A Novel Marker of Inflammation: Azurocidin in Patients with ST Segment Elevation Myocardial Infarction

 , ,
, ,
Abstract
:1. Introduction
2. Results
3. Discussion
4. Patients and Methods
4.1. Study Population
4.2. Measurement of Plasma Azurocidin Levels
4.3. Patient Assessments
4.4. Statistical Analyses
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lopez, A.D.; Mathers, C.D.; Ezzati, M.; Jamison, D.T.; Murray, C.J. Global and regional burden of disease and risk factors. 2001: Systematic analysis of population health data. Lancet 2006, 367, 1747–1757. [Google Scholar] [CrossRef]
- Acet, H.; Ertaş, F.; Bilik, M.Z.; Akıl, M.A.; Özyurtlu, F.; Aydın, M.; Oylumlu, M.; Polat, N.; Yüksel, M.; Yıldız, A.; et al. The relationship between neutrophil to lymphocyte ratio, platelet to lymphocyte ratio and thrombolysis in myocardial infarction risk score in patients with ST elevation acute myocardial infarction before primary coronary intervention. Postepy Kardiologii Interwencyjnej 2015, 11, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Libby, P. Inflammation in atherosclerosis. Nature 2002, 420, 868–874. [Google Scholar] [CrossRef] [PubMed]
- Pearson, T.A.; Mensah, G.A.; Alexander, R.W.; Anderson, J.L.; Cannon, R.O., 3rd; Criqui, M.; Fadl, Y.Y.; Fortmann, S.P.; Hong, Y.; Myers, G.L.; et al. Markers of inflammation and cardiovascular disease: Application to clinical and public health practice: A statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart Association. Circulation 2003, 107, 499–511. [Google Scholar] [CrossRef] [PubMed]
- Libby, P.; Tabas, I.; Fredman, G.; Fisher, E.A. Inflammation and its resolution as determinants of acute coronary syndromes. Circ. Res. 2014, 114, 1867–1879. [Google Scholar] [CrossRef] [PubMed]
- Keeley, E.C.; Boura, J.A.; Grines, C.L. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: A quantitative review of 23 randomised trials. Lancet 2003, 361, 13–20. [Google Scholar] [CrossRef]
- Thune, J.J.; Hoefsten, D.E.; Lindholm, M.G.; Mortensen, L.S.; Andersen, H.R.; Nielsen, T.T.; Kober, L.; Kelbaek, H. Simple risk stratification at admission to identify patients with reduced mortality from primary angioplasty. Circulation 2005, 112, 2017–2021. [Google Scholar] [CrossRef] [PubMed]
- Morrow, D.A.; Antman, E.M.; Charlesworth, A.; Cairns, R.; Murphy, S.A.; de Lemos, J.A.; Giugliano, R.P.; McCabe, C.H.; Braunwald, E. TIMI risk score for ST-elevation myocardial infarction: A convenient, bedside, clinical score for risk assessment at presentation: An intravenous nPA for treatment of infarcting myocardium early II trial substudy. Circulation 2000, 102, 2031–2037. [Google Scholar] [CrossRef] [PubMed]
- Addala, S.; Grines, C.L.; Dixon, S.R.; Stone, G.W.; Boura, J.A.; Ochoa, A.B.; Pellizzon, G.; O’Neill, W.W.; Kahn, J.K. Predicting mortality in patients with ST-elevation myocardial infarction treated with primary percutaneous coronary intervention (PAMI risk score). Am. J. Cardiol. 2004, 93, 629–632. [Google Scholar] [CrossRef] [PubMed]
- Halkin, A.; Singh, M.; Nikolsky, E.; Grines, C.L.; Tcheng, J.E.; Garcia, E.; Cox, D.A.; Turco, M.; Stuckey, T.D.; Na, Y.; et al. Prediction of mortality after primary percutaneous coronary intervention for acute myocardial infarction: The CADILLAC risk score. J. Am. Coll. Cardiol. 2005, 45, 1397–1405. [Google Scholar] [CrossRef] [PubMed]
