
Combined Use of Delamanid and Bedaquiline to Treat Multidrug-Resistant and Extensively Drug-Resistant Tuberculosis: A Systematic Review

 , ,
, , 
Abstract
:1. Introduction
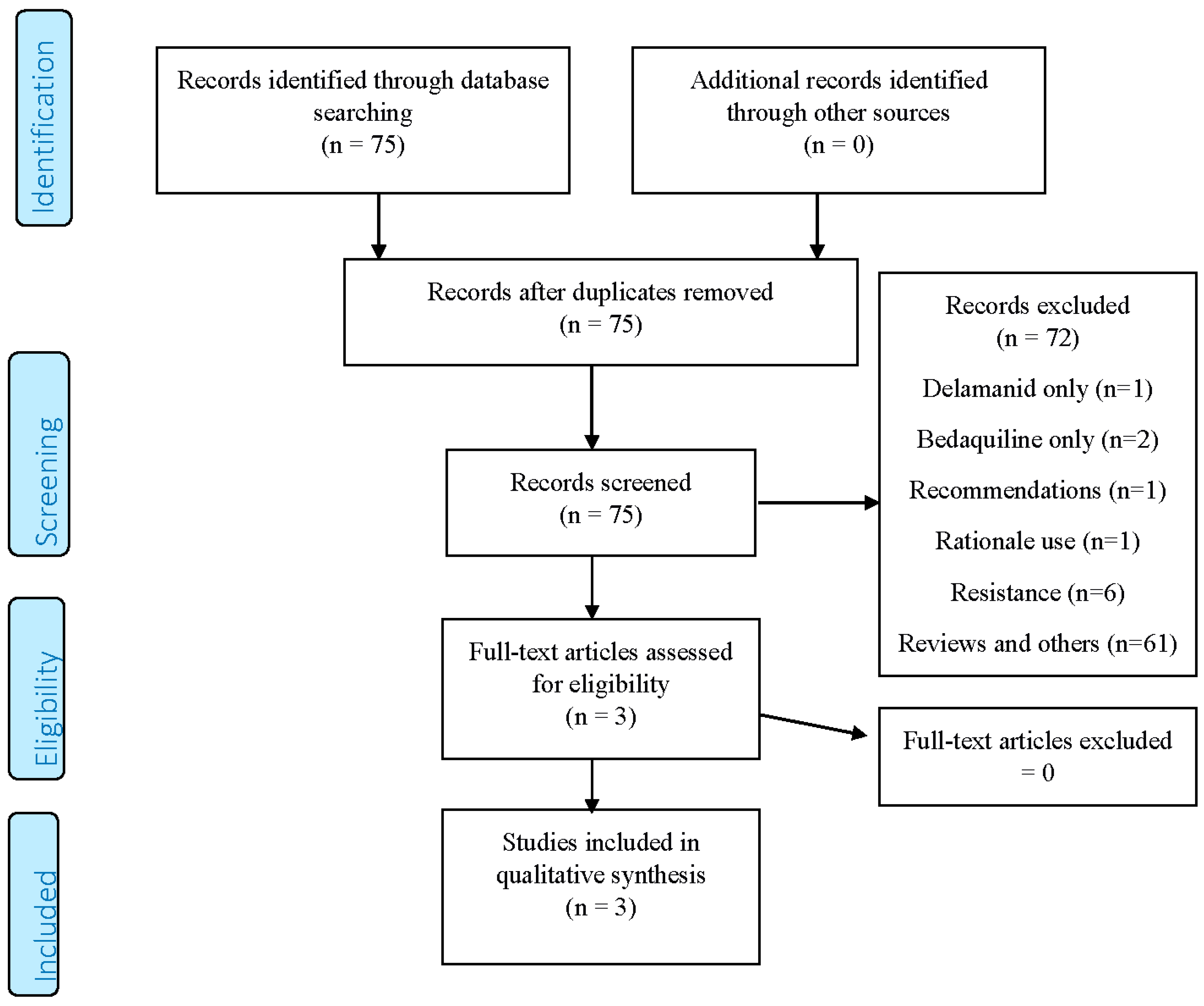
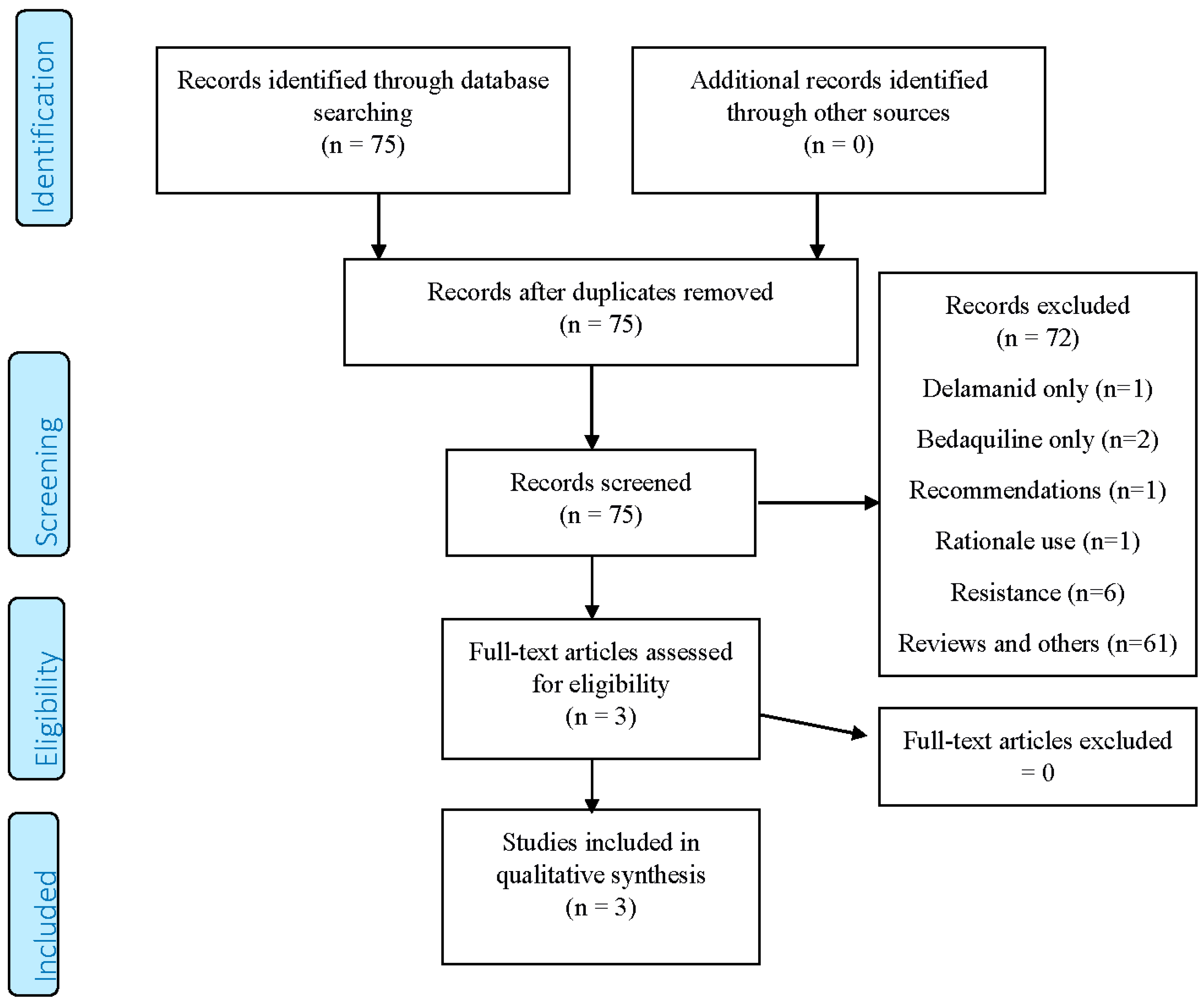
2. Methods
- 1
- Experimental studies on animals with TB;
- 2
- Reviews and editorials on delamanid and bedaquiline;
- 3
- M/XDR-TB diagnosis of treated patients not confirmed with conventional bacteriological criteria.
