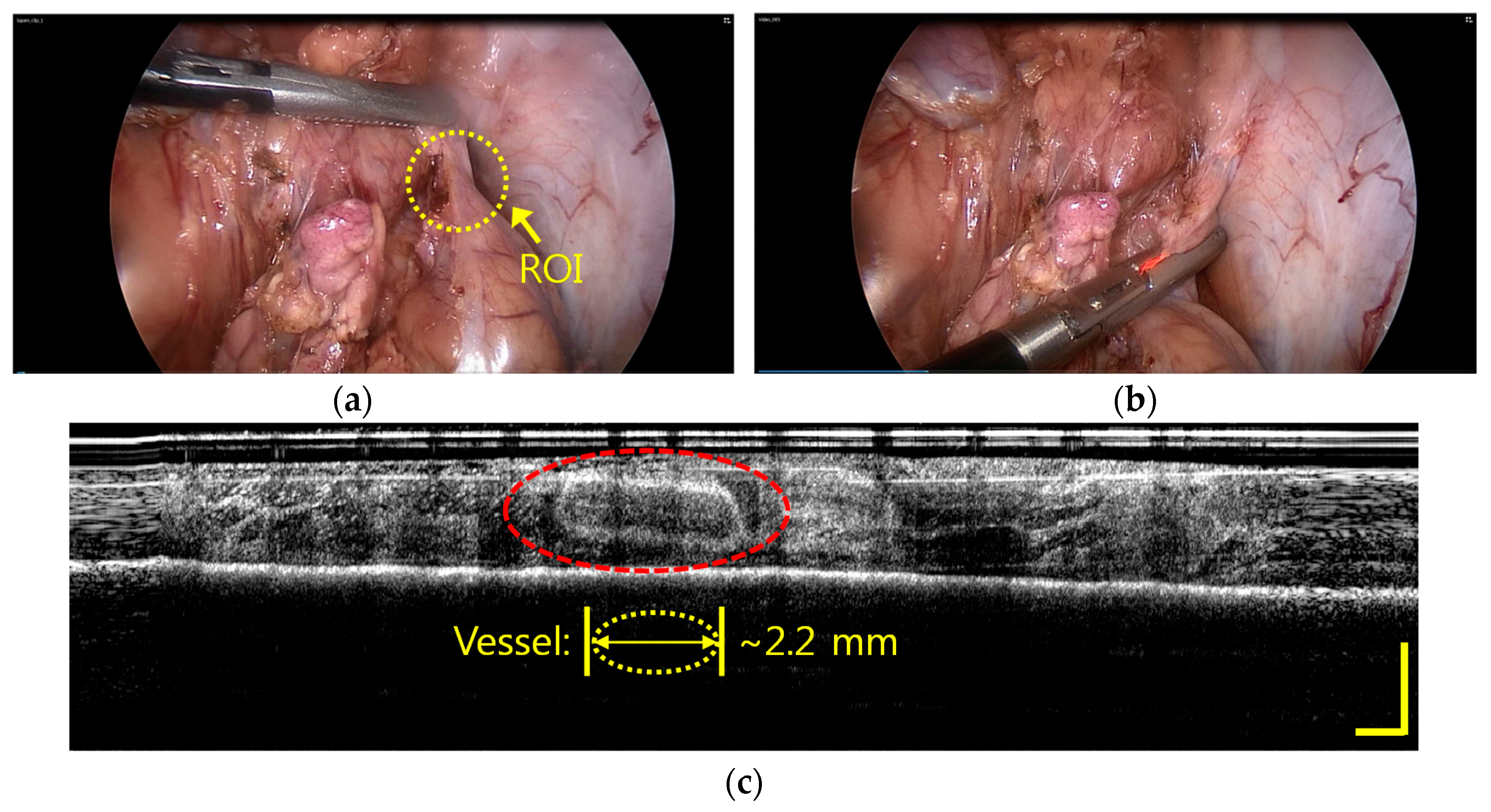
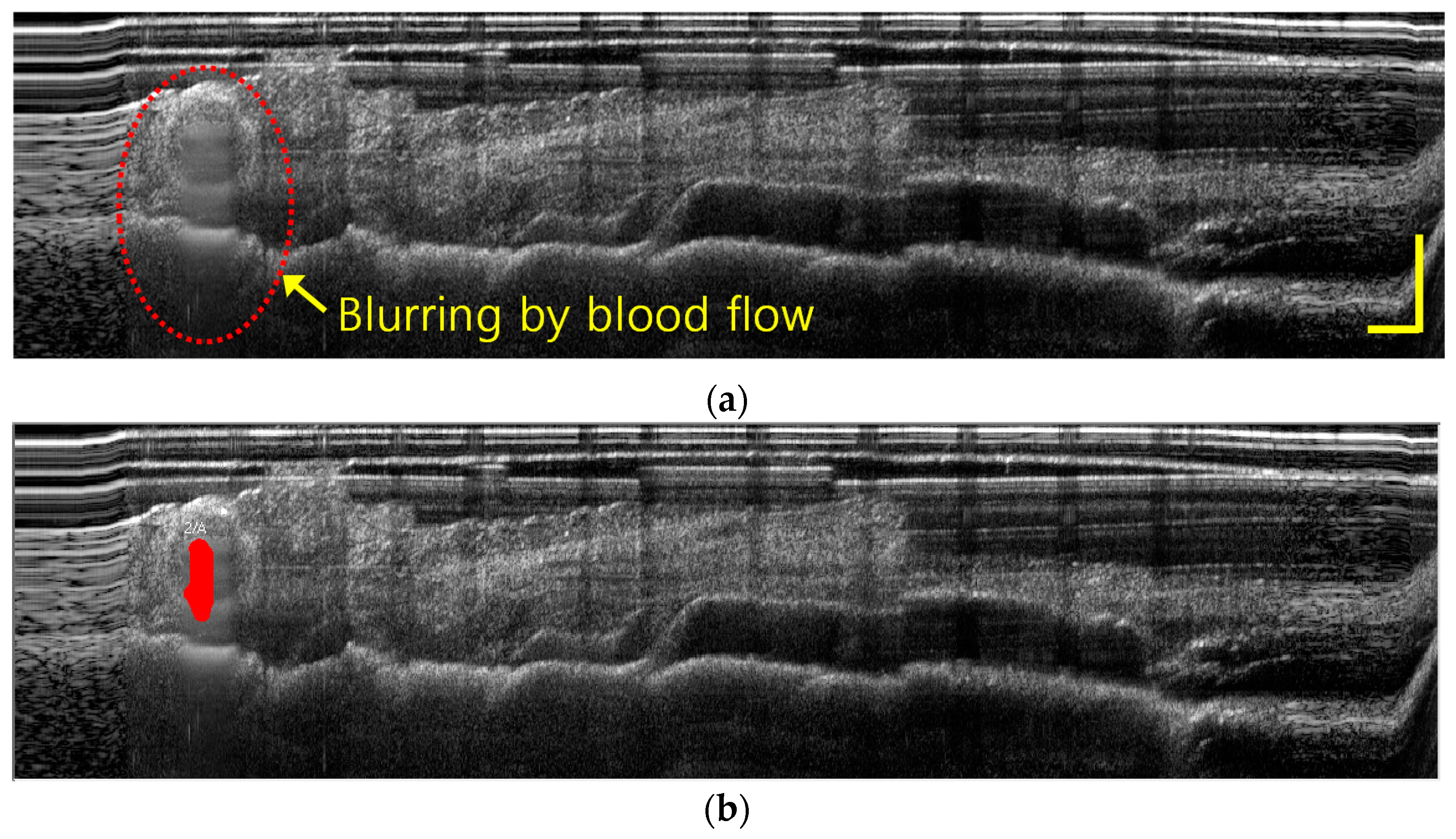
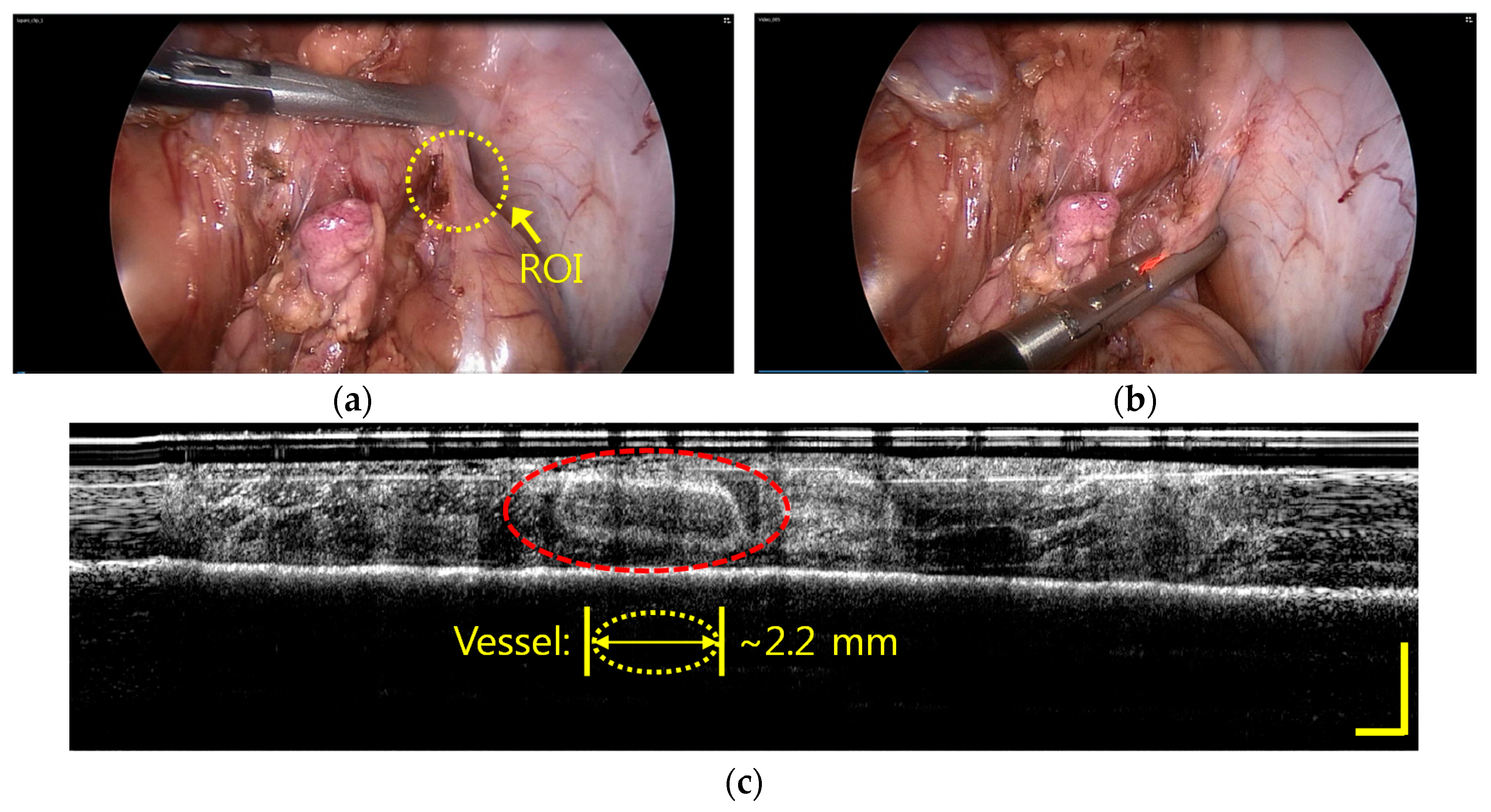
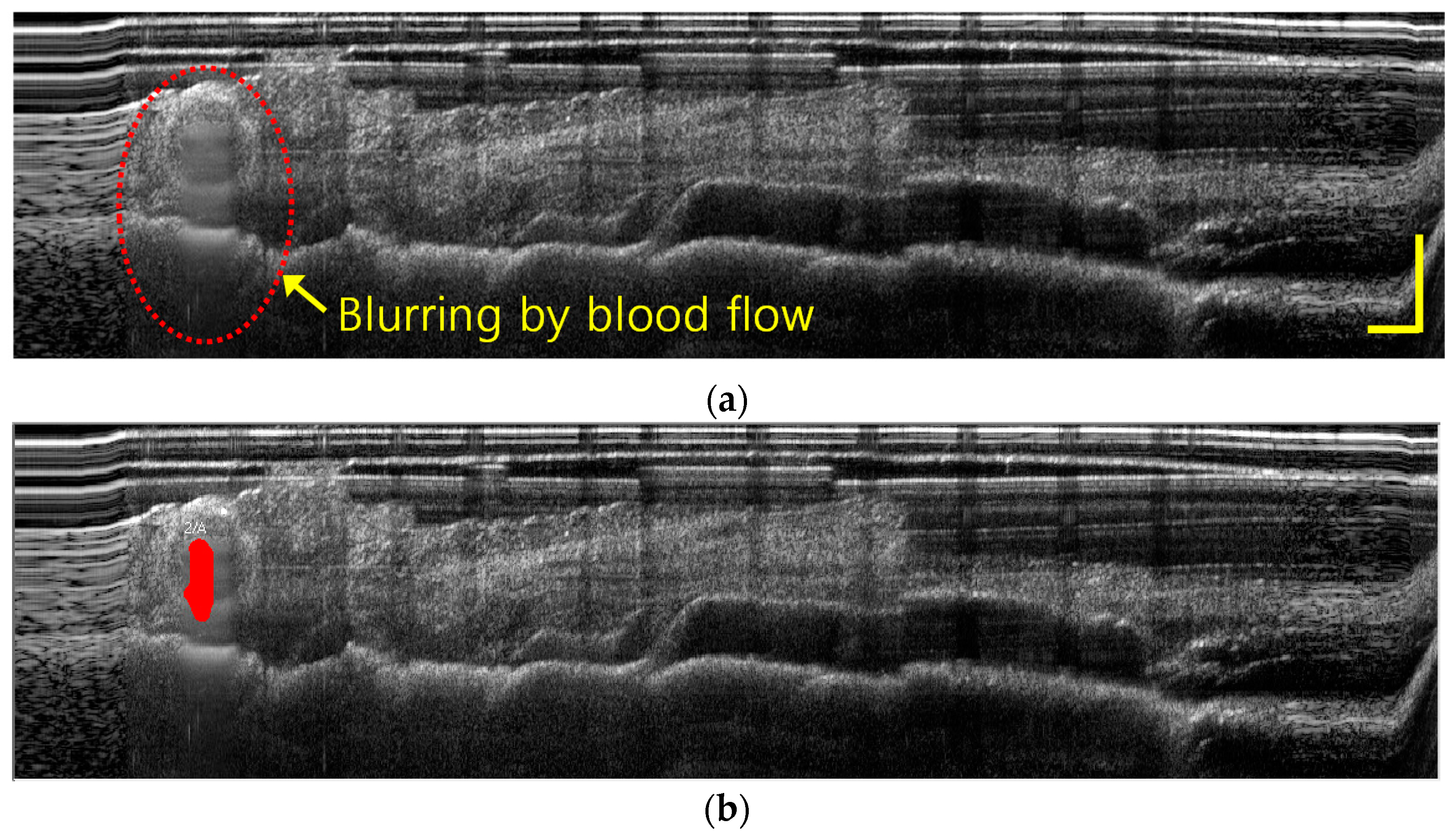
3.2. Imaging of a Vessel Inside the Fatty Tissues of a Porcine Model with IGLaST
4. Discussion and Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Swanstrom, L.L.; Soper, N.J. Mastery of Endoscopic and Laparoscopic Surgery; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- Der Putten, E.P.W.; Goossens, R.H.M.; Jakimowicz, J.J.; Dankelman, J. Haptics in minimally invasive surgery—A review. Minim. Invasive Ther. Alied Technol. 2008, 17, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, A.G.; McClure, N.; McGuigan, J.; Ritchie, K.; Sheehy, N.P. An ergonomic analysis of the fulcrum effect in the acquisition of endoscopic skills. Endoscopy 1998, 30, 617–620. [Google Scholar] [CrossRef] [PubMed]
- Fercher, A.F.; Drexler, W.; Hitzenberger, C.K.; Lasser, T. Optical coherence tomography—Principles and applications. Rep. Prog. Phys. 2003, 66, 239–303. [Google Scholar] [CrossRef]
