Low P16INK4A Expression Associated with High Expression of Cancer Stem Cell Markers Predicts Poor Prognosis in Cervical Cancer after Radiotherapy


Abstract
:
1. Introduction
2. Results
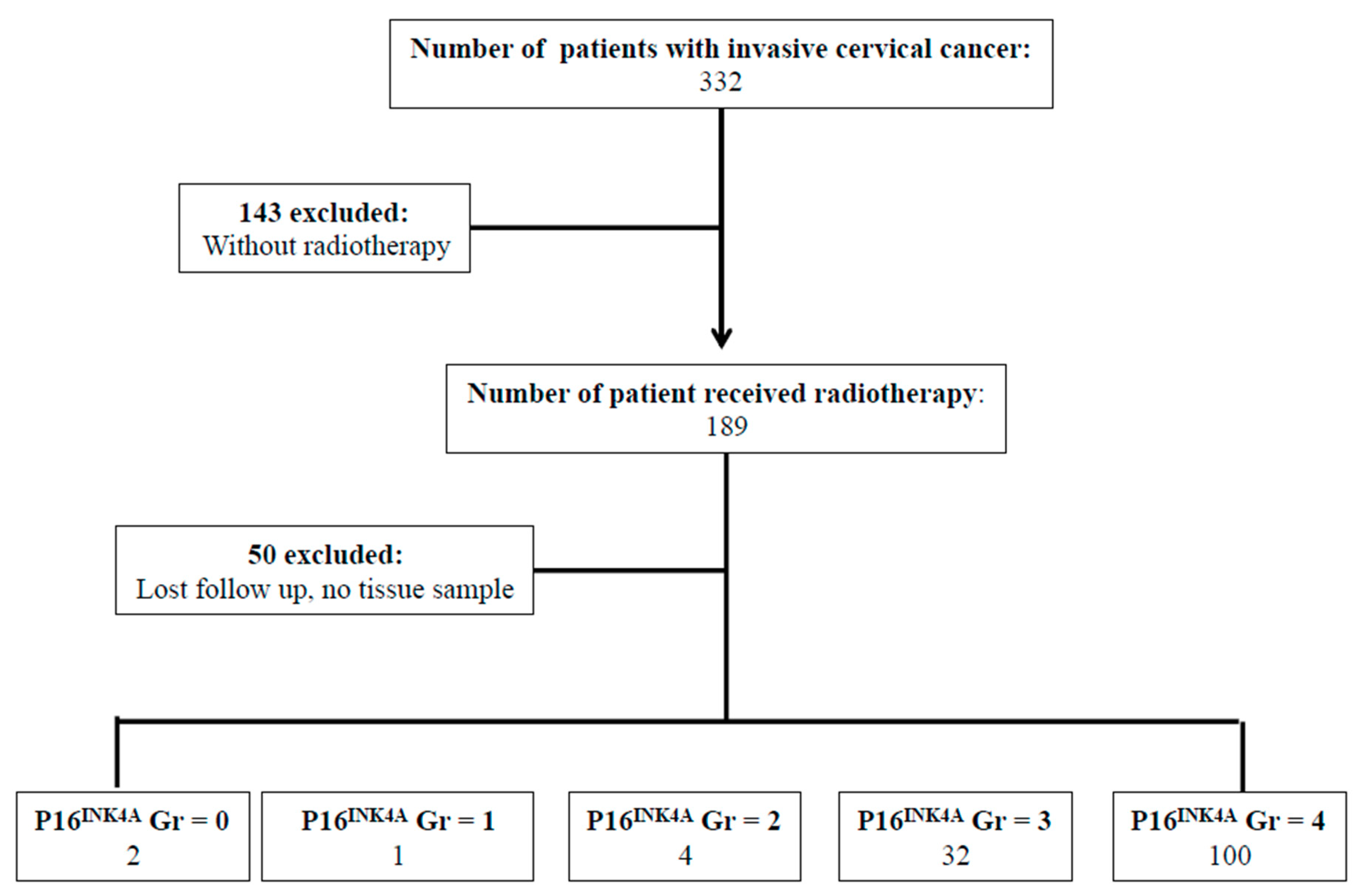
2.1. Patient Characteristics
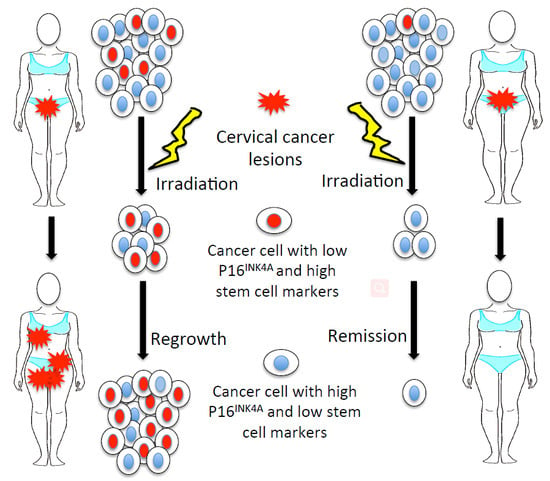
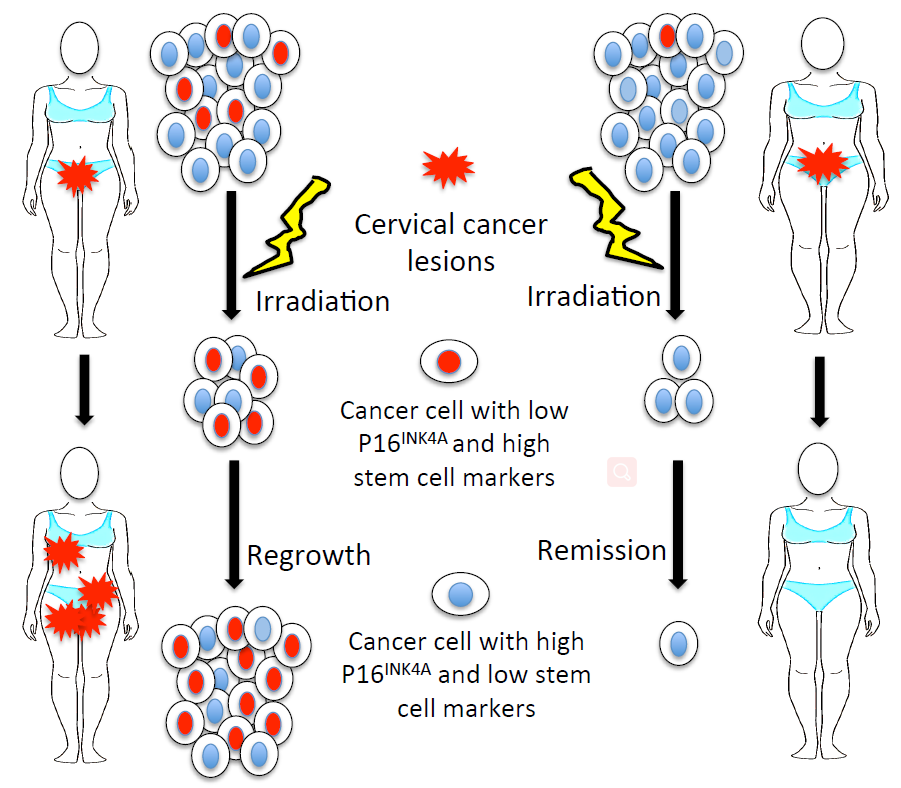
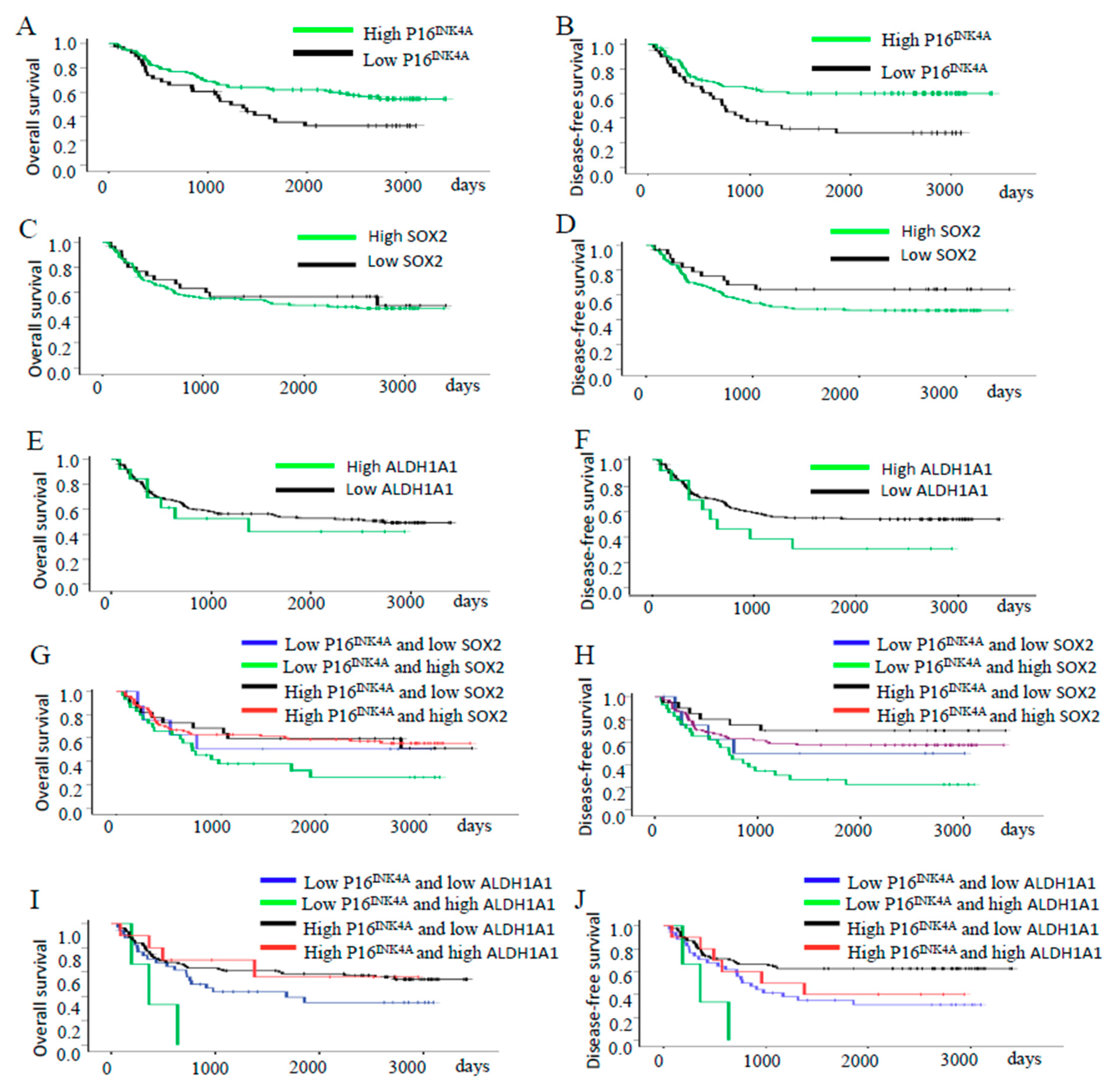
2.2. Survival Pattern of the Patients’ Tumors with Different Expression of P16INK4A
2.3. Analysis of Risk Factors for Recurrence of Disease
2.4. Depletion of P16INK4A Increased the Resistance to Cisplatin and Irradiation of Cervical Cancer Cells
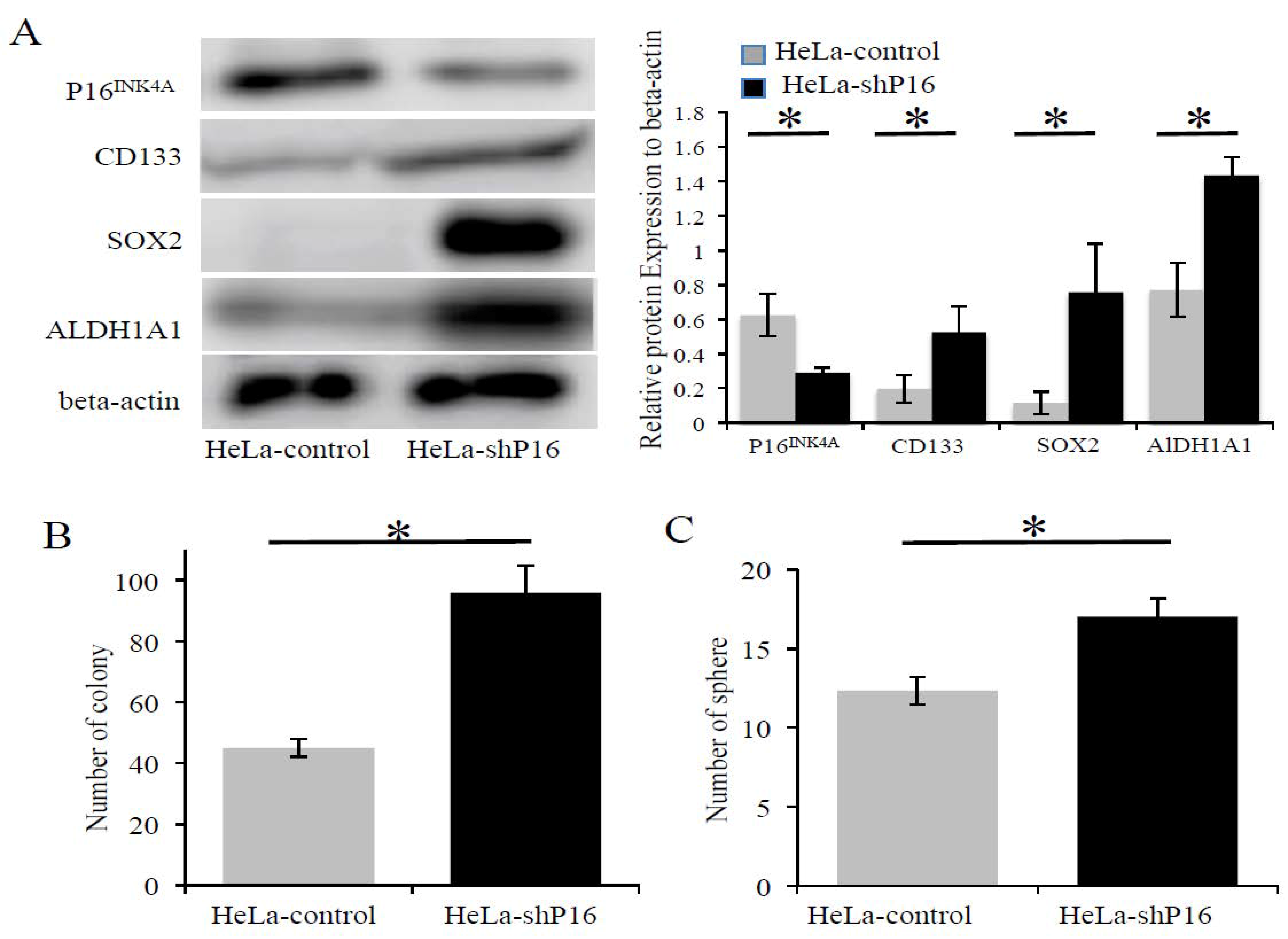
2.5. The Inhibition of P16INK4A Protein Expression Associated with Higher SOX2, ALDH1A1 Expression and Self-Renewal Ability in Cervical Cancer Cells
3. Discussion
4. Materials and Methods
4.1. Patients and Tissues
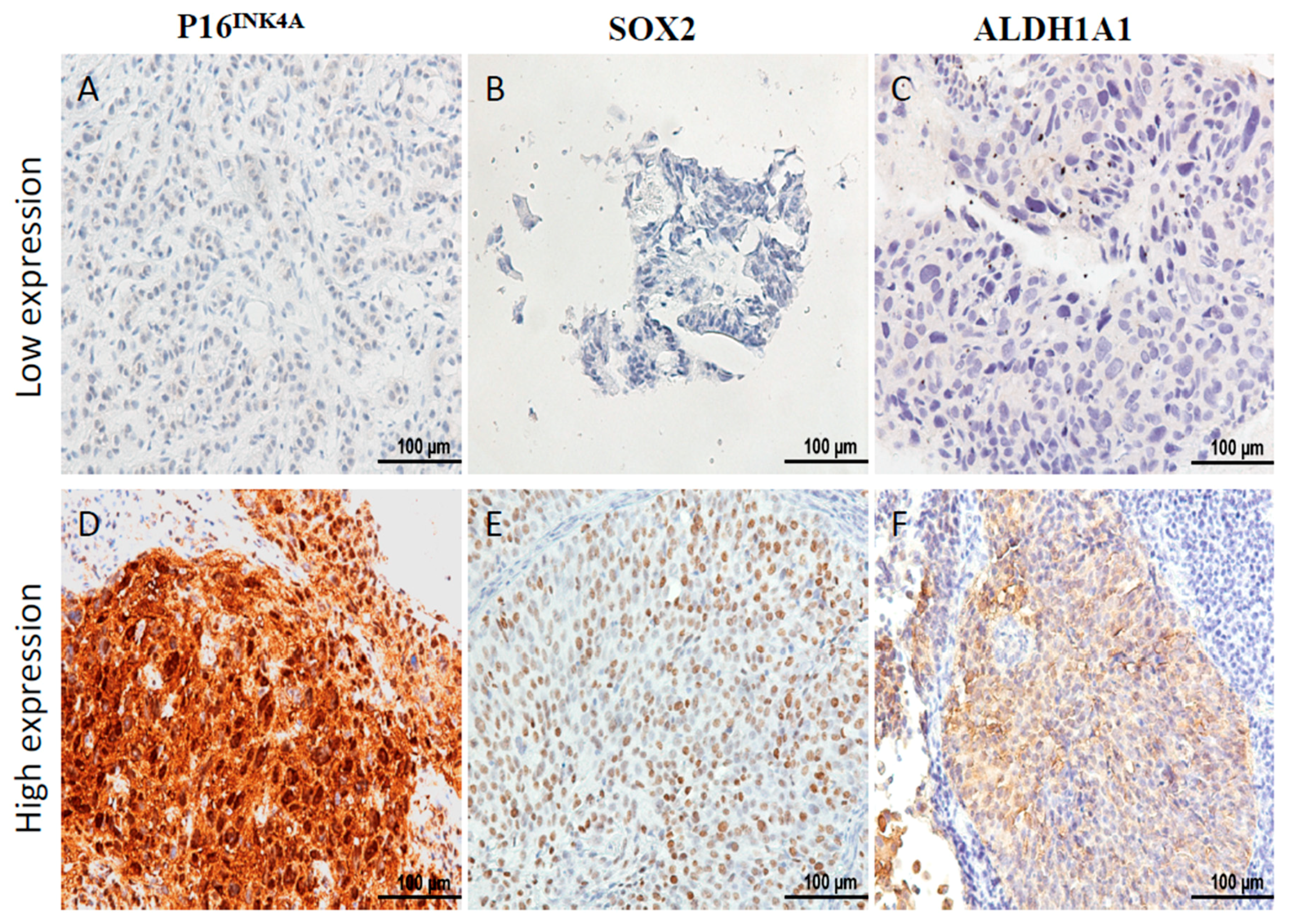
4.2. Immunohistochemical Staining
4.3. Cell Culture and Reagents
4.4. Transfection of Cervical Cancer Cell Lines
4.5. Irradiation of Cells
4.6. Clonogenic Assay
4.7. Western Blotting
4.8. Cellular Toxicity via CCK-8 Assay
4.9. Sphere Formation Assay
4.10. Real-Time PCR Assay
4.11. Statistical Analysis
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Torre, L.A.; Siegel, R.L.; Ward, E.M.; Jemal, A. Global Cancer Incidence and Mortality Rates and Trends—An Update. Cancer Epidemiol. Biomarker Prev. 2016, 25, 16–27. [Google Scholar] [CrossRef] [PubMed]
