Noise Maps for Quantitative and Clinical Severity Towards Long-Term ECG Monitoring

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
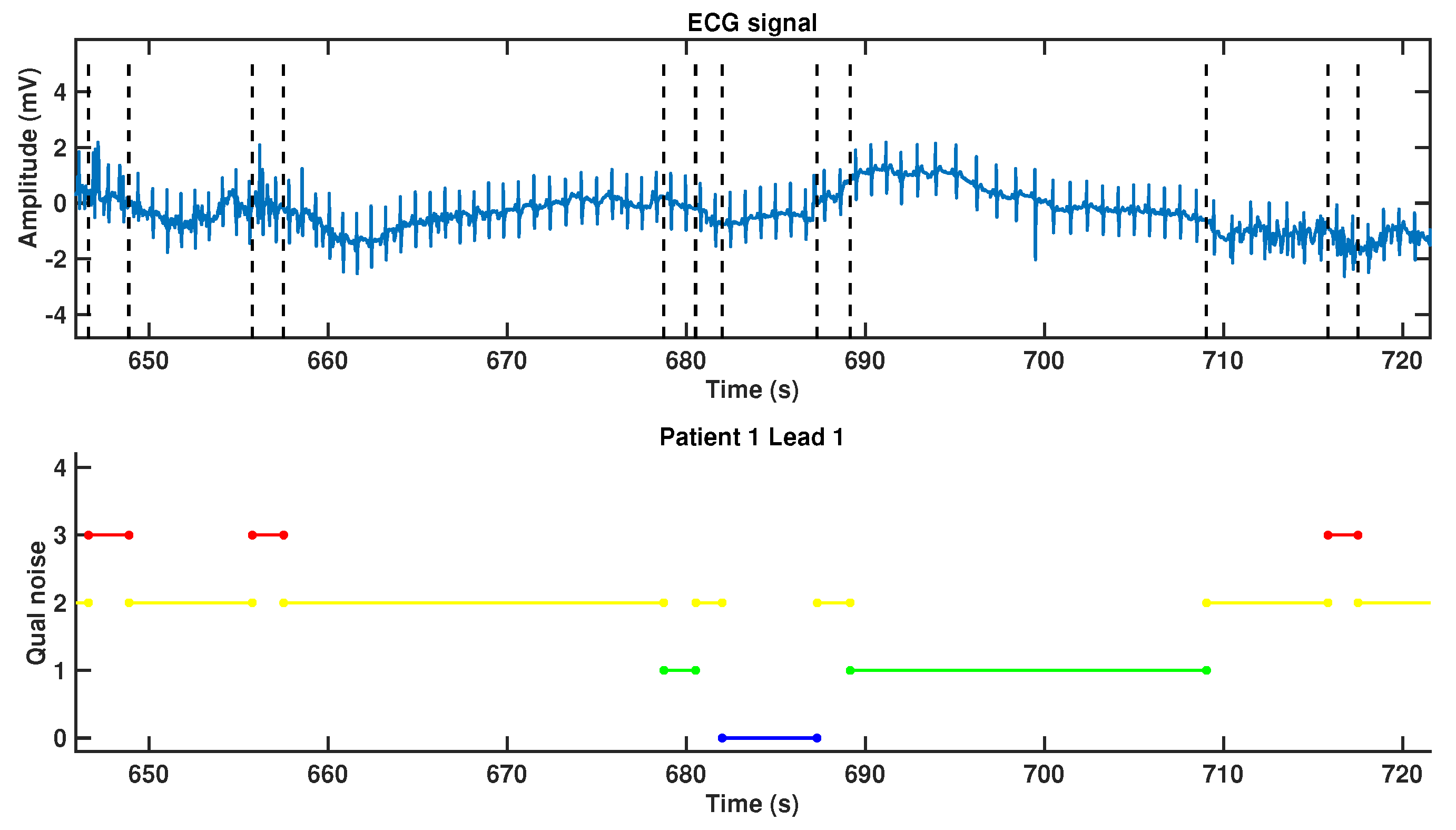
2.2. Noise Clinical Severity
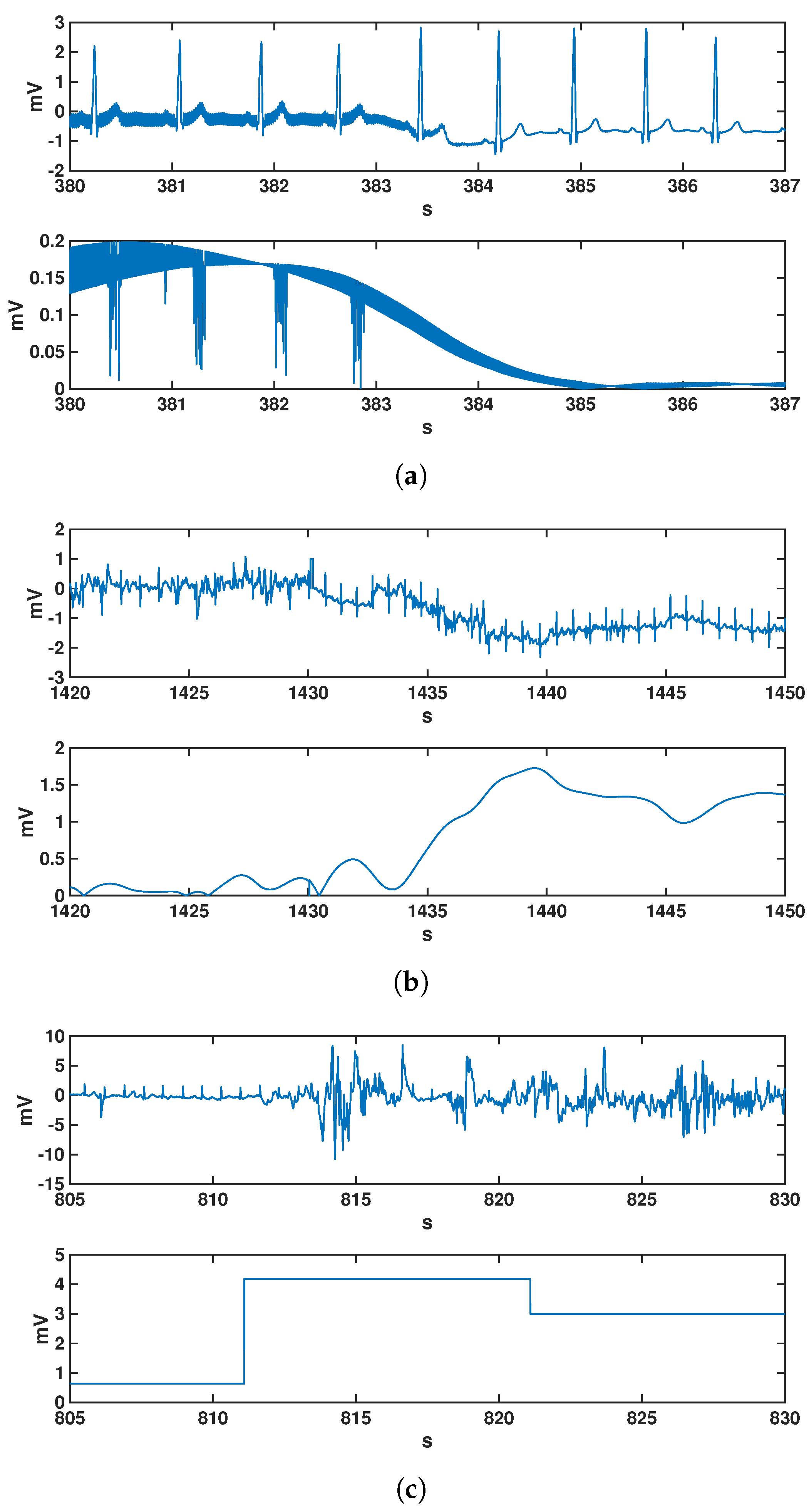
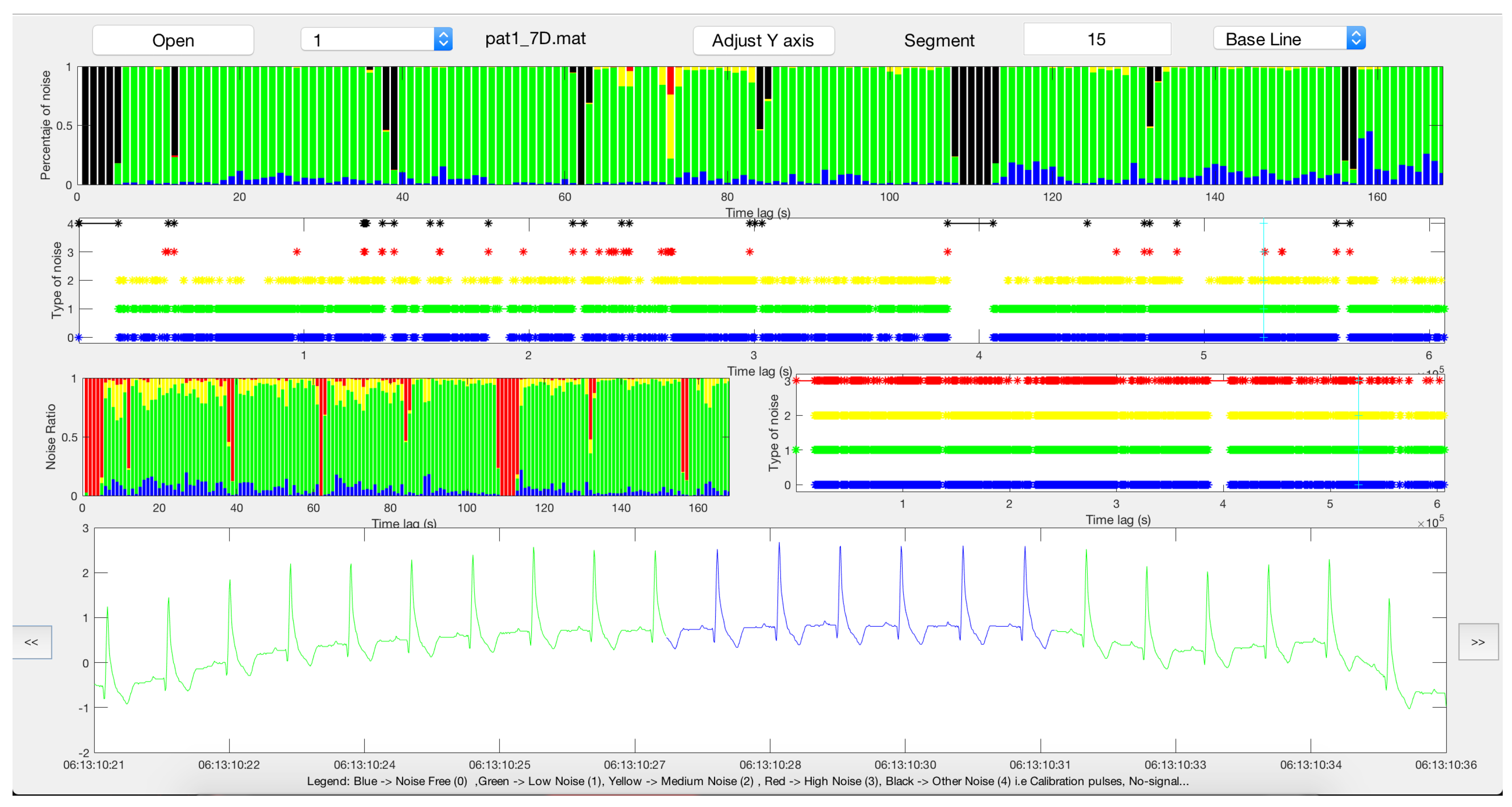
- Noise-free (type 0): segment without noise.