3. Results
4. Discussion
- In extremely challenging M/XDR-TB cases, when the number of drugs are not enough to reach the recommended number of at least four to design an effective regimen, some clinicians have considered using delamanid and bedaquiline in combination.
- The combination was effective in the two cases observed as it achieved smear and culture conversion, but their number is insufficient to draw any firm conclusions.
- The combination of delamanid and bedaquiline, and, eventually, of other QT interval-prolonging drugs (e.g., fluoroquinolones, clofazimine) is prone to adverse events and potentially harmful QT prolongation [41,46]. The recommendation to obtain and assess a baseline electrocardiogram (ECG) prior to starting the combination treatment and regularly repeat ECGs during treatment with such drugs to monitor the QT interval is not just ‘formal’, but clinically relevant. ECG should be performed at baseline and, then, at regular intervals (e.g., weekly on the first instance and in reduced frequency should QTc prolongation not manifest).
- Electrolytes (potassium and magnesium) as well as albumin should be monitored as electrolyte disturbance and/or hypoalbuminemia (delamanid) may precede QTc prolongation.
- Given the arguments above, only specialised centres should manage patients with delamanid-bedaquiline combined treatment, according to the criteria proposed by Matteelli A. et al. [41].
- As the global experience with combined delamanid-bedaquiline treatment is still very limited, new clinical trials are needed to assess the real efficacy, safety, and tolerability of these drugs in TB cases with complicated drug-resistance patterns.
- Interestingly, both patients made a good clinical improvement on treatment. Surgery was performed on the Congolese patient (who likely benefited from it). However, the Tibetan patient could not afford an operation having bilateral lesions at the chest radiography. The combination regimen may be surgery-sparing; it could be utilised in patients with relative or absolute contraindications for surgery. [43,44,45].
- No published evidence is available in children yet, although clinically-based recommendations have been recently published in this sense [17] and a recent study by Medecins Sans Frontieres (MSF) demonstrates the real need to increase the availability of new drugs [47]. Interestingly, a preliminary report from the MSF projects presented in Liverpool on 24 cases [48] seems to be encouraging.
Author Contributions
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report 2016; WHO/HTM/TB/2016.13; World Health Organization: Geneva, Switzerland, 2016; Available online: http://www.who.int/tb/publications/global_report/en/ (accessed on 30 December 2016).
- Tiberi, S.; D’Ambrosio, L.; de Lorenzo, S.; Viggiani, P.; Centis, R.; Migliori, G.B. Tuberculosis elimination, patients’ lives and rational use of new drugs: Revisited. Eur. Respir. J. 2016. [Google Scholar] [CrossRef] [PubMed]
- Falzon, D.; Gandhi, N.; Migliori, G.B.; Sotgiu, G.; Cox, H.S.; Holtz, T.H.; Hollm-Delgado, M.G.; Keshavjee, S.; de Riemer, K.; Centis, R.; et al. Collaborative Group for Meta-Analysis of Individual Patient Data in MDR-TB. Resistance to fluoroquinolones and second-line injectable drugs: Impact on multidrug-resistant TB outcomes. Eur. Respir. J. 2013, 42, 156–168. [Google Scholar] [CrossRef] [PubMed]
- Migliori, G.B.; Sotgiu, G.; Gandhi, N.R.; Falzon, D.; de Riemer, K.; Centis, R.; Hollm-Delgado, M.G.; Palmero, D.; Pérez-Guzmán, C.; Vargas, M.H.; et al. Collaborative Group for Meta-Analysis of Individual Patient Data in MDR-TB. Drug resistance beyond extensively drug-resistant tuberculosis: Individual patient data meta-analysis. Eur. Respir. J. 2013, 42, 169–179. [Google Scholar] [CrossRef] [PubMed]
- Diel, R.; Rutz, S.; Castell, S.; Schaberg, T. Tuberculosis: Cost of illness in Germany. Eur. Respir. J. 2012, 40, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Diel, R.; Vandeputte, J.; de Vries, G.; Stillo, J.; Wanlin, M.; Nienhaus, A. Costs of tuberculosis disease in the European Union: A systematic analysis and cost calculation. Eur. Respir. J. 2014, 43, 554–565. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Treatment Guidelines for Drug-Resistant Tuberculosis 2016 Update; WHO/HTM/TB 2016.04; World Health Organization: Geneva, Switzerland, 2016; Available online: http://apps.who.int/iris/bitstream/10665/250125/1/9789241549639-eng.pdf (accessed on 30 December 2016).
