Alpha Lipoic Acid: A Therapeutic Strategy that Tend to Limit the Action of Free Radicals in Transplantation

Abstract
:1. Introduction
2. Pharmacological Treatments for IRI Prevention
2.1. ALA in Nervous System
2.2. ALA in Reproductive System
2.3. ALA in Liver
2.4. ALA in Intestine
2.5. ALA in Kidney
2.6. ALA in Circulatory System
2.7. Summary of the Experimental IRI Models
3. Clinical Trials
4. Discussion
5. Future Prospect
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| ALA | Alpha Lipoic Acid |
| LDH | Lactate Deshidrogenase |
| ROS | Reactive Oxygen Species |
| GST | Glutathione S-Transferase |
| ATP | Adenosine Triphosphate |
| TNF-α | Tumor Necrosis Factor Alpha |
| DHLA | Dihydrolipoic Acid |
| MDA | Malondialdehyde |
| SOD | Superoxide Dismutase |
| XO | Xanthine Oxidase |
| NO | Nitric Oxide |
| PNP | Purine Nucleoside Phosphorylase |
| NF-κB | Nuclear Factor Kappa B |
| AP-1 | Activator Protein-1 |
| GPx | Glutathione Peroxidase |
| CK | Creatine Kinase |
| ALDH2 | Aldehyde Dehydrogenase 2 |
| HO-1 | Hemoxigenase-1 |
| PCC | Protein Carbonyl Content |
| KDPI | Kidney Donor Profile Index |
| AST | Aspartate Transaminase |
| ALT | Alanine Transaminase |
References
- Teoh, N.; Dela Pena, A.; Farrell, G. Hepatic ischemic preconditioning in mice is associated with activation of NF-kappaB, p38 kinase, and cell cycle entry. Hepatology 2002, 36, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Carroll, W.R.; Esclamado, R.M. Ischemia/reperfusion injury in microvascular surgery. Head Neck 2000, 22, 700–713. [Google Scholar] [CrossRef]
- Buja, L.M. Myocardial ischemia and reperfusion injury. Cardiovasc. Pathol. 2005, 14, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Hossmann, K.A. Pathophysiology and therapy of experimental stroke. Cell Mol. Neurobiol. 2006, 26, 1057–1083. [Google Scholar] [CrossRef] [PubMed]
- Mergenthaler, P.; Dirnagl, U.; Meisel, A. Pathophysiology of stroke: Lessons from animal models. Metab. Brain Dis. 2004, 19, 151–167. [Google Scholar] [CrossRef] [PubMed]
- Rauen, U.; de Groot, H. New insights into the cellular and molecular mechanisms of cold storage injury. J. Investig. Med. 2004, 52, 299–309. [Google Scholar] [CrossRef] [PubMed]
- De Groot, H.; Rauen, U. Ischemia-reperfusion injury: Processes in pathogenetic networks: A review. Transplant. Proc. 2007, 39, 481–484. [Google Scholar] [CrossRef] [PubMed]
- Kaminski, K.A.; Bonda, T.A.; Korecki, J.; Musial, W.J. Oxidative stress and neutrophil activation--the two keystones of ischemia/reperfusion injury. Int. J. Cardiol. 2002, 86, 41–59. [Google Scholar] [CrossRef]
- Zweier, J.L.; Talukder, M.A. The role of oxidants and free radicals in reperfusion injury. Cardiovasc. Res. 2006, 70, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Granger, D.N. Role of xanthine oxidase and granulocytes in ischemia-reperfusion injury. Am. J. Physiol. 1988, 255, 1269–1275. [Google Scholar] [CrossRef] [PubMed]
