
Current and Emerging Technology for Continuous Glucose Monitoring

 ,
,  ,
,
Abstract
:1. Introduction
2. Mini-Invasive Biosensors for CGM
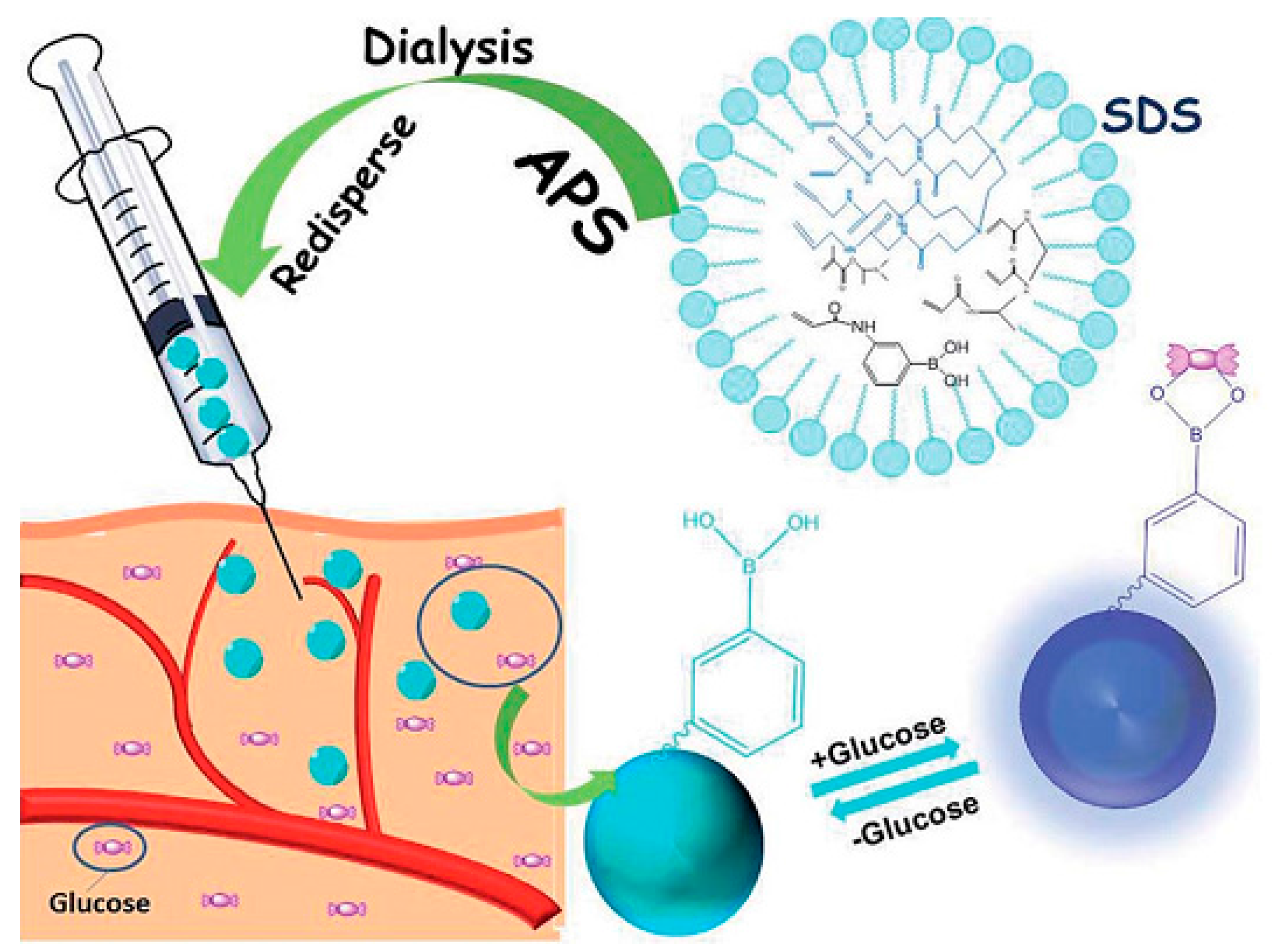
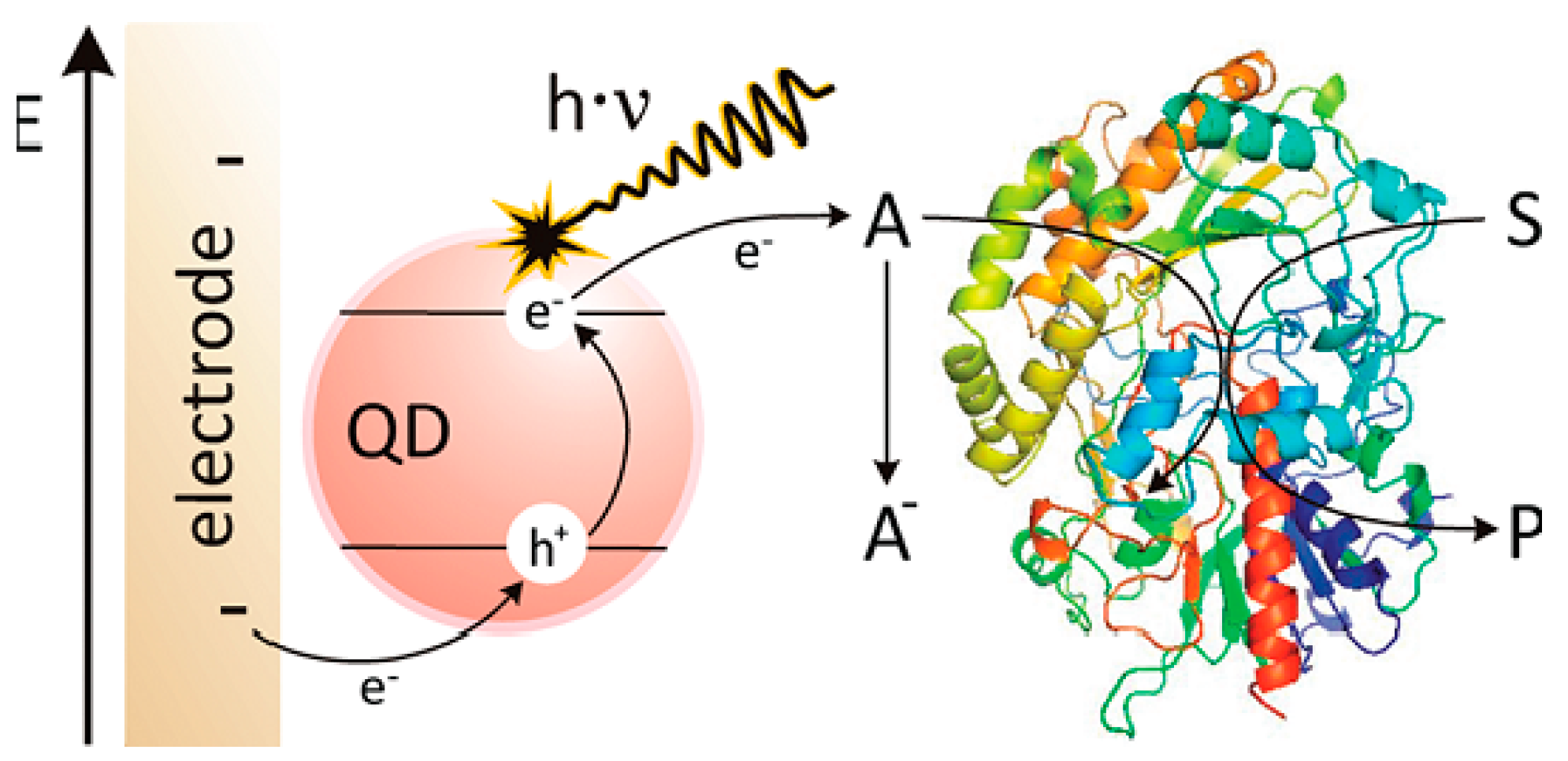
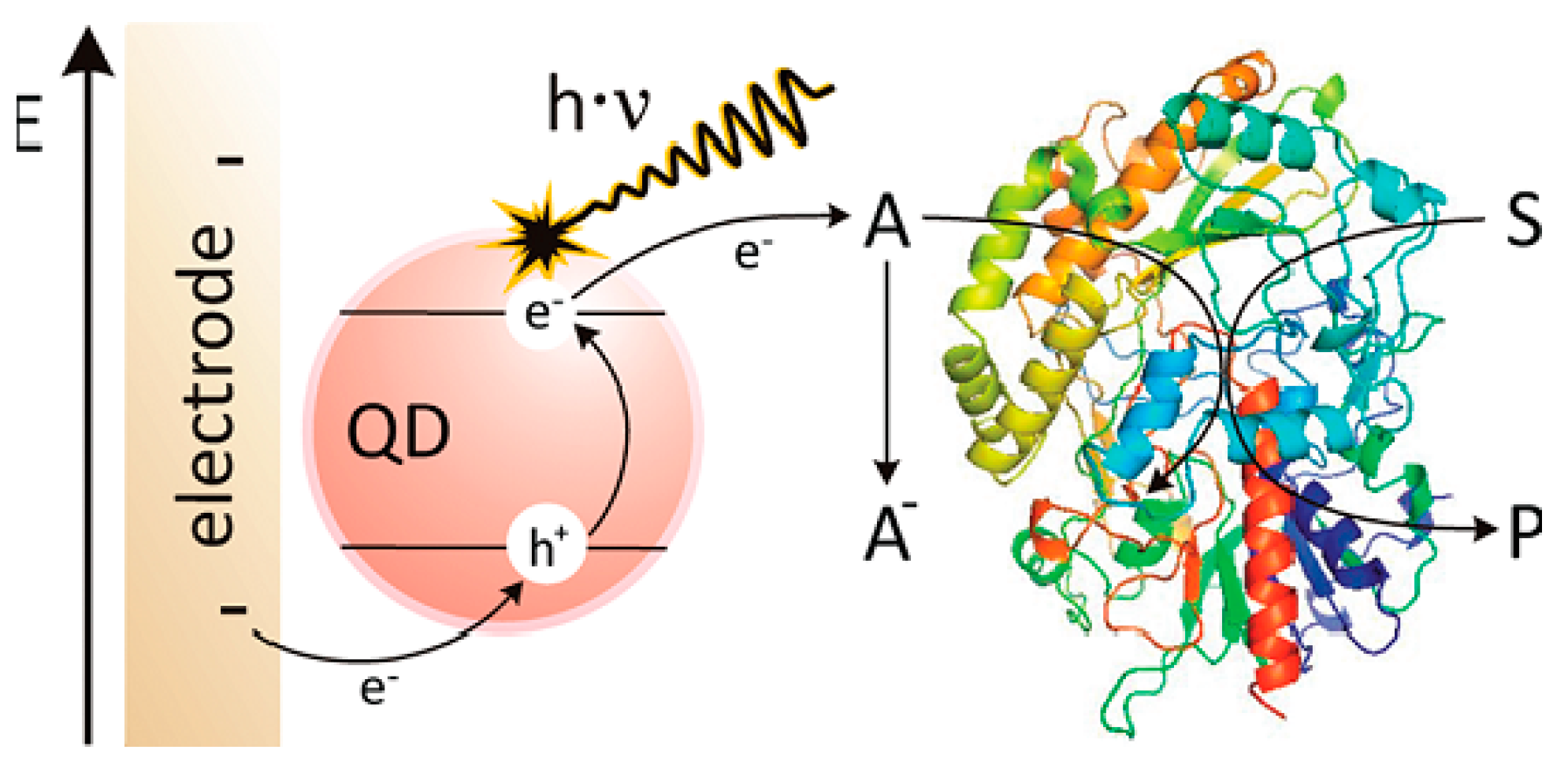
