
Can Early Rehabilitation Prevent Posttraumatic Osteoarthritis in the Patellofemoral Joint after Anterior Cruciate Ligament Rupture? Understanding the Pathological Features

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. Rabbit Exercise Compliance and Health Status
2.2. Histological Observations
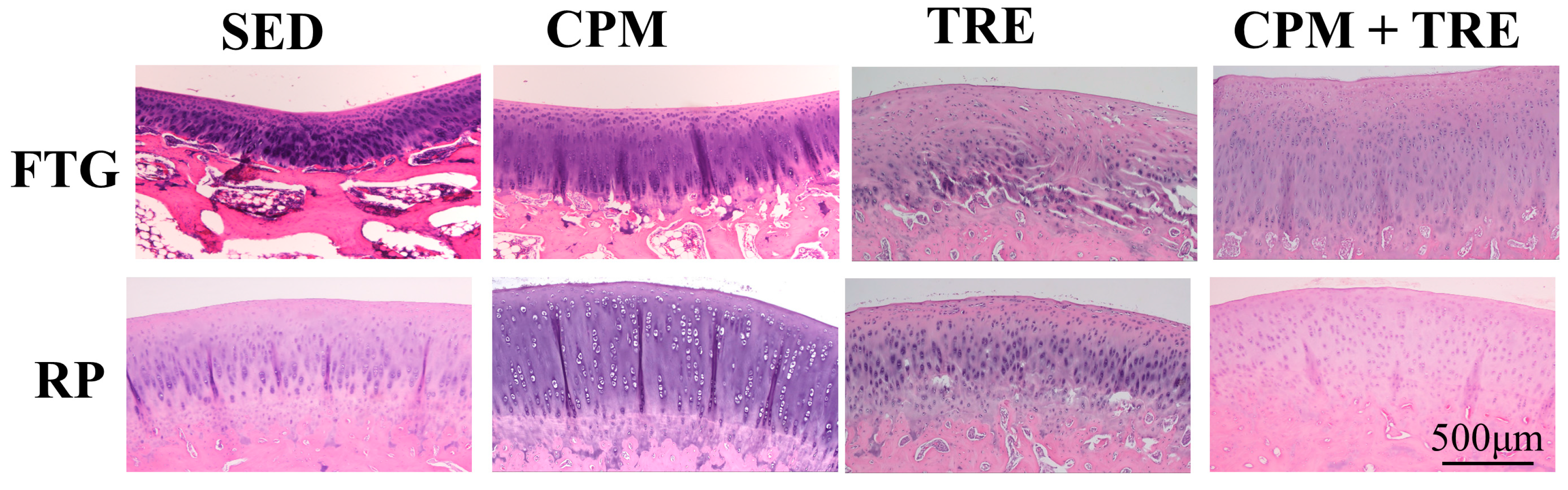
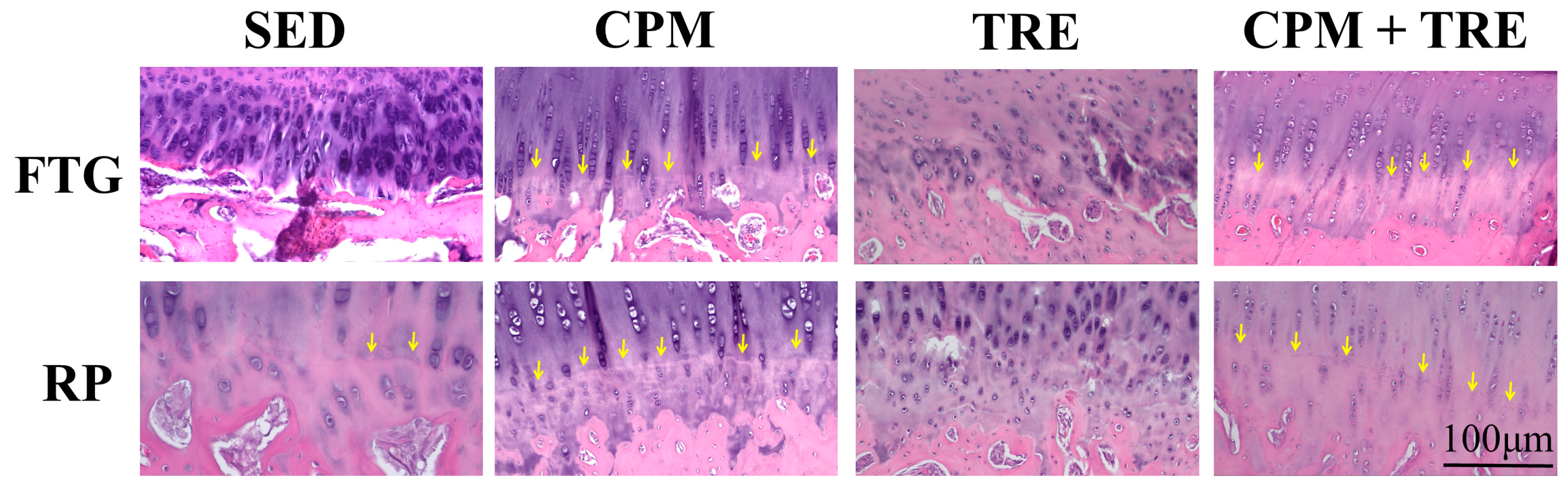
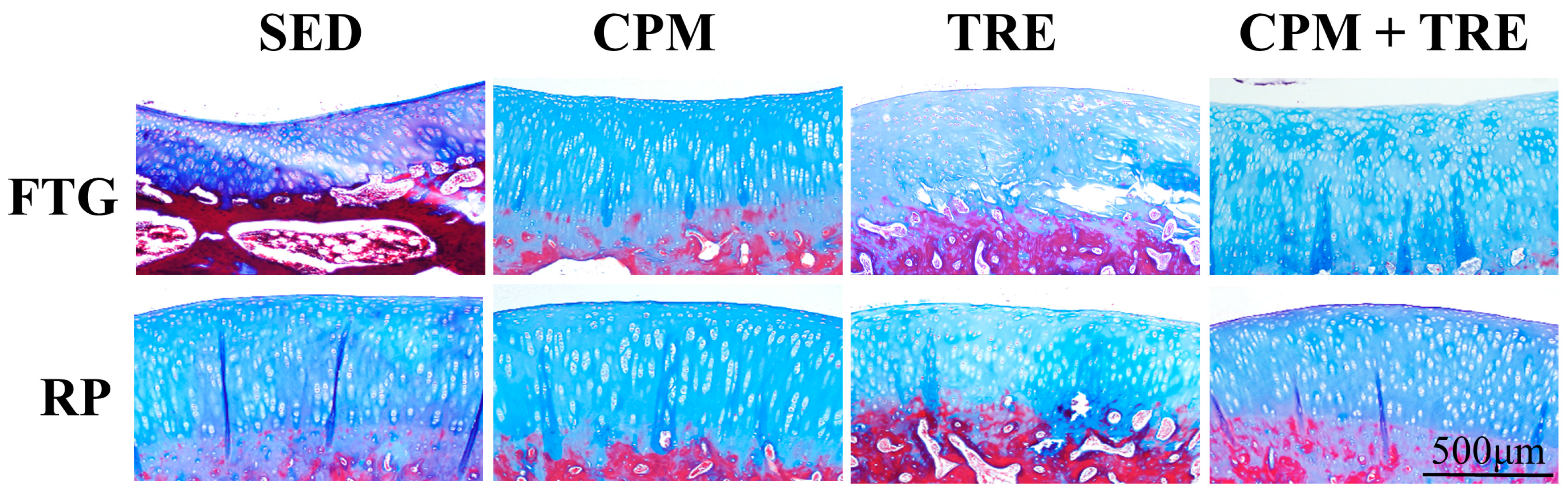
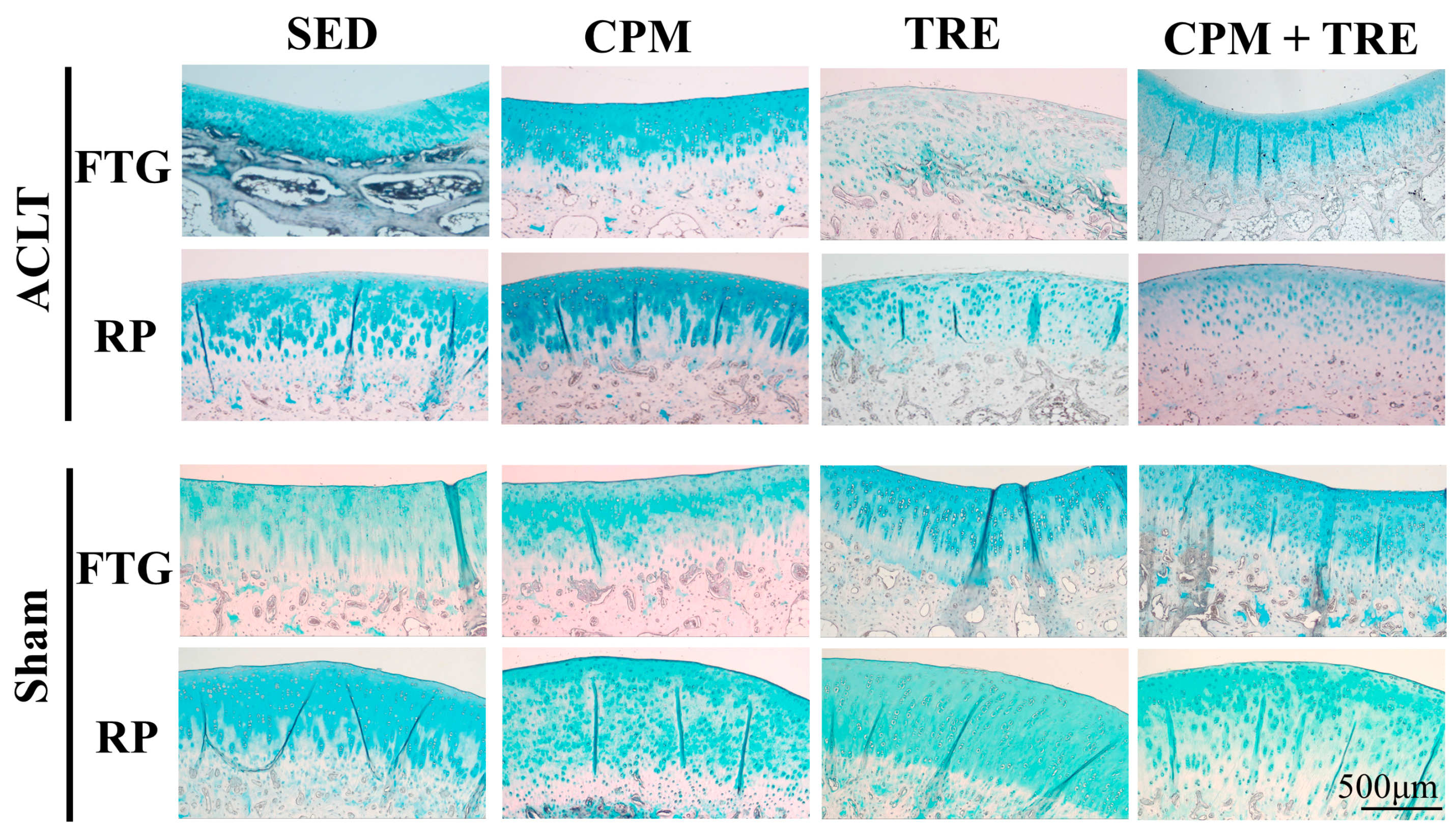
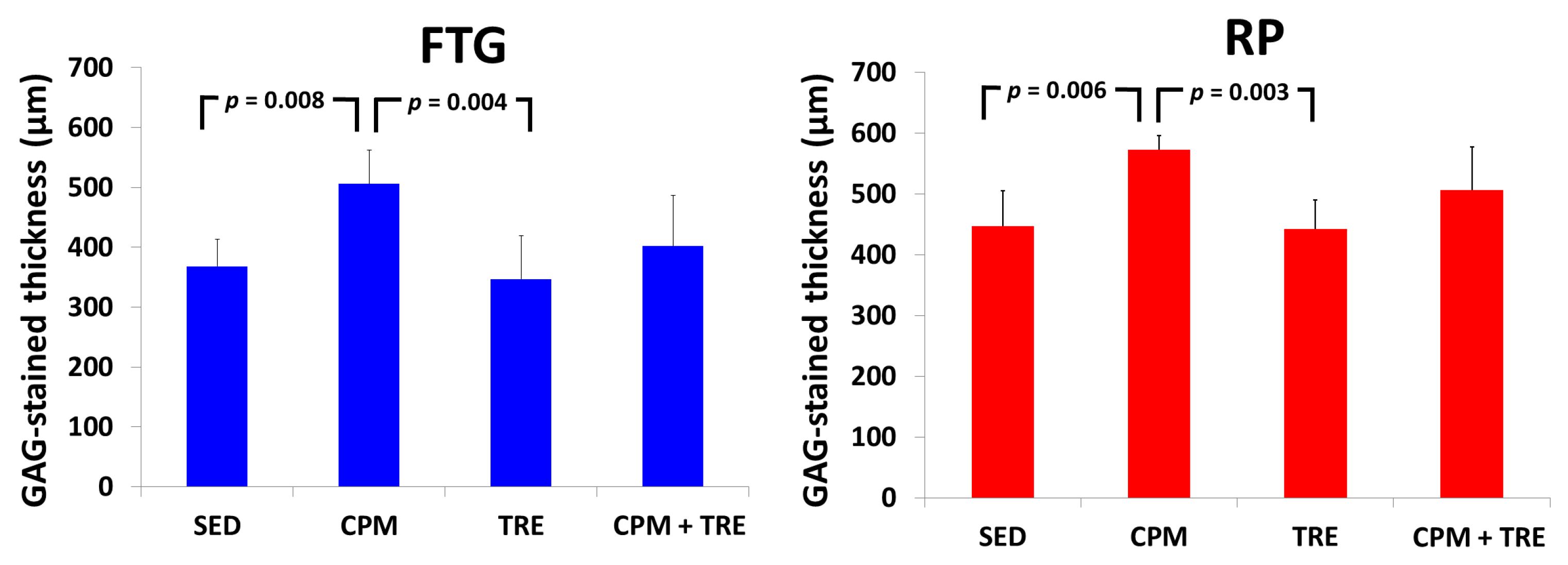
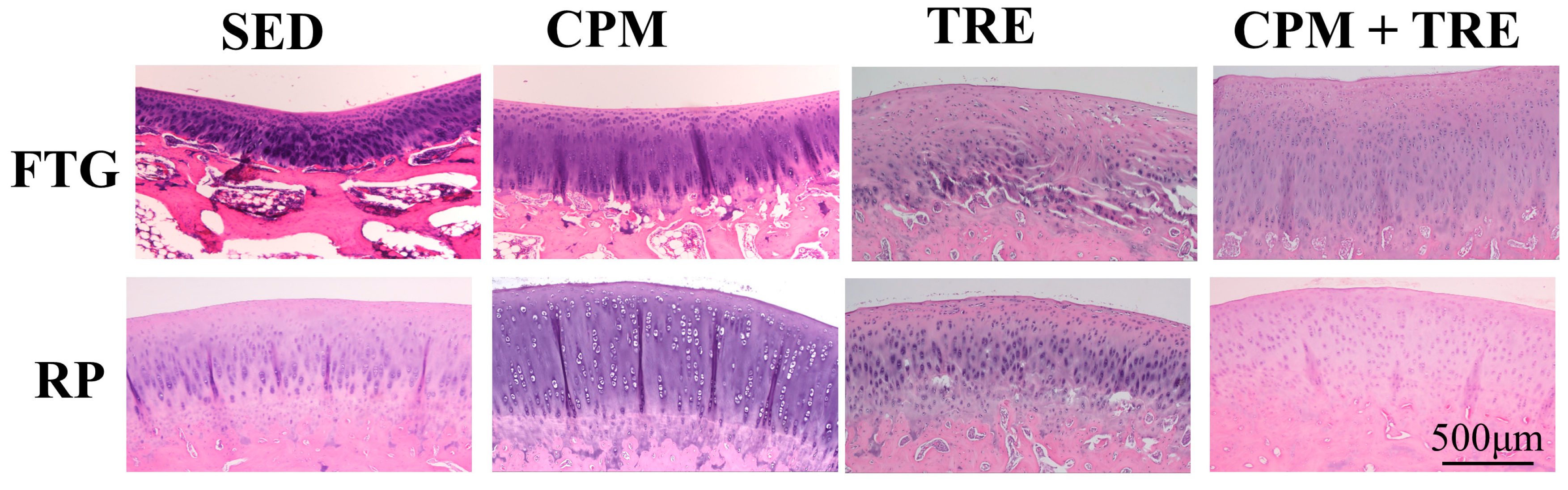
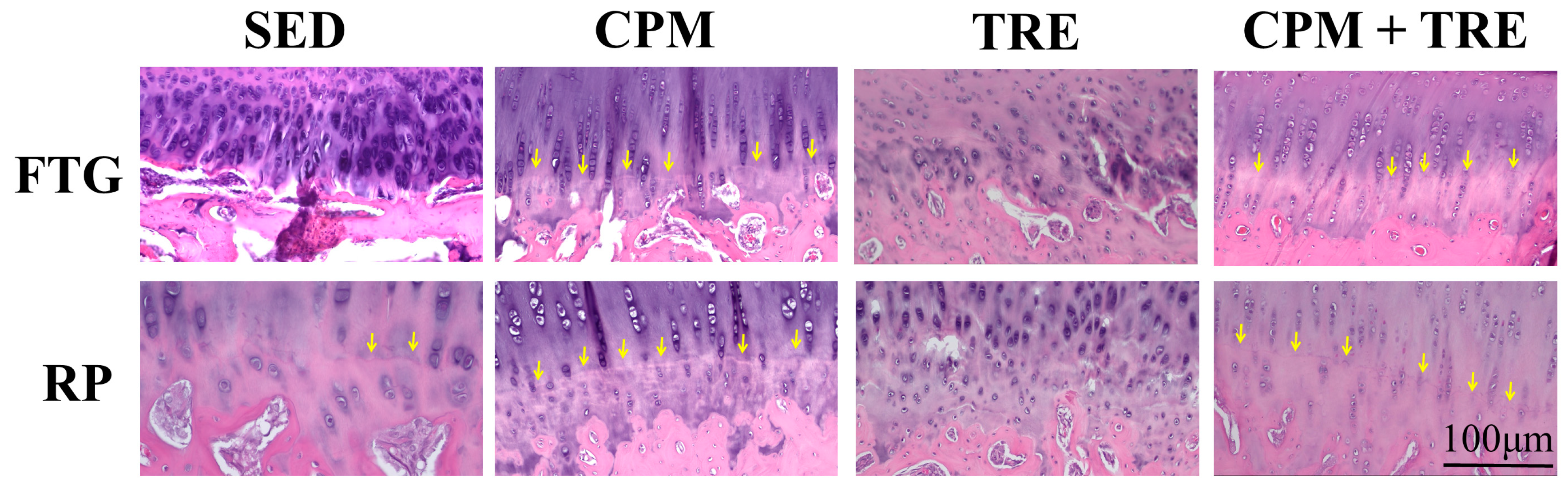
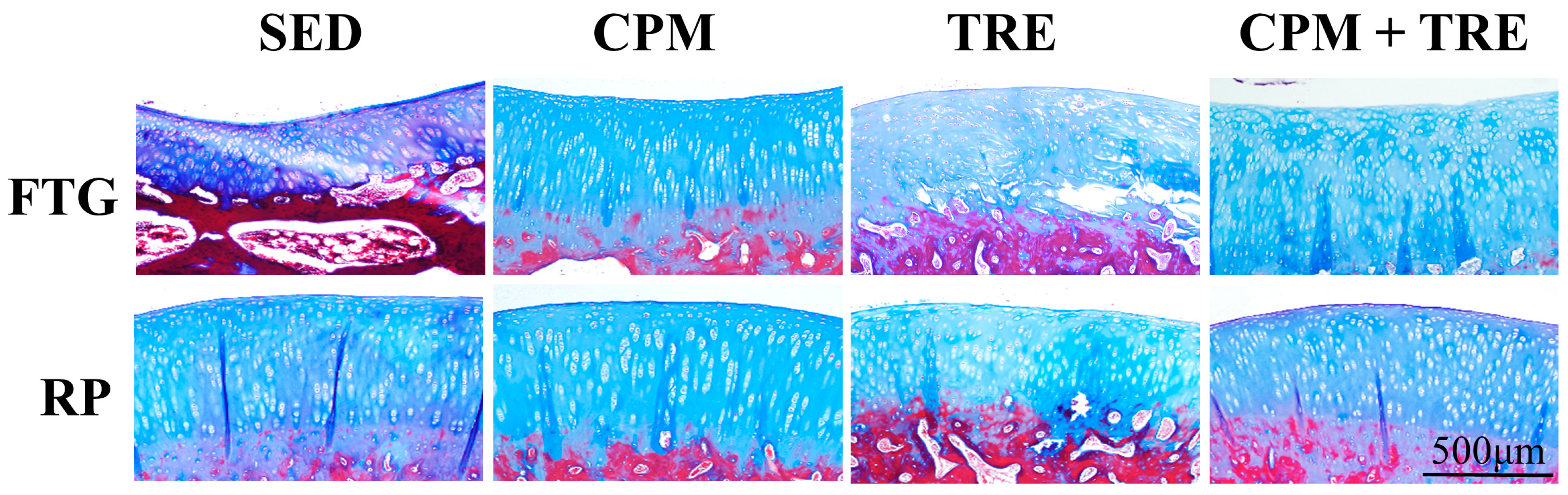
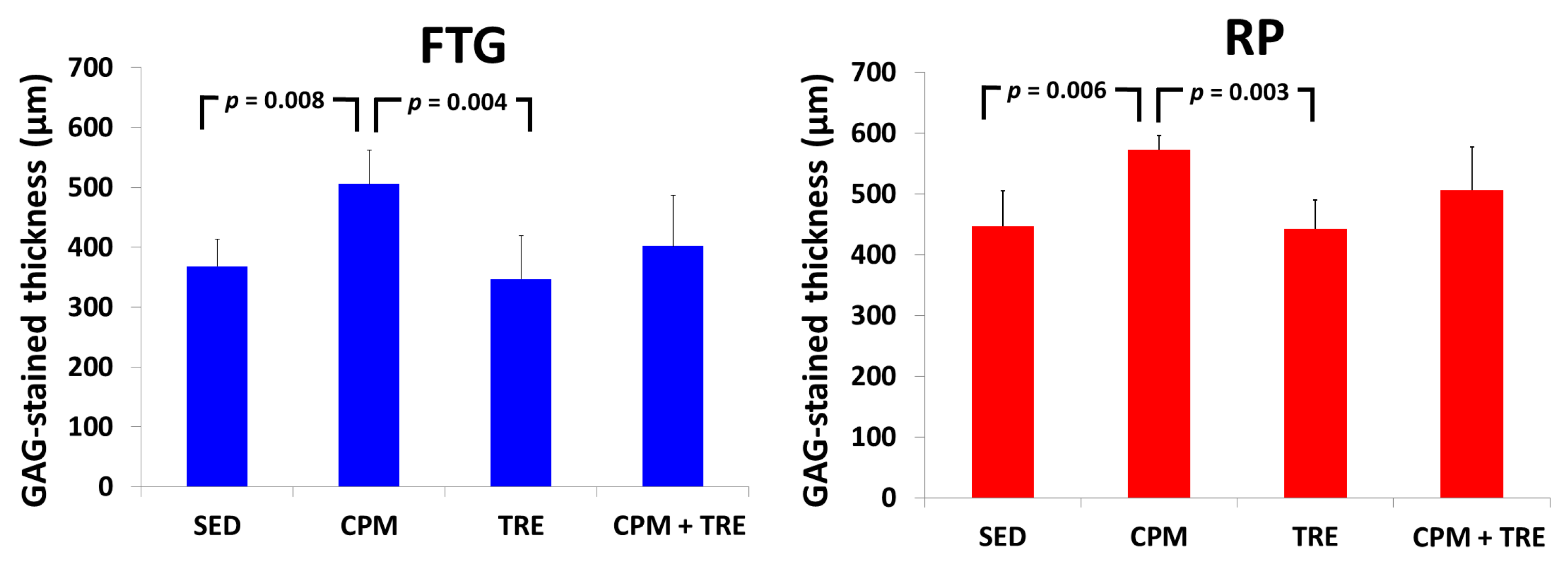
2.2.1. CPM Group Had a Significantly Greater Articular Cartilage Thickness and Maintenance of Tidemark Continuity and More Abundant Glycosaminoglycan (GAG)
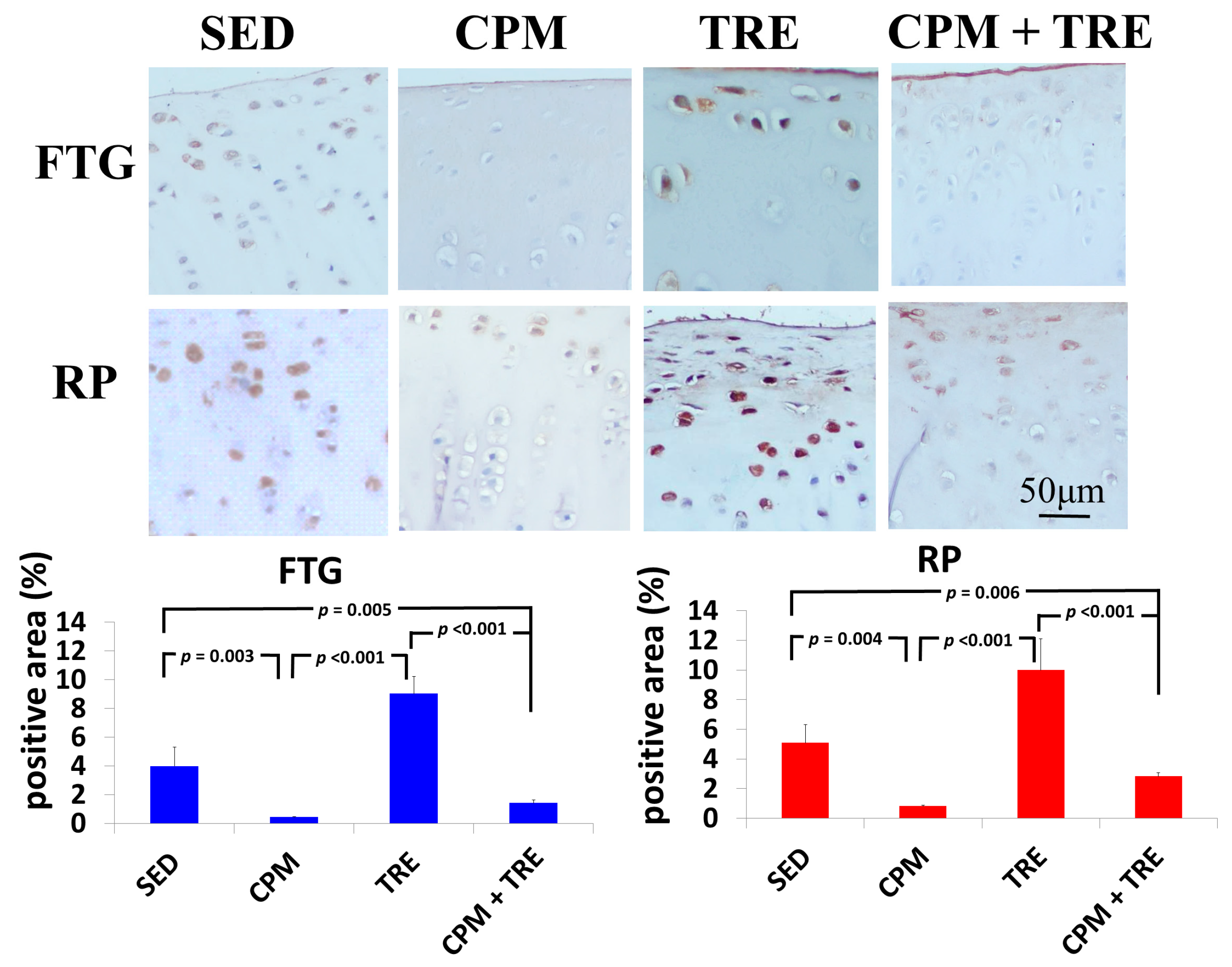
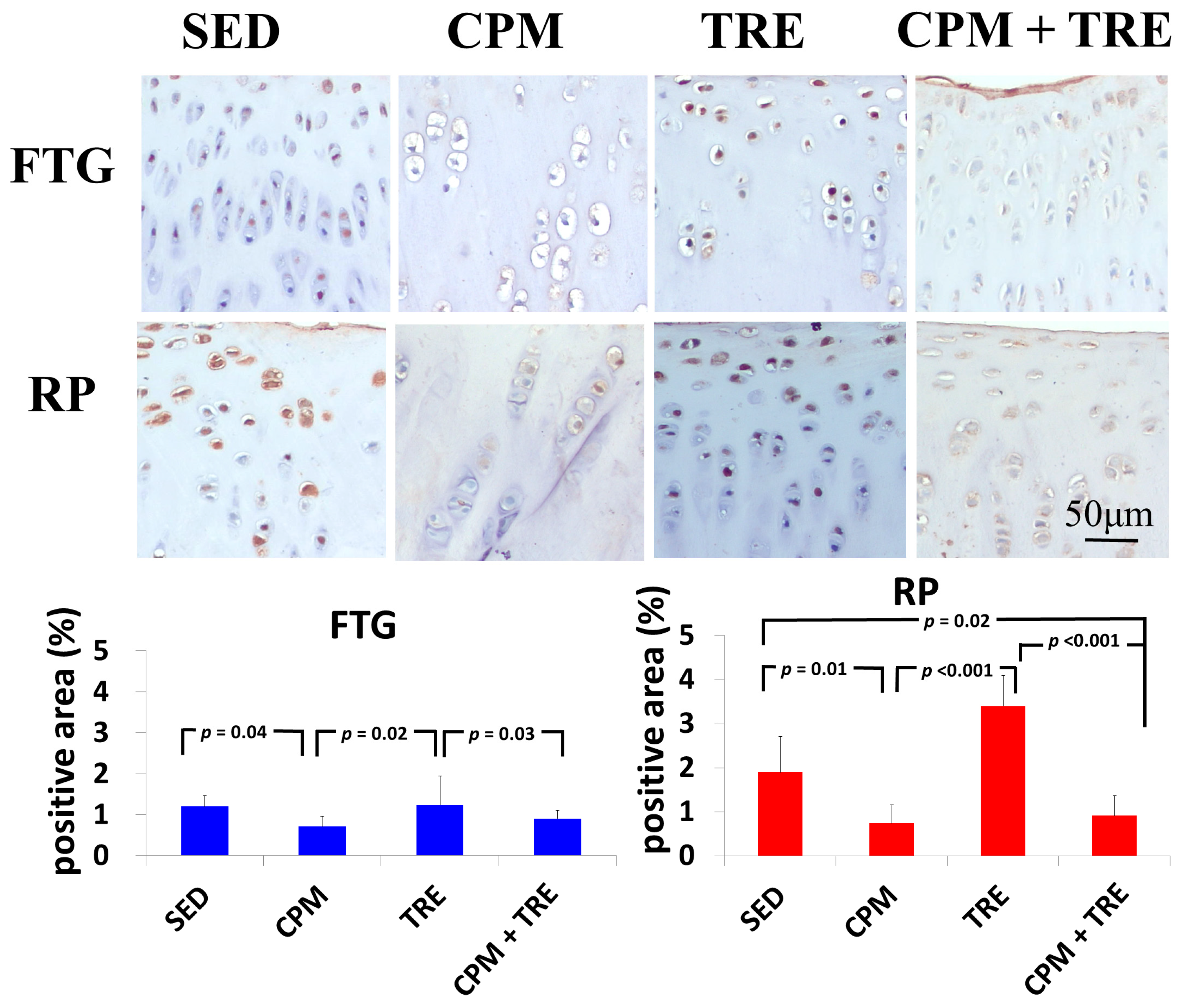
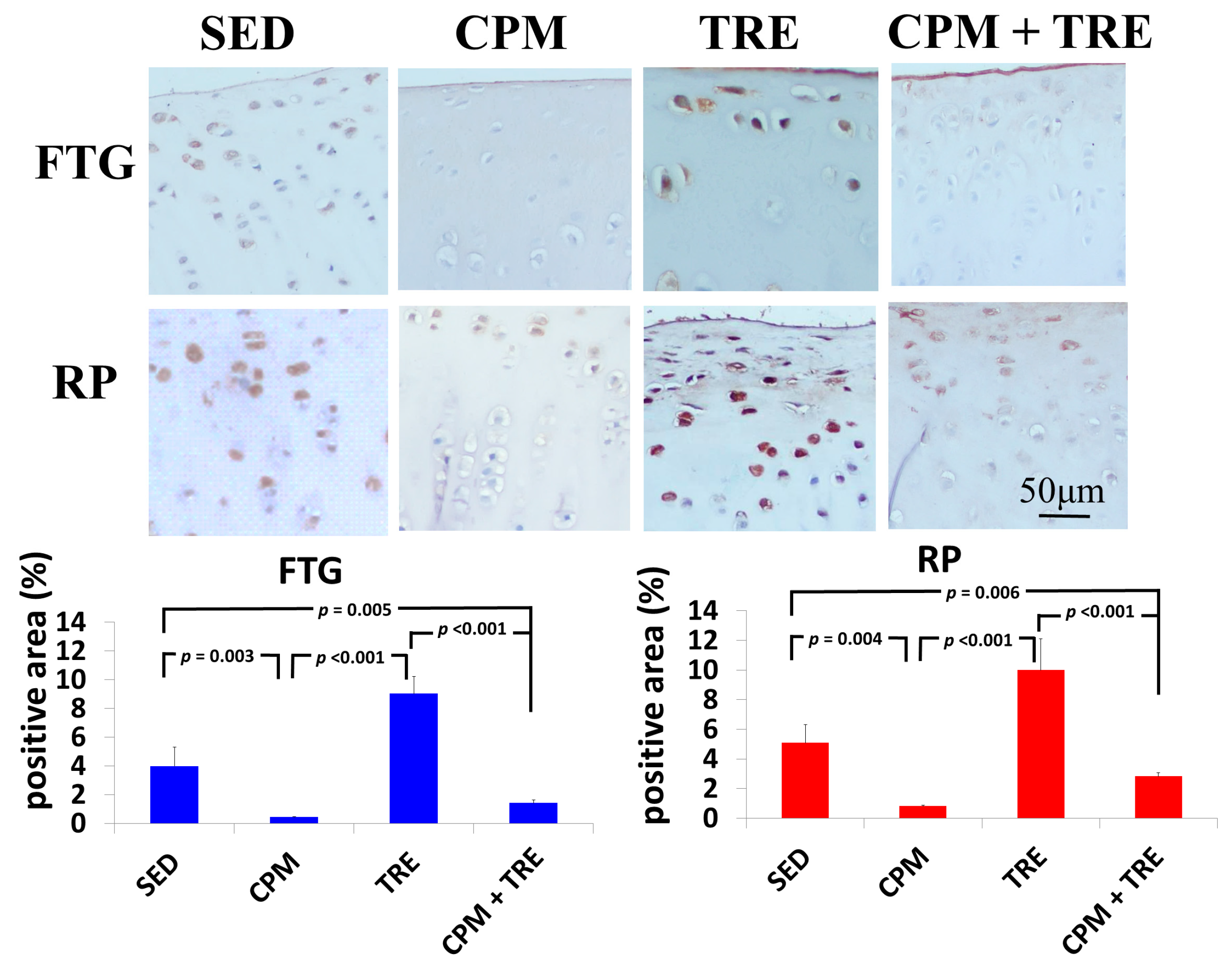
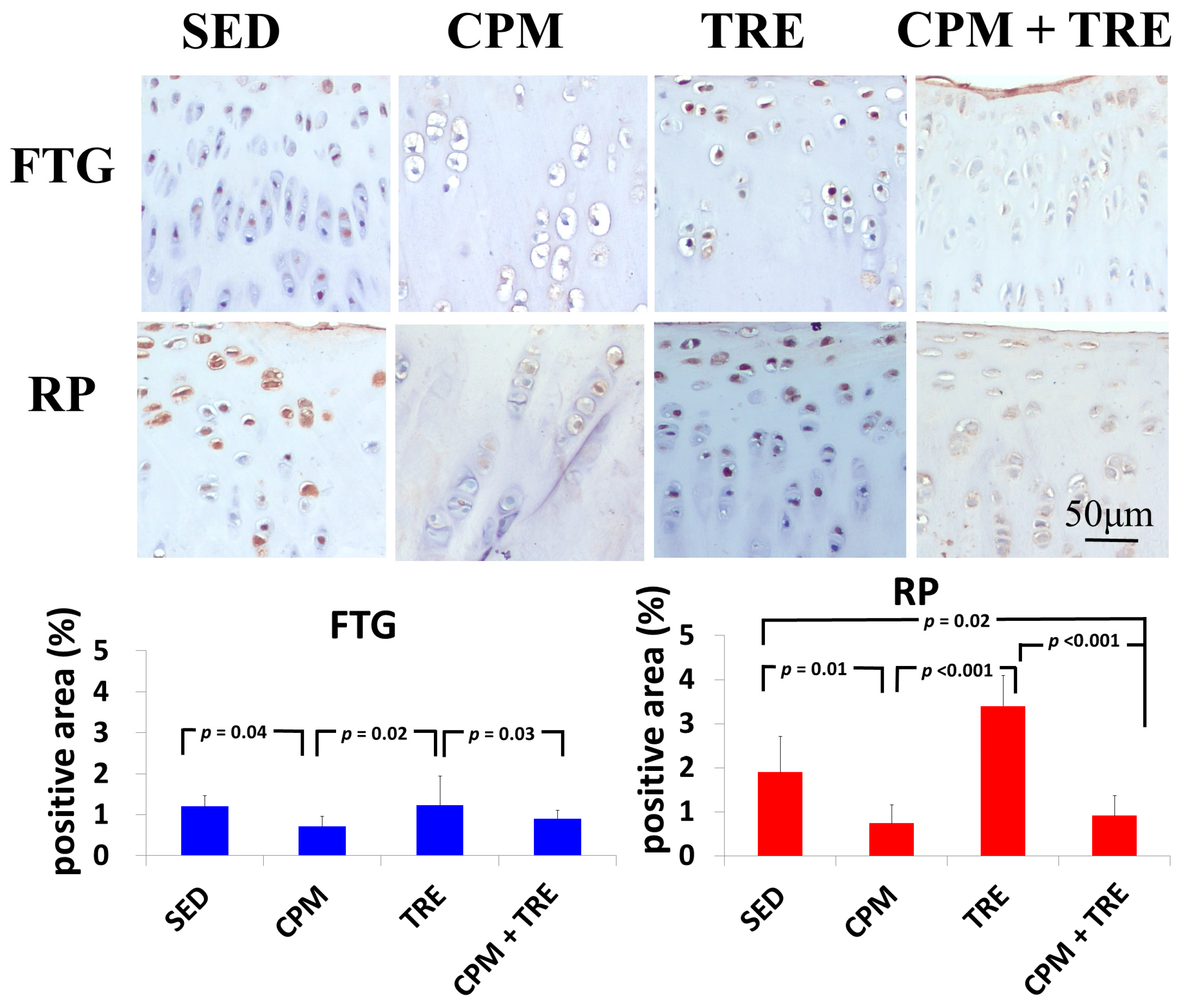
2.2.2. TNF-α and Caspase-3 Expression Increased Significantly (Highest Values) in the TRE Group and Modestly in the CPM Group
3. Discussion
4. Materials and Methods
4.1. An ACLT Model
4.2. Treatment Regimens
4.3. Histological Processing and OA Scores
4.4. Statistics
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| PFJ | Patellofemoral joint |
| TFJ | Tibiofemoral joint |
| FTG | Femoral trochlear groove |
| RP | Retropatella |
| PTOA | Posttraumatic osteoarthritis |
| ACL | Anterior cruciate ligament |
| TNF-α | Tumor necrosis factor-alpha |
| CPM | Continuous passive motion |
| TRE | Treadmill exercise |
| ROM | Range of motion |
| ACLT | Anterior cruciate ligament transection |