- Migliori, G.B.; de Iaco, G.; Besozzi, G.; Centis, R.; Cirillo, D.M. First tuberculosis cases in Italy resistant to all tested drugs. Euro Surveill. 2007, 12, E070517.1. [Google Scholar] [PubMed]
- Caminero, J.A.; Scardigli, A. Classification of antituberculosis drugs: A new proposal based on the most recent evidence. Eur. Respir. J. 2015, 46, 887–893. [Google Scholar] [CrossRef] [PubMed]
- Sotgiu, G.; Tiberi, S.; D’Ambrosio, L.; Centis, R.; Alffenaar, J.W.; Caminero, J.A.; Arbex, M.A.; Guizado, V.A.; Aleksa, A.; Dore, S.; et al. Faster for less, the new “Shorter” regimen for multidrug-resistant tuberculosis. Eur. Respir. J. 2016, 48, 1503–1507. [Google Scholar] [CrossRef] [PubMed]
- Falzon, D.; Jaramillo, E.; Schünemann, H.J.; Arentz, M.; Bauer, M.; Bayona, J.; Blanc, L.; Caminero, J.A.; Daley, C.L.; Duncombe, C.; et al. WHO guidelines for the programmatic management of drug-resistant tuberculosis: 2011 update. Eur. Respir. J. 2011, 38, 516–528. [Google Scholar] [CrossRef] [PubMed]
- Tiberi, S.; Scardigli, A.; Centis, R.; D’Ambrosio, L.; Muñoz-Torrico, M.; Salazar-Lezama, M.Á.; Spanevello, A.; Visca, D.; Zumla, A.; Migliori, G.B.; Luna, J.A. Classifying new anti-TB drugs: Rationale and future perspectives. Int. J. Infect. Dis. 2016. [Google Scholar] [CrossRef] [PubMed]
- Sotgiu, G.; Pontali, E.; Centis, R.; D'Ambrosio, L.; Migliori, G.B. New anti-tuberculosis drugs for special populations: A difficult-to-address issue. Eur. Respir. J. 2016. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The Use of Delamanid in the Treatment of Multidrug-Resistant Tuberculosis: Interim Policy Guidance; WHO/HTM/TB2014.23; World Health Organization: Geneva, Switzerland, 2014; Available online: http://apps.who.int/iris/bitstream/10665/137334/1/WHO_HTM_TB_2014.23_eng.pdf (accessed on 30 December 2016).
- World Health Organization. The Use of Bedaquiline in the Treatment of Multidrug-Resistant Tuberculosis: Interim Policy Guidance; WHO/HTM/TB/2013.6; World Health Organization: Geneva, Switzerland, 2013; Available online: http://apps.who.int/iris/bitstream/10665/84879/1/9789241505482_eng.pdf (accessed on 30 December 2016).
- World Health Organization. The Use of Delamanid in the Treatment of Multidrug-Resistant Tuberculosis in Children and Adolescents: Interim Policy Guidance; WHO/HTM/TB/2016.14; World Health Organization: Geneva, Switzerland, 2016; Available online: https://www.ghdonline.org/uploads/Delamanid_guideline_child-adol_Oct16.pdf (accessed on 30 December 2016).