- Low noise (type 1): some noise present in the segment, but P and T waves (corresponding to atrial deporalization and ventricular repolarization, respectively) and the QRS complexes are readable and their morphology can be identified.
- Moderate-noise (type 2): noisy segment in which only the QRS complexes are reliably identified, in at least three consecutive beats.
- Hard-noise (type 3): noisy segment with hardly recognizable or unrecognizable QRS complexes.
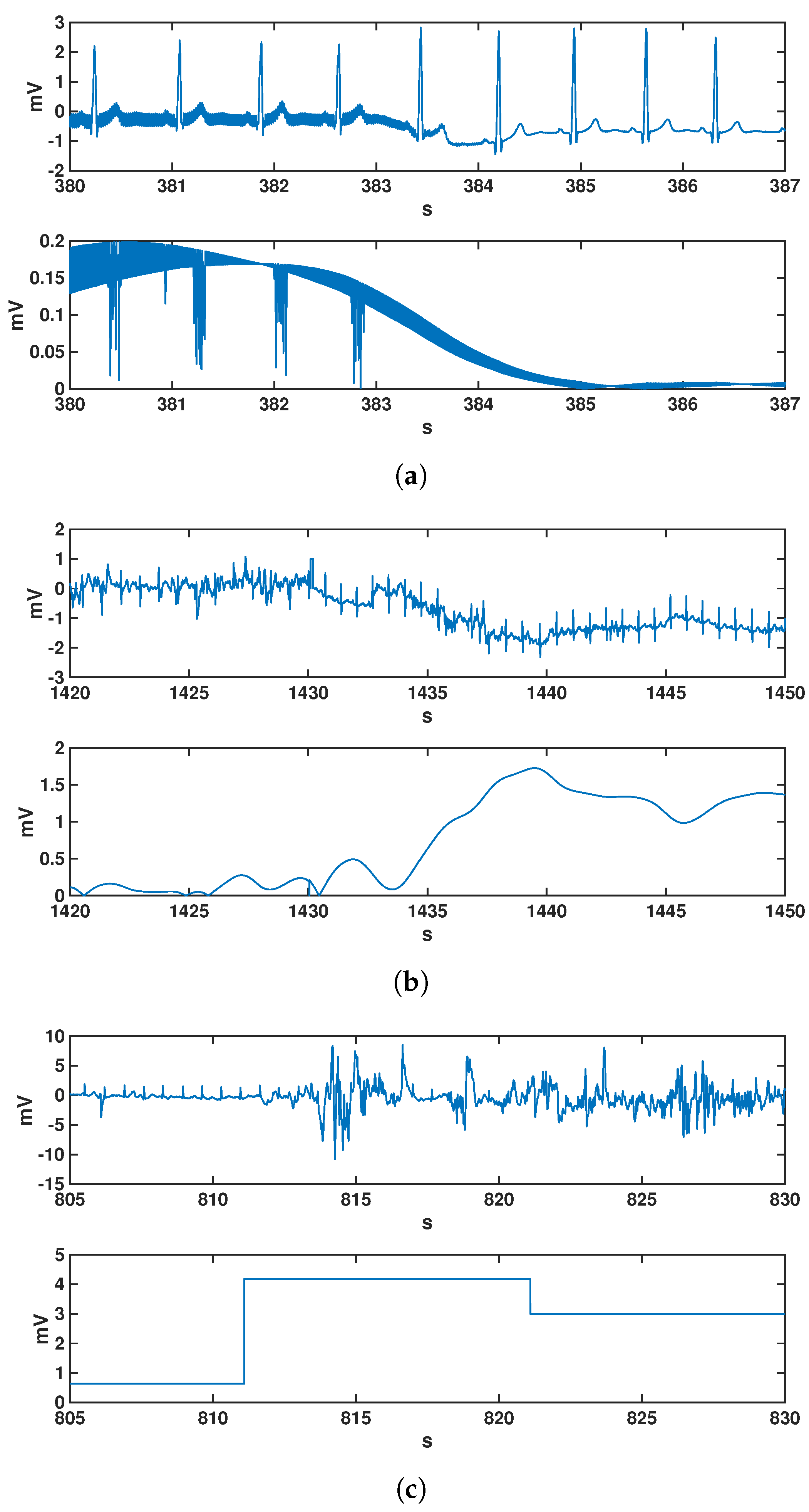
- Other noise (type 4): segments are calibration pulses or straight lines because of the complete absence of signal or amplifier saturation.
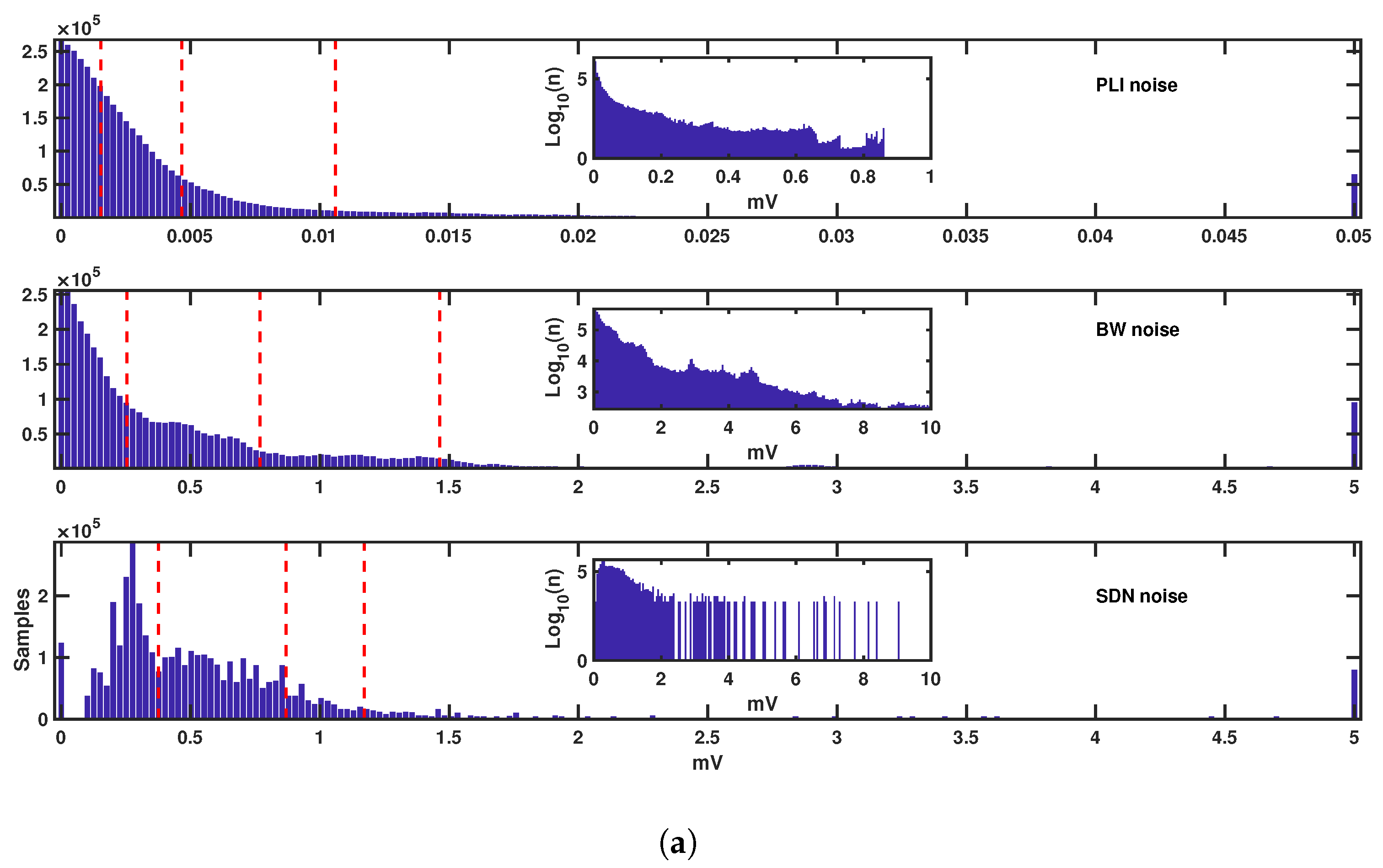
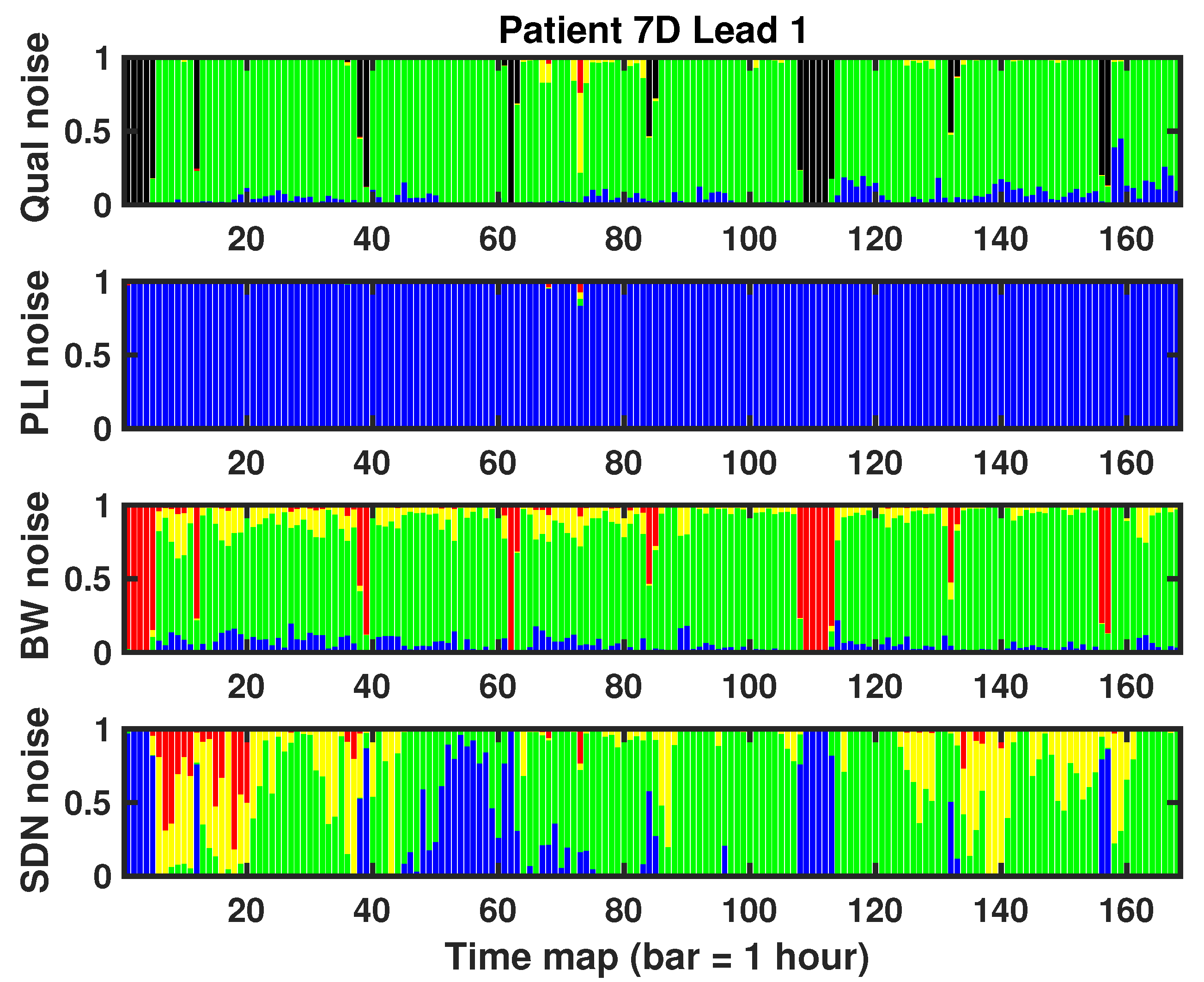
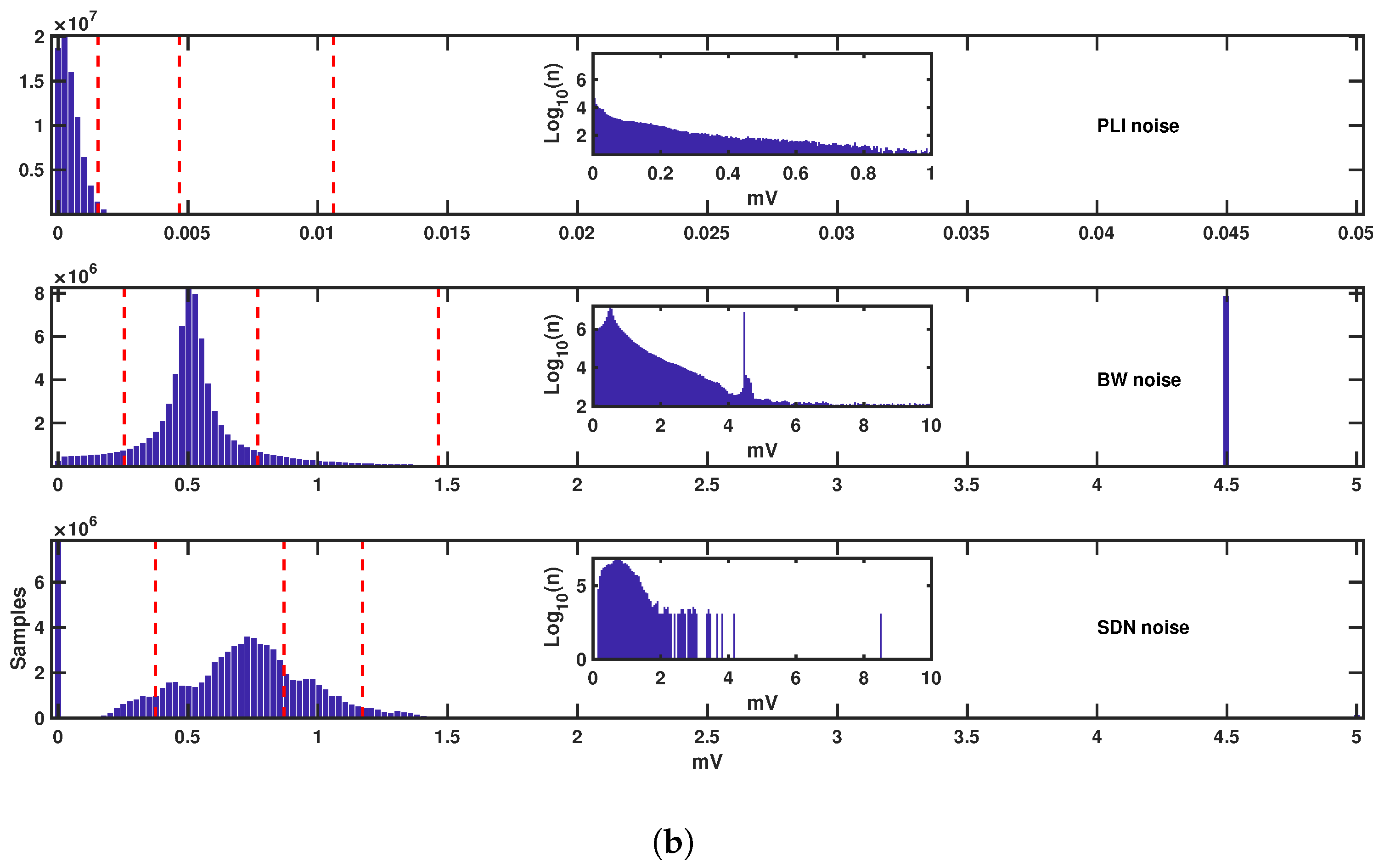
2.3. Noise Measurements using Quantitative Metrics
- BW was calculated by using a cubic spline with a third-order polynomial interpolation and a 0.8 s time window for node estimation.
