
A Vibrotactile and Plantar Force Measurement-Based Biofeedback System: Paving the Way towards Wearable Balance-Improving Devices

 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Experimental Section
2.1. Participants

{kind=link}
{kind=link}
| [Mean ± SD] | Older Subjects (n = 15) | Young Subjects (n = 15) |
|---|---|---|
| Age (years) | 70.1 ± 3.7 | 26.7 ± 2.9 |
| Gender | 6 females and 9 males | 7 females and 8 males |
| Height (cm) | 160.6 ± 7.6 | 167.6 ± 5.8 |
| Weight (kg) | 61.7 ± 11.4 | 61.4 ± 11.2 |
2.2. The Vibrotactile Biofeedback System

2.3. Experimental Design and Procedures
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results and Discussion
3.1. Results
| Monofilament Scores (Mean ± SD) | |||||||
|---|---|---|---|---|---|---|---|
| Elderly Subjects (n = 15) | Young Subjects (n = 15) | ||||||
| Position | Without socks | With socks | p-value | Position | Without socks | With socks | p-value |
| Hallux | 3.0 ± 0.0 | 1.1 ± 0.4 | <0.001 | Hallux | 3.0 ± 0.0 | 1.0 ± 0.0 | <0.001 |
| 1st metatarsal head | 2.9 ± 0.3 | 1.0 ± 0.0 | <0.001 | 1st metatarsal head | 3.0 ± 0.0 | 1.0 ± 0.0 | <0.001 |
| 5th metatarsal head | 2.7 ± 0.8 | 1.0 ± 0.0 | <0.001 | 5th metatarsal head | 3.0 ± 0.0 | 1.0 ± 0.0 | <0.001 |
| Average | 2.9 ± 0.4 | 1.0 ± 0.1 | <0.001 | Average | 3.0 ± 0.0 | 1.0 ± 0.0 | <0.001 |

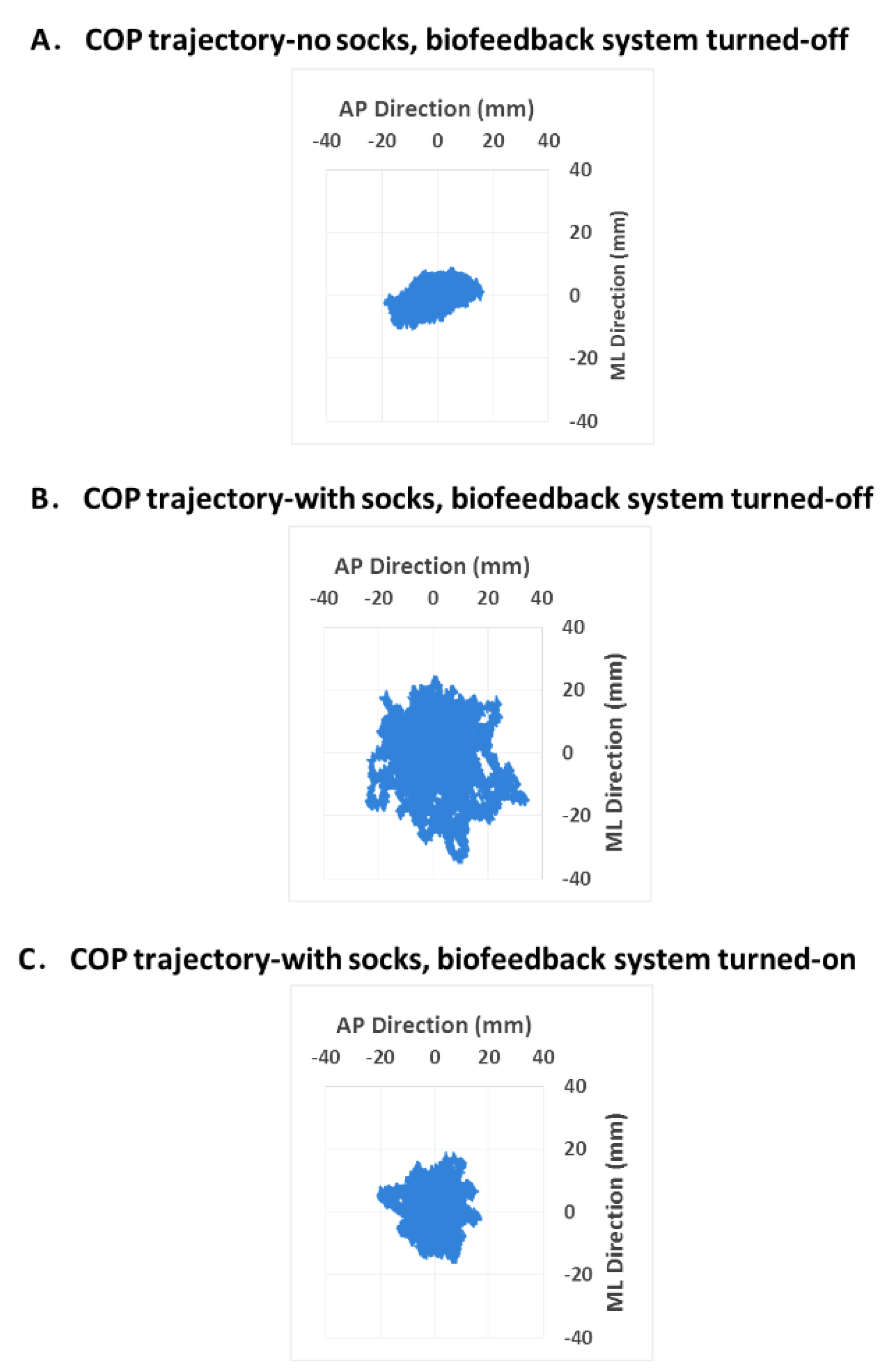
| Young and Elderly Subjects (n = 30) | Condition 2 Minus Condition 1 | Condition 3 Minus Condition 2 | |||||
|---|---|---|---|---|---|---|---|
| COP parameters (mean ± SD) | No socks, biofeedback system turned-off (condition 1) | With socks, biofeedback system turned-off (condition 2) | With socks, biofeedback system turned-on (condition 3) | Difference | p-value | Difference | p-value |
| Mean Distance (mm) | 6.68 ± 1.89 | 8.30 ± 1.94 | 7.24 ± 2.11 | +24.2% | 0.000 | −12.7% | 0.000 |
| Root Mean Square Distance (mm) | 7.67 ± 2.18 | 9.57 ± 2.29 | 8.26 ± 2.48 | +24.8% | 0.000 | −13.7% | 0.000 |
| 95% Confidence Circle Area (mm2) | 568.12 ± 383.74 | 876.52 ± 516.33 | 660.86 ± 516.28 | +54.3% | 0.000 | −24.6% | 0.000 |
| 95% Confidence Ellipse Area (mm2) | 550.47 ± 392.19 | 861.38 ± 490.55 | 668.10 ± 500.98 | +56.5% | 0.000 | −22.4% | 0.000 |
| Planar Diameter- 95% Confidence Circle Area (mm) | 25.69 ± 7.38 | 32.19 ± 7.93 | 27.50 ± 8.53 | +25.3% | 0.000 | −14.6% | 0.000 |
| Planar Diameter- 95% Confidence Ellipse Area (mm) | 25.20 ± 7.58 | 31.99 ± 7.85 | 27.73 ± 8.37 | +26.9% | 0.000 | −13.3% | 0.000 |
| Mediolateral Range of COP (mm) | 34.44 ± 11.60 | 46.91 ± 11.41 | 38.32 ± 9.38 | +36.2% | 0.000 | −18.3% | 0.000 |
| Anteroposterior Range of COP (mm) | 38.40 ± 10.00 | 45.84 ± 9.96 | 39.60 ± 12.09 | +19.4% | 0.000 | −13.6% | 0.001 |
3.2. Discussion
4. Conclusions/Outlook
Acknowledgments
Author Contributions
Conflicts of Interests
References