2.1. Sensing Design and New Materials
2.2. Novel Biocompatible Coatings for Sensors
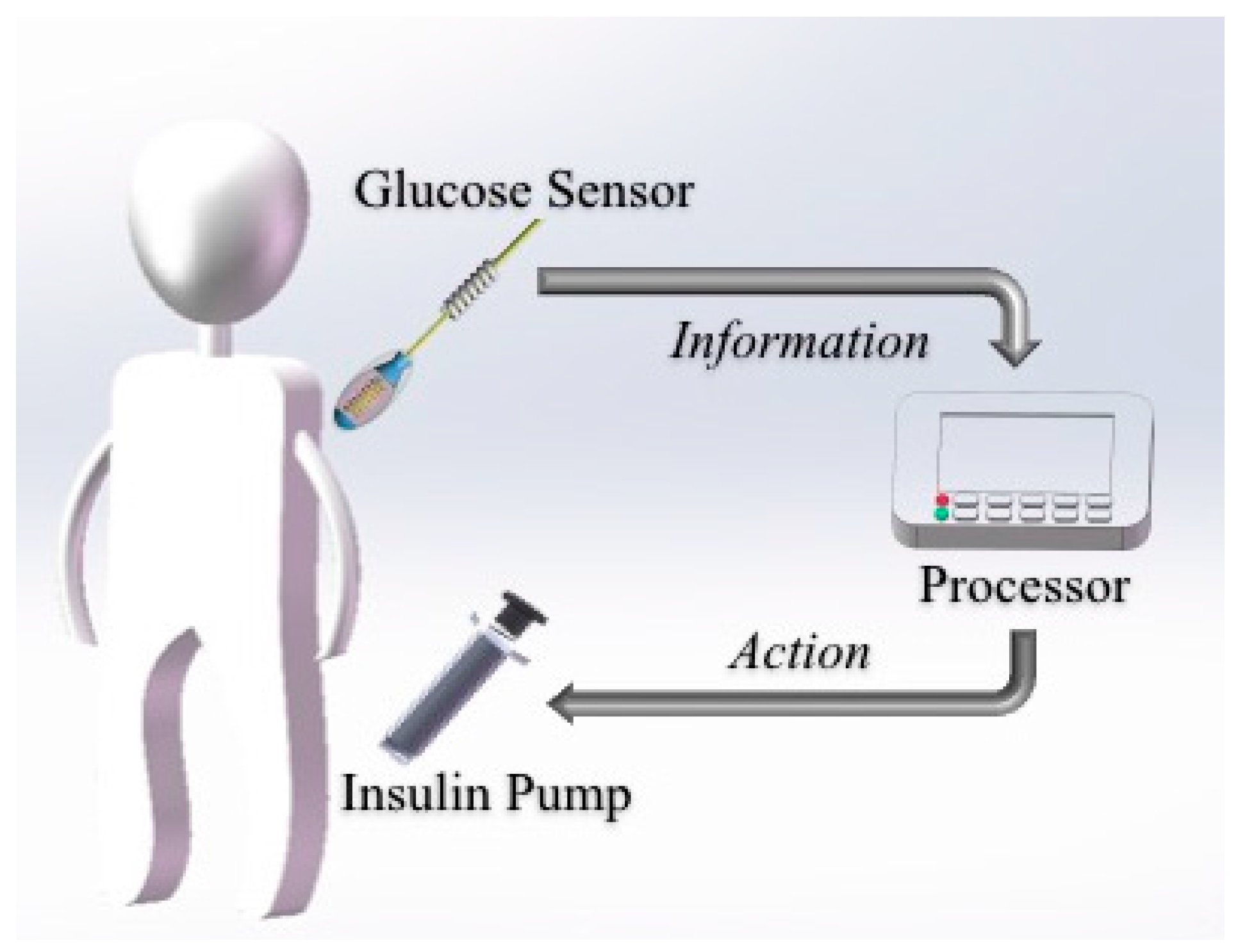
2.3. Drug Deliver and Its System
3. Non-Invasive Technology
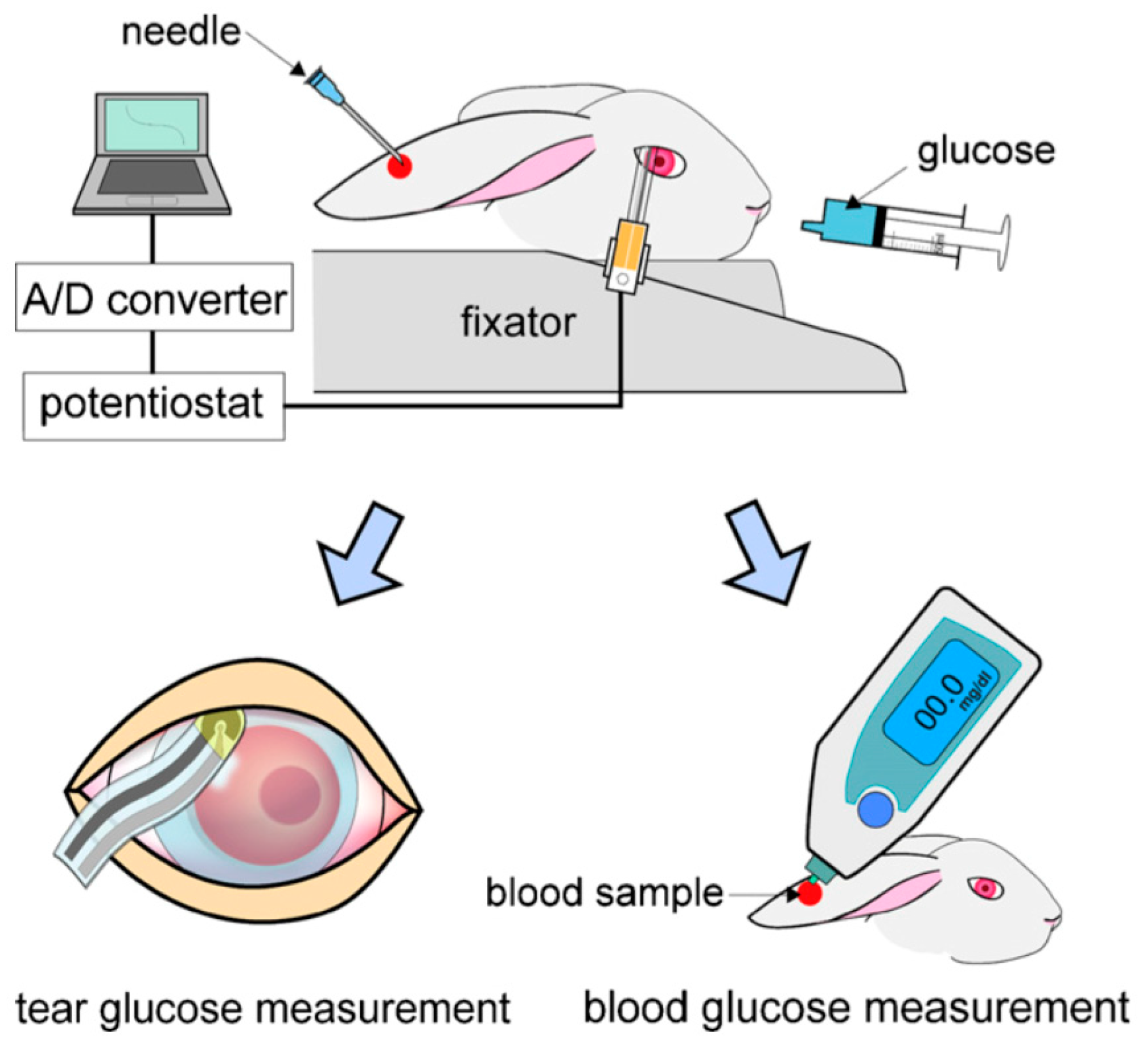
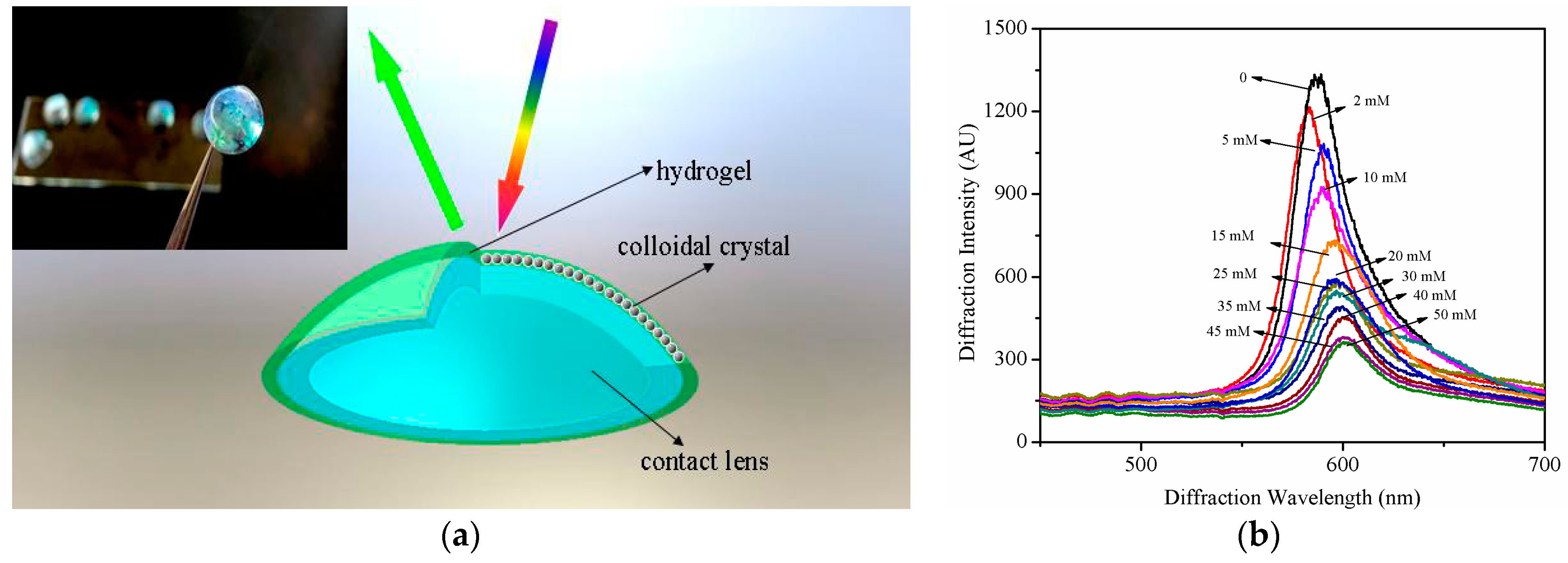