- Tyler, D.D. Polarographic assay and intracellular distribution of superoxide dismutase in rat liver. Biochem. J. 1975, 147, 493–504. [Google Scholar] [CrossRef] [PubMed]
- Packer, M.A.; Porteous, C.M.; Murphy, M.P. Superoxide production by mitochondria in the presence of nitric oxide forms peroxynitrite. Biochem. Mol. Biol. Int. 1996, 40, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Halliwell, B.; Gutteridge, J.M.; Cross, C.E. Free radicals, antioxidants, and human disease: Where are we now? J. Lab. Clin. Med. 1992, 119, 598–620. [Google Scholar] [PubMed]
- Anaya-Prado, R.; Toledo-Pereyra, L.H.; Lentsch, A.B.; Ward, P.A. Ischemia/reperfusion injury. J. Surg. Res. 2002, 105, 248–258. [Google Scholar] [CrossRef] [PubMed]
- Maier, C.M.; Chan, P.H. Role of superoxide dismutases in oxidative damage and neurodegenerative disorders. Neuroscientist 2002, 8, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Kayawake, S.; Narbaitz, R.; Kako, K.J. Effects of chloroquine and nifedipine on the phospholipid content and enzyme activity in the subcellular fraction of ischemic rat liver. Basic Res. Cardiol. 1982, 77, 140–157. [Google Scholar] [CrossRef] [PubMed]
- Farber, J.L.; Martin, J.T.; Chien, K.R. Irreversible ischemic cell injury. Prevention by chlorpromazine of the aggregation of the intramembranous particles of rat liver plasma membranes. Am. J. Pathol. 1978, 92, 713–732. [Google Scholar] [PubMed]
- Singbartl, K.; Ley, K. Protection from ischemia-reperfusion induced severe acute renal failure by blocking E-selectin. Crit. Care. Med. 2000, 28, 2507–2514. [Google Scholar] [CrossRef] [PubMed]
- Guven, C.; Borcek, A.O.; Cemil, B.; Kurt, G.; Yildirim, Z.; Ucankus, N.L.; Kilic, N.; Ceviker, N. Neuroprotective effects of infliximab in experimental spinal cord ischemic injury. J. Clin. Neurosci. 2010, 17, 1563–1567. [Google Scholar] [CrossRef] [PubMed]
- Raafat, A.M.; Murray, M.T.; McGuire, T.; DeFrain, M.; Franko, A.P.; Zafar, R.S.; Palmer, K.; Diebel, L.; Dulchavsky, S.A. Calcium blockade reduces renal apoptosis during ischemia reperfusion. Shock 1997, 8, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Wollin, S.D.; Jones, P.J. Alpha-lipoic acid and cardiovascular disease. J. Nutr. 2003, 133, 3327–3330. [Google Scholar] [PubMed]
- Whiteman, M.; Tritschler, H.; Halliwell, B. Protection against peroxynitrite-dependent tyrosine nitration and alpha 1-antiproteinase inactivation by oxidized and reduced lipoic acid. FEBS Lett. 1996, 379, 74–76. [Google Scholar] [CrossRef]
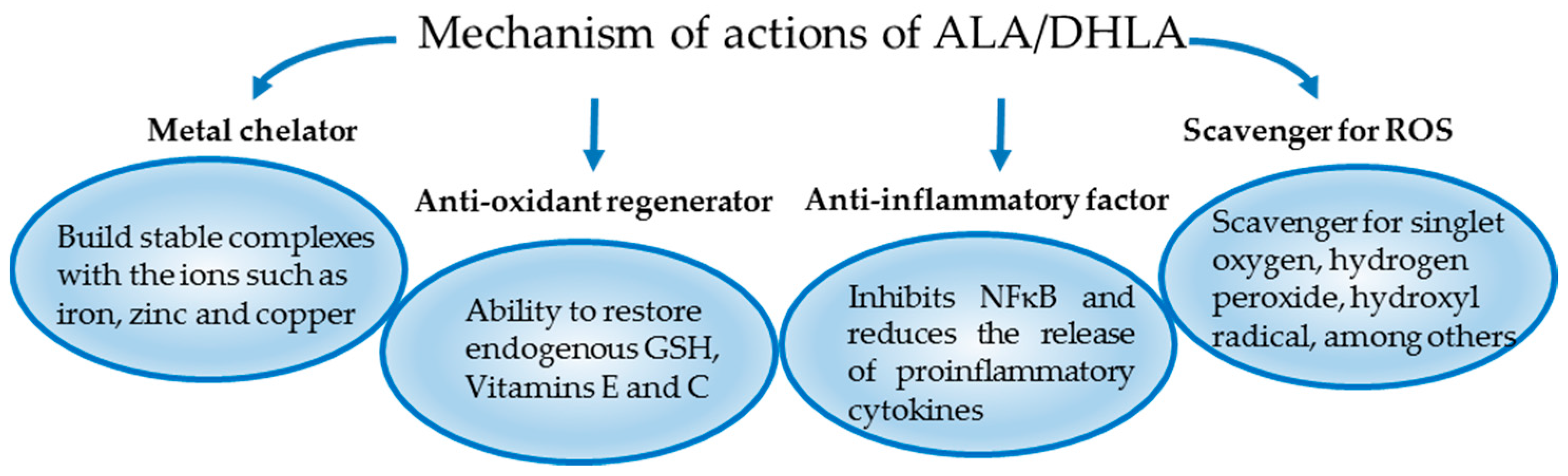
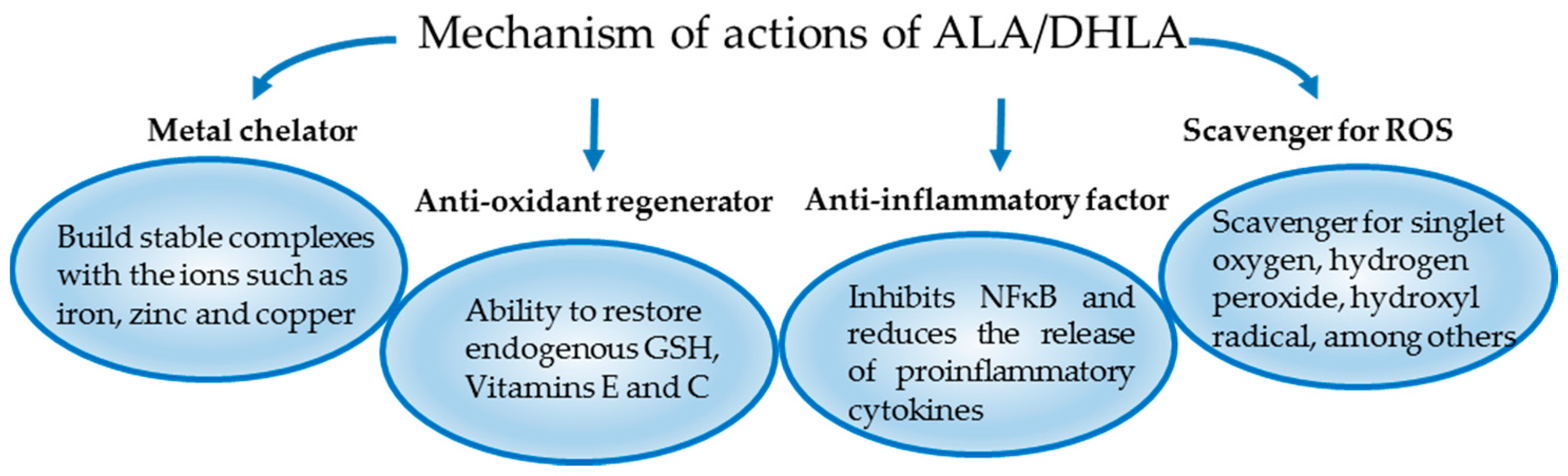
- Packer, L. Alpha-lipoic acid: A metabolic antioxidant which regulates NF-kappa B signal transduction and protects against oxidative injury. Drug Metab. Rev. 1998, 30, 245–275. [Google Scholar] [CrossRef] [PubMed]