| GAG | Glycosaminoglycan |
References
- Hinman, R.S.; Crossley, K.M. Patellofemoral joint osteoarthritis: An important subgroup of knee osteoarthritis. Rheumatology 2007, 46, 1057–1062. [Google Scholar] [CrossRef] [PubMed]
- Peat, G.; Duncan, R.C.; Wood, L.R.; Thomas, E.; Muller, S. Clinical features of symptomatic patellofemoral joint osteoarthritis. Arthritis Res. Ther. 2012, 14, R63. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.M.; Joo, Y.B. Patellofemoral osteoarthritis. Knee Surg. Relat. Res. 2012, 24, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Szebenyi, B.; Hollander, A.P.; Dieppe, P.; Quilty, B.; Duddy, J.; Clarke, S.; Kirwan, J.R. Associations between pain, function, and radiographic features in osteoarthritis of the knee. Arthritis Rheum. 2006, 54, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Duncan, R.C.; Hay, E.M.; Saklatvala, J.; Croft, P.R. Prevalence of radiographic osteoarthritis—It all depends on your point of view. Rheumatology 2006, 45, 757–760. [Google Scholar] [CrossRef] [PubMed]
- Nagelli, C.V.; Cook, J.L.; Kuroki, K.; Bozynski, C.; Ma, R.; Hewett, T.E. Does anterior cruciate ligament innervation matter for joint function and development of osteoarthritis? J. Knee Surg. 2016. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Chen, C.; Chen, S. Posttraumatic knee osteoarthritis following anterior cruciate ligament injury: Potential biochemical mediators of degenerative alteration and specific biochemical markers. Biomed. Rep. 2015, 3, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Frobell, R.B.; Roos, E.M.; Roos, H.P.; Ranstam, J.; Lohmander, L.S. A randomized trial of treatment for acute anterior cruciate ligament tears. N. Engl. J. Med. 2010, 363, 331–342. [Google Scholar] [CrossRef] [PubMed]