- Chemoradiotherapy for Cervical Cancer Meta-Analysis Collaboration. Reducing uncertainties about the effects of chemoradiotherapy for cervical cancer: Individual patient data meta-analysis. Cochrane Database Syst. Rev. 2010, 1, CD008285. [Google Scholar] [CrossRef]
- Koh, W.J.; Greer, B.E.; Abu-Rustum, N.R.; Apte, S.M.; Campos, S.M.; Cho, K.R.; Chu, C.; Cohn, D.; Crispens, M.A.; Dorigo, O. Cervical Cancer, Version 2.2015. J. Natl. Compr. Cancer Netw. 2015, 13, 395–404. [Google Scholar] [CrossRef]
- Czerniak, B.; Olszewska-Slonina, D. Biomarkers could facilitate prediction of worse clinical outcome of cancer with special insight to cervical cancer. Contemp. Oncol. 2018, 22, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Fu, H.C.; Yang, Y.C.; Chen, Y.J.; Lin, H.; Ou, Y.C.; Chien, C.C.; Huang, E.Y.; Huang, H.Y.; Lan, J.; Chi, H.P. Increased expression of SKP2 is an independent predictor of locoregional recurrence in cervical cancer via promoting DNA-damage response after irradiation. Oncotarget 2016, 7, 44047–44061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, K.; Li, L.A.; Meng, Y.G.; Fu, X.Y. p16 expression in patients with cervical cancer and its prognostic significance: Meta-analysis of published literature. Eur. J. Obstet. Gyn. Reprod. Biol. 2014, 183, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Huang, E.Y.; Chanchien, C.C.; Lin, H.; Wang, C.C.; Wang, C.J.; Huang, C.C. Galectin-1 is an independent prognostic factor for local recurrence and survival after definitive radiation therapy for patients with squamous cell carcinoma of the uterine cervix. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 975–982. [Google Scholar] [CrossRef] [PubMed]