- InTIME-II Investigators. Intravenous NPA for the treatment of infarcting myocardium early; InTIME-II, a double-blind comparison of single-bolus lanoteplase vs. accelerated alteplase for the treatment of patients with acute myocardial infarction. Eur. Heart J. 2000, 21, 2005–2013. [Google Scholar] [CrossRef] [PubMed]
- McAuley O’Kane, C.M.; Craig, T.R.; Shyamsundar, M.; Herwald, H.; Dib, K. Simvastatin decreases the level of heparin-binding protein in patients with acute lung injury. BMC Pulm. Med. 2013, 13, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pereira, H.A.; Shafer, W.M.; Pohl, J.; Martin, L.E.; Spitznagel, J.K. CAP37, a human neutrophil-derived chemotactic factor with monocyte specific activity. J. Clin. Investig. 1990, 85, 1468–1476. [Google Scholar] [CrossRef] [PubMed]
- Chertov, O.; Michiel, D.F.; Xu, L.; Wang, J.M.; Tani, K.; Murphy, W.J.; Longo, D.L.; Taub, D.D.; Oppenheim, J.J. Identification of defensin-1, defensin-2, and CAP37/azurocidin as T-cell chemoattractant proteins released from interleukin-8 stimulated neutrophils. J. Biol. Chem. 1996, 271, 2935–2940. [Google Scholar] [CrossRef] [PubMed]
- Linder, A.; Christensson, B.; Herwald, H.; Björck, L.; Akesson, P. Heparin-binding protein: An early marker of circulatory failure in sepsis. Clin. Infect. Dis. 2009, 49, 1044–1050. [Google Scholar] [CrossRef] [PubMed]
- Linder, A.; Akesson, P.; Inghammar, M.; Treutiger, C.J.; Linnér, A.; Sundén-Cullberg, J. Elevated plasma levels of heparin-binding protein in intensive care unit patients with severe sepsis and septic shock. Crit. Care 2012, 16, R90. [Google Scholar] [CrossRef] [PubMed]
- Herwald, H.; Cramer, H.; Morgelin, M.; Russell, W.; Sollenberg, U.; Norrby-Teglund, A.; Flodgaard, H.; Lindbom, L.; Björck, L. M protein, a classical bacterial virulence determinant, forms complexes with fibrinogen that induce vascular leakage. Cell 2004, 116, 367–379. [Google Scholar] [CrossRef]
- Gautam, N.; Olofsson, A.M.; Herwald, H.; Iversen, L.F.; Lundgren-Akerlund, E.; Hedqvist, P.; Arfors, K.E.; Flodgaard, H.; Lindbom, L. Heparin-binding protein (HBP/CAP37): A missing link in neutrophil-evoked alteration of vascular permeability. Nat. Med. 2001, 7, 1123–1127. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, N.; Howell, M.D.; Bates, D.W.; Angus, D.C.; Ngo, L.; Talmor, D. The association of sepsis syndrome and organ dysfunction with mortality in emergency department patients with suspected infection. Ann. Emerg. Med. 2006, 48, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Lin, Q.; Shen, J.; Shen, L.; Zhang, Z.; Fu, F. Increased plasma levels of heparin-binding protein in patients with acute respiratory distress syndrome. Crit. Care 2013, 17, R155. [Google Scholar] [CrossRef] [PubMed]
- Medina, I.; Cougoule, C.; Drechsler, M.; Bermudez, B.; Koenen, R.R.; Sluimer, J.; Wolfs, I.; Döring, Y.; Herias, V.; Gijbels, M.; et al. Hck/Fgr kinase deficiency reduces plaque growth and stability by blunting monocyte recruitment and intraplaque motility. Circulation 2015, 132, 490–501. [Google Scholar] [CrossRef] [PubMed]
- Horckmans, M.; Ring, L.; Duchene, J.; Santovito, D.; Schloss, M.J.; Drechsler, M.; Weber, C.; Soehnlein, O.; Steffens, S. Neutrophils orchestrate post-myocardial infarction healing by polarizing macrophages towards a reparative phenotype. Eur. Heart J. 2017, 38, 187–197. [Google Scholar] [CrossRef] [PubMed]