- Harausz, E.P.; Garcia-Prats, A.; Seddon, J.A.; Schaaf, H.S.; Hesseling, A.; Achar, J.; Bernheimer, J.; Cruz, A.; D’Ambrosio, L.; Detjen, A.; et al. New Drugs, Repurposed Drugs, and Novel Regimens for Children with Multidrug-Resistant Tuberculosis: Practice-Based Recommendations. Am. J. Respir. Crit. Care Med. 2016. Available online: http://www.atsjournals.org/doi/abs/10.1164/rccm.201606-1227CI?url_ver=Z39.88-2003&rfr_id=ori%3Arid%3Acrossref.org&rfr_dat=cr_pub%3Dpubmed& (accessed on 30 December 2016). [Google Scholar]
- Pontali, E.; Sotgiu, G.; D’Ambrosio, L.; Centis, R.; Migliori, G.B. Bedaquiline and MDR-TB: A systematic and critical analysis of the evidence. Eur. Respir. J. 2016. [Google Scholar] [CrossRef] [PubMed]
- Sotgiu, G.; Pontali, E.; Centis, R.; D’Ambrosio, L.; Migliori, G.B. Delamanid (OPC-67683) for treatment of multi-drug-resistant tuberculosis. Expert Rev. Anti Infect. Ther. 2015, 13, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Tadolini, M.; Garcia-Prats, A.J.; D’Ambrosio, L.; Hewison, C.; Centis, R.; Schaaf, H.S.; Marais, B.J.; Ferreira, H.; Caminero, J.A.; Jonckheere, S.; et al. Compassionate use of new drugs in children and adolescents with multidrug-resistant and extensively-drug resistant tuberculosis: Early experiences and challenges. Eur. Respir. J. 2016, 48, 938–943. [Google Scholar] [CrossRef] [PubMed]
- Esposito, S.; D’Ambrosio, L.; Tadolini, M.; Schaaf, H.S.; Caminero Luna, J.; Marais, B.; Centis, R.; Dara, M.; Matteelli, A.; Blasi, F.; et al. ERS/WHO Tuberculosis Consilium assistance with extensively drug-resistant tuberculosis management in a child: Case study of compassionate delamanid use. Eur. Respir. J. 2014, 44, 811–815. [Google Scholar] [CrossRef] [PubMed]
- Skripconoka, V.; Danilovits, M.; Pehme, L.; Tomson, T.; Skenders, G.; Kummik, T.; Cirule, A.; Leimane, V.; Kurve, A.; Levina, K.; et al. Delamanid improves outcomes and reduces mortality in multidrug-resistant tuberculosis. Eur. Respir. J. 2013, 41, 1393–1400. [Google Scholar] [CrossRef] [PubMed]
- Gler, M.T.; Skripconoka, V.; Sanchez-Garavito, E.; Xiao, H.; Cabrera-Rivero, J.L.; Vargas-Vasquez, D.E.; Gao, M.; Awad, M.; Park, S.K.; Shim, T.S.; et al. Delamanid for multidrug-resistant pulmonary tuberculosis. N. Engl. J. Med. 2012, 366, 2151–2160. [Google Scholar] [CrossRef] [PubMed]
- Pym, A.S.; Diacon, A.H.; Tang, S.J.; Conradie, F.; Danilovits, M.; Chuchottaworn, C.; Vasilyeva, I.; Andries, K.; Bakare, N.; de Marez, T.; et al. Bedaquiline in the treatment of multi- and extensively drug-resistant tuberculosis. Eur. Respir. J. 2016. [Google Scholar] [CrossRef] [PubMed]
- Diacon, A.H.; Pym, A.; Grobusch, M.; Patientia, R.; Rustomjee, R.; Liesl, P.S.; Pistorius, C.; Krause, R.; Bogoshi, M.; Churchyard, G.; et al. The diarylquinoline TMC207 for multidrug-resistant tuberculosis. N. Engl. J. Med. 2009, 360, 2397–2405. [Google Scholar] [CrossRef] [PubMed]
- Diacon, A.H.; Pym, A.; Grobusch, M.P.; de Ios Rios, J.M.; Gotuzzo, E.; Vasilyeva, I.; Leimane, V.; Andries, K.; Bakare, N.; de Marez, T.; et al. Multidrug-resistant tuberculosis and culture conversion with bedaquiline. N. Engl. J. Med. 2014, 371, 723–732. [Google Scholar] [CrossRef] [PubMed]
- ClinicalTrials.gov. A Service of the U.S. National Institutes of Health. Available online: www.clinicaltrials.gov (accessed on 12 January 2017).
