
Effect of Silver Diamine Fluoride and Potassium Iodide Treatment on Secondary Caries Prevention and Tooth Discolouration in Cervical Glass Ionomer Cement Restoration

 and
and 
Abstract
:1. Introduction
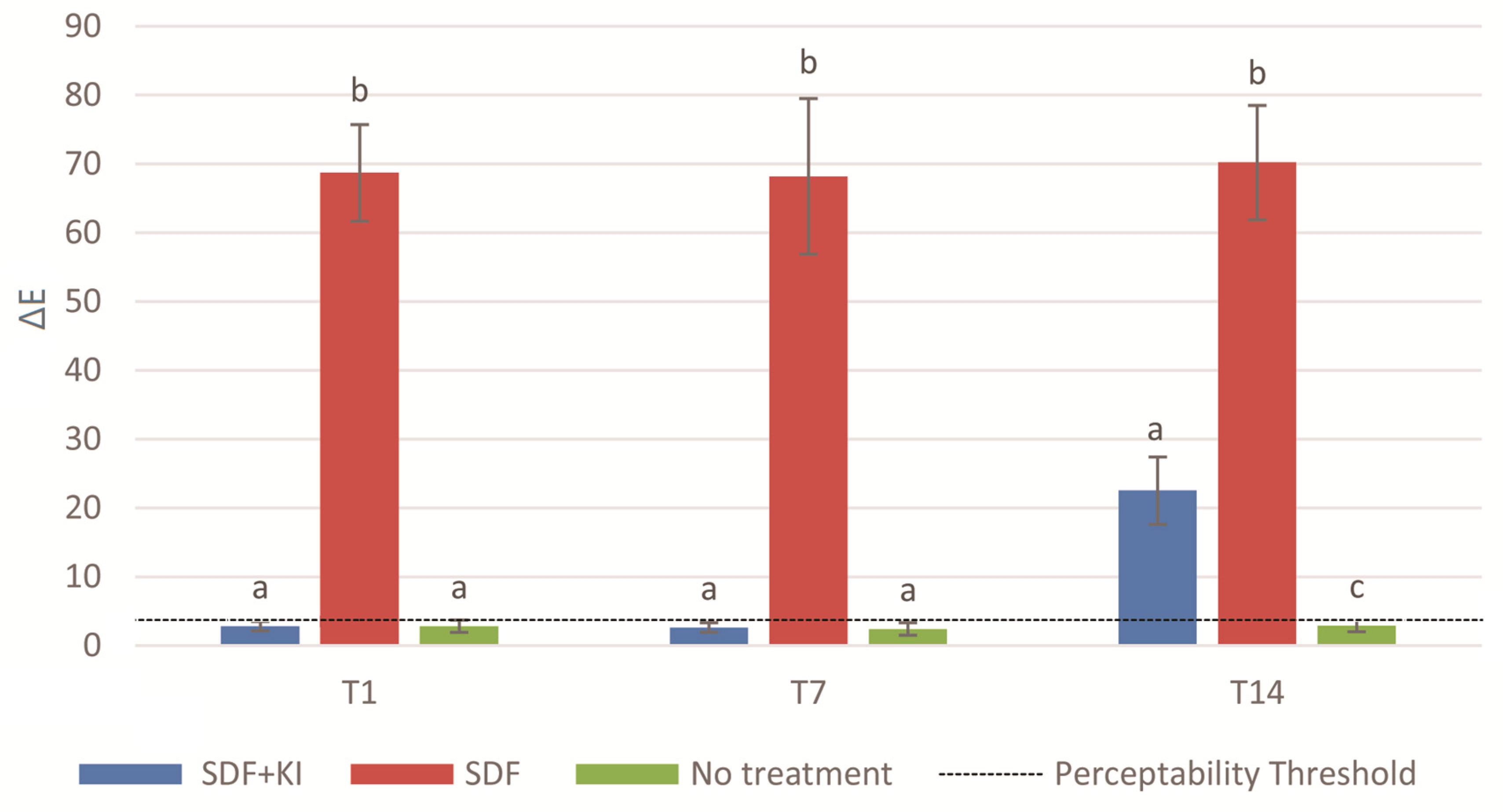