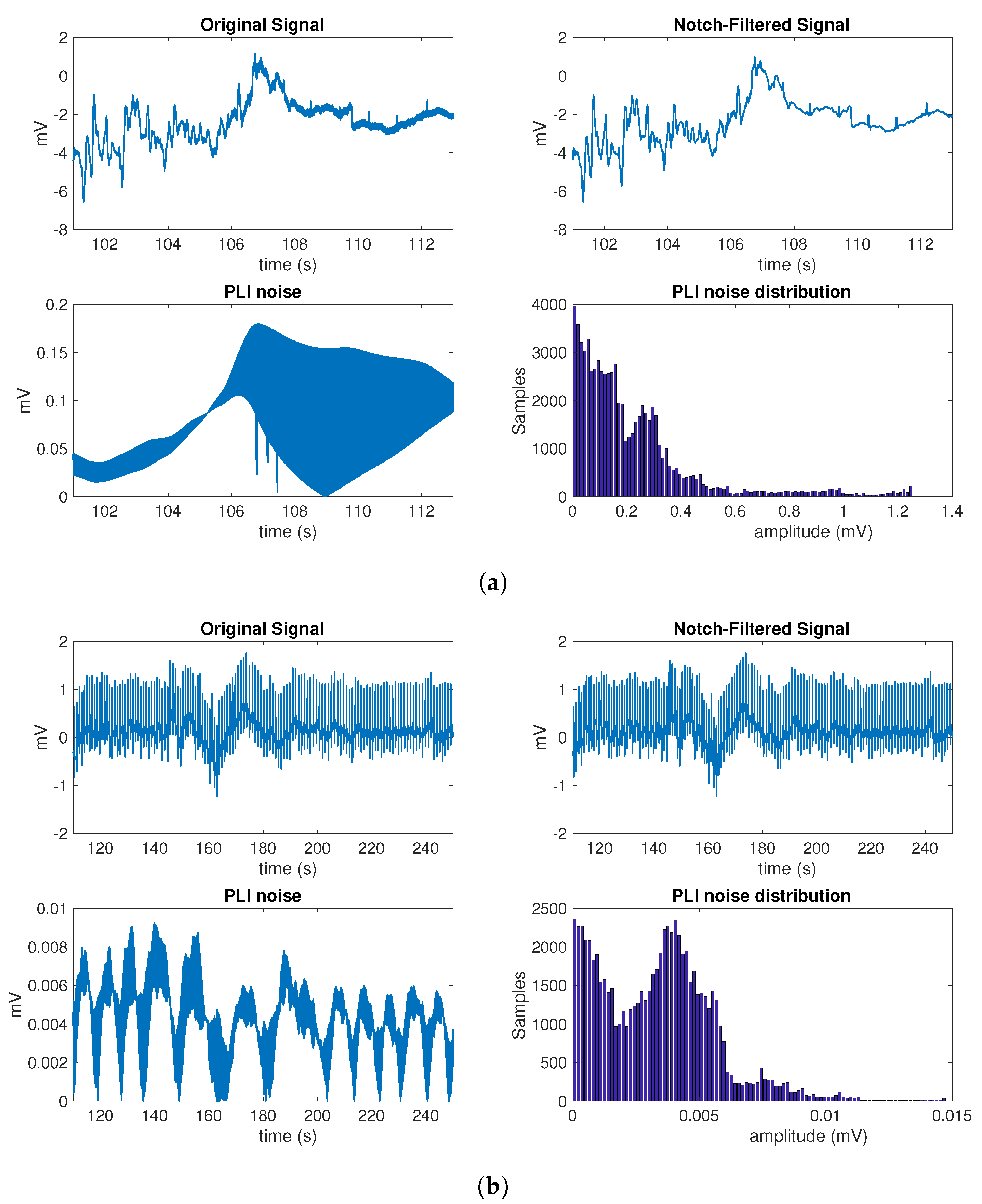
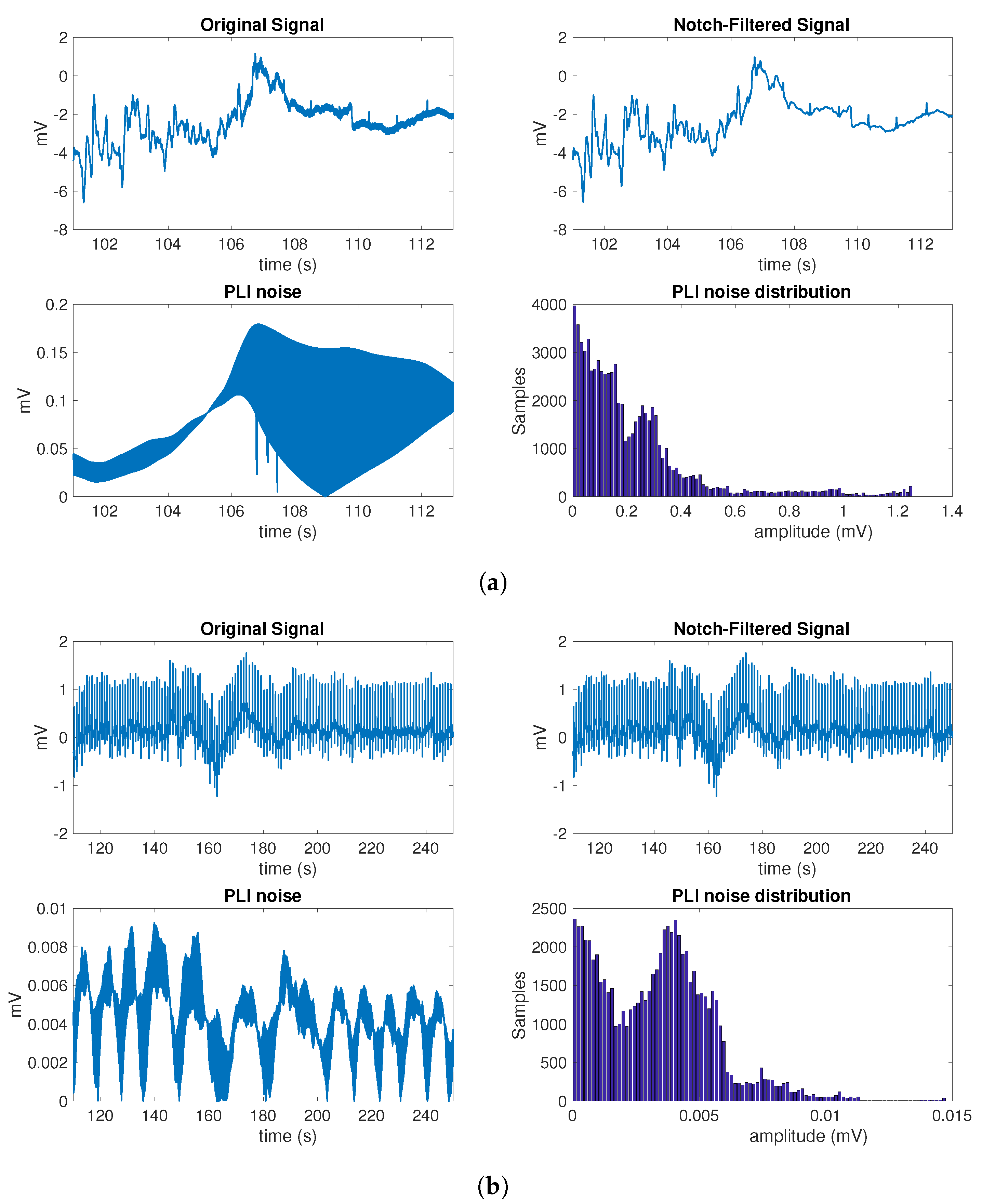
- The quantification of PLI was made with a notch filter with the center frequency at 50 Hz.
- The proposed SDN was extracted by following these steps: (a) the standard deviation of the signal was computed in blocks of 0.5 s; (b) every 10 blocks, the mean and the standard deviation were calculated; (c) finally, the mean plus twice the standard deviation was used as a measure of the noise for each block.