- Zietek, P.; Dziedziejko, V.; Safranow, K.; Zietek, J.; Stepien-Slodkowska, M.; Bialecka, M.; Zietek, M.; Kotrych, D.; Kaminski, A.; Kowalska, A. TNF-α concentrations in pre-operative synovial fluid for predicting early post-operative function and pain after fast-track total knee arthroplasty. Knee 2016, 23, 1044–1048. [Google Scholar] [CrossRef] [PubMed]
- Ding, L.J.; Liu, Y.L.; Ma, G.; Jia, Y.Q.; Wei, Y.S.; Liu, X.M. Correlation of acetabular chondrocyte apoptosis with caspase-3 and BCL-2 expression in developmental dislocations of the hip. Genet. Mol. Res. GMR 2016, 15. [Google Scholar] [CrossRef] [PubMed]
- Qian, J.; Liang, J.; Wang, Y.; Wang, H. Effect of passive motion on articular cartilage in rat osteoarthritis. Exp. Ther. Med. 2014, 8, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Chang, N.J.; Lin, C.C.; Li, C.F.; Wang, D.A.; Issariyaku, N.; Yeh, M.L. The combined effects of continuous passive motion treatment and acellular plga implants on osteochondral regeneration in the rabbit. Biomaterials 2012, 33, 3153–3163. [Google Scholar] [CrossRef] [PubMed]
- Bruun-Olsen, V.; Heiberg, K.E.; Mengshoel, A.M. Continuous passive motion as an adjunct to active exercises in early rehabilitation following total knee arthroplasty—A randomized controlled trial. Disabil. Rehabil. 2009, 31, 277–283. [Google Scholar] [CrossRef] [PubMed]
- O’Driscoll, S.W.; Giori, N.J. Continuous passive motion (CPM): Theory and principles of clinical application. J. Rehabil. Res. Dev. 2000, 37, 179–188. [Google Scholar] [PubMed]