- Tinetti, M.E. Preventing falls in elderly persons. N. Engl. J. Med. 2003, 348, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Saverino, A.; Moriarty, A.; Rantell, K.; Waller, D.; Ayres, R.; Playford, D. A qualitative description of falls in a neuro-rehabilitation unit: The use of a standardised fall report including the international classification of functioning (icf) to describe activities and environmental factors. Disabil. Rehabil. 2014, 37, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kannus, P.; Sievänen, H.; Palvanen, M.; Järvinen, T.; Parkkari, J. Prevention of falls and consequent injuries in elderly people. The Lancet 2005, 366, 1885–1893. [Google Scholar] [CrossRef]
- Todd, C.; Skelton, D. What Are the Main Risk Factors for Falls amongst Older People and What Are the most Effective Interventions to Prevent these Falls? How should Interventions to Prevent Falls Be Implemented; World Health Organization Europe: Copenhagen, Denmark, 2004. [Google Scholar]
- Rubenstein, L.Z. Falls in older people: Epidemiology, risk factors and strategies for prevention. Age Ageing 2006, 35, ii37–ii41. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, L.Z.; Josephson, K.R. The epidemiology of falls and syncope. Clin. Geriatr. Med. 2002, 18, 141–158. [Google Scholar] [CrossRef]
- Salzman, B. Gait and balance disorders in older adults. Am. Fam. Physician 2010, 82, 61–68. [Google Scholar] [PubMed]
- DiStefano, L.J.; Clark, M.A.; Padua, D.A. Evidence supporting balance training in healthy individuals: A systemic review. J. Strength Cond. Res. 2009, 23, 2718–2731. [Google Scholar] [CrossRef] [PubMed]
- Zijlstra, A.; Mancini, M.; Chiari, L.; Zijlstra, W. Biofeedback for training balance and mobility tasks in older populations: A systematic review. J Neuroeng. Rehabil. 2010, 7. [Google Scholar] [CrossRef] [PubMed]
- Vuillerme, N.; Chenu, O.; Demongeot, J.; Payan, Y. Controlling posture using a plantar pressure-based, tongue-placed tactile biofeedback system. Exp. Brain Res. 2007, 179, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Hijmans, J.M.; Geertzen, J.; Zijlstra, W.; Hof, A.L.; Postema, K. Effects of vibrating insoles on standing balance in diabetic neuropathy. J. Rehabil. Res. Dev. 2008, 45, 1442–1450. [Google Scholar] [CrossRef]
- Priplata, A.A.; Niemi, J.B.; Harry, J.D.; Lipsitz, L.A.; Collins, J.J. Vibrating insoles and balance control in elderly people. The Lancet 2003, 362, 1123–1124. [Google Scholar] [CrossRef]
- Dozza, M.; Horak, F.B.; Chiari, L. Auditory biofeedback substitutes for loss of sensory information in maintaining stance. Exp. Brain Res. 2007, 178, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Kojima, S.; Takeda, H.; Ino, S.; Ifukube, T. The influence of moving auditory stimuli on standing balance in healthy young adults and the elderly. Ergonomics 2001, 44, 1403–1412. [Google Scholar] [CrossRef] [PubMed]
- Sienko, K.H.; Balkwill, M.D.; Wall, C. Biofeedback improves postural control recovery from multi-axis discrete perturbations. J. Neuroeng. Rehabil. 2012, 9, 53. [Google Scholar] [CrossRef] [PubMed]