- Krause, M.; Yaromina, A.; Eicheler, W.; Koch, U.; Baumann, M. Cancer stem cells: Targets and potential biomarkers for radiotherapy. Clin. Cancer Res. 2011, 17, 7224–7229. [Google Scholar] [CrossRef] [PubMed]
- Baumann, M.; Krause, M.; Hill, R. Exploring the role of cancer stem cells in radioresistance. Nat. Rev. Cancer 2008, 8, 545–554. [Google Scholar] [CrossRef] [PubMed]
- Kreso, A.; Dick, J.E. Evolution of the cancer stem cell model. Cell Stem Cell 2014, 14, 275–291. [Google Scholar] [CrossRef] [PubMed]
- Enderling, H. Cancer stem cells and tumor dormancy. Adv. Exp. Med. Biol. 2013, 734, 55–71. [Google Scholar] [PubMed]
- Huang, R.; Rofstad, E.K. Cancer stem cells (CSCs), cervical CSCs and targeted therapies. Oncotarget 2017, 8, 35351–35367. [Google Scholar] [CrossRef] [PubMed]
- Qi, W.; Zhao, C.; Zhao, L.; Liu, N.; Li, X.; Yu, W.; Wei, L. Sorting and identification of side population cells in the human cervical cancer cell line HeLa. Cancer Cell Int. 2014, 14, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tyagi, A.; Vishnoi, K.; Kaur, H.; Srivastava, Y.; Roy, B.G.; Das, B.C.; Bharti, A.C. Cervical cancer stem cells manifest radioresistance: Association with upregulated AP-1 activity. Sci. Rep. 2017, 7, 4781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, T. Cell cycle inhibitors in normal and tumor stem cells. Oncogene 2004, 23, 7256–7266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Arcangelo, D.; Tinaburri, L.; Dellambra, E. The Role of p16(INK4a) Pathway in Human Epidermal Stem Cell Self-Renewal, Aging and Cancer. Int. J. Mol. Sci. 2017, 18, 1591. [Google Scholar] [CrossRef] [PubMed]