3.1. Tear Sensing Designs
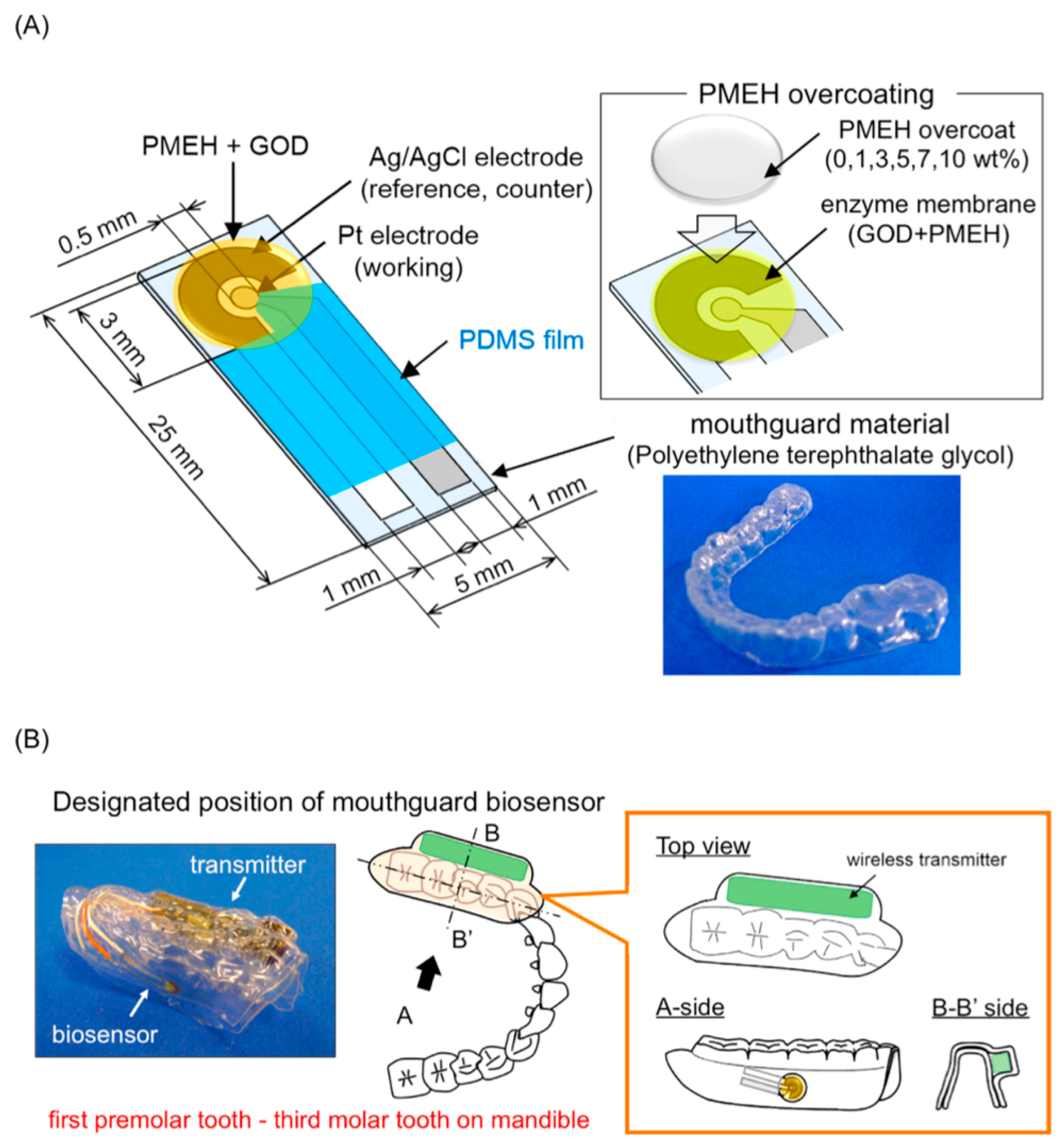
3.2. Salivary Biosensors
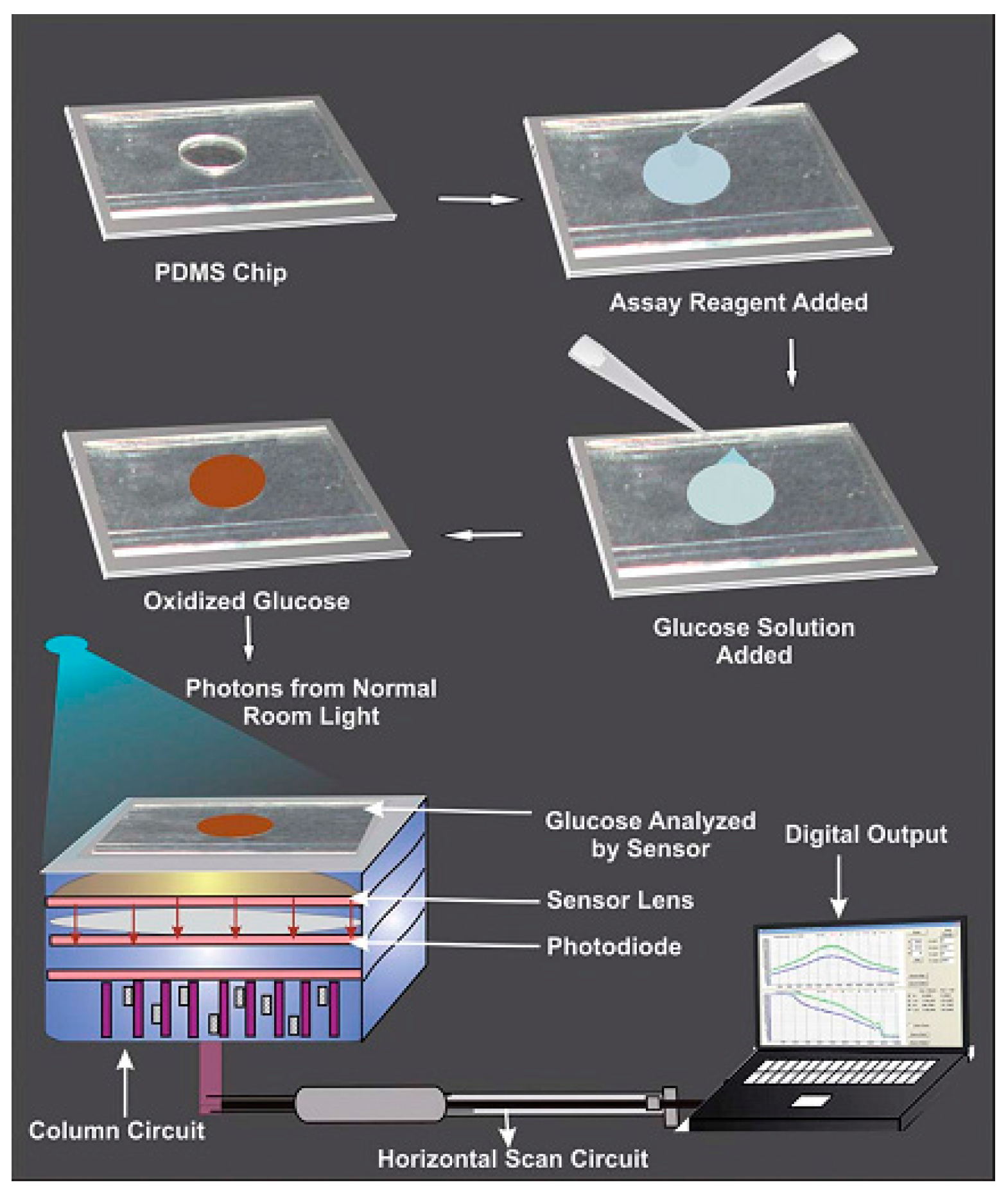
3.3. Other Methods
4. Future Perspectives
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Global Report on Diabetes 2016; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Centers for Disease Control and Prevention. National Diabetes Fact Sheet: National Estimates and General Information on Diabetes and Prediabetes in the United States; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2011.