- Goebel, J.A.; Sinks, B.C.; Parker, B.E., Jr.; Richardson, N.T.; Olowin, A.B.; Cholewiak, R.W. Effectiveness of head-mounted vibrotactile stimulation in subjects with bilateral vestibular loss: A phase 1 clinical trial. Otol. Neurotol. 2009, 30, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.-C.; Kim, J.; Chen, S.; Sienko, K.H. Cell phone based balance trainer. J. Neuroeng. Rehabil. 2012, 9, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Nanhoe-Mahabier, W.; Allum, J.; Pasman, E.; Overeem, S.; Bloem, B. The effects of vibrotactile biofeedback training on trunk sway in parkinson’s disease patients. Parkinsonism Relat. Disord. 2012, 18, 1017–1021. [Google Scholar] [CrossRef] [PubMed]
- Sienko, K.H.; Balkwill, M.D.; Oddsson, L.; Wall, C. Effects of multi-directional vibrotactile feedback on vestibular-deficient postural performance during continuous multi-directional support surface perturbations. J. Vestib. Res. 2008, 18, 273–285. [Google Scholar] [PubMed]
- Rossi-Izquierdo, M.; Ernst, A.; Soto-Varela, A.; Santos-Pérez, S.; Faraldo-García, A.; Sesar-Ignacio, Á.; Basta, D. Vibrotactile neurofeedback balance training in patients with parkinson's disease: Reducing the number of falls. Gait Posture 2013, 37, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Sienko, K.H.; Balkwill, M.D.; Oddsson, L.I.; Wall, C. The effect of vibrotactile feedback on postural sway during locomotor activities. J. Neuroeng. Rehabil. 2013, 10. [Google Scholar] [CrossRef] [PubMed]
- Wall, C.; Wrisley, D.M.; Statler, K.D. Vibrotactile tilt feedback improves dynamic gait index: A fall risk indicator in older adults. Gait Posture 2009, 30, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Wall, C.; Weinberg, M.S. Balance prostheses for postural control. IEEE Eng. Med. Biol. Mag. 2003, 22, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Nitz, J.; Kuys, S.; Isles, R.; Fu, S. Is the wii fit™ a new-generation tool for improving balance, health and well-being? A pilot study. Climacteric 2010, 13, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Esculier, J.-F.; Vaudrin, J.; Beriault, P.; Gagnon, K.; Tremblay, L.E. Home-based balance training programme using wii fit with balance board for parkinson’s disease: A pilot study. J. Rehabil. Med. 2012, 44, 144–150. [Google Scholar] [PubMed]
- Koslucher, F.; Wade, M.G.; Nelson, B.; Lim, K.; Chen, F.C.; Stoffregen, T.A. Nintendo wii balance board is sensitive to effects of visual tasks on standing sway in healthy elderly adults. GaitPosture 2012, 36, 605–608. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.D.; Chang, W.Y.; Lee, C.L.; Feng, C.Y. Validity and reliability of wii fit balance board for the assessment of balance of healthy young adults and the elderly. J. Phys. Ther. Sci. 2013, 25, 1251–1253. [Google Scholar] [CrossRef] [PubMed]
- Dozza, M.; Chiari, L.; Horak, F.B. Audio-biofeedback improves balance in patients with bilateral vestibular loss. Arch. Phys. Med. Rehabil. 2005, 86, 1401–1403. [Google Scholar] [CrossRef] [PubMed]