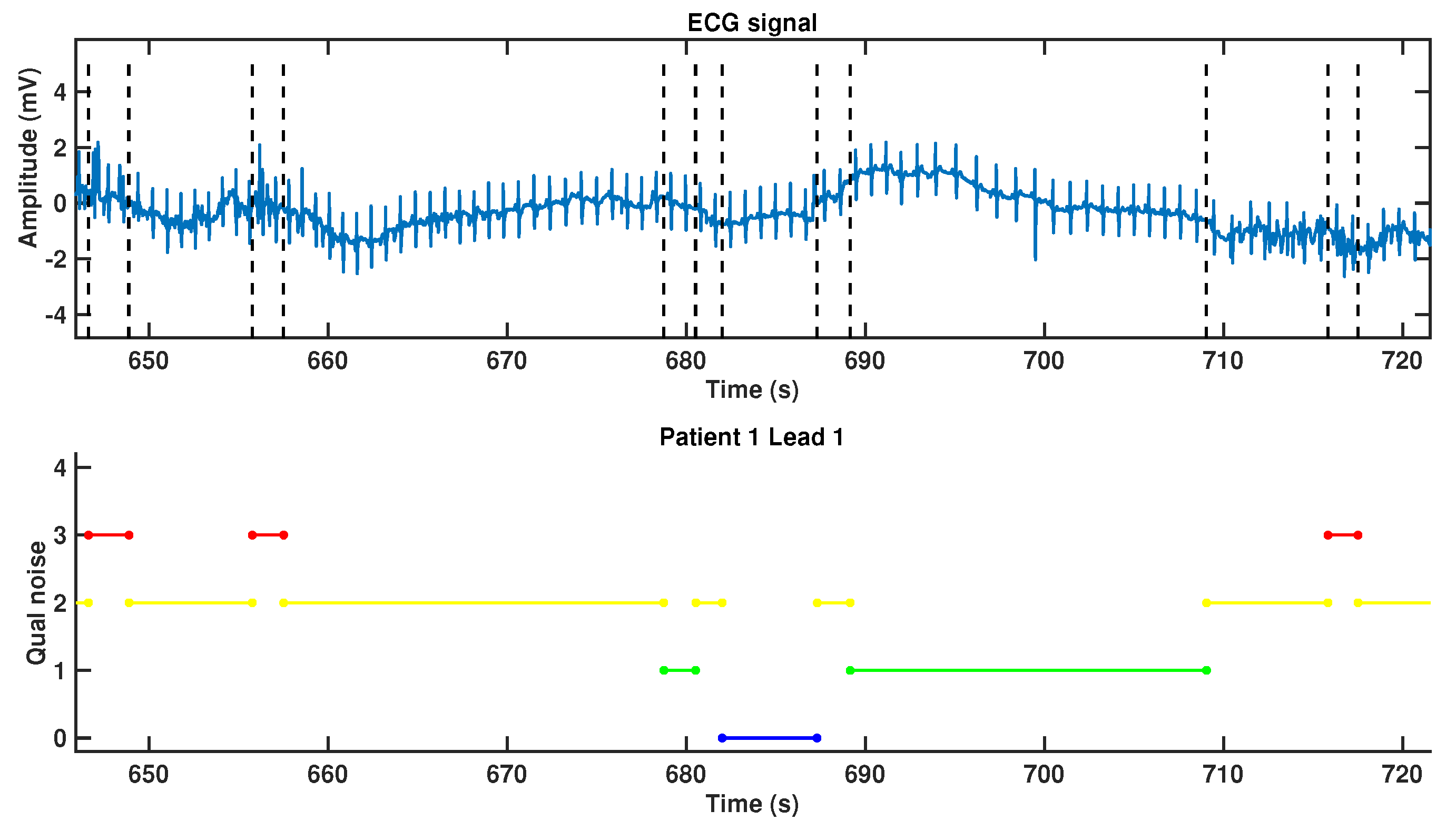
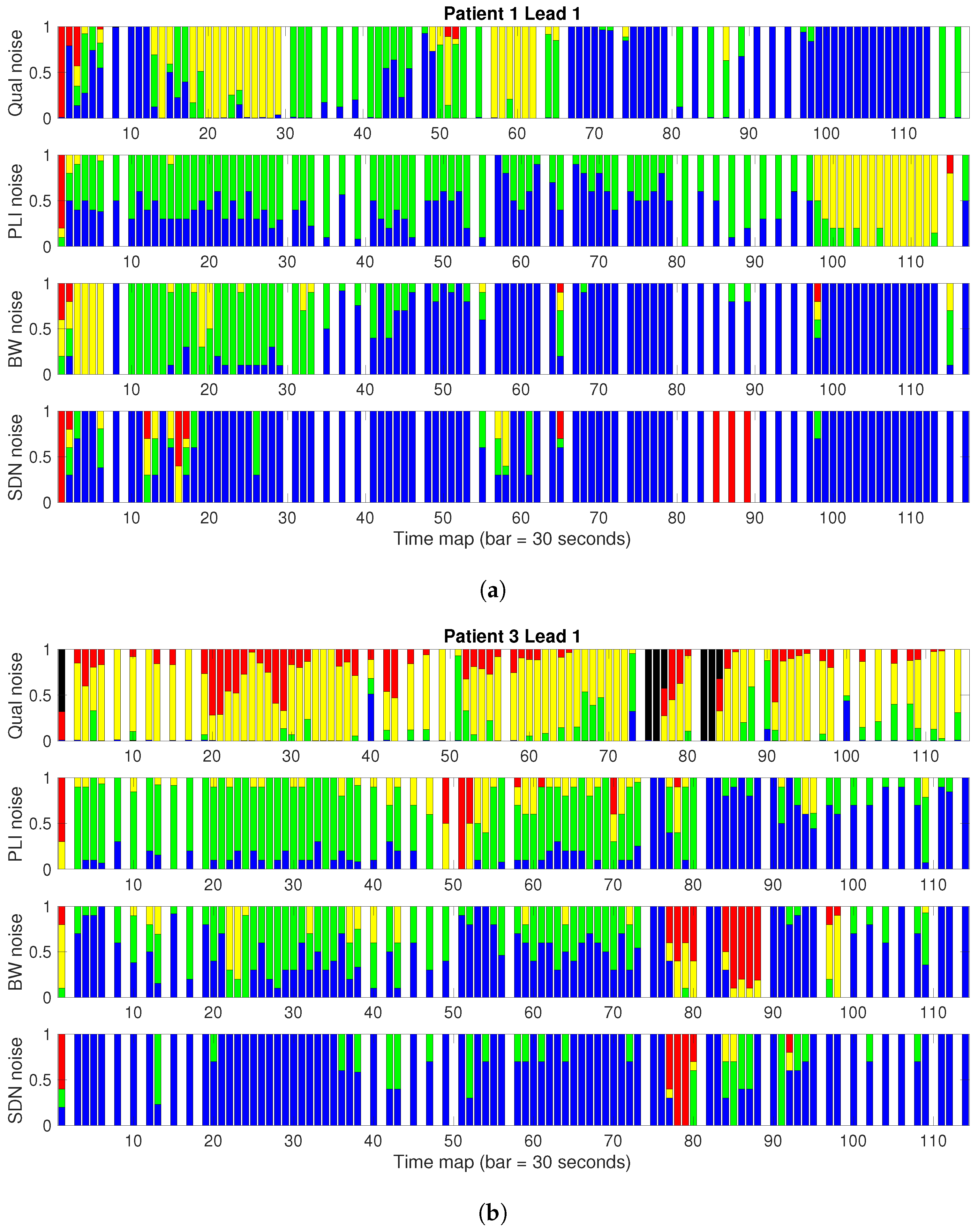
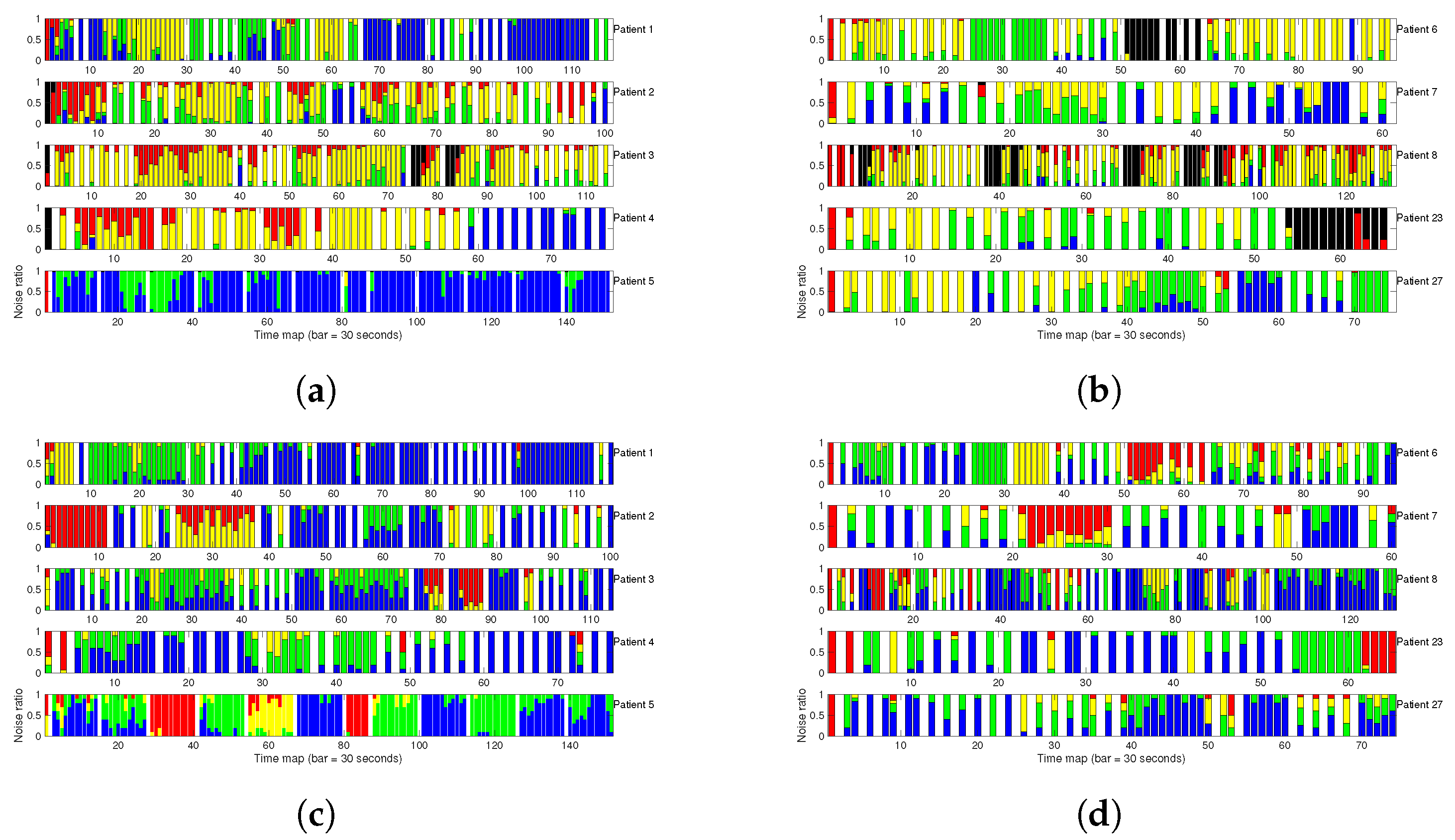
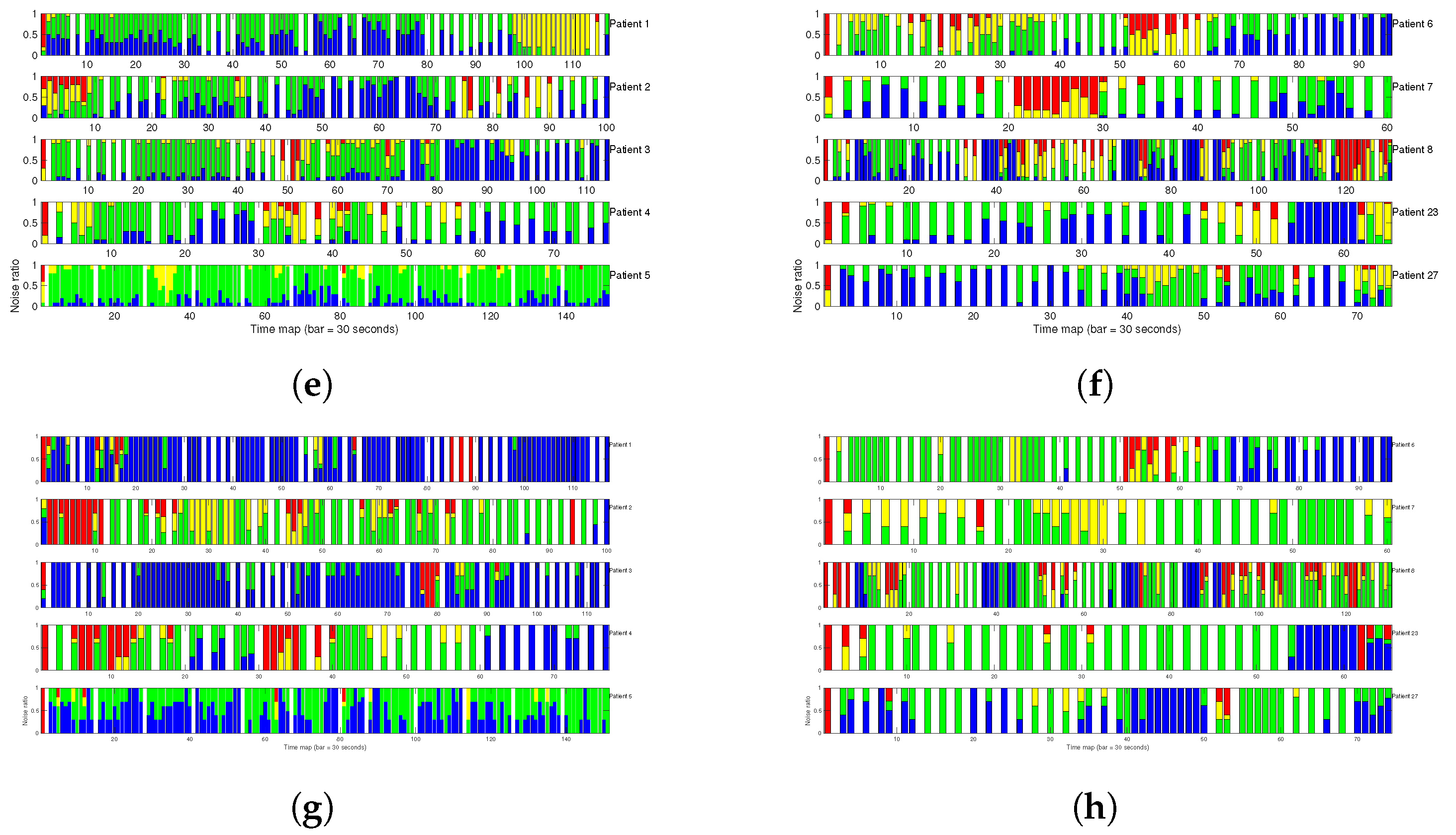
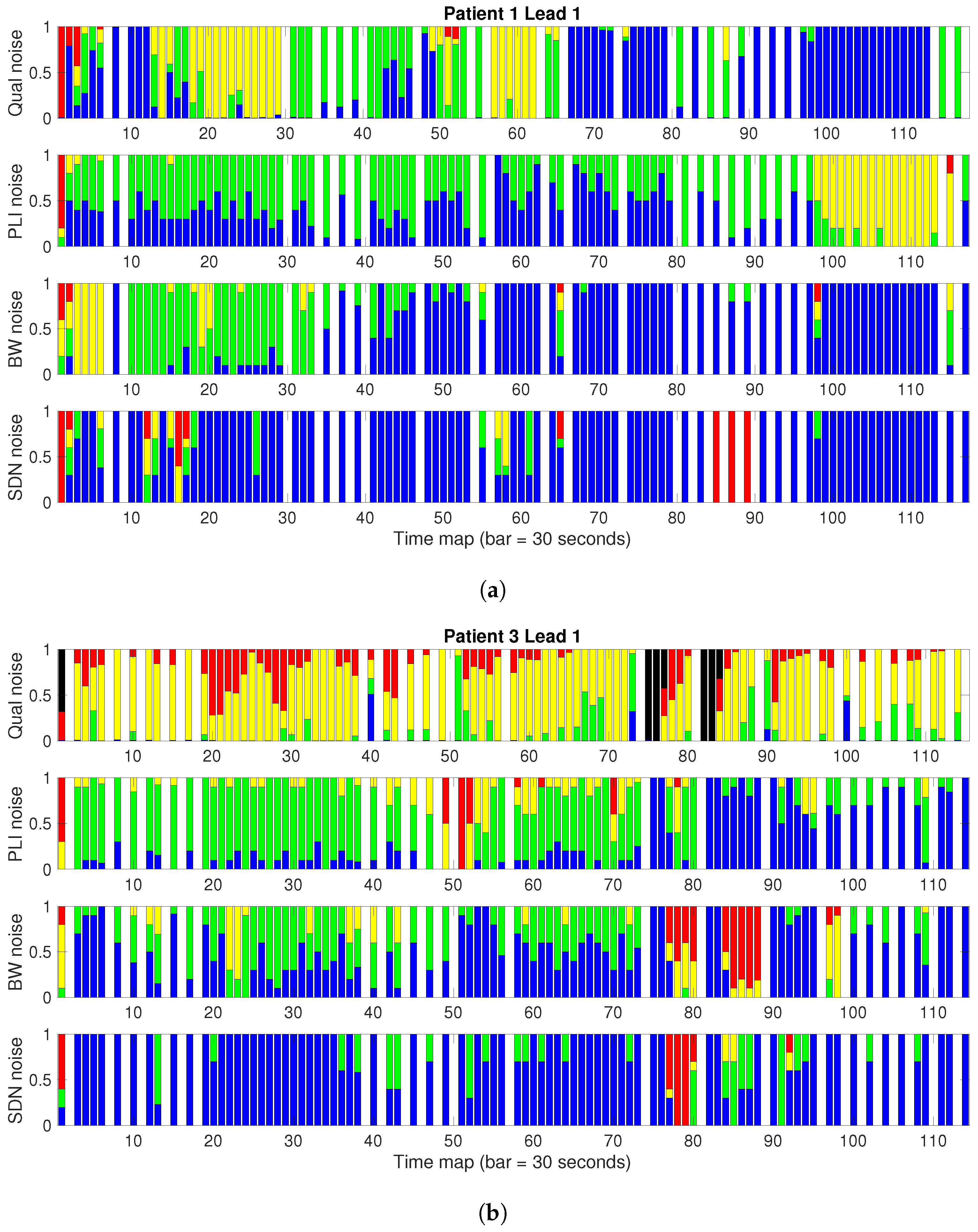
2.4. Time Characterization with Noise Maps
- First, the ECG signal is divided into segments, which are labeled according to their noise power; the labels for clinical severity were defined in Section 2.2.