- Wild, S.; Roglic, G.; Green, A.; Sicree, R.; King, H. Global prevalence of diabetes: Estimates for the year 2000 and projections for 2030. Diabetes Care 2004, 27, 1047–1053. [Google Scholar] [CrossRef] [PubMed]
- Chase, H.P.; Beck, R.W.; Xing, D.; Tamborlane, W.V.; Coffey, J.; Fox, L.A.; Ives, B.; Keady, J.; Kollman, C.; Laffel, L.; et al. Continuous glucose monitoring in youth with type 1 diabetes: 12-month follow-up of the Juvenile Diabetes Research Foundation continuous glucose monitoring randomized trial. Diabetes Technol. Ther. 2010, 12, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Vigersky, R.A. The benefits, limitations, and cost-effectiveness of advanced technologies in the management of patients with diabetes mellitus. J. Diabetes Sci. Technol. 2015, 9, 320–330. [Google Scholar] [CrossRef] [PubMed]
- Ehrhardt, N.M.; Chellappa, M.; Walker, M.S.; Fonda, S.J.; Vigersky, R.A. The effect of real-time continuous glucose monitoring on glycemic control in patients with type 2 diabetes mellitus. J. Diabetes Sci. Technol. 2011, 5, 668–675. [Google Scholar] [CrossRef] [PubMed]
- Clark, L.C.; Lyon, C. Electrode systems for continuous monitoring in cardiovascular surgery. Ann. N. Y. Acad. Sci. 1962, 102, 29–45. [Google Scholar] [CrossRef] [PubMed]
- Dovč, K.; Bratina, N.; Battelino, T. A new horizon for glucose monitoring. Horm. Res. Paediatr. 2015, 83, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Mauras, N.; Fox, L.; Englert, K.; Beck, R.W. Continuous glucose monitoring in type 1 diabetes. Endocrine 2013, 43, 41–50. [Google Scholar] [CrossRef] [PubMed]
- McGarraugh, G.; Bergenstal, R. Detection of hypoglycemia with continuous interstitial and traditional blood glucose monitoring using the FreeStyle navigator continuous glucose monitoring system. Diabetes Technol. Ther. 2009, 11, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Sparacino, G.; Facchinetti, A.; Cobelli, C. “Smart” continuous glucose monitoring sensors: Online signal processing issues. Sensors 2010, 10, 6751–6772. [Google Scholar] [CrossRef] [PubMed]
- Cobelli, C.; Renard, E.; Kovatchev, B. Artificial pancreas: Past, present, future. Diabetes 2011, 60, 2672–2682. [Google Scholar] [CrossRef] [PubMed]
- Langendam, M.; Luijf, Y.M.; Hooft, L.; DeVries, J.H.; Mudde, A.H.; Scholten, R.J.P.M. Continuous glucose monitoring systems for type 1 diabetes mellitus. Cochrane Database Syst. Rev. 2012, 1, CD008101. [Google Scholar] [PubMed]
- McQueen, R.B.; Ellis, S.L.; Campbell, J.D.; Nair, K.V.; Sullivan, P.W. Cost-effectiveness of continuous glucose monitoring and intensive insulin therapy for type 1 diabetes. Cost Eff. Resour. Alloc. 2011, 9, 13. [Google Scholar] [CrossRef] [PubMed]
- Szypowska, A.; Ramotowska, A.; Dżygało, K.; Golicki, D. Beneficial effect of real-time continuous glucose monitoring system on glycemic control in type 1 diabetic patients: Systematic review and meta-analysis of randomized trials. Eur. J. Endocrinol. 2012, 166, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.G.; Garcia-Gancedo, L.; Flewitt, A.J.; Xie, H.Q.; Moussy, F.; Milne, W.I. A Critical Review of Glucose Biosensors Based on Carbon Nanomaterials: Carbon Nanotubes and Graphene. Sensors 2012, 12, 5996–6022. [Google Scholar] [CrossRef] [PubMed]
- Aggidis, A.G.A.; Newman, J.D.; Aggidis, G.A. Investigating pipeline and state of the art blood glucose biosensors to formulate next steps. Biosens. Bioelectron. 2015, 74, 243–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bailey, T.; Bode, B.W.; Christiansen, M.P.; Klaff, L.J.; Alva, S. The performance and usability of a factory-calibrated flash glucose monitoring system. Diabetes Technol. Ther. 2015, 17, 787–794. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.J.; Wu, S.Y.; Chen, P.C.; Lin, Y.S. An Innovative Smartphone-Based Otorhinoendoscope and Its Application in Mobile Health and Teleotolaryngology. J. Med. Internet. Res. 2014, 16, e71. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.G.; Garcia-Gancedo, L.; Chen, C.; Zhu, X.R.; Xie, H.Q.; Flewitt, A.J.; Milne, W.I. Enzyme-free glucose biosensor based on low density CNT forest grown directly on a Si/SiO2 substrate. Sens. Actuators B Chem. 2013, 178, 586–592. [Google Scholar] [CrossRef]
- Wang, H.C.; Zhou, H.; Chen, B.Q.; Mendes, P.M.; Fossey, J.S.; James, T.D.; Long, Y.T. A bis-boronic acid modified electrode for the sensitive and selective determination of glucose concentrations. Analyst 2013, 138, 7146–7151. [Google Scholar] [CrossRef] [PubMed]
- Moon, B.; de Vries, M.G.; Cordeiro, C.A.; Westerink, B.H.C.; Verpoorte, E. Microdialysis-Coupled Enzymatic Microreactor for in vivo Glucose Monitoring in Rats. Anal. Chem. 2013, 85, 10949–10955. [Google Scholar] [CrossRef] [PubMed]
- Yu, B.; Long, N.; Moussy, Y.; Moussy, F. A long-term flexible minimally-invasive implantable glucose biosensor based on an epoxy-enhanced polyurethane membrane. Biosens. Bioelectron. 2006, 21, 2275–2282. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.G.; Song, W.H.; Burugapalli, K.; Moussy, F. Nano-yarn carbon nanotube fiber based enzymatic glucose biosensor. Nanotechnology 2010, 21, 165501–165510. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.G.; Garcia-Gancedo, L.; Flewitt, A.J.; Milne, W.I.; Moussy, F. Design of carbon nanotube fiber microelectrode for glucose biosensing. J. Chem. Technol. Biotechnol. 2012, 87, 256–262. [Google Scholar] [CrossRef]
- Al-Sagura, H.; Komathia, S.; Khanb, M.A.; Gurekc, A.G.; Hassana, A. A novel glucose sensor using lutetium phthalocyanine as redox mediator in reduced graphene oxide conducting polymer multifunctional hydrogel. Biosens. Bioelectron. 2006. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.G.; Chen, C.; Zhu, X.R.; Xie, R.S.; Flewitt, A.J.; Milne, W.I. Effects of Ni Deposition on the Electrochemical Properties of CNT/Ni Electrode and Its Application for Glucose Sensing. J. Nanosci. Nanotechnol. 2015, 15, 3196–3199. [Google Scholar] [CrossRef] [PubMed]
- El-Ads, E.H.; Galala, A.; Atta, N.F. The effect of A-site doping in a strontium palladium perovskite and its applications for non-enzymatic glucose sensing. RSC Adv. 2016, 6, 16183–16196. [Google Scholar] [CrossRef]
- Kataoka, K.; Miyazaki, H.; Bunya, M.; Okano, T.; Sakurai, Y. Totally synthetic polymer gels responding to external glucose concentration: Their preparation and application to on–off regulation of insulin release. J. Am. Chem. Soc. 1998, 120, 12694–12695. [Google Scholar] [CrossRef]
- Horkay, F.; Cho, S.H.; Tathireddy, P.; Rieth, L.; Solzbacher, F.; Magda, J. Thermodynamic analysis of the selectivity enhancement obtained by using smart hydrogels that are zwitterionic when detecting glucose with boronic acid moieties. Sens. Actuators B Chem. 2011, 160, 1363–1371. [Google Scholar] [CrossRef] [PubMed]
- Gamsey, S.; Suri, J.T.; Wessling, R.A.; Singaram, B. Continuous glucose detection using boronic acid-substituted viologens in fluorescent hydrogels: Linker effects and extension to fiber optics. Langmuir 2006, 22, 9067–9074. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.C.; Kabilan, S.; Hussain, A.; Yang, X.; Blyth, J.; Lowe, C.R. Glucose-sensitive holographic sensors for monitoring bacterial growth. Anal. Chem. 2004, 76, 5748–5755. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Pan, X.; Blyth, J.; Lowe, C.R. Towards the real-time monitoring of glucose in tear fluid: Holographic glucose sensors with reduced interference from lactate and pH. Biosens. Bioelectron. 2008, 23, 899–905. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhang, Y.; Guan, Y. New polymerized crystalline colloidal array for glucose sensing. Chem. Commun. 2009, 1, 1867–1869. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.Y.; Zhou, S.Q. A simple method to fabricate fluorescent glucose sensor based on dye-complexed microgels. Sens. Actuators B Chem. 2013, 177, 1363–1371. [Google Scholar] [CrossRef]
- Zhang, X.J.; Gao, C.M.; Lu, S.Y.; Duan, H.G.; Jing, N.N.; Dong, D.; Shi, C.F.; Liu, M.Z. Anti-photobleaching flower-like microgels as optical nanobiosensors with high selectivity at physiological conditions for continuous glucose monitoring. J. Mater. Chem. B 2014, 2, 5452–5460. [Google Scholar] [CrossRef]
- Rosenthal, S.J.; Chang, J.C.; Kovtun, O.; McBride, J.R.; Tomlinson, I.D. Biocompatible quantum dots for biological applications. Chem. Biol. 2011, 18, 10–24. [Google Scholar] [CrossRef] [PubMed]
- Schubert, K.; Khalid, W.; Yue, Z.; Parak, W.J.; Lisdat, F. Quantum-dot-modified electrode in combination with NADH-dependent dehydrogenase reactions for substrate analysis. Langmuir 2010, 26, 1395–1400. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.; Zhu, Y.; Yang, X.; Sun, J.; Li, C. Self-assembled CNTs/CdS/dehydrogenase hybrid-based amperometric biosensor triggered by photovoltaic effect. Biosens. Bioelectron. 2008, 24, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Tanne, J.; Schafer, D.; Khalid, W.; Parak, W.J.; Lisdat, F. Light-controlled bioelectrochemical sensor based on CdSe/ZnS quantum dots. Anal. Chem. 2011, 83, 7778–7785. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M.; Cui, Y.; Li, X.; Liu, S.; Tang, Z.J. Photoelectrochemical sensing of glucose based on quantum dot and enzyme nanocomposites. Electroanal. Chem. 2011, 656, 167–173. [Google Scholar] [CrossRef]
- Alrouq, F.A.; Al-Masri, A.A.; AL-Dokhi, L.M.; Alregaiey, K.A.; Bayoumy, N.M. Study of the association of adrenomedullin and basic-fibroblast growth factors with the peripheral arterial blood flow and endothelial dysfunction biomarkers in type 2 diabetic patients with peripheral vascular insufficiency. J. Biomed. Sci. 2014, 21, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Rosenbloom, A.J.; Gandhi, H.R.; Subrebost, G.L. Microdialysis coupled with an embedded systems controller and CMOS image sensor. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 1230–1233.