- Guasti, L.; Dentali, F.; Castiglioni, L.; Maroni, L.; Marino, F.; Squizzato, A.; Ageno, W.; Gianni, M.; Gaudio, G.; Grandi, A.M.; et al. Neutrophils and clinical outcomes in patients with acute coronary syndromes and/or cardiac revascularisation. A systematic review on more than 34,000 subjects. Thromb. Haemost. 2011, 106, 591–599. [Google Scholar] [CrossRef] [PubMed]
- Arruda-Olson, A.M.; Reeder, G.S.; Bell, M.R.; Weston, S.A.; Roger, V.L. Neutrophilia predicts death and heart failure after myocardial infarction: A community-based study. Circ. Cardiovasc. Qual. Outcomes 2009, 2, 656–662. [Google Scholar] [CrossRef] [PubMed]
- Baumann, S.; Huseynov, A.; Koepp, J.; Jabbour, C.; Behnes, M.; Becher, T.; Renker, M.; Lang, S.; Borggrefe, M.; Lehmann, R.; et al. Comparison of serum uric acid, bilirubin, and C-reactive protein as prognostic biomarkers of in-hospital MACE between women and men with ST-segment elevation myocardial infarction. Angiology 2016, 67, 272–280. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.H.; Zhang, S.Y.; Fang, Q.; Shen, Z.; Fan, Z.; Jin, X.; Zeng, Y.; Liu, Z.; Xie, H. Renal dysfunction and hsCRP predict long-term outcomes of percutaneous coronary intervention in acute myocardial infarction. Am. J. Med. Sci. 2015, 349, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Foussas, S.G.; Zairis, M.N.; Lyras, A.G.; Patsourakos, N.G.; Tsirimpis, V.G.; Katsaros, K.; Beldekos, D.J.; Handanis, S.M.; Mytas, D.Z.; Karidis, K.S.; et al. Early prognostic usefulness of C-reactive protein added to the Thrombolysis in Myocardial Infarction risk score in acute coronary syndromes. Am. J. Cardiol. 2005, 96, 533–537. [Google Scholar] [CrossRef] [PubMed]
- Linder, A.; Arnold, R.; Boyd, J.H.; Zindovic, M.; Zindovic, I.; Lange, A.; Paulsson, M.; Nyberg, P.; Russell, J.A.; Pritchard, D.; et al. Heparin-Binding Protein Measurement Improves the Prediction of Severe Infection with Organ Dysfunction in the Emergency Department. Crit. Care Med. 2015, 43, 2378–2386. [Google Scholar] [CrossRef] [PubMed]
- Dankiewicz, J.; Linder, A.; Annborn, M.; Rundgren, M.; Friberg, H. Heparin-binding protein: An early indicator of critical illness and predictor of outcome in cardiac arrest. Resuscitation 2013, 84, 935–939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Killip, T.; Kimball, J.T. Treatment of myocardial infarction in a coronary care unit. A two-year experience with 250 patients. Am. J. Cardiol. 1967, 20, 457–464. [Google Scholar] [CrossRef]
- TIMI Risk Score for STEMI. MD+Calc. Available online: http://www.mdcalc.com/timi-risk-score-for-stemi (accessed on 2 February 2016).
- Granger, C.B.; Goldberg, R.J.; Dabbous, O.; Pieper, K.S.; Eagle, K.A.; Cannon, C.P.; Van De Werf, F.; Avezum, A.; Goodman, S.G.; Flather, M.D.; et al. Predictors of hospital mortality in the global registry of acute coronary events. Arch. Intern. Med. 2003, 163, 2345–2353. [Google Scholar] [CrossRef] [PubMed]
- GRACE ACS Risk Model. ALS Functional Rating Scale. Available online: http://www.outcomes-umassmed.org/risk_models_grace_orig.aspx (accessed on 2 February 2016).
- SYNTAX Score. 2016. Available online: http://www.syntaxscore.com/ (accessed on 2 February 2016).