- Afterwards, quantitative noise is split into four unevenly distributed levels, which in this work were adjusted in the event recorder noise distributions in order to match the quantitative noise map as closely as possible for an expert observer (FMM) to the clinical severity noise maps. This action generates a segmentation on the ECG, for which a list needs to be stored that includes the reference number of each segment, its starting and ending times, and its noise severity labels.
- Finally, label category changes are used for the time instants to define different-size segments corresponding to the set of samples with the same label.
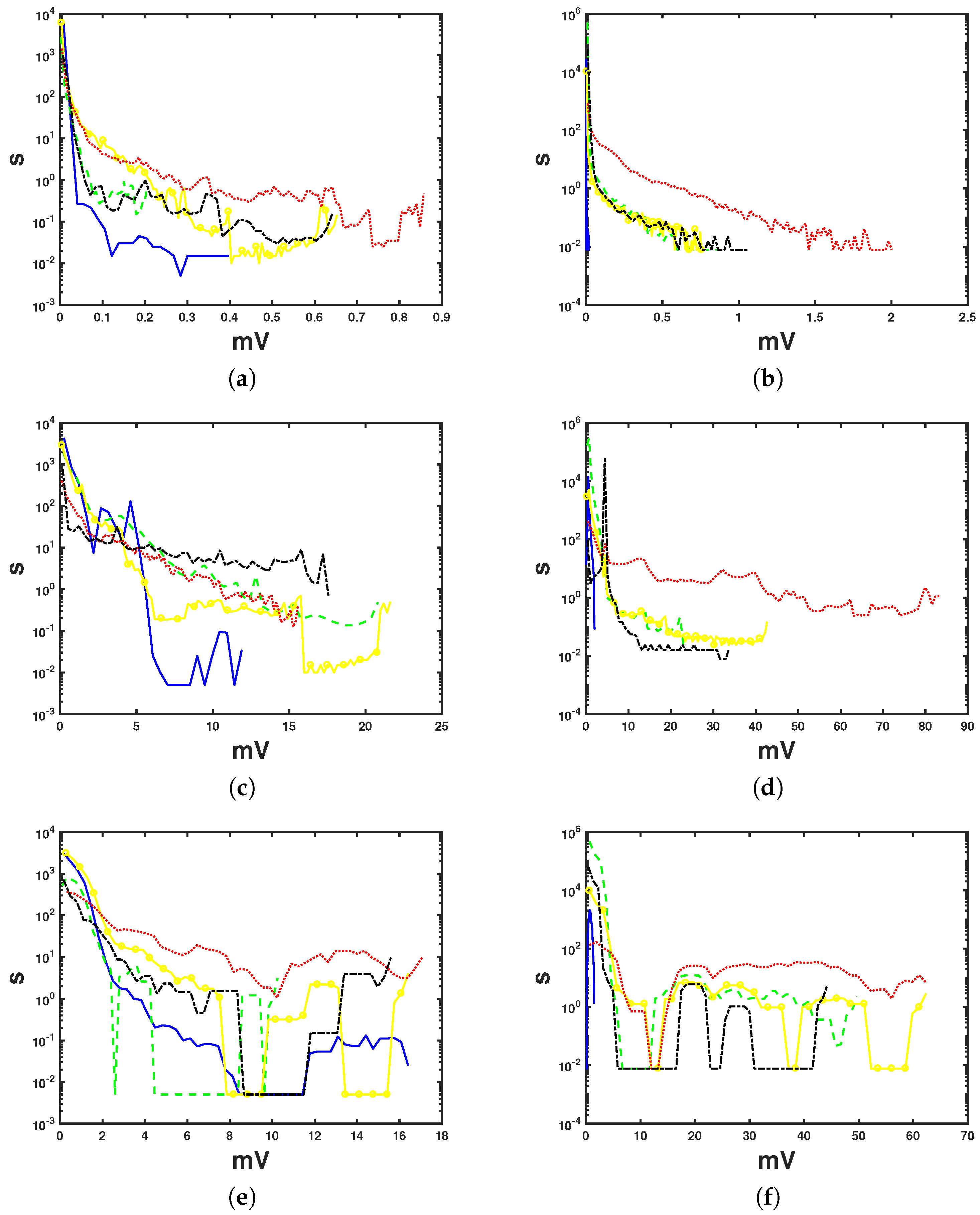
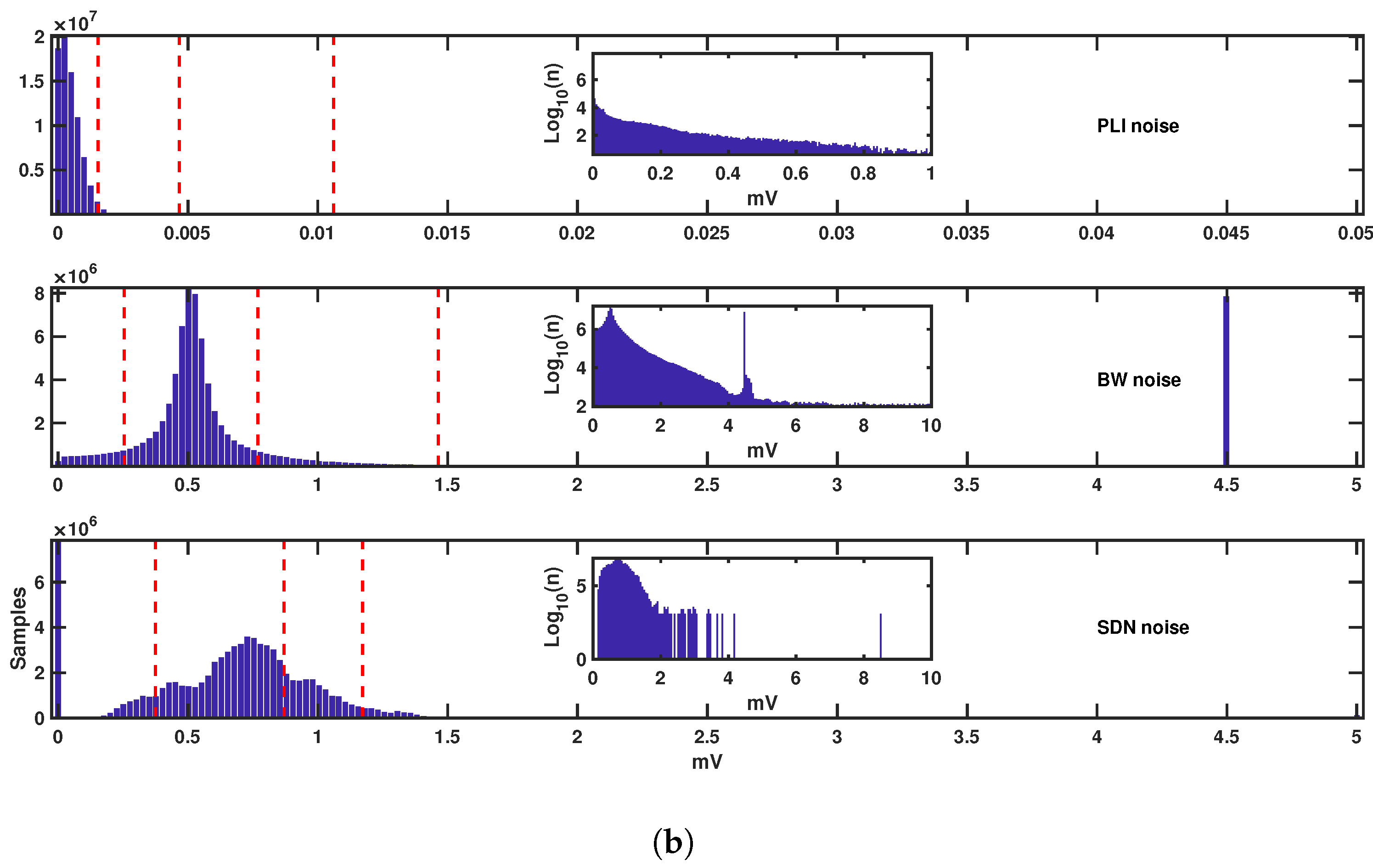
2.5. Statistical Characterization of the Noise Amplitude
3. Results
3.1. Analysis of the Conditional Distributions
3.2. Results of Noise Maps for EER
3.3. Specific Considerations of PLI Noise
3.4. Considerations of Inter-Observer Variability
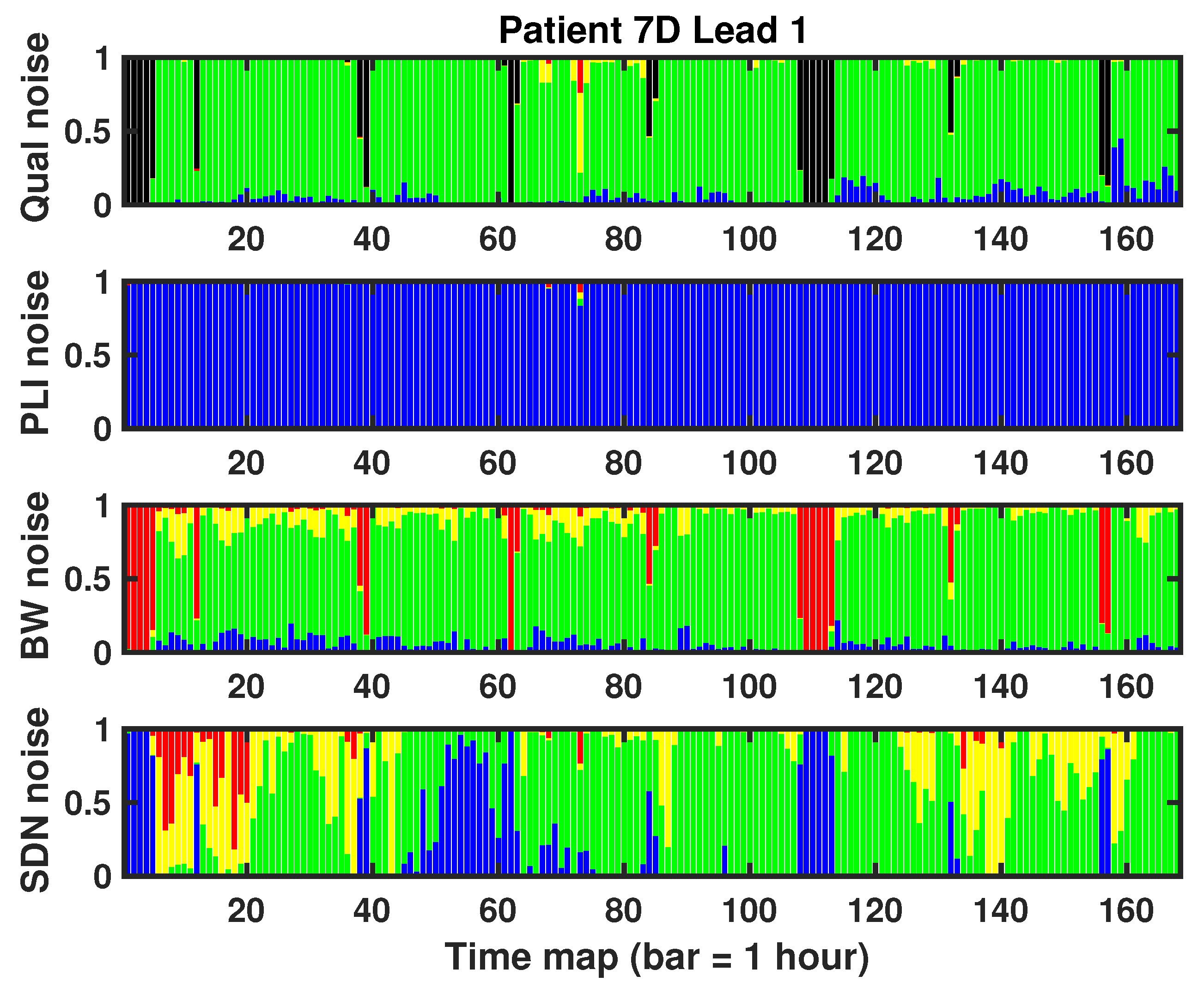
3.5. Results of the 7 Day Holter Case
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Sornmo, L.; Laguna, P. Bioelectrical Signal Processing in Cardiac and Neurological Applications; Elsevier Academic Press: Burlington, MA, USA, 2005. [Google Scholar]
- Holter, N.E. New method for heart studies. Science 1961, 134, 1214–1220. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Choi, Y.Y.; Kim, D.J.; Chae, H.Y.; Park, K.; Oh, Y.M.; Woo, S.H.; Kim, J.J. A Wireless ExG Interface for Patch-Type ECG Holter and EMG-Controlled Robot Hand. Sensors 2017, 17, 1888. [Google Scholar] [CrossRef] [PubMed]
- Leth, S.; Hansen, J.; Nielsen, O.W.; Dinesen, B. Evaluation of Commercial Self-Monitoring Devices for Clinical Purposes: Results from the Future Patient Trial, Phase I. Sensors 2017, 17, 211. [Google Scholar] [CrossRef] [PubMed]
- Clifford, G.D.; Behar, J.; Li, Q.; Rezek, I. Signal quality indices and data fusion for determining clinical acceptability of electrocardiograms. Physiol. Meas. 2012, 33, 1419–1433. [Google Scholar] [CrossRef] [PubMed]
- Free, C.; Phillips, G.; Galli, L.; Watson, L.; Felix, L.; Edwards, P.; Patel, V.; Haines, A. The Effectiveness of Mobile-Health Technology-Based Health Behaviour Change or Disease Management Interventions for Health Care Consumers: A Systematic Review. Plos Med. 2013, 10, e1001362. [Google Scholar] [CrossRef] [PubMed]
- Jabaudon, D.; Sztajzel, J.; Sievert, K.; Landis, T.; Sztajzel, R. Usefulness of Ambulatory 7-Day ECG Monitoring for the Detection of Atrial Fibrillation and Flutter After Acute Stroke and Transient Ischemic Attack. Stroke 2004, 35, 1647–1651. [Google Scholar] [CrossRef] [PubMed]
- Dagres, N.; Kottkamp, H.; Piorkowski, C.; Weis, S.; Arya, A.; Sommer, P.; Bode, K.; Gerds-Li, J.H.; Kremastinos, D.T.; Hindricks, G. Influence of the duration of Holter monitoring on the detection of arrhythmia recurrences after catheter ablation of atrial fibrillation: Implications for patient follow-up. Int. J. Cardiol. 2010, 139, 305–306. [Google Scholar] [CrossRef] [PubMed]
- Pastor-Pérez, F.J.; Manzano-Fernández, S.; Goya-Esteban, R.; Pascual-Figal, D.A.; Barquero-Pérez, O.; Rojo-Álvarez, J.L.; Martínez-Martínez-Espejo, M.D.; Chavarri, M.V.; García-Alberola, A. Comparison of Detection of Arrhythmias in Patients With Chronic Heart Failure Secondary to Non-Ischemic Versus Ischemic Cardiomyopathy by 1 Versus 7-Day Holter Monitoring. Am. J. Cardiol. 2010, 106, 677–681. [Google Scholar] [CrossRef] [PubMed]
- Goya-Esteban, R.; Barquero-Pérez, O.; Caamaño-Fernández, A.; Rojo-Álvarez, J.L.; Pastor-Pérez, F.J.; Manzano-Fernández, S.; García-Alberola, A. Usefulness of 7-Day Holter Monitoring for Heart Eate Variability Nonlinear Dynamics Evaluation. In Proceedings of the Computing in Cardiology, Hangzhou, China, 18–21 September 2011; pp. 105–108. [Google Scholar]
- Clifford, G.D.; Azuaje, F.; McSharry, P.E. Advanced Methods and Tools for ECG Data Analysis; Artech House: Boston, MA, USA, 2006. [Google Scholar]
- Ari, S.; Das, M.K.; Chacko, A. ECG signal enhancement using S-Transform. Comput. Biol. Med. 2013, 43, 649–660. [Google Scholar] [CrossRef] [PubMed]
- Jenkal, W.; Latif, R.; Toumanari, A.; Dliou, A.; Bâcharri, O.E.; Maoulainine, F.M. An efficient algorithm of ECG signal denoising using the adaptive dual threshold filter and the discrete wavelet transform. Biocybern. Biomed. Eng. 2016, 36, 499–508. [Google Scholar] [CrossRef]
- Wang, Z.; Wan, F.; Wong, C.M.; Zhang, L. Adaptive Fourier decomposition based ECG denoising. Comput. Biol. Med. 2016, 77, 195–205. [Google Scholar] [CrossRef] [PubMed]
- Yadav, S.K.; Sinha, R.; Bora, P.K. Electrocardiogram signal denoising using non-local wavelet transform domain filtering. IET Signal Process. 2015, 9, 88–96. [Google Scholar] [CrossRef]