- Madureira, M.M.; Takayama, L.; Gallinaro, A.; Caparbo, V.; Costa, R.; Pereira, R.M. Balance training program is highly effective in improving functional status and reducing the risk of falls in elderly women with osteoporosis: A randomized controlled trial. Osteoporos. Int. 2007, 18, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Liu-Ambrose, T.; Donaldson, M.G.; Ahamed, Y.; Graf, P.; Cook, W.L.; Close, J.; Lord, S.R.; Khan, K.M. Otago home-based strength and balance retraining improves executive functioning in older fallers: A randomized controlled trial. J. Am. Geriatr. Soc. 2008, 56, 1821–1830. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.C.; Robertson, M.C.; Ashe, M.C.; Liu-Ambrose, T.; Khan, K.M.; Marra, C.A. Does a home based strength and balance programme in people aged ≥ 80 years provide the best value for money to prevent falls? A systematic review of economic analyses of falls prevention interventions. Br. J. Sports Med. 2009. [Google Scholar] [CrossRef] [PubMed]
- Hatton, A.L.; Rome, K.; Dixon, J.; Martin, D.J.; McKeon, P.O. Footwear interventions a review of their sensorimotor and mechanical effects on balance performance and gait in older adults. J. Am. Podiatr. Med. Assoc. 2013, 103, 516–533. [Google Scholar] [CrossRef] [PubMed]
- Hijmans, J.M.; Geertzen, J.H.; Schokker, B.; Postema, K. Development of vibrating insoles. Int. J. Rehabil. Res. 2007, 30, 343–345. [Google Scholar] [CrossRef] [PubMed]
- Priplata, A.A.; Niemi, J.B.; Veves, A.; Lipsitz, L.A.; Collins, J.J. Vibrating insoles improve balance in diabetic patients with peripheral neuropathy. Med. Sci. Sports Exerc. 2004, 36. [Google Scholar] [CrossRef]
- Ruhe, A.; Fejer, R.; Walker, B. The test–retest reliability of centre of pressure measures in bipedal static task conditions–a systematic review of the literature. Gait Posture 2010, 32, 436–445. [Google Scholar] [CrossRef] [PubMed]
- Moghadam, M.; Ashayeri, H.; Salavati, M.; Sarafzadeh, J.; Taghipoor, K.D.; Saeedi, A.; Salehi, R. Reliability of center of pressure measures of postural stability in healthy older adults: Effects of postural task difficulty and cognitive load. Gait Posture 2011, 33, 651–655. [Google Scholar] [CrossRef] [PubMed]
- Prieto, T.E.; Myklebust, J.; Hoffmann, R.; Lovett, E.; Myklebust, B. Measures of postural steadiness: Differences between healthy young and elderly adults. IEEE Trans. Biomed. Eng. 1996, 43, 956–966. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.R.; Campbell, A.D.; Adkin, A.L.; Carpenter, M.G. The relationship between fear of falling and human postural control. Gait Posture 2009, 29, 275–279. [Google Scholar] [CrossRef] [PubMed]
- Melzer, I.; Kurz, I.; Oddsson, L.I.E. A retrospective analysis of balance control parameters in elderly fallers and non-fallers. Clin. Biomech. 2010, 25, 984–988. [Google Scholar] [CrossRef] [PubMed]
- Kyung, K.-U.; Ahn, M.; Kwon, D.-S.; Srinivasan, M. Perceptual and biomechanical frequency response of human skin: Implication for design of tactile displays. In Proceedings of the First Joint Eurohaptics Conference and Symposium on Haptic Interfaces for Virtual Environment and Teleoperator Systems, Pisa, Italy, 18–20 March 2005; pp. 96–101.