- Sianos, G.; Morel, M.A.; Kappetein, A.P.; Morice, M.C.; Colombo, A.; Dawkins, K.; van den Brand, M.; Van Dyck, N.; Russell, M.E.; Mohr, F.W.; et al. The SYNTAX Score: An angiographic tool grading the complexity of coronary artery disease. Eurointervention 2005, 1, 219–227. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Patients with STEMI | Control Subjects | Statistical Significance a |
|---|---|---|---|
| n = 76 | n = 30 | ||
| Age, years | 60.0 ± 13.6 | 53.4 ± 12.3 | NS |
| Sex, males | 58 (76.3) | 20 (66.7) | NS |
| BMI | 24.08 ± 6.99 | 20.25 ± 7.94 | NS |
| Smokers | 38 (50.0) | 17 (56.7) | NS |
| Hypertension | 34 (44.7) | 0 (0.0) | NA |
| SBP, mmHg | 126 (50–220) | 115 (100–125) | NS |
| DBP, mmHg | 80 (30–88) | 75 (50–81) | NS |
| Diabetes mellitus | 59 (77.6) | 0 (0.0) | NA |
| Glucose, mg/dL | 128 (79–361) | 94 (89–105) | p = 0.02 |
| Hyperlipidaemia | 65 (85.5) | 0 (0.0) | NA |
| LDL-C, mg/dL | 133.37 ± 39.14 | 92.0 ± 12.2 | p = 0.042 |
| WBC, 103/µL | 11.97 (6.79–22.05) | 8.09 (6.79–8.88) | p < 0.001 |
| Neutrophil, 103/µL | 9.43 ± 3.69 | 5.78 ± 1.16 | p < 0.001 |