- Lienhardt, C.; Nahid, P.; Rich, M.L.; Bansbach, C.; Kendall, E.A.; Churchyard, G.; González-Angulo, L.; D'Ambrosio, L.; Migliori, G.B.; Raviglione, M. Target regimen profiles for treatment of tuberculosis: A WHO document. Eur. Respir. J. 2017. [Google Scholar] [CrossRef] [PubMed]
- Sotgiu, G.; Pontali, E.; Migliori, G.B. Linezolid to treat MDR-/XDR-Tuberculosis: Available evidence and future scenarios. Eur. Respir. J. 2015, 45, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Villar, M.; Sotgiu, G.; D'Ambrosio, L.; Raymundo, E.; Fernandes, L.; Barbedo, J.; Diogo, N.; Lange, C.; Centis, R.; Migliori, G.B. Linezolid safety, tolerability and efficacy to treat multidrug- and extensively drug-resistant tuberculosis. Eur. Respir. J. 2011, 38, 730–733. [Google Scholar] [CrossRef] [PubMed]
- De Lorenzo, S.; Centis, R.; D’Ambrosio, L.; Sotgiu, G.; Migliori, G.B. On linezolid efficacy and tolerability. Eur. Respir. J. 2012, 39, 770–772. [Google Scholar] [CrossRef] [PubMed]
- Sotgiu, G.; Centis, R.; D'Ambrosio, L.; Alffenaar, J.; Anger, H.; Caminero, J.; Castiglia, P.; de Lorenzo, S.; Ferrara, G.; Koh, W.; et al. Efficacy, safety and tolerability of linezolid containing regimens in treating MDR-TB and XDR-TB: Systematic review and meta-analysis. Eur. Respir. J. 2012, 40, 1430–1442. [Google Scholar] [CrossRef] [PubMed]
- Sotgiu, G.; Centis, R.; D’Ambrosio, L.; Spanevello, A.; Migliori, G.B. International Group for the study of Linezolid. Linezolid to treat extensively drug-resistant TB: Retrospective data are confirmed by experimental evidence. Eur. Respir. J. 2013, 42, 288–290. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.; Lee, J.; Carroll, M.W.; Choi, H.; Min, S.; Song, T.; Via, L.E.; Goldfeder, L.C.; Kang, E.; Jin, B.; et al. Linezolid for treatment of chronic extensively drug-resistant tuberculosis. N. Engl. J. Med. 2012, 367, 1508–1518. [Google Scholar] [CrossRef] [PubMed]
- Sotgiu, G.; Centis, R.; D’Ambrosio, L.; Castiglia, P.; Migliori, G.B. Low minimal inhibitory concentrations of linezolid against multidrug-resistant tuberculosis strains. Eur. Respir. J. 2015, 45, 287–289. [Google Scholar] [CrossRef] [PubMed]
- De Lorenzo, S.; Alffenaar, J.W.; Sotgiu, G.; Centis, R.; D’Ambrosio, L.; Tiberi, S.; Bolhuis, M.S.; van Altena, R.; Viggiani, P.; Piana, A.; et al. Efficacy and safety of meropenem-clavulanate added to linezolid-containing regimens in the treatment of MDR-/XDR-TB. Eur. Respir. J. 2013, 41, 1386–1392. [Google Scholar] [CrossRef] [PubMed]
- Tiberi, S.; Payen, M.C.; Sotgiu, G.; D’Ambrosio, L.; Alarcon Guizado, V.; Alffenaar, J.W.; Abdo Arbex, M.; Caminero, J.A.; Centis, R.; de Lorenzo, S.; et al. Effectiveness and safety of meropenem/clavulanate-containing regimens in the treatment of multidrug and extensively drug-resistant tuberculosis. Eur. Respir. J. 2016, 47, 1235–1243. [Google Scholar] [CrossRef] [PubMed]
- Tiberi, S.; Sotgiu, G.; D'Ambrosio, L.; Centis, R.; Abdo Arbex, M.; Alarcon Arrascue, E.; Alffenaar, J.W.; Caminero, J.A.; Gaga, M.; Gualano, G.; et al. Effectiveness and Safety of Imipenem-Clavulanate Added to an Optimized Background Regimen (OBR) versus OBR Control Regimens in the Treatment of Multidrug-Resistant and Extensively Drug-Resistant Tuberculosis. Clin. Infect. Dis. 2016. [Google Scholar] [CrossRef] [PubMed]