- Agrawal, Y.; Carey, J.P.; Hoffman, H.J.; Sklare, D.A.; Schubert, M.C. The modified romberg balance test: Normative data in us adults. Otol. Neurotol. 2011, 32, 1309–1311. [Google Scholar] [CrossRef] [PubMed]
- Hatton, A.L.; Sturnieks, D.L.; Lord, S.R.; Lo, J.C.; Menz, H.B.; Menant, J.C. Effects of nonslip socks on the gait patterns of older people when walking on a slippery surface. J. Am. Podiatr. Med. Assoc. 2013, 103, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Menant, J.C.; Steele, J.R.; Menz, H.B.; Munro, B.J.; Lord, S.R. Optimizing footwear for older people at risk of falls. J. Rehabil. Res. Dev. 2008, 45, 1167–1181. [Google Scholar] [CrossRef] [PubMed]
- Perry, S.D. Evaluation of age-related plantar-surface insensitivity and onset age of advanced insensitivity in older adults using vibratory and touch sensation tests. Neurosci. lett. 2006, 392, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Höhne, A.; Ali, S.; Stark, C.; Brüggemann, G.-P. Reduced plantar cutaneous sensation modifies gait dynamics, lower-limb kinematics and muscle activity during walking. Eur. J. Appl. Phys. 2012, 112, 3829–3838. [Google Scholar] [CrossRef] [PubMed]
- Slater, R.A.; Koren, S.; Ramot, Y.; Buchs, A.; Rapoport, M.J. Interpreting the results of the semmes-weinstein monofilament test: Accounting for false-positive answers in the international consensus on the diabetic foot protocol by a new model. Diabet. Metab. Res. Rev. 2014, 30, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Zakas, A. Bilateral isokinetic peak torque of quadriceps and hamstring muscles in professional soccer players with dominance on one or both two sides. J. Sports Med. Phys. Fit. 2006, 46, 28. [Google Scholar]
- Nurse, M.A.; Nigg, B.M. The effect of changes in foot sensation on plantar pressure and muscle activity. Clin. Biomech. 2001, 16, 719–727. [Google Scholar] [CrossRef]
- Tsai, Y.-J.; Lin, S.-I. Older adults adopted more cautious gait patterns when walking in socks than barefoot. Gait Posture 2013, 37, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Prasansuk, S.; Siriyananda, C.; Nakorn, A.N.; Atipas, S.; Chongvisal, S. Balance disorders in the elderly and the benefit of balance exercise. J. Med. Assoc. Thail. Chotmaihet Thangphaet 2004, 87, 1225–1233. [Google Scholar]
- Hennig, E.M.; Sterzing, T. Sensitivity mapping of the human foot: Thresholds at 30 skin locations. Foot Ankle Int. 2009, 30, 986–991. [Google Scholar] [CrossRef] [PubMed]
- Bronstein, A.M.; Brandt, T.; Woollacott, M.H.; Nutt, J.G. Clinical Disorders of Balance, Posture and Gait; CRC Press: Boca Raton, FL, USA, 2004. [Google Scholar]
- Merlo, A.; Zemp, D.; Zanda, E.; Rocchi, S.; Meroni, F.; Tettamanti, M.; Recchia, A.; Lucca, U.; Quadri, P. Postural stability and history of falls in cognitively able older adults: The canton ticino study. Gait Posture 2012, 36, 662–666. [Google Scholar] [CrossRef] [PubMed]
- Wu, G. Evaluation of the effectiveness of tai chi for improving balance and preventing falls in the older population—A review. J. Am. Geriatr. Soc. 2002, 50, 746–754. [Google Scholar] [CrossRef] [PubMed]
- Lord, S.R. Falls in Older People: Risk Factors and Strategies for Prevention; Cambridge University Press: Cambridge, MA, USA, 2007. [Google Scholar]