- Shay, K.P.; Moreau, R.F.; Smith, E.J.; Smith, A.R.; Hagen, T.M. Alpha-lipoic acid as a dietary supplement: Molecular mechanisms and therapeutic potential. Biochim. Biophys. Acta 2009, 1790, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Reed, L.J. From lipoic acid to multi-enzyme complexes. Protein Sci. 1998, 7, 220–224. [Google Scholar] [CrossRef] [PubMed]
- Bilska, A.; Wlodek, L. Lipoic acid—The drug of the future? Pharmacol. Rep. PR 2005, 57, 570–577. [Google Scholar] [PubMed]
- Li, G.; Fu, J.; Zhao, Y.; Ji, K.; Luan, T.; Zang, B. Alpha-lipoic acid exerts anti-inflammatory effects on lipopolysaccharide-stimulated rat mesangial cells via inhibition of nuclear factor kappa B (NF-κb) signaling pathway. Inflammation 2015, 38, 510–519. [Google Scholar] [CrossRef] [PubMed]
- Ying, Z.; Kampfrath, T.; Sun, Q.; Parthasarathy, S.; Rajagopalan, S. Evidence that α-lipoic acid inhibits NF-κB activation independent of its antioxidant function. Inflamm. Res. 2011, 60, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Chang, P.; Liu, J.; Yu, Y.; Cui, S.Y.; Guo, Z.H.; Chen, G.M.; Huang, Q.; Liu, Z.G. Alpha-lipoic acid suppresses extracellular histone-induced release of the infammatory mediator tumor necrosis factor-alpha by macrophages. Cell. Physiol. Biochem. 2017, 42, 2559–2568. [Google Scholar] [CrossRef] [PubMed]
- Cremer, D.R.; Rabeler, R.; Roberts, A.; Lynch, B. Safety evaluation of alpha-lipoic acid (ALA). Regul. Toxicol. Pharmacol. 2006, 46, 29–41. [Google Scholar] [CrossRef] [PubMed]
- Mitsui, Y.; Schmelzer, J.D.; Zollman, P.J.; Mitsui, M.; Tritschler, H.J.; Low, P.A. Alpha-lipoic acid provides neuroprotection from ischemia-reperfusion injury of peripheral nerve. J. Neurol. Sci. 1999, 163, 11–16. [Google Scholar] [CrossRef]
- Cosar, E.; Sahin, F.K.; Koken, G.; Toy, H.; Basarali, K.; Buyukbas, S. The protective effect of alpha-lipoic acid in experimental ovarian ischaemia-reperfusion injury. Aust. N. Z. J. Obstet. Gynaecol. 2007, 47, 499–503. [Google Scholar] [CrossRef] [PubMed]
- Ozbal, S.; Ergur, B.U.; Erbil, G.; Tekmen, I.; Bagriyanik, A.; Cavdar, Z. The effects of α-lipoic acid against testicular ischemia-reperfusion injury in rats. Sci. World J. 2012, 2012, 489248. [Google Scholar] [CrossRef] [PubMed]
- Muller, C.; Dunschede, F.; Koch, E.; Vollmar, A.M.; Kiemer, A.K. Alpha-lipoic acid preconditioning reduces ischemia-reperfusion injury of the rat liver via the PI3-kinase/Akt pathway. Am. J. Physiol. Gastrointest. Liver Physiol. 2003, 285, 769–778. [Google Scholar] [CrossRef] [PubMed]
- Bae, E.H.; Lee, K.S.; Lee, J.; Ma, S.K.; Kim, N.H.; Choi, K.C.; Frokiaer, J.; Nielsen, S.; Kim, S.Y.; Kim, S.Z.; et al. Effects of alpha-lipoic acid on ischemia-reperfusion-induced renal dysfunction in rats. Am. J. Physiol. Ren. Physiol. 2008, 294, 272–280. [Google Scholar] [CrossRef] [PubMed]