| Lymphocyte, 103/µL | 1.76 (0.6–9.4) | 1.65 (0.78–2.56) | NS |
| NLR | 7.97 ± 4.10 | 4.56 ± 2.61 | p = 0.034 |
| CRP, mg/dL | 1.47 ± 2.80 | 0.39 ± 1.12 | p = 0.028 |
| Creatinine, mg/dL | 0.87 ± 0.18 | 0.84 ± 0.17 | NS |
| EF, % | 45 (10–62) | 65 (60–65) | p < 0.001 |
| CK-MB, mg/dL | 52.0 ± 12.4 | – | NA |
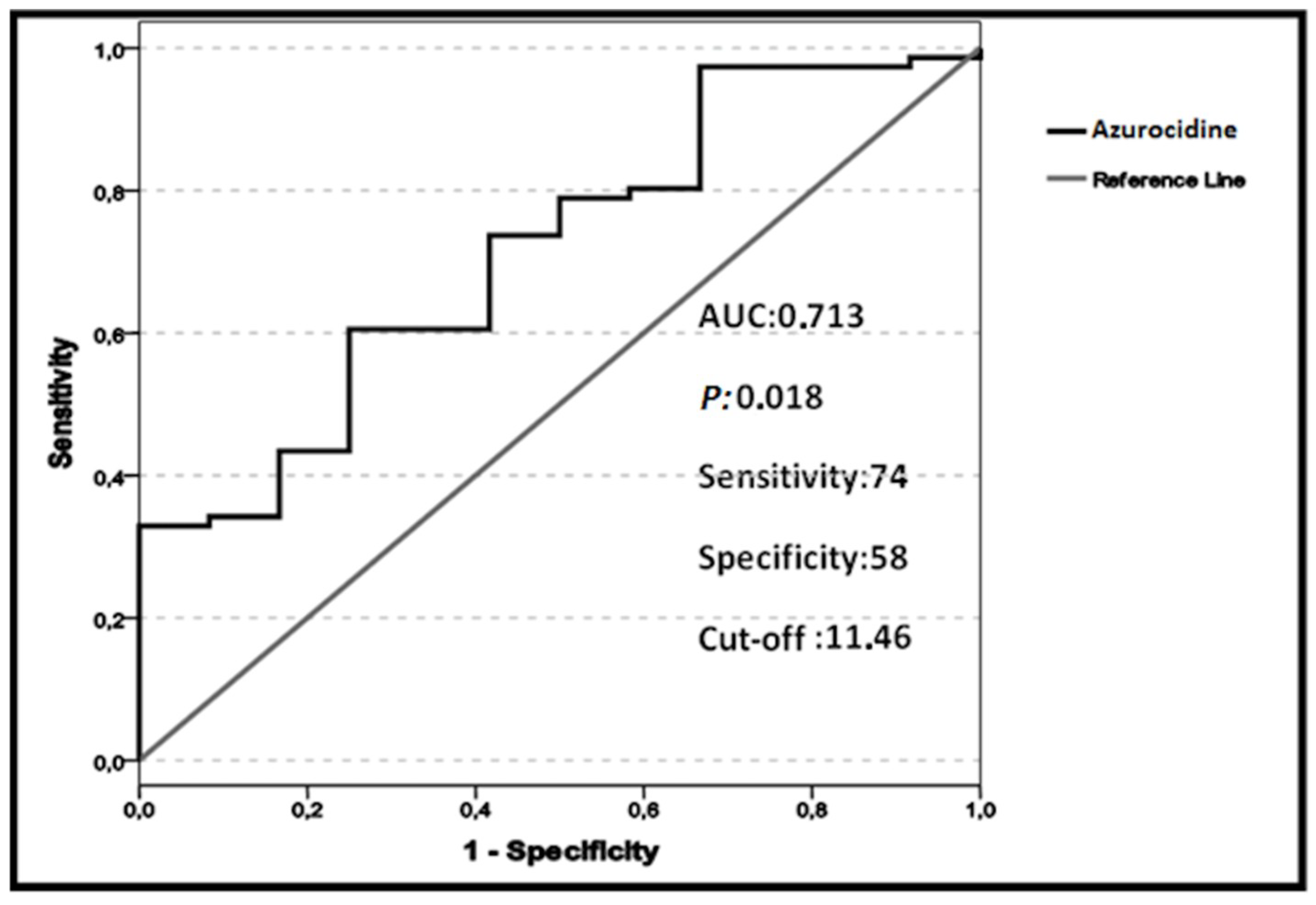
| Azurocidin, ng/mL | 18.07 ± 13.99 | 10.09 ± 5.29 | p = 0.018 |
| TIMI score | 4.5 ± 2.9 | – | NA |
| SYNTAX score | 14.9 ± 9.7 | – | NA |
| GRACE score | 122.6 ± 35.0 | – | NA |
| Characteristic | Azurocidin Levels | |
|---|---|---|
| Correlation Coefficient r | Statistical Significance a | |
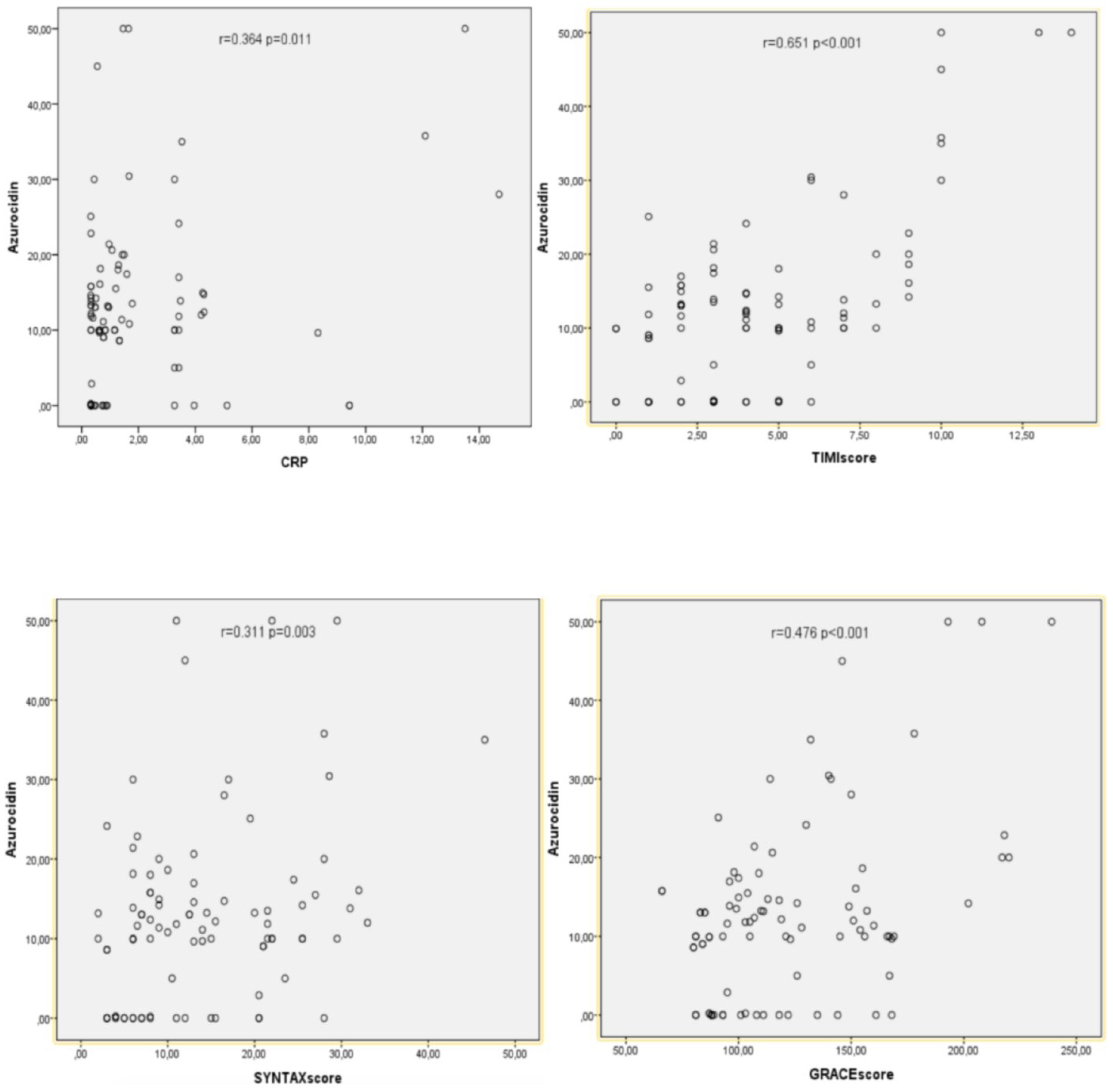
| TIMI score | 0.651 | p < 0.001 |
| CRP | 0.364 | p = 0.011 |
| NLR | 0.110 | NS |
| CK-MB | 0.104 | NS |
| SYNTAX score | 0.311 | p = 0.003 |
| GRACE score | 0.476 | p < 0.001 |
| Killip class | 0.505 | p < 0.001 |
| Dependent Variable: Azurocidin | ||
|---|---|---|
| Independent Variables | β (95% CI) | Statistical Significance a |
| TIMI score | 0.642 (0.337, 0.947) | p < 0.001 |
| GRACE score | 0.184 (−0.476, 0.109) | NS |
| SYNTAX score | 0.041 (−0.140, 0.225) | NS |