- Yu, K.R.; Kang, K.S. Aging-related genes in mesenchymal stem cells: A mini-review. Gerontology 2013, 59, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, E.; Chen, T. A matter of life and death: Self-renewal in stem cells. EMBO Rep. 2013, 14, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Lanza, R.; Atala, A. Essentials of Stem Cell Biology; Elsevier Science: New York, NY, USA, 2013. [Google Scholar]
- De Freitas, A.C.; Coimbra, E.C.; Leitao Mda, C. Molecular targets of HPV oncoproteins: Potential biomarkers for cervical carcinogenesis. Biochim. Biophys. Acta 2014, 1845, 91–103. [Google Scholar] [CrossRef] [PubMed]
- Lesnikova, I.; Lidang, M.; Hamilton-Dutoit, S.; Koch, J. p16 as a diagnostic marker of cervical neoplasia: A tissue microarray study of 796 archival specimens. Diagn. Pathol. 2009, 4, 22. [Google Scholar] [CrossRef] [PubMed]
- Steenbergen, R.D.; Snijders, P.J.; Heideman, D.A.; Meijer, C.J. Clinical implications of (epi)genetic changes in HPV-induced cervical precancerous lesions. Nat. Rev. Cancer 2014, 14, 395–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, J.; Albers, A.E.; Qin, J.; Kaufmann, A.M. Prognostic significance of overexpressed p16INK4a in patients with cervical cancer: A meta-analysis. PLoS ONE 2014, 9, e106384. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, J.K.; Lewis, J.S., Jr.; Pfeifer, J.; Huettner, P.; Grigsby, P. Prognostic significance of p16 expression in advanced cervical cancer treated with definitive radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.W.; Cho, H.; Choi, C.H.; Ylaya, K.; Chung, J.Y.; Kim, J.H.; Hewitt, S.M. Clinical significance of OCT4 and SOX2 protein expression in cervical cancer. BMC Cancer 2015, 15, 1015. [Google Scholar] [CrossRef] [PubMed]
- Yao, T.; Chen, Q.; Zhang, B.; Zhou, H.; Lin, Z. The expression of ALDH1 in cervical carcinoma. Med. Sci. Monit. 2011, 17, HY21–HY26. [Google Scholar] [CrossRef] [PubMed]
- Lv, Y.; Yang, L.; Wang, F. Chemoradiation therapy reduces aldehyde dehydrogenase 1 expression in cervical cancer but does not improve patient survival. Med. Oncol. 2015, 32, 155. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Collado, M.; Villasante, A.; Strati, K.; Ortega, S.; Canamero, M.; Blasco, M.A.; Serrano, M. The Ink4/Arf locus is a barrier for iPS cell reprogramming. Nature 2009, 460, 1136–1139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arima, Y.; Hayashi, N.; Hayashi, H.; Sasaki, M.; Kai, K.; Sugihara, E.; Abe, E.; Yoshida, A.; Mikami, S.; Nakamura, S. Loss of p16 expression is associated with the stem cell characteristics of surface markers and therapeutic resistance in estrogen receptor-negative breast cancer. Int. J. Cancer 2012, 130, 2568–2579. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Zhang, J.; Shi, H. Expression of cancer stem markers could be influenced by silencing of p16 gene in HeLa cervical carcinoma cells. Eur. J. Gynaecol. Oncol. 2016, 37, 221–225. [Google Scholar] [PubMed]