- Guven, A.; Tunc, T.; Topal, T.; Kul, M.; Korkmaz, A.; Gundogdu, G.; Onguru, O.; Ozturk, H. Alpha-lipoic acid and ebselen prevent ischemia/reperfusion injury in the rat intestine. Surg. Today 2008, 38, 1029–1035. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Liu, B.; Dai, Z.; Zhang, H.F.; Zhang, Y.S.; Luo, X.J.; Ma, Q.L.; Peng, J. Alpha lipoic acid protects heart against myocardial ischemia-reperfusion injury through a mechanism involving aldehyde dehydrogenase 2 activation. Eur. J. Pharmacol. 2012, 678, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Deng, C.; Sun, Z.; Tong, G.; Yi, W.; Ma, L.; Zhao, B.; Cheng, L.; Zhang, J.; Cao, F.; Yi, D. α-lipoic acid reduces infarct size and preserves cardiac function in rat myocardial ischemia/reperfusion injury through activation of PI3k/Akt/Nrf2 pathway. PLoS ONE 2013, 8, e58371. [Google Scholar] [CrossRef] [PubMed]
- Panigrahi, M.; Sadguna, Y.; Shivakumar, B.R.; Kolluri, S.V.; Roy, S.; Packer, L.; Ravindranath, V. Alpha-lipoic acid protects against reperfusion injury following cerebral ischemia in rats. Brain Res. 1996, 717, 184–188. [Google Scholar] [CrossRef]
- Hibbard, L.T. Adnexal torsion. Am. J. Obstet. Gynecol. 1985, 152, 456–461. [Google Scholar] [CrossRef]
- Duenschede, F.; Erbes, K.; Kircher, A.; Westermann, S.; Schad, A.; Riegler, N.; Ewald, P.; Dutkowski, P.; Kiemer, A.K.; Kempski, O.; et al. Protection from hepatic ischemia/reperfusion injury and improvement of liver regeneration by alpha-lipoic acid. Shock 2007, 27, 644–651. [Google Scholar] [CrossRef] [PubMed]
- Cerqueira, N.F.; Hussni, C.A.; Yoshida, W.B. Pathophysiology of mesenteric ischemia/reperfusion: A review. Acta Cir. Bras. 2005, 20, 336–343. [Google Scholar] [CrossRef] [PubMed]
- Deitch, E.A. Multiple organ failure. Pathophysiology and potential future therapy. Ann. Surg. 1992, 216, 117–134. [Google Scholar] [CrossRef] [PubMed]
- Yasuhara, H. Acute mesenteric ischemia: The challenge of gastroenterology. Surg. Today 2005, 35, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Muller, A.; Gabriel, H.; Sies, H.; Terlinden, R.; Fischer, H.; Romer, A. A novel biologically active selenooorganic compound—VII. Biotransformation of ebselen in perfused rat liver. Biochem. Pharmacol. 1988, 37, 1103–1109. [Google Scholar] [CrossRef]
- Ozaki, M.; Nakamura, M.; Teraoka, S.; Ota, K. Ebselen, a novel anti-oxidant compound, protects the rat liver from ischemia-reperfusion injury. Transpl. Int 1997, 10, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Sehirli, O.; Sener, E.; Cetinel, S.; Yuksel, M.; Gedik, N.; Sener, G. Alpha-lipoic acid protects against renal ischaemia-reperfusion injury in rats. Clin. Exp. Pharmacol. Physiol. 2008, 35, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Yu, Y.; Ji, L.; Liang, X.; Zhang, T.; Hai, C.X. Alpha-lipoic acid protects against myocardial ischemia/reperfusion injury via multiple target effects. Food Chem. Toxicol. 2011, 49, 2750–2757. [Google Scholar] [CrossRef] [PubMed]