- Zysk, A.M.; Nguyen, F.T.; Oldenburg, A.L.; Marks, D.L.; Boppart, S.A. Optical coherence tomography: A review of clinical development from bench to bedside. J. Biomed. Opt. 2007, 12, 051403. [Google Scholar] [CrossRef] [PubMed]
- Costa, R.A.; Skaf, M.; Melo, L.A.S.; Calucci, D.; Cardillo, J.A.; Castro, J.C.; Huang, D.; Wojtkowski, M. Retinal assessment using optical coherence tomography. Prog. Retin. Eye Res. 2006, 25, 325–353. [Google Scholar] [CrossRef] [PubMed]
- Dogra, M.R.; Gupta, A.; Gupta, V. Atlas of Optical Coherence Tomography of Macular Diseases; Taylor & Francis: Boca Raton, FL, USA, 2004. [Google Scholar]
- Brezinski, M.E.; Tearney, G.J.; Bouma, B.E.; Izatt, J.A.; Hee, M.R.; Swanson, E.A.; Southern, J.F.; Fujimoto, J.G. Optical coherence tomography for optical biopsy: Properties and demonstration of vascular pathology. Circulation 1996, 93, 1206–1213. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.S.; Jang, S.-J.; Kim, K.; Dan-Chin-Yu, A.V.; Shishkov, M.; Bouma, B.E.; Oh, W.