| Killip class | 0.169 (−0.076, 0.413) | NS |
| CRP | 0.077 (−0.095, 0.248) | NS |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ipek, E.; Yolcu, M.; Yildirim, E.; Altinkaynak, K.; Ozbek Sebin, S.; Kalkan, K.; Gulcu, O.; Ermis, E.; Ozturk, M. A Novel Marker of Inflammation: Azurocidin in Patients with ST Segment Elevation Myocardial Infarction. Int. J. Mol. Sci. 2018, 19, 3797. https://doi.org/10.3390/ijms19123797
Ipek E, Yolcu M, Yildirim E, Altinkaynak K, Ozbek Sebin S, Kalkan K, Gulcu O, Ermis E, Ozturk M. A Novel Marker of Inflammation: Azurocidin in Patients with ST Segment Elevation Myocardial Infarction. International Journal of Molecular Sciences. 2018; 19(12):3797. https://doi.org/10.3390/ijms19123797
Chicago/Turabian StyleIpek, Emrah, Mustafa Yolcu, Erkan Yildirim, Konca Altinkaynak, Saime Ozbek Sebin, Kamuran Kalkan, Oktay Gulcu, Emrah Ermis, and Mustafa Ozturk. 2018. "A Novel Marker of Inflammation: Azurocidin in Patients with ST Segment Elevation Myocardial Infarction" International Journal of Molecular Sciences 19, no. 12: 3797. https://doi.org/10.3390/ijms19123797