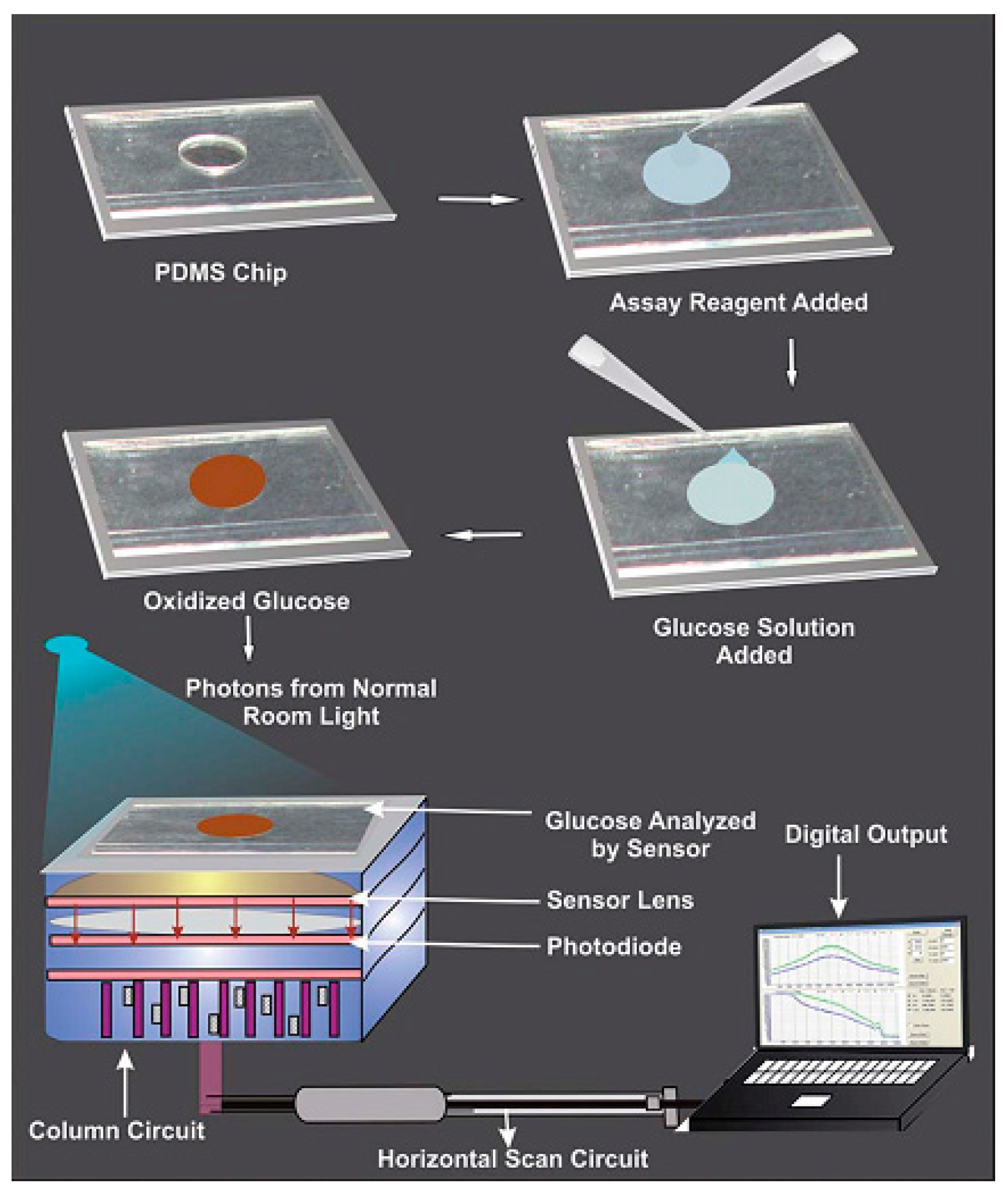
- Devadhasan, J.P.; Kim, S. Toward CMOS image sensor based glucose monitoring. Analyst 2012, 137, 3917–3920. [Google Scholar] [CrossRef] [PubMed]
- Devadhasan, J.P.; Kim, S.; Choi, C.S. CMOS image sensors as an efficient platform for glucose monitoring. Analyst 2013, 138, 5679–5684. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.Y.; Lu, M.S.C. CMOS thermal sensor arrays for enzymatic glucose detection. IEEE Sens. J. 2011, 11, 3469–3475. [Google Scholar] [CrossRef]
- Wickramasinghe, Y.; Yang, Y.; Spencer, S.A. Current Problems and Potential Techniques in In Vivo Glucose Monitoring. J. Fluoresc. 2004, 14, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Chou, Y.N.; Chang, Y.; Wen, T.C. Applying Thermosettable Zwitterionic Copolymers as General Fouling-Resistant and Thermal-Tolerant Biomaterial Interfaces. ACS Appl. Mater. Interf. 2015, 7, 10096–10107. [Google Scholar] [CrossRef] [PubMed]
- Mohsen, D.S.; Pazuki, G.; Vossoughi, M. PEGylated silica-enzyme nanoconjugates: A new frontier in large scale separation of α-amylase. Sci. Rep. 2015, 5, 18221. [Google Scholar] [CrossRef] [PubMed]
- Gerritsen, M.; Kros, A.; Sprakel, V.; Lutterman, J.A.; Nolte, R.J.M.; Jansen, J.A. Biocompatibility evaluation of sol-gel coatings for subcutaneously implantable glucose sensors. Biomaterials 2000, 21, 71–78. [Google Scholar] [CrossRef]
- Kros, A.; Gerritsen, M.; Sprakel, V.; Lutterman, J.A.; Sommerdijk, N.; Jansen, J.A.; Nolte, R.J.M. Silica-based hybrid materials as biocompatible coatings for glucose sensors. Sens. Actuators B Chem. 2001, 81, 68–75. [Google Scholar] [CrossRef]
- Jayakumar, R.; Prabaharan, M.; Nair, S.V.; Tamura, H. Novel chitin and chitosan nanofibers in biomedical applications. Biotechnol. Adv. 2010, 28, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Jayakumar, R.; Prabaharan, M.; Kumar, R.T.S.; Nair, S.V.; Tamura, H. Biomaterials based on chitin and chitosan in wound dressing applications. Biotechnol. Adv. 2011, 29, 322–337. [Google Scholar] [CrossRef] [PubMed]
- Morais, J.M.; Papadimitrakopoulos, F.; Burgess, D.J. Biomaterials/Tissue Interactions: Possible Solutions to Overcome Foreign Body Response. AAPS J. 2010, 12, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Quinn, C.A.P.; Conner, R.E.; Heller, A. Biocompatible, glucose-perme able hydrogel for in situ coating of implantable biosensors. Biomaterials 1997, 18, 1665–1670. [Google Scholar] [CrossRef]
- Chen, C.; Zhao, X.L.; Bao, H.; Liang, X.W.; Zhu, Z.G.; Zhu, Y.H. Polymerized Crystalline Colloidal Array Photonic Crystal with Enhanced Mechanical Property. Chem. Lett. 2015, 44, 1566–1568. [Google Scholar] [CrossRef]
- Heo, Y.J.; Takeucho, S. Towards Smart Tattoos: Implantable Biosensors for Continuous Glucose Monitoring. Adv. Healthc. Mater. 2013, 2, 43–56. [Google Scholar] [CrossRef] [PubMed]
- Yeh, C.C.; Venault, A.; Chang, Y. Structural effect of poly(ethylene glycol) segmental length on biofouling and hemocompatibility. Polym. J. 2016, 48, 1–8. [Google Scholar] [CrossRef]
- Wang, J. In vivo glucose monitoring: Towards ‘Sense and Act’ feedback-loop individualized medical systems. Talanta 2008, 75, 636–641. [Google Scholar] [CrossRef] [PubMed]
- Kotanen, C.N.; Moussy, F.J.; Carrara, S.; Guiseppi-Elie, A. Implantable enzyme amperometric biosensors. Biosens. Bioelectron. 2012, 35, 14–26. [Google Scholar] [CrossRef] [PubMed]
- Hickey, T.; Kreutzer, D.; Burgess, D.J.; Moussy, F. Dexamethasone/PLGA microspheres for continuous delivery of an anti-inflammatory drug for implantable medical devices. Biomaterials 2002, 23, 1649–1656. [Google Scholar] [CrossRef]
- Heo, D.N.; Song, S.J.; Kim, H.J.; Lee, Y.J.; Ko, W.K.; Lee, S.J.; Lee, D.H.; Park, S.J.; Zhang, L.J.; Kang, J.Y.; et al. Multifunctional hydrogel coatings on the surface of neural cuff electrode for improving electrode-nerve tissue interfaces. Acta Biomater. 2016, 39, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Avula, M.; Jones, D.; Rao, A.N.; McClain, D.; McGill, L.D.; Grainger, D.W.; Solzbacher, F. Local release of masitinib alters in vivo implantable continuous glucose sensor performance. Biosens. Bioelectron. 2016, 77, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.Y.; Zhu, Z.G.; Chen, C.; Li, Z.H.; Chen, Y.X. The implantable glucose biosensor based on the spiral-type Pt-Ir electrode. Chin. J. Sens. Actuators 2016, 29, 9–14. [Google Scholar]
- Yu, D.H.; Sun, C.L.; Zheng, Z.Z.; Wang, X.L.; Chen, D.Y.; Wu, H.; Wang, X.Q.; Shi, F.X. Inner ear delivery of dexamethasone using injectable silk-polyethylene glycol (PEG) hydrogel. Int. J. Pharm. 2016, 503, 229–237. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, C.; Efron, N. Diabetes and contact lens wear. Clin. Exp. Optom. 2012, 95, 328–337. [Google Scholar] [CrossRef] [PubMed]
- Mann, A.; Tighe, B. Contact lens interactions with the tear film. Exp. Eye Res. 2013, 117, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Yao, H.F.; Shum, A.J.; Cowan, M.; Lähdesmäki, I.; Parviz, B.A. A contact lens with embedded sensor for monitoring tear glucose level. Biosens. Bioelectron. 2011, 26, 3290–3296. [Google Scholar] [CrossRef] [PubMed]
- Chu, M.X.; Miyajima, K.; Takahashi, D.; Arakawa, T.; Sano, K.; Sawada, X.; Kudo, H.; Iwasaki, Y.; Akiyoshi, K.; Mochizuki, M.; et al. Soft contact lens biosensor for in situ monitoring of tear glucose as non-invasive blood sugar assessment. Talanta 2011, 83, 960–965. [Google Scholar] [CrossRef] [PubMed]