- Smital, L.; Vítek, M.; Kozumplík, J.; Provazník, I. Adaptive Wavelet Wiener Filtering of ECG Signals. IEEE Trans. Biomed. Eng. 2013, 60, 437–445. [Google Scholar] [CrossRef] [PubMed]
- Barros, A.K.; Mansour, A.; Ohnishi, N. Removing artifacts from electrocardiographic signals using independent components analysis. Neurocomputing 1998, 22, 173–186. [Google Scholar] [CrossRef]
- Chawla, M. PCA and ICA processing methods for removal of artifacts and noise in electrocardiograms: A survey and comparison. Appl. Softw. Comput. 2011, 11, 2216–2226. [Google Scholar] [CrossRef]
- Sameni, R. Online filtering using piecewise smoothness priors: Application to normal and abnormal electrocardiogram denoising. Signal Process. 2017, 133, 52–63. [Google Scholar] [CrossRef]
- Nguyen, P.; Kim, J.M. Adaptive ECG denoising using genetic algorithm based thresholding and ensemble empirical mode decomposition. Inf. Sci. 2016, 373, 499–511. [Google Scholar] [CrossRef]
- Blanco-Velasco, M.; Weng, B.; Barner, K.E. ECG signal denoising and baseline wander correction based on the empirical mode decomposition. Comput. Biol. Med. 2008, 38, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Kaergaard, K.; Jensen, S.H.; Puthusserypady, S. A comprehensive performance analysis of EEMD-BLMS and DWT-NN hybrid algorithms for ECG denoising. Biomed. Signal Process. Control 2016, 25, 178–187. [Google Scholar] [CrossRef] [Green Version]
- Reddy, A.S.K.; Chand, N.V.S. ECG Noise Removal by Using Fuzzy Logic Filters. Int. J. Comput. Sci. Math. Eng. 2017, 4, 17–22. [Google Scholar]
- Poungponsri, S.; Yu, X. An adaptive filtering approach for electrocardiogram (ECG) signal noise reduction using neural networks. Neurocomputing 2013, 117, 206–213. [Google Scholar] [CrossRef]
- Xiong, P.; Wang, H.; Liu, M.; Zhou, S.; Hou, Z.; Liu, X. ECG signal enhancement based on improved denoising auto-encoder. Eng. Appl. Artif. Intell. 2016, 52, 194–202. [Google Scholar] [CrossRef]
- Ochoa, A.; Mena, L.J.; Felix, V.G. Noise-Tolerant Neural Network Approach for Electrocardiogram Signal Classification. In Proceedings of the International Conference on Compute and Data Analysis, ICCDA ’17, Lakeland, FL, USA, 19–23 May 2017; pp. 277–282. [Google Scholar]
- Li, Q.; Rajagopalan, C.; Clifford, G. A machine learning approach to multi-level ECG signal quality classification. Comput. Methods Prog. Biomed. 2014, 117, 435–447. [Google Scholar] [CrossRef] [PubMed]
- Redmond, S.J.; Lovell, N.H.; Basilakis, J.; Celler, B.G. ECG quality measures in telecare monitoring. In Proceedings of the 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–25 August 2008; pp. 2869–2872. [Google Scholar]
- Satija, U.; Ramkumar, B.; Manikandan, M.S. A simple method for detection and classification of ECG noises for wearable ECG monitoring devices. In Proceedings of the International Conference on Signal Processing and Integrated Networks (SPIN), Noida, India, 19–20 February 2015; pp. 164–169. [Google Scholar]
- Everss-Villalba, E.; Melgarejo-Meseguer, F.; Gimeno-Blanes, J.; Sala-Pla, S.; Blasco-Velasco, M.; Rojo-Álvarez, J.; García-Alberola, A. Clinical Severity of Noise in ECG. In Proceedings of the Computing in Cardiology Conference (CinC), Vancouver, BC, Canada, 11–14 September 2016; pp. 2869–2872. [Google Scholar]
- Palma-Gámiz, J.L.; Arribas, A.; González-Juanatey, J.R.; Marí-Huerta, E.; Simarro, E. Guías de práctica clínica de la Sociedad Española de Cardiología en la monitorización ambulatoria del electrocardiograma y presión arterial. Rev. Esp. De Cardiol. 2000, 53, 91–109. (In Spanish) [Google Scholar] [CrossRef]
- Moody, G.B.; Muldrow, W.; Mark, R.G. A noise stress test for arrhythmia detectors. Comput. Cardiol. 1984, 11, 381–384. [Google Scholar]
- Goldberger, A.L.; Amaral, L.A.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.K.; Stanley, H.E. PhysioBank, PhysioToolkit, and PhysioNet. Circulation 2000, 101, E215–E220. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. A Coefficient of Agreement for Nominal Scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Lee, J.; McManus, D.; Merchant, S.; Chon, K. Automatic Motion and Noise Artifact Detection in Holter ECG Data Using Empirical Mode Decomposition and Statistical Approaches. IEEE Trans. Biomed. Eng. 2012, 59, 1499–1506. [Google Scholar] [PubMed]
- Agrawal, S.; Gupta, A. Fractal and EMD based removal of baseline wander and powerline interference from ECG signals. Comput. Biol. Med. 2013, 43, 1889–1899. [Google Scholar] [CrossRef] [PubMed]
- ElB’charri, O.; Latif, R.; Elmansouri, K.; Abenaou, A.; Jenkal, W. ECG signal performance denoising assessment based on threshold tuning of dual-tree wavelet transform. Biomed. Eng. Online 2017, 16, 26. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, J.; Belo, D.; Gamboa, H. Noise detection on ECG based on agglomerative clustering of morphological features. Comput. Biol. Med. 2017, 87, 322–334. [Google Scholar] [CrossRef] [PubMed]