- McLaughlin-Drubin, M.E.; Park, D.; Munger, K. Tumor suppressor p16INK4A is necessary for survival of cervical carcinoma cell lines. Proc. Natl. Acad. Sci. USA 2013, 110, 16175–16180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koo, C.L.; Kok, L.F.; Lee, M.Y.; Wu, T.S.; Cheng, Y.W.; Hsu, J.D.; Ruan, A.; Chao, K.C.; Han, C.P. Scoring mechanisms of p16INK4a immunohistochemistry based on either independent nucleic stain or mixed cytoplasmic with nucleic expression can significantly signal to distinguish between endocervical and endometrial adenocarcinomas in a tissue microarray study. J. Transl. Med. 2009, 7, 25. [Google Scholar] [PubMed] [Green Version]
- Ji, J.; Zheng, P.S. Expression of Sox2 in human cervical carcinogenesis. Hum. Pathol. 2010, 41, 1438–1447. [Google Scholar] [CrossRef] [PubMed]
- Franken, N.A.; Rodermond, H.M.; Stap, J.; Haveman, J.; van Bree, C. Clonogenic assay of cells in vitro. Nat. Protoc. 2006, 1, 2315–2359. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total (%) | Status of P16INK4A Staining | p Value | |
|---|---|---|---|---|
| Low | High | |||
| All cases | 139 | 39 | 100 | |
| Age | ||||
| ≥60 | 69 (49.6) | 21 (53.8) | 48 (48.0) | |
| <60 | 70 (50.4) | 18 (46.2) | 52 (52.0) | 0.536 |
| Stage | ||||
| lower (I,II) | 110 (79.1) | 29 (74.4) | 81 (81.0) | |
| higher (III,IV) | 29 (20.9) | 10 (25.6) | 19 (19.0) | 0.387 |
| Histologic type | ||||