-Y. High-frame-rate intravascular optical frequency-domain imaging in vivo. Biomed. Opt. Exp. 2014, 5, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, J.G.; Pitris, C.; Boppart, S.A.; Brezinski, M.E. Optical coherence tomography: An emerging technology for biomedical imaging and optical biopsy. Neoplasia 2000, 2, 9–25. [Google Scholar] [CrossRef] [PubMed]
- Cogliati, A.; Canavesi, C.; Hayes, A.; Tankam, P.; Duma, V.-F.; Santhanam, A.; Thompson, K.P.; Rolland, J.P. MEMS—Based handheld scanning probe with pre-shaped input signals for distortion-free images in Gabor-domain optical coherence microscopy. Opt. Express 2016, 24, 13365–13374. [Google Scholar] [CrossRef] [PubMed]
- Testoni, P.A.; Mangiavillano, B. Optical coherence tomography in detection of dysplasia and cancer of the gastrointestinal tract and bilio-pancreatic ductal system. World J. Gastroenterol. 2008, 14, 6444–6452. [Google Scholar] [CrossRef] [PubMed]
- Suter, M.J.; Vakoc, B.J.; Yachimski, P.S.; Shishkov, M.; Lauwers, G.Y.; Mino-Kenudson, M.; Bouma, B.E.; Nishioka, N.S.; Tearney, G.J. Comprehensive microscopy of the esophagus in human patients with optical frequency domain imaging. Gastrointest. Endosc. 2008, 68, 745–753. [Google Scholar] [CrossRef] [PubMed]