- Endo, J.; Sano, M.; Katayama, T.; Hishiki, T.; Shinmura, K.; Morizane, S.; Matsuhashi, T.; Katsumata, Y.; Zhang, Y.; Ito, H.; et al. Metabolic remodeling induced by mitochondrial aldehyde stress stimulates tolerance to oxidative stress in the heart. Circ. Res. 2009, 105, 1118–1127. [Google Scholar] [CrossRef] [PubMed]
- Genazzani, A.D.; Shefer, K.; Della Casa, D.; Prati, A.; Napolitano, A.; Manzo, A.; Despini, G.; Simoncini, T. Modulatory effects of alpha-lipoic acid (ALA) administration on insulin sensitivity in obese PCOS patients. J. Endocrinol. Investig. 2017. [Google Scholar] [CrossRef] [PubMed]
- Borcea, V.; Nourooz-Zadeh, J.; Wolff, S.P.; Klevesath, M.; Hofmann, M.; Urich, H.; Wahl, P.; Ziegler, R.; Tritschler, H.; Halliwell, B.; et al. Alpha-lipoic acid decreases oxidative stress even in diabetic patients with poor glycemic control and albuminuria. Free Radic. Biol. Med. 1999, 26, 1495–1500. [Google Scholar] [CrossRef]
- Jariwalla, R.J.; Lalezari, J.; Cenko, D.; Mansour, S.E.; Kumar, A.; Gangapurkar, B.; Nakamura, D. Restoration of blood total glutathione status and lymphocyte function following alpha-lipoic acid supplementation in patients with HIV infection. J. Altern. Complement. Med. 2008, 14, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Papanas, N.; Ziegler, D. Efficacy of α-lipoic acid in diabetic neuropathy. Expert Opin. Pharmacother. 2014, 15, 2721–2731. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, D.; Low, P.A.; Litchy, W.J.; Boulton, A.J.; Vinik, A.I.; Freeman, R.; Samigullin, R.; Tritschler, H.; Munzel, U.; Maus, J.; et al. Efficacy and safety of antioxidant treatment with alpha-lipoic acid over 4 years in diabetic polyneuropathy: The NATHAN 1 trial. Diabetes Care 2011, 34, 2054–2060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziegler, D.; Hanefeld, M.; Ruhnau, K.J.; Hasche, H.; Lobisch, M.; Schutte, K.; Kerum, G.; Malessa, R. Treatment of symptomatic diabetic polyneuropathy with the antioxidant alpha-lipoic acid: A 7-month multicenter randomized controlled trial (ALADIN III study). ALADIN III study group. Alpha-lipoic acid in diabetic neuropathy. Diabetes Care 1999, 22, 1296–1301. [Google Scholar] [CrossRef] [PubMed]
- Carlson, D.A.; Smith, A.R.; Fischer, S.J.; Young, K.L.; Packer, L. The plasma pharmacokinetics of R-(+)-lipoic acid administered as sodium R-(+)-lipoate to healthy human subjects. Altern. Med. Rev. 2007, 12, 343–351. [Google Scholar] [PubMed]
- Packer, L.; Witt, E.H.; Tritschler, H.J. Alpha-lipoic acid as a biological antioxidant. Free Radic. Biol. Med. 1995, 19, 227–250. [Google Scholar] [CrossRef]