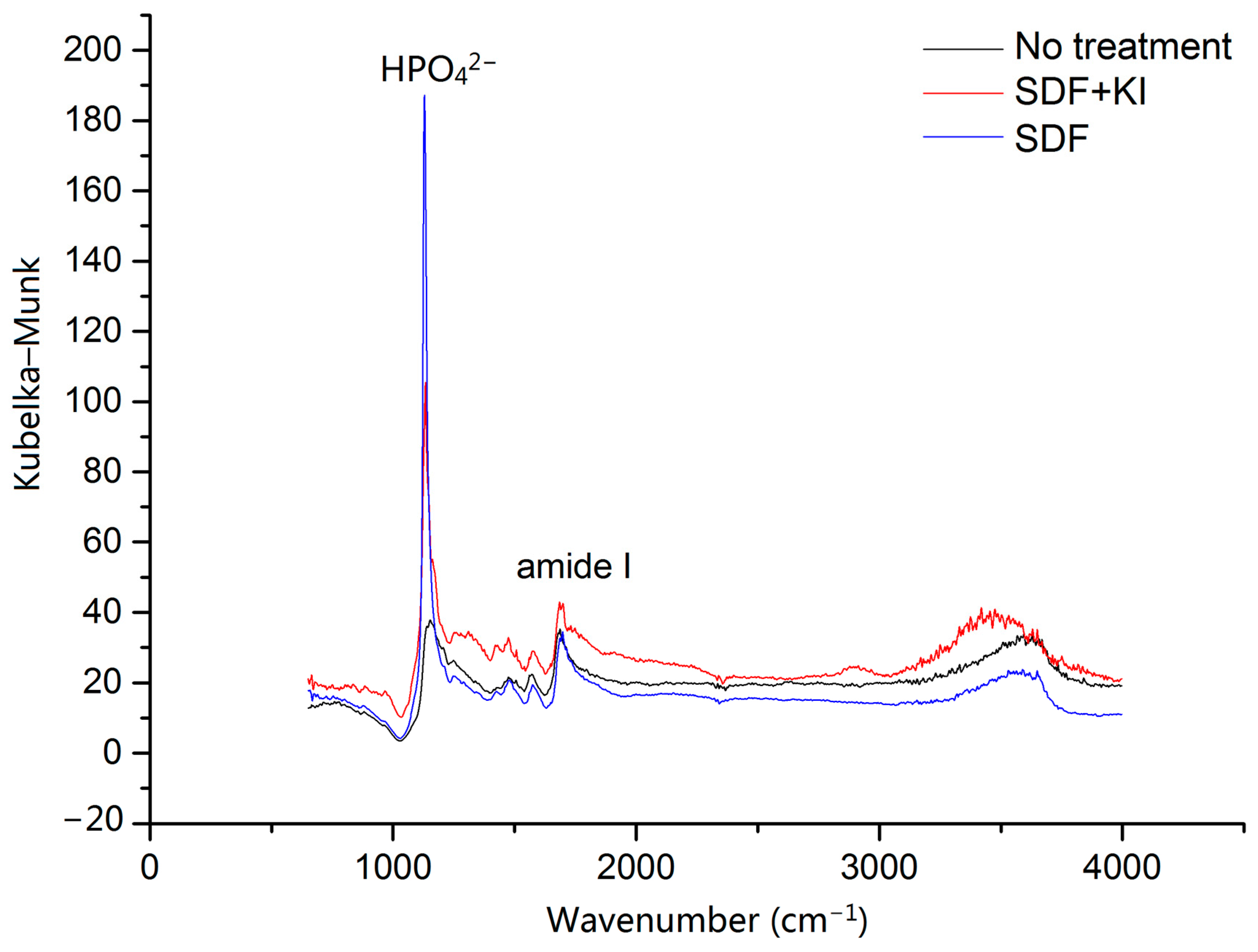
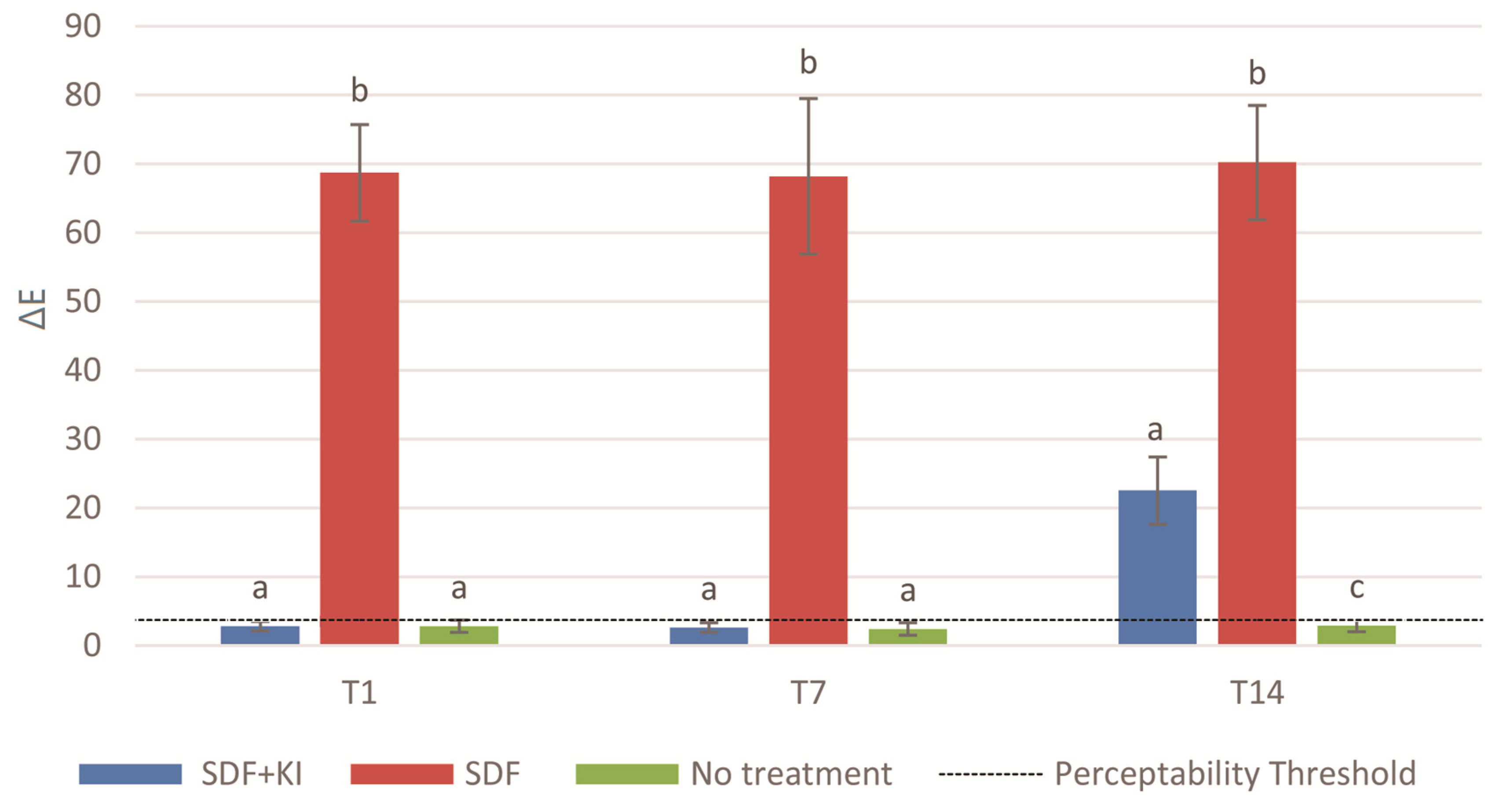
2. Results
3. Discussion
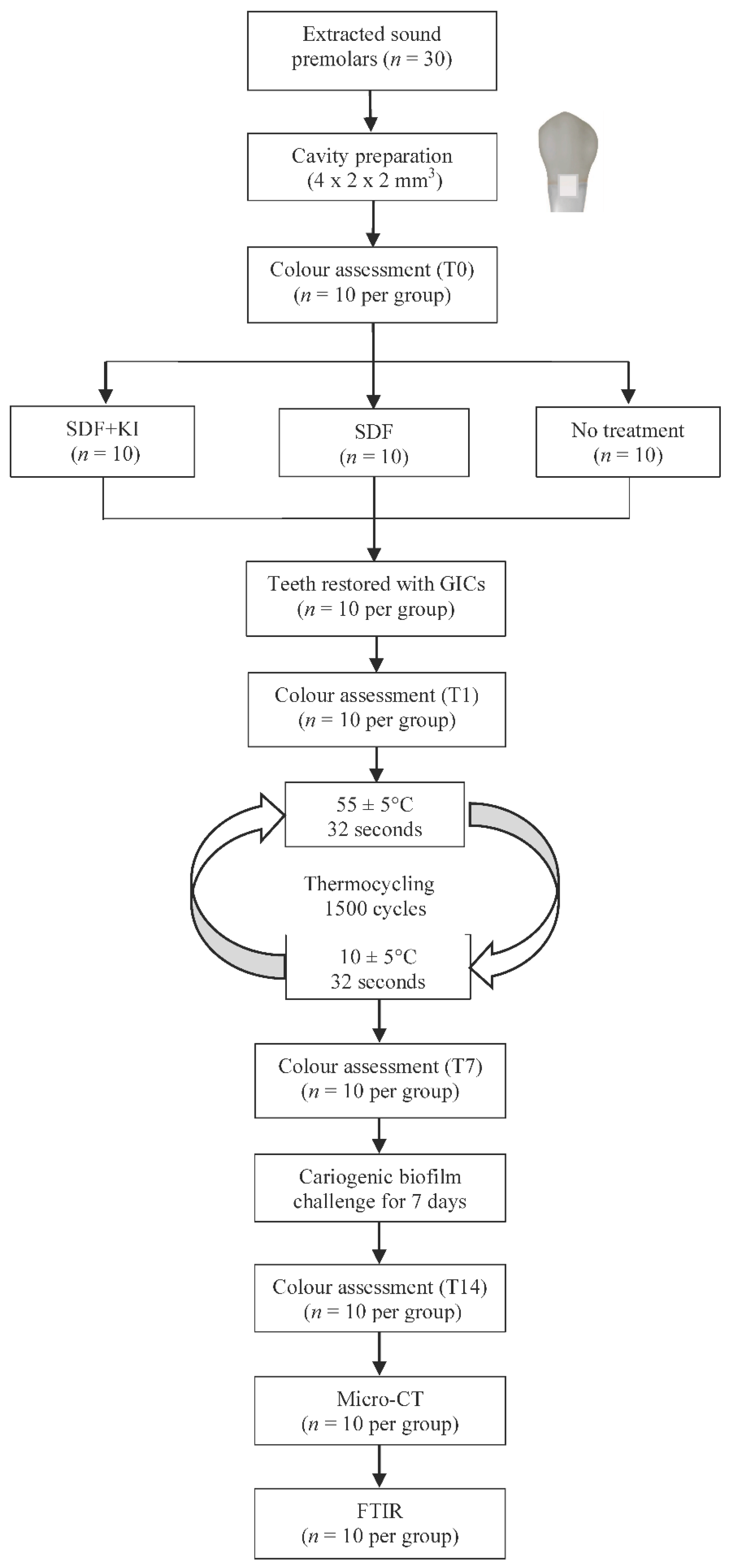
4. Materials and Methods
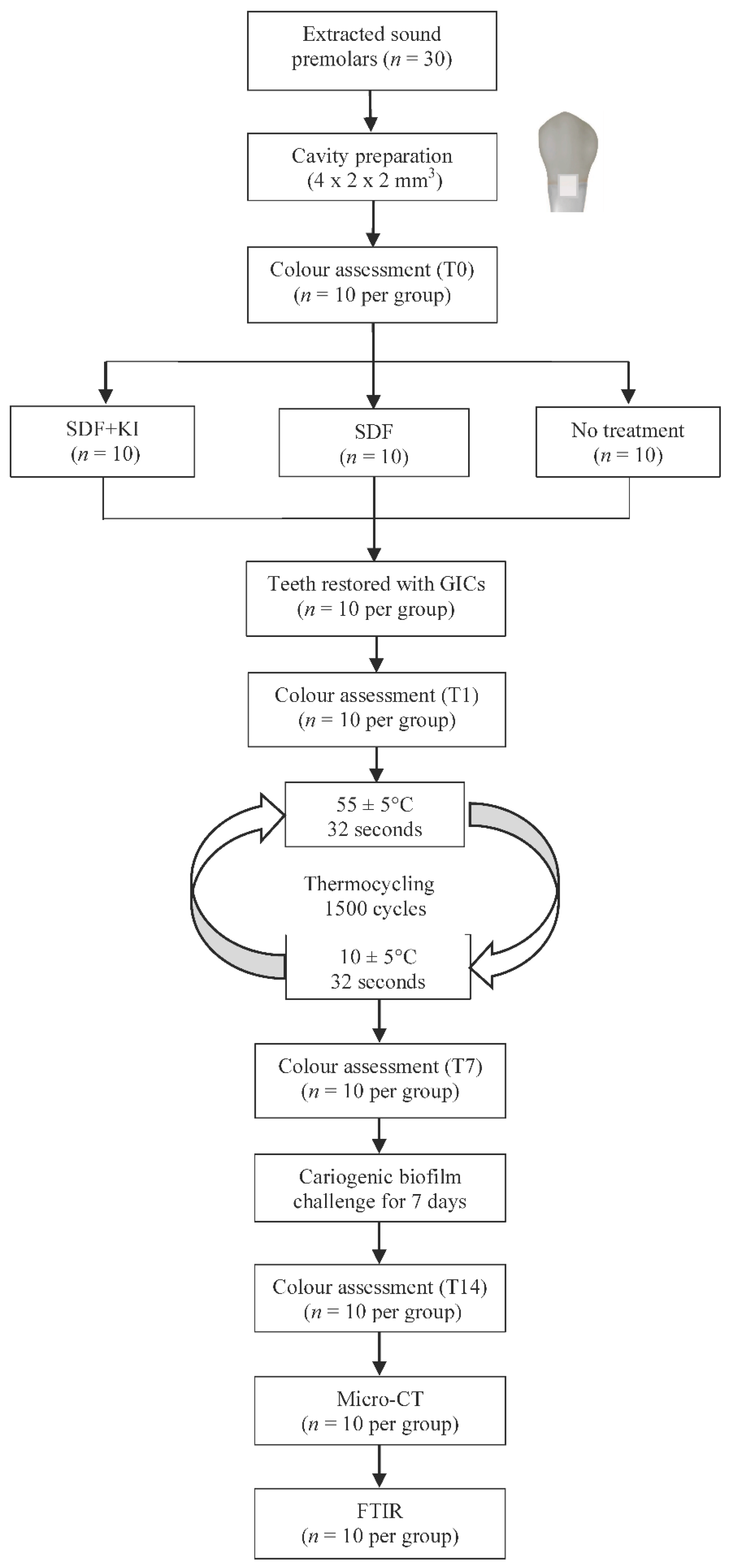
4.1. Specimen Preparation and Materials Selection
- Group 1 (SDF + KI), the cavity was treated with SDF + KI (Riva Star, SDI, Bayswater, Australia). A layer of 38% SDF solution was topically applied to the cavity, immediately followed by a saturated KI solution until the creamy white solution turned clear. The reaction products were washed off with copious distilled water [28]. Then the cavity was dried with oil-free compressed air and filled with GIC (Fuji VII capsule, GC International, Tokyo, Japan).
- Group 2 (SDF), positive control—the cavity was treated with 38% SDF (Saforide; Toyo Seiyaku Kasei Co., Ltd., Osaka, Japan) for 3 min, followed by GIC restoration (Fuji VII capsule).
- Group 3 (no treatment), negative control, the cavity was filled with GIC (Fuji VII capsule).