| squamous cell carcinoma | 131 (94.2) | 35 (89.7) | 96 (96.0) | |
| adenocarcinoma | 3 (2.2) | 2 (5.1) | 1 (1.0) | |
| adenosquamous cell carcinoma | 5 (3.6) | 2 (5.1) | 3 (3.0) | 0.261 |
| Histologic grade | ||||
| Grade 1 | 10 (7.2) | 2 (5.1) | 8 (8.0) | |
| Grade 2 | 36 (25.9) | 10 (25.6) | 26 (26.0) | |
| Grade 3 and unknown | 93 (66.9) | 27 (69.2) | 66 (66.0) | 0.832 |
| Tumor size | ||||
| ≥4 cm | 77 (55.4) | 21 (53.8) | 56 (56.0) | |
| <4 cm | 62 (44.6) | 18 (46.2) | 44 (44.0) | 0.818 |
| SCC level before therapy (SD) | 12.5 (26.9) | 14.3 (24.6) | 12.2 (28.8) | 0.703 |
| CEA level before therapy (SD) | 14.2 (57.4) | 20.6 (62.3) | 12.6 (58.2) | 0.527 |
| High SOX2 # | 107 (77.5) | 29 (76.3) | 78 (78.0) | 0.832 |
| High ALDH1A1 ## | 13 (9.6) | 3 (7.9) | 10 (10.0) | 0.681 |
| Hysterectomy | 33 (23.7) | 11 (28.2) | 22 (22.0) | 0.440 |
| Chemotherapy | 84 (61.8) | 24 (61.5) | 60 (60.0) | 0.998 |
| Recurrence | 65 (47.8) | 27 (69.2) | 38 (38.0) | 0.002 * |
| Deaths | 69 (49.6) | 25 (64.1) | 44 (44.0) | 0.033 * |
| Variable | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | |
| Age ≥ 60 | 1.043 | 0.652–1.668 | 0.86 | 1.348 | 0.702–2.591 | 0.369 |
| Stage (III, IV) | 3.607 | 2.159–6.026 | <0.001 * | 2.95 | 1.378–6.317 | 0.005 * |
| Cell type (non-SCC) | 3.009 | 1.489–6.080 | 0.002 * | 4.77 | 1.597–14.25 | 0.005 * |
| Histologic grade (G3) | 1.42 | 0.928–2.171 | 0.106 | 1.306 | 0.763–2.237 | 0.33 |
| Tumor size (≥4 cm) | 1.587 | 0.973–2.591 | 0.064 | 1.053 | 0.518–2.141 | 0.888 |