- Boppart, S.A.; Goodman, A.; Libus, J.; Pitris, C.; Jesser, C.A.; Brezinski, M.E.; Fusimoto, J.G. High resolution imaging of endometriosis and ovarian carcinoma with optical coherence tomography: Feasibility for laparoscopic-based imaging. Br. J. Obstet. Gynaecol. 1999, 106, 1071–1077. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.B.; Chae, Y.G.; Ahn, Y.C.; Moon, S.B. Ultra-thin and flexible endoscopy probe for optical coherence tomography based on stepwise transitional core fiber. Biomed. Opt. Express 2015, 6, 1782–1796. [Google Scholar] [CrossRef] [PubMed]
- Dougherty, E.R.; Lotufo, R.A. Hands-on Morphological Image Processing; SPIE: Bellingham, WA, USA, 2003. [Google Scholar]
- Rollins, A.M.; Yazdanfar, S.; Barton, J.K.; Izatt, J.A. Real-time in vivo color Doppler optical coherence tomography. J. Biomed. Opt. 2002, 7, 123–129. [Google Scholar] [CrossRef] [PubMed]
- De Carlo, T.E.; Romano, A.; Waheed, N.K.; Duker, J.S. A review of optical coherence tomography angiography (OCTA). Int. J. Retin. Vitr. 2015, 1. [Google Scholar] [CrossRef] [PubMed]