4.2. Cariogenic Biofilm Challenge
4.3. Colour Assessment
4.4. Outer Lesion Depth Assessment
4.5. Structural Evaluation of Dentine
4.6. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| SDF | Silver diamine fluoride |
| KI | Potassium iodide |
| GIC | Glass ionomer cement |
| Micro-CT | Micro-computed tomography |
| FTIR | Fourier transform infrared |
References
- Montagner, A.F.; Kuper, N.K.; Opdam, N.J.; Bronkhorst, E.M.; Cenci, M.S.; Huysmans, M.C.D. Wall-lesion development in gaps: The role of the adhesive bonding material. J. Dent. 2015, 43, 1007–1012. [Google Scholar] [CrossRef] [PubMed]
- Jokstad, A. Secondary caries and microleakage. Dent. Mater. 2016, 32, 11–25. [Google Scholar] [CrossRef] [PubMed]
- Wilson, N.H.; Burke, F.; Mjör, I.A. Reasons for placement and replacement of restorations of direct restorative materials by a selected group of practitioners in the United Kingdom. Quintessence Int. 1997, 28, 245–248. [Google Scholar] [PubMed]
- Zafar, M.S.; Ahmed, N. Therapeutic roles of fluoride released from restorative dental materials. Fluoride 2015, 48, 184–194. [Google Scholar]
- Mei, M.L.; Zhao, I.S.; Ito, L.; Lo, E.C.; Chu, C.-H. Prevention of secondary caries by silver diamine fluoride. Int. Dent. J. 2015, 66, 71–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mei, M.L.; Li, Q.L.; Chu, C.-H.; Lo, E.M.; Samaranayake, L.P. Antibacterial effects of silver diamine fluoride on multi-species cariogenic biofilm on caries. Ann. Clin. Microbiol. Antimicrob. 2013, 12, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mei, M.L.; Chu, C.-H.; Low, K.H.; Che, C.M.; Lo, E.C.-M. Caries arresting effect of silver diamine fluoride on dentine carious lesion with S. mutans and L. acidophilus dual-species cariogenic biofilm. Med. Oral Patol. Oral Cir. Bucal. 2013, 18, 824–831. [Google Scholar] [CrossRef]
- Chu, C.-H.; Mei, L.; Seneviratne, C.J.; Lo, E.C.-M. Effects of silver diamine fluoride on dentine carious lesions induced by Streptococcus mutans and Actinomyces naeslundii biofilms. Int. J. Paediatr. Dent. 2012, 22, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Mei, M.L.; Lo, E.C.-M.; Chu, C.-H. Clinical Use of Silver Diamine Fluoride in Dental Treatment, Compendium of continuing education in dentistry. Compend. Contin. Educ. Dent. 2016, 37, 93–98. [Google Scholar] [PubMed]
- Rosenblatt, A.; Stamford, T.; Niederman, R. Silver diamine fluoride: A caries “silver-fluoride bullet”. J. Dent. Res. 2009, 88, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.-H.; Lo, E.C.-M.; Lin, H. Effectiveness of silver diamine fluoride and sodium fluoride varnish in arresting dentin caries in Chinese pre-school children. J. Dent. Res. 2002, 81, 767–770. [Google Scholar] [CrossRef] [PubMed]
- Llodra, J.; Rodriguez, A.; Ferrer, B.; Menardia, V.; Ramos, T.; Morato, M. Efficacy of silver diamine fluoride for caries reduction in primary teeth and first permanent molars of schoolchildren: 36-month clinical trial. J. Dent. Res. 2005, 84, 721–724. [Google Scholar] [CrossRef] [PubMed]
- Quock, R.; Barros, J.; Yang, S.; Patel, S. Effect of silver diamine fluoride on microtensile bond strength to dentin. Oper. Dent. 2012, 37, 610–616. [Google Scholar] [CrossRef] [PubMed]