| High SCC level # | 1.845 | 11.06–3.078 | 0.019 * | 1.312 | 0.640–2.687 | 0.459 |
| High CEA level ## | 3.134 | 1.607–6.110 | 0.001 * | 2.077 | 0.931–4.632 | 0.074 |
| Low P16INK4A | 2.137 | 1.302–3.509 | 0.003 * | 1.941 | 1.057–3.559 | 0.032 * |
| Low P16INK4A/high SOX2 | 2.298 | 1.369–3.857 | 0.002 * | 0.85 | 0.160–4.509 | 0.849 |
| Low P16INK4A/high ALDH1A1 | 4.086 | 1.261–13.24 | 0.019 * | 1.608 | 0.276–9.381 | 0.598 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, H.-C.; Chuang, I.-C.; Yang, Y.-C.; Chuang, P.-C.; Lin, H.; Ou, Y.-C.; Chang Chien, C.-C.; Huang, H.-S.; Kang, H.-Y. Low P16INK4A Expression Associated with High Expression of Cancer Stem Cell Markers Predicts Poor Prognosis in Cervical Cancer after Radiotherapy. Int. J. Mol. Sci. 2018, 19, 2541. https://doi.org/10.3390/ijms19092541
Fu H-C, Chuang I-C, Yang Y-C, Chuang P-C, Lin H, Ou Y-C, Chang Chien C-C, Huang H-S, Kang H-Y. Low P16INK4A Expression Associated with High Expression of Cancer Stem Cell Markers Predicts Poor Prognosis in Cervical Cancer after Radiotherapy. International Journal of Molecular Sciences. 2018; 19(9):2541. https://doi.org/10.3390/ijms19092541
Chicago/Turabian StyleFu, Hung-Chun, I-Chieh Chuang, Yi-Chien Yang, Pei-Chin Chuang, Hao Lin, Yu-Che Ou, Chan-Chao Chang Chien, Hui-Shan Huang, and Hong-Yo Kang. 2018. "Low P16INK4A Expression Associated with High Expression of Cancer Stem Cell Markers Predicts Poor Prognosis in Cervical Cancer after Radiotherapy" International Journal of Molecular Sciences 19, no. 9: 2541. https://doi.org/10.3390/ijms19092541