- Salter, R.B.; Simmonds, D.F.; Malcolm, B.W.; Rumble, E.J.; MacMichael, D.; Clements, N.D. The biological effect of continuous passive motion on the healing of full-thickness defects in articular cartilage. An experimental investigation in the rabbit. J. Bone Jt. Surg. Am. Vol. 1980, 62, 1232–1251. [Google Scholar] [CrossRef]
- Wright, R.W.; Preston, E.; Fleming, B.C.; Amendola, A.; Andrish, J.T.; Bergfeld, J.A.; Dunn, W.R.; Kaeding, C.; Kuhn, J.E.; Marx, R.G.; et al. A systematic review of anterior cruciate ligament reconstruction rehabilitation: Part I: Continuous passive motion, early weight bearing, postoperative bracing, and home-based rehabilitation. J. Knee Surg. 2008, 21, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.D.; Huang, Y.C.; Chiu, Y.S.; Liou, T.H. Effect of body mass index on knee function outcomes following continuous passive motion in patients with osteoarthritis after total knee replacement: A retrospective study. Physiotherapy 2016. [Google Scholar] [CrossRef] [PubMed]
- Chaudhry, H.; Bhandari, M. Cochrane in CORR (®): Continuous passive motion following total knee arthroplasty in people with arthritis (review). Clin. Thopaedics Relat. Res. 2015, 473, 3348–3354. [Google Scholar] [CrossRef] [PubMed]
- Song, J.Q.; Dong, F.; Li, X.; Xu, C.P.; Cui, Z.; Jiang, N.; Jia, J.J.; Yu, B. Effect of treadmill exercise timing on repair of full-thickness defects of articular cartilage by bone-derived mesenchymal stem cells: An experimental investigation in rats. PLoS ONE 2014, 9, e90858. [Google Scholar] [CrossRef] [PubMed]
- Ni, G.X.; Liu, S.Y.; Lei, L.; Li, Z.; Zhou, Y.Z.; Zhan, L.Q. Intensity-dependent effect of treadmill running on knee articular cartilage in a rat model. BioMed Res. Int. 2013, 2013, 172392. [Google Scholar] [CrossRef] [PubMed]