- Alexeev, V.L.; Sharma, A.C.; Goponenko, A.V.; Das, S.; Lednev, I.K.; Wilcox, C.S.; Finegold, D.N.; Asher, S.A. High Ionic Strength Glucose-Sensing Photonic Crystal. Anal. Chem. 2003, 75, 2316–2323. [Google Scholar] [CrossRef] [PubMed]
- Ben-Moshe, M.; Alexeev, V.L.; Asher, S.A. Fast Responsive Crystalline Colloidal Array Photonic Crystal Glucose Sensors. Anal. Chem. 2006, 78, 5149–5157. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.J.; Cano, G.G.; Braun, P.V. Linear and Fast Hydrogel Glucose Sensor Materials Enabled by Volume Resetting Agents. Adv. Mater. 2014, 26, 5678–5683. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.M.; Jiang, X.M.; Zhang, L.Y.; Fan, J.; Wu, W.T. Construction of near-infrared photonic crystal glucose-sensing materials for ratiometric sensing of glucose in tears. Biosens. Bioelectron. 2013, 48, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhu, J.; Akhter, K.F.; Thomas, A.A. Encapsulation of BSA within Gelatin Nanoparticles-laden Biopolymer Film. Mater. Res. Soc. Symp. Proc. 2010. [Google Scholar] [CrossRef]
- Amer, S.; Yousuf, M.; Siddqiui, P.Q.; Alam, J. Salivary glucose concentrations in patients with diabetes mellitus-a minimally invasive technique for monitoring blood glucose levels. Pak. J. Pharm. Sci. 2001, 14, 33–37. [Google Scholar] [PubMed]
- Chavez, E.M.; Borrell, L.N.; Taylor, G.W.; Ship, J.A. A longitudinal analysis of salivary flow in control subjects and older adults with type 2 diabetes. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2001, 91, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Lopez, M.E.; Colloca, M.E.; Paez, R.G.; Schallmach, J.N.; Koss, M.A.; Chervonagura, A. Salivary characteristics of diabetic children. Braz. Dent. J. 2003, 14, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Aydin, S. A comparison of ghrelin, glucose, alpha-amylase and protein levels in saliva from diabetics. J. Biochem. Mol. Biol. 2007, 40, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Imani, S.; de Araujo, W.R.; Warchall, J.; Valdes-Ramirez, G.; Paixao, T.R.L.C.; Mercier, P.P.; Wang, J. Wearable salivary uric acid mouthguard biosensor with integrated wireless electronics. Biosens. Bioelectron. 2015, 74, 1061–1068. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, M.; Mitsumori, M.; Kano, Y. Noninvasively measuring blood glucose using saliva. IEEE Eng. Med. Biol. Mag. 1998, 17, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Abikshyeet, P.; Ramesh, V.; Oza, N. Glucose estimation in the salivary secretion of diabetes mellitus patients. Targets Ther. 2012, 5, 149–154. [Google Scholar]
- Liu, C.; Sheng, Y.; Sun, Y.; Feng, J.; Wang, S.; Zhang, J.; Xu, J.; Jiang, D. A glucose oxidase-coupled DNAzyme sensor for glucose detection in tears and saliva. Biosens. Bioelectron. 2015, 70, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Soni, A.; Jha, S.K. A paper strip based non-invasive glucose biosensor for salivary analysis. Biosens. Bioelectron. 2015, 67, 763–768. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Du, Y.; Wang, M.L. On-chip highly sensitive saliva glucose sensing using multilayer films composed of single-walled carbon nanotubes, gold nanoparticles, and glucose oxidase. Sens. Bio-Sens. Res. 2015, 4, 96–102. [Google Scholar] [CrossRef]
- Lambert, J.L.; Borchert, M.S. Assessijng Blood Brain Barrier Dynamics or Identifying or Measuring Selected Substances or Toxins in a Subject by Analyzing Raman Spectrum Signals of Selected Regions in the Eye. U.S. Patent 6,574,501, 3 June 2003. [Google Scholar]
- Lipson, J.; Bernhardt, J.; Block, U.; Freeman, W.R.; Hofmeister, R.; Hristakeva, M.; Lenosky, T.; McNamara, R.; Petrasek, D.; Veltkamp, D. Requirements for calibration in naninvaive glucose monitoring by Raman spectroscopy. J. Diabetes Sci. Technol. 2009, 3, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Bonato, P. Wearable sensors and systems. IEEE Eng. Med. Biol. Mag. 2010, 293, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Buller, M.; Welles, A.; Jenkins, O.C.; Hoyt, R. Extreme health sensing: The challenges, technologies, and strategies for active health sustainment of military personnel during training and combat missions. Proc. SPIE 2010. [Google Scholar] [CrossRef]
- Jia, W.; Bandodkar, A.J.; Valdes-Ramirez, G.; Windmiller, J.R.; Yang, Z.; Ramirez, J.; Chan, G.; Wang, J. Electrochemical Tattoo Biosensors for Real-Time Noninvasive Lactate Monitoring in Human Perspiration. Anal. Chem. 2013, 85, 6553–6560. [Google Scholar] [CrossRef] [PubMed]
- Thomas, N.; Lahdesmaki, I.; Parviz, B.A. A contact lens with an integrated lactate sensor. Sens. Actuators B Chem. 2012, 162, 128–134. [Google Scholar] [CrossRef]
- Schabmueller, C.G.J.; Loppow, D.; Piechotta, G.; Schutze, B.; Albers, J.; Hintsche, R. Micromachined sensor for lactate monitoring in saliva. Biosens. Bioelectron. 2006, 21, 1770–1776. [Google Scholar] [CrossRef] [PubMed]
- Claver, J.B.; Miron, M.C.V.; Capitan-Vallvey, L.F. Disposable electrochemiluminescent biosensor for lactate determination in saliva. Analyst 2009, 134, 1423–1432. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Valdes-Ramirez, G.; Bandodkar, A.J.; Jia, W.Z.; Martinez, A.G.; Ramirez, J.; Mercier, P.; Wang, J. Non-invasive mouthguard biosensor for continuous salivary monitoring of metabolites. Analyst 2014, 139, 1632–1636. [Google Scholar] [CrossRef] [PubMed]