- Choi, W.J.; Li, Y.D.; Qin, W.; Wang, R.K. Cerebral capillary velocimetry based on temporal OCT speckle contrast. Biomed. Opt. Express 2016, 7, 4859–4873. [Google Scholar] [CrossRef] [PubMed]


© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, B.J.; Lee, S.R.; Bang, H.J.; Kim, B.Y.; Park, J.H.; Kim, D.G.; Park, S.S.; Won, Y.J. Image-Guided Laparoscopic Surgical Tool (IGLaST) Based on the Optical Frequency Domain Imaging (OFDI) to Prevent Bleeding. Sensors 2017, 17, 919. https://doi.org/10.3390/s17040919
Park BJ, Lee SR, Bang HJ, Kim BY, Park JH, Kim DG, Park SS, Won YJ. Image-Guided Laparoscopic Surgical Tool (IGLaST) Based on the Optical Frequency Domain Imaging (OFDI) to Prevent Bleeding. Sensors. 2017; 17(4):919. https://doi.org/10.3390/s17040919
Chicago/Turabian StylePark, Byung Jun, Seung Rag Lee, Hyun Jin Bang, Byung Yeon Kim, Jeong Hun Park, Dong Guk Kim, Sung Soo Park, and Young Jae Won. 2017. "Image-Guided Laparoscopic Surgical Tool (IGLaST) Based on the Optical Frequency Domain Imaging (OFDI) to Prevent Bleeding" Sensors 17, no. 4: 919. https://doi.org/10.3390/s17040919