- Kim, E.; Park, D.W.; Choi, S.H.; Kim, J.J.; Cho, H.S. A preliminary investigation of alpha-lipoic acid treatment of antipsychotic drug-induced weight gain in patients with schizophrenia. J. Clin. Psychopharmacol. 2008, 28, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Koh, E.H.; Lee, W.J.; Lee, S.A.; Kim, E.H.; Cho, E.H.; Jeong, E.; Kim, D.W.; Kim, M.S.; Park, J.Y.; Park, K.G.; et al. Effects of alpha-lipoic acid on body weight in obese subjects. Am. J. Med. 2011, 124, e1–e8. [Google Scholar] [CrossRef] [PubMed]
- Hadzik, B.; Grass, H.; Mayatepek, E.; Daldrup, T.; Hoehn, T. Fatal non-accidental alpha-lipoic acid intoxication in an adolescent girl. Klin. Padiatr. 2014, 226, 292–294. [Google Scholar] [CrossRef] [PubMed]
- Dunschede, F.; Erbes, K.; Kircher, A.; Westermann, S.; Seifert, J.; Schad, A.; Oliver, K.; Kiemer, A.K.; Theodor, J. Reduction of ischemia reperfusion injury after liver resection and hepatic inflow occlusion by alpha-lipoic acid in humans. World J. Gastroenterol. 2006, 12, 6812–6817. [Google Scholar] [CrossRef] [PubMed]
- Ambrosi, N.; Arrosagaray, V.; Guerrieri, D.; Uva, P.D.; Petroni, J.; Herrera, M.B.; Iovanna, J.L.; Leon, L.; Incardona, C.; Chuluyan, H.E.; et al. α-lipoic acid protects against ischemia-reperfusion injury in simultaneous kidney-pancreas transplantation. Transplantation 2016, 100, 908–915. [Google Scholar] [CrossRef] [PubMed]
- Casciato, P.; Ambrosi, N.; Fiorella, C.; Vasquez, M.; Gadano, A.; de Santibañes, M.; de Santibañes, E.; Zandomeni, M.; Chahdi, M.; Laquinandi, J.; et al. α-lipoc acid improve the short term outcomes in human liver transplantation. In Proceedings of the 2017 American Transplant Congress, Chicago, IL, USA, 29 April–3 May 2017. [Google Scholar]
- Pascual, J.; Zamora, J.; Pirsch, J.D. A systematic review of kidney transplantation from expanded criteria donors. Am. J. Kidney Dis. 2008, 52, 553–586. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Vaquera, S.; Navarro Cabello, M.D.; Lopez-Andreu, M.; Jurado, J.M.; Haad, C.R.; Salas, R.O.; Benot, A.R.; Hernandez, J.P.; Arista, J.C.; Aljama, P. Outcomes in renal transplantation with expanded-criteria donors. Transplant. Proc. 2013, 45, 3595–3598. [Google Scholar] [CrossRef] [PubMed]
- McCully, J.D.; Toyoda, Y.; Wakiyama, H.; Rousou, A.J.; Parker, R.A.; Levitsky, S. Age- and gender-related differences in ischemia/reperfusion injury and cardioprotection: Effects of diazoxide. Ann. Thorac. Surg. 2006, 82, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Liu, Z.; Wang, J.; Wong, G.T.; Cheung, C.W.; Zhang, L.; Chen, C.; Xia, Z.; Irwin, M.G. Susceptibility to myocardial ischemia reperfusion injury at early stage of type 1 diabetes in rats. Cardiovasc. Diabetol. 2013, 12, 133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siedlecki, A.; Irish, W.; Brennan, D.C. Delayed graft function in the kidney transplant. Am. J. Transplant. 2011, 11, 2279–2296. [Google Scholar] [CrossRef] [PubMed]