- Arokoski, M.E.; Tiitu, V.; Jurvelin, J.S.; Korhonen, R.K.; Fick, J.M. Topographical investigation of changes in depth-wise proteoglycan distribution in rabbit femoral articular cartilage at 4 weeks after transection of the anterior cruciate ligament. J. Orthop. Res. 2015, 33, 1278–1286. [Google Scholar] [CrossRef] [PubMed]
- Coyle, C.H.; Henry, S.E.; Haleem, A.M.; O’Malley, M.J.; Chu, C.R. Serum CTXII correlates with articular cartilage degeneration after anterior cruciate ligament transection or arthrotomy followed by standardized exercise. Sports Health 2012, 4, 510–517. [Google Scholar] [CrossRef] [PubMed]
- Teng, C.; Zhou, C.; Xu, D.; Bi, F. Combination of platelet-rich plasma and bone marrow mesenchymal stem cells enhances tendon-bone healing in a rabbit model of anterior cruciate ligament reconstruction. J. Orthop. S. Res. 2016, 11, 96. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Wang, Y.; Cui, W.; Xie, J.W.; Li, J.P.; Yang, J.Y.; Xu, H.S.; Liang, L.Q.; Yang, X.Y.; Lian, F. Transplantation of adipose derived mesenchymal stem cells alleviated osteoarthritis induced with anterior cruciate ligament transection. Zhonghua Yi Xue Za Zhi 2016, 96, 1047–1052. [Google Scholar] [PubMed]
- Hermeto, L.C.; Rossi, R.; Jardim, P.H.; Santana, A.E.; Rinaldi, J.C.; Justulin, L.A. Comparison between two different experimental models of osteoarthritis in rabbits. Intra-articular collagenase injection and anterior cruciate ligament transection. Acta Cir. Bras. 2016, 31, 602–607. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.S.; Lim, S.W.; Lee, I.H.; Lee, T.J.; Kim, J.S.; Han, J.S. Intra-articular injection of a nutritive mixture solution protects articular cartilage from osteoarthritic progression induced by anterior cruciate ligament transection in mature rabbits: A randomized controlled trial. Arthritis Res. Ther. 2007, 9, R8. [Google Scholar] [CrossRef] [PubMed]
- Isaksson, H.; Tolvanen, V.; Finnila, M.A.; Iivarinen, J.; Turunen, A.; Silvast, T.S.; Tuukkanen, J.; Seppanen, K.; Arokoski, J.P.; Brama, P.A.; et al. Long-term voluntary exercise of male mice induces more beneficial effects on cancellous and cortical bone than on the collagenous matrix. Exp. Gerontol. 2009, 44, 708–717. [Google Scholar] [CrossRef] [PubMed]
- Chang, N.J.; Lin, C.C.; Shie, M.Y.; Yeh, M.L.; Li, C.F.; Liang, P.I.; Lee, K.W.; Shen, P.H.; Chu, C.J. Positive effects of cell-free porous PLGA implants and early loading exercise on hyaline cartilage regeneration in rabbits. Acta Biomater. 2015, 28, 128–137. [Google Scholar] [CrossRef] [PubMed]
- Kruse, L.M.; Gray, B.; Wright, R.W. Rehabilitation after anterior cruciate ligament reconstruction: A systematic review. J. Bone Jt. Surg. Am. Vol. 2012, 94, 1737–1748. [Google Scholar] [CrossRef] [PubMed]
- Wright, R.W.; Preston, E.; Fleming, B.C.; Amendola, A.; Andrish, J.T.; Bergfeld, J.A.; Dunn, W.R.; Kaeding, C.; Kuhn, J.E.; Marx, R.G.; et al. A systematic review of anterior cruciate ligament reconstruction rehabilitation: Part II: Open versus closed kinetic chain exercises, neuromuscular electrical stimulation, accelerated rehabilitation, and miscellaneous topics. J. Knee Surg. 2008, 21, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.K.; Park, K.K.; Yoon, S.W.; Kim, S.J.; Chang, C.B.; Seong, S.C. Clinical value of regular passive rom exercise by a physical therapist after total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2009, 17, 1152–1158. [Google Scholar] [CrossRef] [PubMed]