- Arakawa, T.; Kuroki, Y.; Nitta, H.; Chouhan, P.; Toma, K.; Sawada, S.; Takeuchi, S.; Sekita, T.; Akiyoshi, K.; Minakuchi, S.; et al. Mouthguard biosensor with telemetry system for monitoring of saliva glucose: A novel cavitas sensor. Biosens. Bioelectron. 2016, 84, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Luchansky, M.S.; Bailey, R.C. High-Q Optical Sensors for Chemical and Biological Analysis. Anal. Chem. 2012, 84, 793–821. [Google Scholar] [CrossRef] [PubMed]
- Paek, S.H.; Cho, I.H.; Kim, D.H.; Jeon, J.W.; Lim, G.S.; Paek, S.H. Label-free, needle-type biosensor for continuous glucose monitoring based on competitive binding. Biosens. Bioelectron. 2013, 40, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Cummins, B.; Garza, J.; Cote, G. Optimization of a Concanavalin A-Based Glucose Sensor Using Fluorescence Anisotropy. Anal. Chem. 2013, 85, 5397–5404. [Google Scholar] [CrossRef] [PubMed]
- Shen, P.F.; Xia, Y.S. Synthesis-Modification Integration: One-Step Fabrication of Boronic Acid Functionalized Carbon Dots for Fluorescent Blood Sugar Sensing. Anal. Chem. 2014, 86, 5323–5329. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, G.; Chen, J.; Parisi, J.; Bruckner, C.; Yao, X.D.; Lei, Y. An Injectable PEG-BSA-Coumarin-GOx Hydrogel for Fluorescence Turn-on Glucose Detection. Appl. Biochem. Biotechnol. 2015, 5, 1115–1126. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, R.; Jayant, R.D.; Chaudhary, A.; Mcshane, M.J. “Smart Tattoo” Glucose Biosensors and Effect of Coencapsulated Anti-inflammatory Agents. J. Diabetes Sci. Technol. 2011, 1, 76–85. [Google Scholar] [CrossRef]
- Wang, H.C.; Lee, A.R. Recent developments in blood glucose sensors. J. Food. Drug. Anal. 2015, 2, 191–200. [Google Scholar] [CrossRef]
- Ferrari, M.; Quaresima, V. A brief review on the history of human functional near-infrared spectroscopy (fNIRS) development and fields of application. Neurolmage 2012, 63, 921–935. [Google Scholar] [CrossRef] [PubMed]
- So, C.F.; Choi, K.S.; Wong, T.K.S.; Chung, J.W.Y. Recent advances in noninvasive glucose monitoring. Med. Devices 2012, 5, 45–52. [Google Scholar]
- Vashist, S.K. Non-invasive glucose monitoring technology in diabetes management: A review. Anal. Chim. Acta 2012, 750, 16–27. [Google Scholar] [CrossRef] [PubMed]
- Hazen, K.H.; Arnold, M.A.; Small, G.W. Measurement of glucose in water with first-overtone near-infrared spectra. Appl. Spectrosc. 1998, 52, 1597–1605. [Google Scholar] [CrossRef]
- Genina, E.A.; Bashkatov, A.N.; Sinichkin, Y.P.; Yanina, I.Y.; Tuchin, V.V. Optical clearing of biological tissues: Prospects of application in medical diagnostics and phototherapy. J. Biomed. Photonics Eng. 2015, 1, 24–58. [Google Scholar] [CrossRef]
- Stiles, P.L.; Dieringer, J.A.; Shah, N.C.; Van Duyne, R.P. Surface-enhanced Raman spectroscopy. Anal. Chem. 2008, 1, 601–626. [Google Scholar] [CrossRef] [PubMed]
- Torul, H.; Ciftci, H.; Dudak, F.C.; Adiguzel, Y.; Kulah, H.; Boyaci, I.H.; Tamer, U. Glucose determination based on a two component self-assembled monolayer functionalized surfaceenhanced Raman spectroscopy (SERS) probe. Anal. Methods 2014, 6, 5097–5104. [Google Scholar] [CrossRef]
- Kong, K.V.; Ho, C.J.H.; Gong, F.X.; Lau, W.K.O. Sensitive SERS glucose sensing in biological media using alkyne functionalized boronic acid on planar substrates. Biosens. Bioelectron. 2014, 56, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.M.; Reyes, C.; Lopez, G.P. Common causes of glucose oxidase instability in in vivo biosensing: A brief review. J. Diabetes Sci. Technol. 2013, 7, 1030–1038. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Polymer | Characters | Formation | Applications |
|---|---|---|---|
| Natural | |||
| Alginate | Immobilization of glucose oxidase | Hydrogel and membrane | Drug delivery |
| Collagen | Extracellular matrix component | Hydrogel, membrane and sponge | Scaffolds |
| Semisynthetic | |||
| Chitin, Chitosan | Hydrogel, membrane and fiber | Anti-microbial and drug delivery | |
| Synthetic | |||
| PLGA | Negligible protein adsorption | Micelle and hydrogel | Coating, drug delivery and scaffolds |
| PHEMA | Negligible protein adsorption | Hydrogel | Coating |
| PVA | Geltaion and mechanical properties | Hydrogel, membrane and sponge | Coating and drug delivery |
| PEG | Negligible protein adsorption | Hydrogel and membrane | Coating and drug delivery |
| PEGMA | Negligible protein adsorption | Hydrogel | Coating |
© 2017 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.; Zhao, X.-L.; Li, Z.-H.; Zhu, Z.-G.; Qian, S.-H.; Flewitt, A.J. Current and Emerging Technology for Continuous Glucose Monitoring. Sensors 2017, 17, 182. https://doi.org/10.3390/s17010182
Chen C, Zhao X-L, Li Z-H, Zhu Z-G, Qian S-H, Flewitt AJ. Current and Emerging Technology for Continuous Glucose Monitoring. Sensors. 2017; 17(1):182. https://doi.org/10.3390/s17010182
Chicago/Turabian StyleChen, Cheng, Xue-Ling Zhao, Zhan-Hong Li, Zhi-Gang Zhu, Shao-Hong Qian, and Andrew J. Flewitt. 2017. "Current and Emerging Technology for Continuous Glucose Monitoring" Sensors 17, no. 1: 182. https://doi.org/10.3390/s17010182