- Baptista, A.P.; Silva, H.T., Jr.; Pestana, J.O. Influence of deceased donor hemodynamic factors in transplant recipients renal function. J. Bras. Nefrol. 2013, 35, 289–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogawa, K.; Suzuki, K.; Okutsu, M.; Yamazaki, K.; Shinkai, S. The association of elevated reactive oxygen species levels from neutrophils with low-grade inflammation in the elderly. Immun. Ageing 2008, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Lassegue, B.; Griendling, K.K. Reactive oxygen species in hypertension; an update. Am. J. Hypertens. 2004, 17, 852–860. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, S.; Fujita, T.; Shimabukuro, M.; Iwaki, M.; Yamada, Y.; Nakajima, Y.; Nakayama, O.; Makishima, M.; Matsuda, M.; Shimomura, I. Increased oxidative stress in obesity and its impact on metabolic syndrome. J. Clin. Investig. 2004, 114, 1752–1761. [Google Scholar] [CrossRef] [PubMed]
- Schuurs, T.A.; Morariu, A.M.; Ottens, P.J.; ’t Hart, N.A.; Popma, S.H.; Leuvenink, H.G.; Ploeg, R.J. Time-dependent changes in donor brain death related processes. Am. J. Transplant. 2006, 6, 2903–2911. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, C.; Al-Faifi, S.; Chaparro, C.; Waddell, T.; Hadjiliadis, D.; Singer, L.; Keshavjee, S.; Hutcheon, M. The effect of recipient’s age on lung transplant outcome. Am. J. Transplant. 2007, 7, 1271–1277. [Google Scholar] [CrossRef] [PubMed]
- Yarlagadda, S.G.; Coca, S.G.; Formica, R.N., Jr.; Poggio, E.D.; Parikh, C.R. Association between delayed graft function and allograft and patient survival: A systematic review and meta-analysis. Nephrol. Dial. Transplant. 2009, 24, 1039–1047. [Google Scholar] [CrossRef] [PubMed]
- Pollak, R.; Andrisevic, J.H.; Maddux, M.S.; Gruber, S.A.; Paller, M.S. A randomized double-blind trial of the use of human recombinant superoxide dismutase in renal transplantation. Transplantation 1993, 55, 57–60. [Google Scholar] [CrossRef] [PubMed]
- Land, W.; Schneeberger, H.; Schleibner, S.; Illner, W.D.; Abendroth, D.; Rutili, G.; Arfors, K.E.; Messmer, K. The beneficial effect of human recombinant superoxide dismutase on acute and chronic rejection events in recipients of cadaveric renal transplants. Transplantation 1994, 57, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Danilovic, A.; Lucon, A.M.; Srougi, M.; Shimizu, M.H.; Ianhez, L.E.; Nahas, W.C.; Seguro, A.C. Protective effect of N-acetylcysteine on early outcomes of deceased renal transplantation. Transplant. Proc. 2011, 43, 1443–1449. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Tissues and Organs | ALA Administration | N | Outcomes | References | |
|---|---|---|---|---|---|
| TIME SCHEDULE | DOSES | ||||