- Gotjamanos, T. Pulp response in primary teeth with deep residual caries treated with silver fluoride and glass ionomer cement (‘atraumatic’technique). Aust. Dent. J. 1996, 41, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Knight, G.; Mclntyre, J.; Craig, G. Ion uptake into demineralized dentine from glass ionomer cement following pretreatment with silver fluoride and potassium iodide. Aust. Dent. J. 2006, 51, 237–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knight, G.; Mclntyre, J. The effect of silver fluoride and potassium iodide on the bond strength of auto cure glass ionomer cement to dentine. Aust. Dent. J. 2006, 51, 42–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, S.S.; Zhao, I.S.; Hiraishi, N.; Duangthip, D.; Mei, M.L.; Lo, E.C.-M.; Chu, C.-H. Clinical Trials of Silver Diamine Fluoride in Arresting Caries among Children: A Systematic Review. JDR Clin. Transl. Res. 2016, 1, 201–210. [Google Scholar] [CrossRef]
- Mei, M.L.; Ito, L.; Cao, Y.; Li, Q.; Chu, C.-H.; Lo, E.C.-M. The inhibitory effects of silver diamine fluorides on cysteine cathepsins. J. Dent. 2014, 42, 329–335. [Google Scholar] [CrossRef] [PubMed]
- Mei, M.L.; Li, Q.; Chu, C.-H.; Yiu, C.K.; Lo, E.C.-M. The inhibitory effects of silver diamine fluoride at different concentrations on matrix metalloproteinases. Dent. Mater. 2012, 28, 903–908. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.-H.; Lo, E.C.-M. Microhardness of dentine in primary teeth after topical fluoride applications. J. Dent. 2008, 36, 387–391. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Lo, E.C.-M.; Li, C. Effect of silver and fluoride ions on enamel demineralization: A quantitative study using micro-computed tomography. Aust. Dent. J. 2012, 57, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Tan, H.; Lo, E.C.-M.; Dyson, J.; Luo, Y.; Corbet, E. A randomized trial on root caries prevention in elders. J. Dent. Res. 2010, 89, 1086–1090. [Google Scholar] [CrossRef] [PubMed]
- Attam, K.; Talwar, S.; Yadav, S.; Miglani, S. Comparative analysis of the effect of autoclaving and 10% formalin storage on extracted teeth: A microleakage evaluation. J. Conserv. Dent. 2009, 12, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Lolayekar, N.V.; Bhat, S.V.; Bhat, S.S. Disinfection methods of extracted human teeth. J. Oral Health Community Dent. 2007, 1, 27–29. [Google Scholar]
- Parsell, D.; Stewart, B.; Barker, J.R.; Nick, T.; Karns, L.; Johnson, R. The effect of steam sterilization on the physical properties and perceived cutting characteristics of extracted teeth. J. Dent. Educ. 1998, 62, 260–263. [Google Scholar] [PubMed]
- Yip, H.; Guo, J.; Wong, W. Protection offered by root-surface restorative materials against biofilm challenge. J. Dent. Res. 2007, 86, 431–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knight, G.M.; McIntyre, J.M.; Craig, G.G.; Mulyani, Z.P.S.; Gully, N.J. Inability to form a biofilm of Streptococcus mutans on silver fluoride-and potassium iodide-treated demineralized dentin. Quintessence Int. 2009, 40, 155–161. [Google Scholar] [PubMed]