- Martin-Hernandez, C.; Cebamanos-Celma, J.; Molina-Ros, A.; Ballester-Jimenez, J.J.; Ballester-Soleda, J. Regenerated cartilage produced by autogenous periosteal grafts: A histologic and mechanical study in rabbits under the influence of continuous passive motion. Arthrosc. J. Arthrosc. Relat. Surg. 2010, 26, 76–83. [Google Scholar] [CrossRef] [PubMed]
- O’Driscoll, S.W.; Keeley, F.W.; Salter, R.B. Durability of regenerated articular cartilage produced by free autogenous periosteal grafts in major full-thickness defects in joint surfaces under the influence of continuous passive motion. A follow-up report at one year. J. Bone Jt. Surg. Am. Vol. 1988, 70, 595–606. [Google Scholar] [CrossRef]
- Lyons, T.J.; Stoddart, R.W.; McClure, S.F.; McClure, J. The tidemark of the chondro-osseous junction of the normal human knee joint. J. Mol. Histol. 2005, 36, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Teshima, R.; Nawata, K.; Hagino, H.; Morio, Y.; Inoue, M.; Irizawa, Y. Effects of weight bearing on the tidemark and osteochondral junction of articular cartilage: Histomorphometric analyses of 7 normal femoral heads. Acta Orthop. Scand. 1999, 70, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Ferretti, M.; Srinivasan, A.; Deschner, J.; Gassner, R.; Baliko, F.; Piesco, N.; Salter, R.; Agarwal, S. Anti-inflammatory effects of continuous passive motion on meniscal fibrocartilage. J. Orthop. Res. 2005, 23, 1165–1171. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, M.R.; Yates, C.K.; Anderson, M.A.; Yates-McCarthy, J.L. The effects of immediate continuous passive motion on pain during the inflammatory phase of soft tissue healing following anterior cruciate ligament reconstruction. J. Orthop. Sports Phys. Ther. 1993, 17, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Punzi, L.; Galozzi, P.; Luisetto, R.; Favero, M.; Ramonda, R.; Oliviero, F.; Scanu, A. Post-traumatic arthritis: Overview on pathogenic mechanisms and role of inflammation. RMD Open 2016, 2, e000279. [Google Scholar] [CrossRef] [PubMed]

© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, N.-J.; Shie, M.-Y.; Lee, K.-W.; Chou, P.-H.; Lin, C.-C.; Chu, C.-J. Can Early Rehabilitation Prevent Posttraumatic Osteoarthritis in the Patellofemoral Joint after Anterior Cruciate Ligament Rupture? Understanding the Pathological Features. Int. J. Mol. Sci. 2017, 18, 829. https://doi.org/10.3390/ijms18040829
Chang N-J, Shie M-Y, Lee K-W, Chou P-H, Lin C-C, Chu C-J. Can Early Rehabilitation Prevent Posttraumatic Osteoarthritis in the Patellofemoral Joint after Anterior Cruciate Ligament Rupture? Understanding the Pathological Features. International Journal of Molecular Sciences. 2017; 18(4):829. https://doi.org/10.3390/ijms18040829
Chicago/Turabian StyleChang, Nai-Jen, Ming-You Shie, Kuan-Wei Lee, Pei-Hsi Chou, Chih-Chan Lin, and Chih-Jou Chu. 2017. "Can Early Rehabilitation Prevent Posttraumatic Osteoarthritis in the Patellofemoral Joint after Anterior Cruciate Ligament Rupture? Understanding the Pathological Features" International Journal of Molecular Sciences 18, no. 4: 829. https://doi.org/10.3390/ijms18040829