| Sciatic-tibial nerve | 3 days before and 3 days after surgery | 100 mg/kg/day intraperitoneal (i.p.) | 44 | Distal sensory conduction and fiber degeneration improvement in the short-time ischemia group | Mitsui et al. 1999 [31] |
| Ovary | 21, 9 and 1 h before torsion of the ovary | 36 mg/kg/day i.p. | 32 | Reduced tissue damage, MDA, NO and XO serum levels | Cosar et al. 2007 [32] |
| Testis | 30 min prior to detorsion | 100 mg/kg i.p. | 35 | Reduced testicular cell damage, apoptosis and MDA. | Ozbal et al. 2012 [33] |
| Liver | Ex vivo model: 20 min before ischemia | 50 μM | 15 | Reduced LDH and PNP efflux, NF-κB and AP-1 activation and increased Akt phosphorylation | Müller et al. 2003 [34] |
| In vivo model: 15 min before ischemia | 500 μM i.v. | 15 | Reduced GST plasma levels and improved liver histology | ||
| Kidney | 48 and 24 h before ischemia and at 6 and 24 h after reperfusion | 80 mg/kg i.p. | 17 | Increased creatinine clearance. Attenuated AQP downregulation and Na+ transporters. Reduced the polyuria normalizing the Na+ excretion | Bae et al. 2008 [35] |
| Intestine | 1 day before and 3 days after surgery | 10 mg/kg oral + ebselen (20 mg/kg) intragastrically | 40 | Increased SOD and GPx activity, reduce MDA and PCC levels and improved intestinal histology | Guven et al. 2008 [36] |
| Heart | council house model: 10 min before ischemia | Low dose: 10−8 M High dose: 5 × 10−8 M | 42 | High-dose treatment improved cardiac function, increased ALDH2 activity and decreased reactive aldehydes levels. | He et al. 2012 [37] |
| Heart | 30 min before ischemia | 15 mg/kg i.v. | 120 | Attenuated myocardial infarct size and preserved heart function. Up-regulated Akt phosphorylation and Nrf2 nuclear translocation. Increased expression of HO-1. PI3K inhibition abolished the beneficial effects. | Deng et al. 2013 [38] |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ambrosi, N.; Guerrieri, D.; Caro, F.; Sanchez, F.; Haeublein, G.; Casadei, D.; Incardona, C.; Chuluyan, E. Alpha Lipoic Acid: A Therapeutic Strategy that Tend to Limit the Action of Free Radicals in Transplantation. Int. J. Mol. Sci. 2018, 19, 102. https://doi.org/10.3390/ijms19010102
Ambrosi N, Guerrieri D, Caro F, Sanchez F, Haeublein G, Casadei D, Incardona C, Chuluyan E. Alpha Lipoic Acid: A Therapeutic Strategy that Tend to Limit the Action of Free Radicals in Transplantation. International Journal of Molecular Sciences. 2018; 19(1):102. https://doi.org/10.3390/ijms19010102
Chicago/Turabian StyleAmbrosi, Nella, Diego Guerrieri, Fiorella Caro, Francisco Sanchez, Geraldine Haeublein, Domingo Casadei, Claudio Incardona, and Eduardo Chuluyan. 2018. "Alpha Lipoic Acid: A Therapeutic Strategy that Tend to Limit the Action of Free Radicals in Transplantation" International Journal of Molecular Sciences 19, no. 1: 102. https://doi.org/10.3390/ijms19010102