- He, H.; Tan, Y.; Wang, Y. Optimal Base Wavelet Selection for ECG Noise Reduction Using a Comprehensive Entropy Criterion. Entropy 2015, 17, 6093–6109. [Google Scholar] [CrossRef]
- Jekova, I.; Krasteva, V.; Christov, I.; Abächerli, R. Threshold-based system for noise detection in multilead ECG recordings. Physiol. Meas. 2012, 33, 1463–1477. [Google Scholar] [CrossRef] [PubMed]
- Sivakumar, R.; Tamilselvi, R.; Abinaya, S. Noise Analysis and QRS Detection in ECG Signals. In Proceedings of the 2012 International Conference on Computer Technology and Science (ICCTS 2012), New Delhi, India, 18–19 August 2012; pp. 141–146. [Google Scholar]
- Clifford, G.D.; López, D.; Li, Q.; Rezek, I. Signal quality indices and data fusion for determining acceptability of electrocardiograms collected in noisy ambulatory environments. Comput. Cardiol. 2011, 6801, 285–288. [Google Scholar]
- Satija, U.; Ramkumar, B.; Manikandan, M.S. Automated ECG Noise Detection and Classification System for Unsupervised Healthcare Monitoring. IEEE J. Biomed. Health Inf. 2017, PP. [Google Scholar] [CrossRef] [PubMed]
- Naseri, H.; Homaeinezhad, M. Electrocardiogram signal quality assessment using an artificially reconstructed target lead. Comput. Methods Biomech. Biomed. Eng. 2014, 18, 1126–1141. [Google Scholar] [CrossRef] [PubMed]
- Jovanovic, B.; Litovski, V.; Pavlovic, M. QRS complex detection based ECG signal artefact discrimination. Facta Univ. 2015, 28, 571–574. [Google Scholar] [CrossRef]
- Hayn, D.; Jammerbund, B.; Schreier, G. Noise detection on ECG based on agglomerative clustering of morphological features. Physiol. Meas. 2012, 33, 1449–1461. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N. Pat | Total Duration | Free | Low | Moderate | Hard | Other | Free | Low | Moderate | Hard | Other |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2843,00 | 1383,55 | 774,36 | 621,97 | 57,26 | 5,88 | 1563,73 | 984,01 | 244,52 | 44,87 | 5,88 |
| 2 | 2433,00 | 195,11 | 719,02 | 994,89 | 480,24 | 43,76 | 180,68 | 725,48 | 994,67 | 488,42 | 43,76 |
| 3 | 2854,00 | 52,53 | 307,62 | 1891,07 | 434,43 | 168,36 | 32,50 | 287,83 | 1483,24 | 810,95 | 239,49 |
| 4 | 1673,00 | 338,98 | 44,54 | 861,47 | 392,53 | 35,49 | 345,50 | 31,84 | 514,52 | 745,66 | 35,49 |
| 5 | 4214,07 | 3451,95 | 709,36 | 10,19 | 29,76 | 12,82 | 3268,71 | 892,67 | 10,19 | 29,76 | 12,75 |
| 6 | 2134,00 | 65,05 | 611,16 | 1025,32 | 50,13 | 382,35 | 49,65 | 831,60 | 822,24 | 51,24 | 379,28 |
| 7 | 1172,00 | 376,00 | 356,04 | 394,61 | 37,70 | 7,67 | 403,24 | 364,32 | 357,38 | 39,41 | 7,67 |
| 8 | 3114,00 | 77,08 | 366,84 | 1561,03 | 512,31 | 596,76 | 50,16 | 341,99 | 1240,41 | 884,84 | 596,61 |
| 23 | 1278,00 | 31,38 | 501,94 | 347,98 | 86,20 | 310,51 | 31,38 | 501,94 | 347,98 | 86,20 | 310,51 |
| 27 | 1588,00 | 289,45 | 761,25 | 483,28 | 48,16 | 5,88 | 289,45 | 761,25 | 483,28 | 48,16 | 5,88 |
| 7d | 606716 | 33602,99 | 500037,07 | 10355,21 | 1252,02 | 61468,7 | 36306,41 | 500046,92 | 10355,13 | 1252,02 | 58755,52 |
| Observer 2 | ||||||
| Free | Low | Moderate | Hard | Others | ||
| Free | 3.67 | 1.86 | 0.00 | 0.00 | 0.00 | |
| Low | 0.30 | 20.46 | 0.29 | 0.00 | 0.00 | |
| Observer 1 | Moderate | 0.05 | 6.92 | 6.88 | 0.01 | 0.00 |
| Hard | 0.00 | 0.03 | 0.06 | 2.14 | 0.01 | |
| Others | 0.00 | 0.00 | 0.00 | 0.00 | 5.08 | |
| Observer 2 | ||||||
| Free-Low | Moderate | Hard | Others | |||
| Observer 1 | Free–Low | 26.30 | 0.29 | 0.00 | 0.00 | |
| Moderate | 6.97 | 6.88 | 0.01 | 0.00 | ||
| Hard | 0.03 | 0.06 | 2.14 | 0.01 | ||
| Others | 0.00 | 0.00 | 0.00 | 5.08 | ||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Everss-Villalba, E.; Melgarejo-Meseguer, F.M.; Blanco-Velasco, M.; Gimeno-Blanes, F.J.; Sala-Pla, S.; Rojo-Álvarez, J.L.; García-Alberola, A. Noise Maps for Quantitative and Clinical Severity Towards Long-Term ECG Monitoring. Sensors 2017, 17, 2448. https://doi.org/10.3390/s17112448
Everss-Villalba E, Melgarejo-Meseguer FM, Blanco-Velasco M, Gimeno-Blanes FJ, Sala-Pla S, Rojo-Álvarez JL, García-Alberola A. Noise Maps for Quantitative and Clinical Severity Towards Long-Term ECG Monitoring. Sensors. 2017; 17(11):2448. https://doi.org/10.3390/s17112448
Chicago/Turabian StyleEverss-Villalba, Estrella, Francisco Manuel Melgarejo-Meseguer, Manuel Blanco-Velasco, Francisco Javier Gimeno-Blanes, Salvador Sala-Pla, José Luis Rojo-Álvarez, and Arcadi García-Alberola. 2017. "Noise Maps for Quantitative and Clinical Severity Towards Long-Term ECG Monitoring" Sensors 17, no. 11: 2448. https://doi.org/10.3390/s17112448