- Tiberi, S.; Sotgiu, G.; D’Ambrosio, L.; Centis, R.; Abdo Arbex, M.; Alarcon Arrascue, E.; Alffenaar, J.W.; Caminero, J.A.; Gaga, M.; Gualano, G.; et al. Comparison of effectiveness and safety of imipenem/clavulanate- versus meropenem/clavulanate-containing regimens in the treatment of multidrug and extensively drug-resistant tuberculosis. Eur. Respir. J. 2016. [Google Scholar] [CrossRef]
- Tiberi, S.; D'Ambrosio, L.; de Lorenzo, S.; Viggiani, P.; Centis, R.; Sotgiu, G.; Alffenaar, J.W. Migliori, G.B. Ertapenem in the treatment of multidrug-resistant tuberculosis: First clinical experience. Eur. Respir. J. 2016, 47, 333–336. [Google Scholar] [CrossRef] [PubMed]
- Matteelli, A.; D'Ambrosio, L.; Centis, R.; Tadolini, M.; Migliori, G.B. Compassionate and optimum use of new tuberculosis drugs. Lancet. Infect. Dis. 2015, 15, 1131–1132. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The Prisma Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Lachâtre, M.; Rioux, C.; Le Dû, D.; Frèchet-Jachym, M.; Veziris, N.; Bouvet, E.; Yazdanpanah, Y. Bedaquiline plus delamanid for XDR tuberculosis. Lancet. Infect. Dis. 2016, 16, 294. [Google Scholar] [CrossRef]
- Tadolini, M.; Lingtsang, R.D.; Tiberi, S.; Enwerem, M.; D’Ambrosio, L.; Sadutshang, T.D.; Centis R Migliori, G.B. First case of extensively drug-resistant tuberculosis treated with both delamanid and bedaquiline. Eur. Respir. J. 2016, 48, 935–938. [Google Scholar] [CrossRef] [PubMed]
- Tadolini, M.; Lingtsang, R.D.; Tiberi, S.; Enwerem, M.; D’Ambrosio, L.; Sadutshang, T.D.; Centis, R.; Migliori, G.B. Cardiac safety of extensively drug-resistant tuberculosis regimens including bedaquiline, delamanid, and clofazimine. Eur. Respir. J. 2016. [Google Scholar] [CrossRef] [PubMed]
- Wallis, R.S. Cardiac safety of extensively drug-resistant tuberculosis regimens including bedaquiline, delamanid and clofazimine. Eur. Respir. J. 2016. [Google Scholar] [CrossRef] [PubMed]
- Bonnet, M.; Bastard, M.; du Cros, P.; Khamraev, A.; Kimenye, K.; Khurkhumal, S.; Hayrapetyan, A.; Themba, D.; Telnov, A.; Sanchez-Padilla, E.; Hewison, C.; Varaine, F. Identification of patients who could benefit from bedaquiline or delamanid: A multisite MDR-TB cohort study. Int. J. Tuberc. Lung Dis. 2016, 20, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Ferlazzo, G. Dlm-Bdq combination: Programmatic aspects and preliminary results of patients receiving Dlm and Bdq combination in MSFNTP projects. Satellite session (SS) 02. Pushing the boundaries: Use of new TB drugs. In Proceedings of the 47th Union World Conference on Lung Health, Liverpool, UK, 26–29 October 2016.
- Conradie, F.; Diacon, A.; Mendel, C.; Everitt, D.; van Niekerk, C.; Howell, P.; Spigelman, M. Interim results of nix-TB clinical study of pretomanid, bedaquiline and linezolid for treatment of XDR and treatment intolerant/failed MDR-TB. In Proceedings of the 47th Union World Conference on Lung Health, Liverpool, UK, 26–29 October 2016.