- Kwan, M.M.S.; Close, J.C.; Wong, A.K.W.; Lord, S.R. Falls incidence, risk factors, and consequences in chinese older people: A systematic review. J. Am. Geriatr. Soc. 2011, 59, 536–543. [Google Scholar] [CrossRef] [PubMed]
- Delbaere, K.; Close, J.C.; Heim, J.; Sachdev, P.S.; Brodaty, H.; Slavin, M.J.; Kochan, N.A.; Lord, S.R. A multifactorial approach to understanding fall risk in older people. J. Am. Geriatr. Soc. 2010, 58, 1679–1685. [Google Scholar] [CrossRef] [PubMed]
- Perry, S.D.; Radtke, A.; McIlroy, W.E.; Fernie, G.R.; Maki, B.E. Efficacy and effectiveness of a balance-enhancing insole. J. Gerontol. Ser. A: Biol. Sci. Med.Sci. 2008, 63, 595–602. [Google Scholar] [CrossRef]
- Maki, B.E.; Sibley, K.M.; Jaglal, S.B.; Bayley, M.; Brooks, D.; Fernie, G.R.; Flint, A.J.; Gage, W.; Liu, B.A.; McIlroy, W.E. Reducing fall risk by improving balance control: Development, evaluation and knowledge-translation of new approaches. J. Saf. Res. 2011, 42, 473–485. [Google Scholar] [CrossRef] [PubMed]
- Aruin, A.S.; Kanekar, N. Effect of a textured insole on balance and gait symmetry. Exp. Brain Res. 2013, 231, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Wall III, C. Application of vibrotactile feedback of body motion to improve rehabilitation in individuals with imbalance. J. Neurol. Phys. Ther.: JNPT 2010, 34, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Janssen, M.; Stokroos, R.; Aarts, J.; van Lummel, R.; Kingma, H. Salient and placebo vibrotactile feedback are equally effective in reducing sway in bilateral vestibular loss patients. Gait Posture 2010, 31, 213–217. [Google Scholar] [CrossRef] [PubMed]
- Haggerty, S.; Jiang, L.-T.; Galecki, A.; Sienko, K.H. Effects of biofeedback on secondary-task response time and postural stability in older adults. Gait Posture 2012, 35, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Grampp, J.; Willson, J.; Kernozek, T. The plantar loading variations to uphill and downhill gradients during treadmill walking. Foot Ankle Int. 2000, 21, 227–231. [Google Scholar] [PubMed]
- Chen, C.; Hong, P.; Chen, C.; Chou, S.W.; Wu, C.; Cheng, P.; Tang, F.; Chen, H. Ground reaction force patterns in stroke patients with various degrees of motor recovery determined by plantar dynamic analysis. Chang Gung Med. J. 2007, 30, 62–72. [Google Scholar] [PubMed]
- Lewek, M.D.; Bradley, C.E.; Wutzke, C.J.; Zinder, S.M. The relationship between spatiotemporal gait asymmetry and balance in individuals with chronic stroke. J. Appl. Biomech. 2014, 30, 31–36. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, C.Z.-H.; Wan, A.H.-P.; Wong, D.W.-C.; Zheng, Y.-P.; Lee, W.C.-C. A Vibrotactile and Plantar Force Measurement-Based Biofeedback System: Paving the Way towards Wearable Balance-Improving Devices. Sensors 2015, 15, 31709-31722. https://doi.org/10.3390/s151229883
Ma CZ-H, Wan AH-P, Wong DW-C, Zheng Y-P, Lee WC-C. A Vibrotactile and Plantar Force Measurement-Based Biofeedback System: Paving the Way towards Wearable Balance-Improving Devices. Sensors. 2015; 15(12):31709-31722. https://doi.org/10.3390/s151229883
Chicago/Turabian StyleMa, Christina Zong-Hao, Anson Hong-Ping Wan, Duo Wai-Chi Wong, Yong-Ping Zheng, and Winson Chiu-Chun Lee. 2015. "A Vibrotactile and Plantar Force Measurement-Based Biofeedback System: Paving the Way towards Wearable Balance-Improving Devices" Sensors 15, no. 12: 31709-31722. https://doi.org/10.3390/s151229883