- Knight, G.M.; McIntyre, J.M.; Craig, G.G.; Mulyani; Zilm, P.S.; Gully, N.J. An in vitro model to measure the effect of a silver fluoride and potassium iodide treatment on the permeability of demineralized dentine to Streptococcus mutans. Aust. Dent. J. 2005, 50, 242–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Besinis, A.; De Peralta, T.; Handy, R.D. Inhibition of biofilm formation and antibacterial properties of a silver nano-coating on human dentine. Nanotoxicology 2014, 8, 745–754. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Lo, E.; Liu, B.; Wong, M.; Chu, C. Randomized clinical trial on arresting dental root caries through silver diammine fluoride applications in community-dwelling elders. J. Dent. 2016, 51, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Xie, D.; Weng, Y.; Guo, X.; Zhao, J.; Gregory, R.L.; Zheng, C. Preparation and evaluation of a novel glass-ionomer cement with antibacterial functions. Dent. Mater. 2011, 27, 487–496. [Google Scholar] [CrossRef] [PubMed]
- Akcay, M.; Arslan, H.; Yasa, B.; Kavrık, F.; Yasa, E. Spectrophotometric analysis of crown discoloration induced by various antibiotic pastes used in revascularization. J. Endod. 2014, 40, 845–848. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Li, N.; Qi, Y.; Niu, L.; Elshafiy, S.; Mao, J.; Breschi, L.; Pashley, D.H.; Tay, F.R. The use of sodium trimetaphosphate as a biomimetic analog of matrix phosphoproteins for remineralization of artificial caries-like dentin. Dent. Mater. 2011, 27, 465–477. [Google Scholar] [CrossRef] [PubMed]
- Mei, M.L.; Ito, L.; Cao, Y.; Li, Q.L.; Lo, E.C.-M.; Chu, C.-H. Inhibitory effect of silver diamine fluoride on dentine demineralisation and collagen degradation. J. Dent. 2013, 41, 809–817. [Google Scholar] [CrossRef] [PubMed]
- Schneider, C.A.; Rasband, W.S.; Eliceiri, K.W. NIH Image to ImageJ: 25 years of image analysis. Nat. Methods 2012, 9, 671–675. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Coordinates | T0 | T1 | T7 | T14 | p-Value |
|---|---|---|---|---|---|---|
| SDF + KI | L* | 90.2 ± 6.0 | 89.9 ± 5.1 | 88.6 ± 6.4 | 68.5 ± 4.2 | <0.001 |
| a* | 0.6 ± 0.9 | 0.6 ± 0.9 | 0.6 ± 0.7 | 4.2 ± 1.1 | <0.001 | |
| b* | 33.6 ± 4.7 | 33.4 ± 5.2 | 33.9 ± 3.1 | 34.0 ± 4.3 | 0.840 | |
| SDF | L* | 89.5 ± 6.9 | 25.3 ± 4.1 | 27.4 ± 8.1 | 24.7 ± 5.8 | <0.001 |
| a* | 0.6 ± 1.0 | 4.5 ± 0.9 | 3.7 ± 1.6 | 3.9 ± 1.3 | <0.001 | |
| b* | 35.9 ± 5.1 | 12.2 ± 1.9 | 8.5 ± 4.4 | 9.6 ± 3.3 | <0.001 | |
| No treatment | L* | 89.2 ± 5.2 | 88.4 ± 6.0 | 88.4 ± 6.1 | 88.0 ± 5.5 | 0.281 |
| a* | 0.7 ± 1.1 | 0.6 ± 1.0 | 0.7 ± 0.9 | 0.6 ± 1.0 | 0.951 | |
| b* | 32.8 ± 4.7 | 33.2 ± 4.1 | 32.5 ± 4.9 | 33.1 ± 4.1 | 0.702 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, I.S.; Mei, M.L.; Burrow, M.F.; Lo, E.C.-M.; Chu, C.-H. Effect of Silver Diamine Fluoride and Potassium Iodide Treatment on Secondary Caries Prevention and Tooth Discolouration in Cervical Glass Ionomer Cement Restoration. Int. J. Mol. Sci. 2017, 18, 340. https://doi.org/10.3390/ijms18020340
Zhao IS, Mei ML, Burrow MF, Lo EC-M, Chu C-H. Effect of Silver Diamine Fluoride and Potassium Iodide Treatment on Secondary Caries Prevention and Tooth Discolouration in Cervical Glass Ionomer Cement Restoration. International Journal of Molecular Sciences. 2017; 18(2):340. https://doi.org/10.3390/ijms18020340
Chicago/Turabian StyleZhao, Irene Shuping, May Lei Mei, Michael F. Burrow, Edward Chin-Man Lo, and Chun-Hung Chu. 2017. "Effect of Silver Diamine Fluoride and Potassium Iodide Treatment on Secondary Caries Prevention and Tooth Discolouration in Cervical Glass Ionomer Cement Restoration" International Journal of Molecular Sciences 18, no. 2: 340. https://doi.org/10.3390/ijms18020340