{kind=link}
| First Author | Publication Year | Country | Study Design | Clinical Setting | Study Duration |
|---|---|---|---|---|---|
| Lachâtre M. [43] | 2016 | France | Case 1 Report | Reference Hospital, Paris, France | March–September 2015 |
| Tadolini M. [44] | 2016 | India | Case 2 Report | Reference Hospital, Dharamshala, India | February–March 2016 |
| Tadolini M. [45] | 2016 | India | Case 2 Report update | Reference Hospital, Dharamshala, India | February–July 2016 |
| First Author | Number of Individuals Exposed to Delamanid + Bedaquiline/HIV Status | Age (Years)/Sex/Country of Birth | XDR-TB/Previous Relapses | Body Weight at the Start of Treatment | Drug Resistance Profile | Regimen Administered (Doses if Available) |
|---|---|---|---|---|---|---|
| Lachâtre M. [43] | 1, HIV ND | 20/male/DR Congo | Yes/ND | ND | ND | delamanid, bedaquiline, ethambutol, para-aminosalicylic acid, linezolid, imipenem, amoxicillin/clavulanate |
| Tadolini M. [44] | 1, HIV negative | 39/female/Tibet | Yes/2 | 65 kg | Resistant to 12 drugs: isoniazid, rifampicin, kanamycin, amikacin, capreomycin, moxifloxacin, ofloxacin, ethionamide, Para-amino-salicylic acid, linezolid, high dose isoniazid, moxifloxacin, Susceptible to: clofazimine | delamanid (200 mg), bedaquiline (400 mg), clofazimine (200 mg), terizidone (1 g), meropenem 1g TID, amoxicillin/clavulanate 1 g/200 mg TID i.v.) |
| Tadolini M. [45] | same as above | same as above | same as above | same as above | same as above |
| First Author | Sputum Smear Conversion | Sputum Culture Conversion | Treatment Outcome | QT Interval Prolongation | Interruption of Bedaquiline or Delamanid due to Adverse Events |
|---|---|---|---|---|---|
| Lachâtre M. [43] | Yes | Yes | After six months favourable clinical, microbiological, and radiological responses | No | ND |
| Tadolini M. [44] | Yes | Yes | After two months favourable clinical, microbiological, and radiological responses | Yes | Bedaquiline stopped on 7th March 2016 restarted on 12 March 2016 |
| Tadolini M. [45] | Yes (consistent negative sputum smear) | Yes (consistent negative culture) | After six months favourable clinical, microbiological, and radiological responses. Body weight increased 4 kg. | Yes, W5: 508 ms; W7: 500 ms; W8: 508 ms; W12: 512 ms; W13: 510 ms; W15: 507; W16: 520 ms; W17: 501 ms | Not after 12 March 2016 and addition of verapamil |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Migliori, G.B.; Pontali, E.; Sotgiu, G.; Centis, R.; D’Ambrosio, L.; Tiberi, S.; Tadolini, M.; Esposito, S. Combined Use of Delamanid and Bedaquiline to Treat Multidrug-Resistant and Extensively Drug-Resistant Tuberculosis: A Systematic Review. Int. J. Mol. Sci. 2017, 18, 341. https://doi.org/10.3390/ijms18020341
Migliori GB, Pontali E, Sotgiu G, Centis R, D’Ambrosio L, Tiberi S, Tadolini M, Esposito S. Combined Use of Delamanid and Bedaquiline to Treat Multidrug-Resistant and Extensively Drug-Resistant Tuberculosis: A Systematic Review. International Journal of Molecular Sciences. 2017; 18(2):341. https://doi.org/10.3390/ijms18020341
Chicago/Turabian StyleMigliori, Giovanni Battista, Emanuele Pontali, Giovanni Sotgiu, Rosella Centis, Lia D’Ambrosio, Simon Tiberi, Marina Tadolini, and Susanna Esposito. 2017. "Combined Use of Delamanid and Bedaquiline to Treat Multidrug-Resistant and Extensively Drug-Resistant Tuberculosis: A Systematic Review" International Journal of Molecular Sciences 18, no. 2: 341. https://doi.org/10.3390/ijms18020341